Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
2.2. Ethics
2.3. Iodine Intake from Food and Supplements
2.4. Determination of Urinary Iodine and Creatinine
2.5. Definitions
2.6. Statistics
3. Results
3.1. Participant Characteristics
3.2. Urinary Iodine Concentration (UIC) and Iodine Intake from Food and Supplements
3.3. Estimated Usual Iodine Intake and Probability of Adequate Iodine Intake
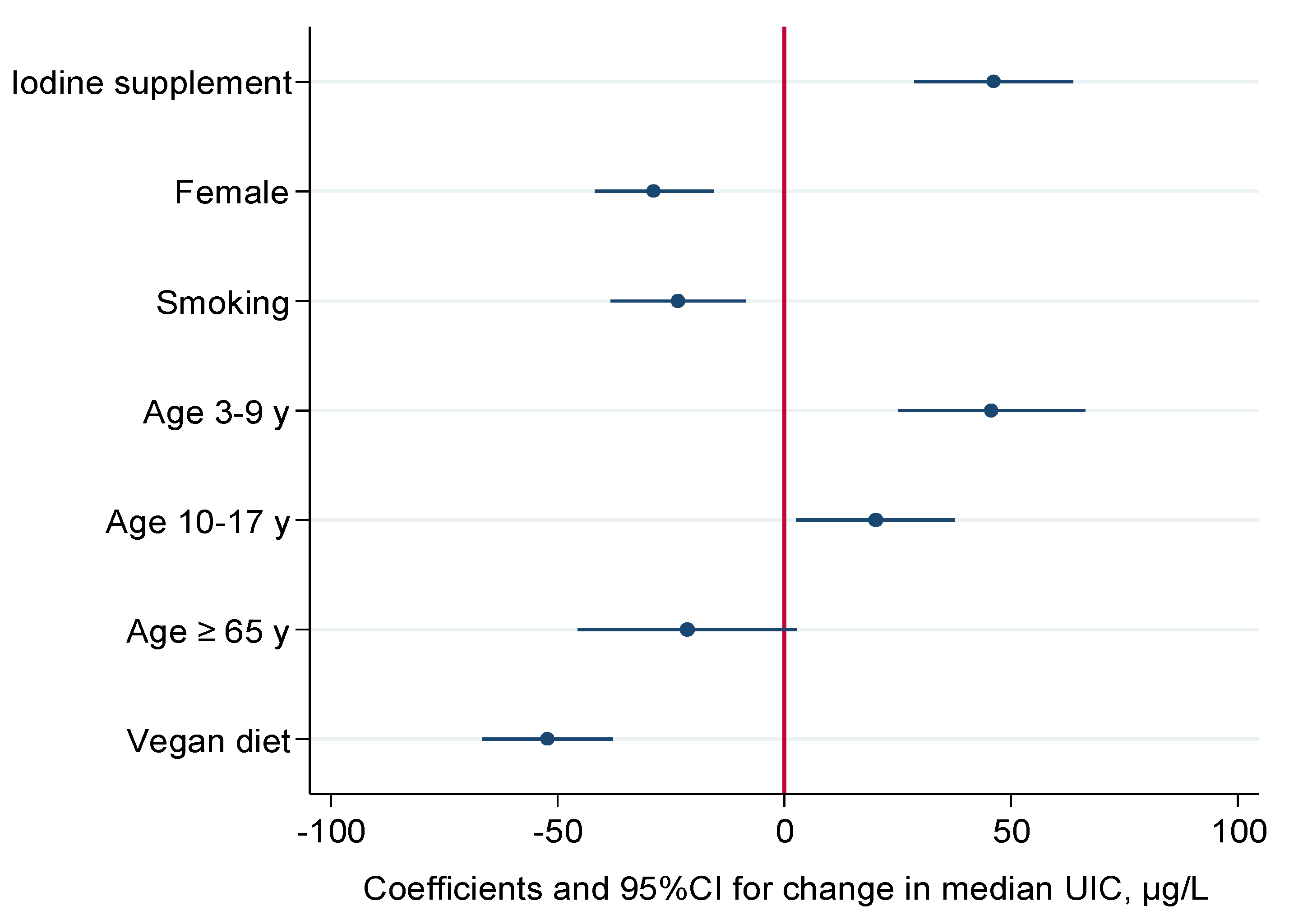
3.4. Predictors of Urinary Iodine Concentrations
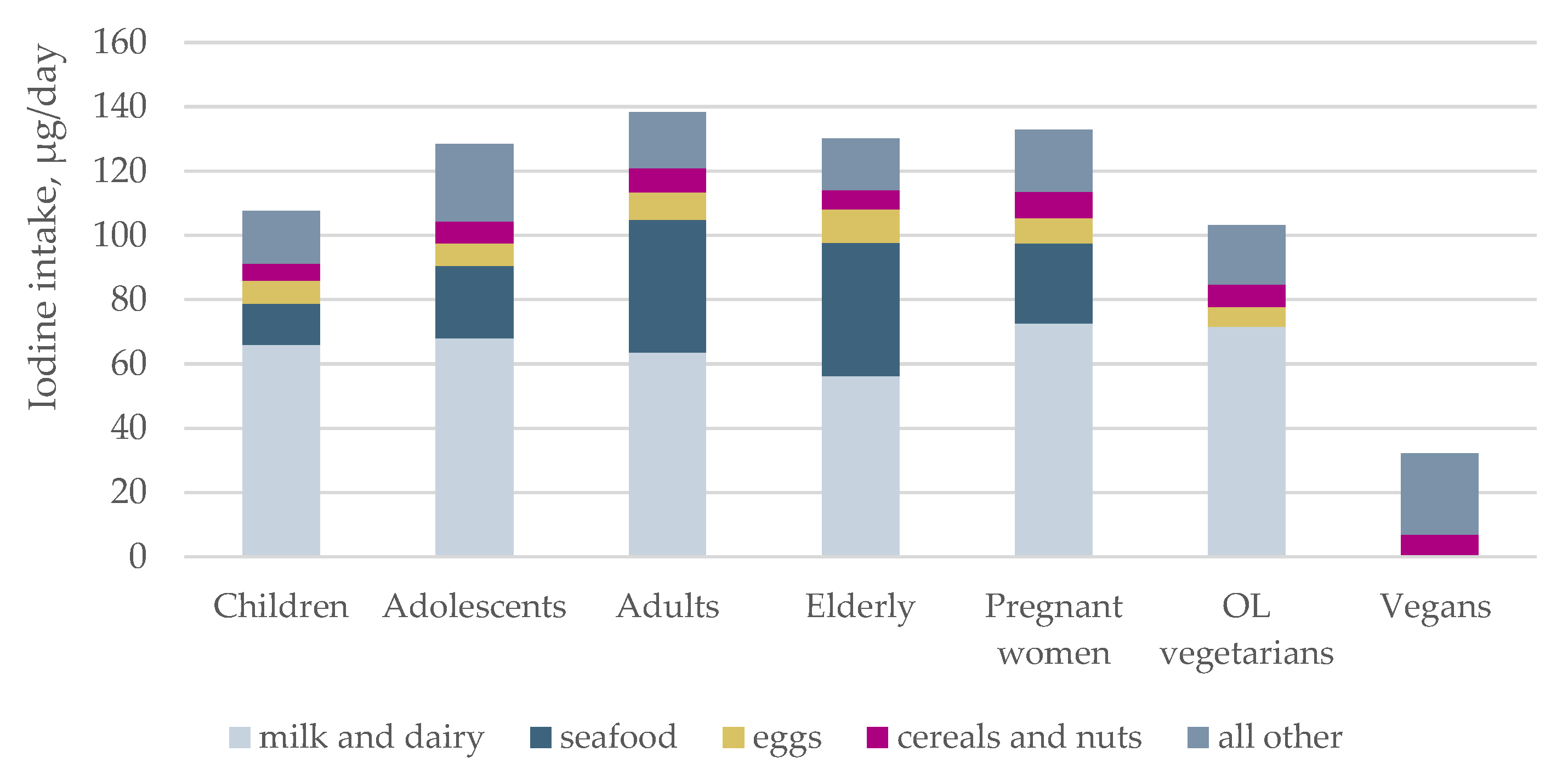
3.5. Sources of Iodine
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). International Council for Control of Iodine Deficiency Disorders (ICCIDD), United Nations International Children's Emergency Fund (UNICEF). In Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Dahl, L.; Meltzer, H.M. The Iodine Content of Foods and Diets: Norwegian Perspectives. In Comprehensive Handbook of Iodine; Preedy, V.R., Burrow, G.N., Watson, R.R., Eds.; Academic Press: London, UK, 2009; pp. 345–352. [Google Scholar]
- Frey, H.; Rosenlund, B.; Try, K.; Theodorsen, L. Urinary excretion of iodine in Norway. In Iodine Deficiency in Europe; Delange, F., Ed.; Plenum Press: New York, NY, USA, 1993; pp. 297–300. [Google Scholar]
- Lazarus, J.H. Iodine status in europe in 2014. Eur. Thyroid J. 2014, 3, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Manousou, S.; Dahl, L.; Heinsbaek Thuesen, B.; Hulthen, L.; Nystrom Filipsson, H. Iodine deficiency and nutrition in Scandinavia. Minerva Med. 2017, 108, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, H.F.; Brantsaeter, A.L.; Erlund, I.; Gunnarsdottir, I.; Hulthen, L.; Laurberg, P.; Mattisson, I.; Rasmussen, L.B.; Virtanen, S.; Meltzer, H.M. Iodine status in the Nordic countries—Past and present. Food Nutr. Res. 2016, 60, 31969. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Abel, M.H.; Haugen, M.; Meltzer, H.M. Risk of suboptimal iodine intake in pregnant norwegian women. Nutrients 2013, 5, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Lilleengen, A.M.; Aakre, I.; Dudareva, A.; Gjengedal, E.L.F.; Meltzer, H.M.; Brantsaeter, A.L. Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Abel, M.H.; Caspersen, I.H.; Meltzer, H.M.; Haugen, M.; Brandlistuen, R.E.; Aase, H.; Alexander, J.; Torheim, L.E.; Brantsaeter, A.L. Suboptimal Maternal Iodine Intake Is Associated with Impaired Child Neurodevelopment at 3 Years of Age in the Norwegian Mother and Child Cohort Study. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Hynes, K.L.; Otahal, P.; Hay, I.; Burgess, J.R. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. J. Clin. Endocrinol. Metab. 2013, 98, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104, 918s–923s. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. Iodine deficiency and excess in children: Worldwide status in 2013. Endocr. Pract. 2013, 19, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Skeaff, S.A. Assessment of Population Iodine Status. In Iodine Dificiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer: Cham, Switzerland, 2017; pp. 15–28. [Google Scholar]
- Rasmussen, L.B.; Carle, A.; Jorgensen, T.; Knudsen, N.; Laurberg, P.; Pedersen, I.B.; Perrild, H.; Vejbjerg, P.; Ovesen, L. Iodine intake before and after mandatory iodization in Denmark: Results from the Danish Investigation of Iodine Intake and Thyroid Diseases (DanThyr) study. Br. J. Nutr. 2008, 100, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Gizak, M.; Gorstein, J.; Andersson, M. Epidemiology of Iodine Deficiency. In Iodine Deficiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 29–43. [Google Scholar]
- National Nutrition Council. Risk of Iodine Deficiency in Norway. Identification of an Acute Need for Action; Report in Norwegian; Technical Report; The Norwegian Directorate of Health: Oslo, Norway, 2016. Available online: http://www.ernaeringsradet.no/wp-content/uploads/2016/06/IS-0591_RisikoForJodmangeliNorge.pdf (accessed on 7 March 2017).
- Bath, S.C.; Rayman, M.P. Iodine deficiency in the U.K.: An overlooked cause of impaired neurodevelopment? Proc. Nutr. Soc. 2013, 72, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; McLean, R.; Davies, B.; Hawkins, R.; Meiklejohn, E.; Ma, Z.F.; Skeaff, S. Adequate Iodine Status in New Zealand School Children Post-Fortification of Bread with Iodised Salt. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Johansson, L.; Julshamn, K.; Meltzer, H.M. The iodine content of Norwegian foods and diets. Public Health Nutr. 2004, 7, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Directorate of Health. Utviklingen i Norsk kosthold 2015; IS-2382; Helsedirektoratet: Oslo, Norway, 2015. (In Norwegian) [Google Scholar]
- Totland, T.H.; Melnæs, B.K.; Lundberg-Hallén, N.; Helland-Kigen, K.M.; Lund-Blix, N.A.; Myhre, J.B.; Johansen, A.M.W.; Løken, E.B.; Andersen, L.F. Norkost 3, National Dietary Survey in Men and Women in Norway Aged 18–70 Years; The University of Oslo, the Norwegian Food Safety Authority and the Norwegian Directorate of Health: Oslo, Norway, 2012. (In Norwegian) [Google Scholar]
- Troan, G.; Dahl, L.; Meltzer, H.M.; Abel, M.H.; Indahl, U.G.; Haug, A.; Prestlokken, E. A model to secure a stable iodine concentration in milk. Food Nutr. Res. 2015, 59, 29829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.B.; Ovesen, L.; Christiansen, E. Day-to-day and within-day variation in urinary iodine excretion. Eur. J. Clin. Nutr. 1999, 53, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Hussein, I.; Al Ghannami, S.; El Badawi, S.; Al Hamad, N.M.; Abbas Hajj, B.; Al-Thani, M.; Al-Thani, A.A.; Winichagoon, P.; Pongcharoen, T.; et al. Estimation of the Prevalence of Inadequate and Excessive Iodine Intakes in School-Age Children from the Adjusted Distribution of Urinary Iodine Concentrations from Population Surveys. J. Nutr. 2016, 146, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Venn, B.J.; Manning, P.J.; Cameron, C.M.; Skeaff, S.A. The sensitivity and specificity of thyroglobulin concentration using repeated measures of urinary iodine excretion. Eur. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Perrine, C.G.; Cogswell, M.E.; Swanson, C.A.; Sullivan, K.M.; Chen, T.C.; Carriquiry, A.L.; Dodd, K.W.; Caldwell, K.L.; Wang, C.Y. Comparison of population iodine estimates from 24-hour urine and timed-spot urine samples. Thyroid 2014, 24, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Laurberg, P.; Andersen, S.; Rasmussen, L.B.; Ovesen, L.; Jorgensen, T. Estimation of iodine intake from various urinary iodine measurements in population studies. Thyroid 2009, 19, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Juan, W.; Trumbo, P.R.; Spungen, J.H.; Dwyer, J.T.; Carriquiry, A.L.; Zimmerman, T.P.; Swanson, C.A.; Murphy, S.P. Comparison of 2 methods for estimating the prevalences of inadequate and excessive iodine intakes. Am. J. Clin. Nutr. 2016, 104, 888s–897s. [Google Scholar] [CrossRef] [PubMed]
- Brera, C.; de Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Lanzone, A.; Del Sordo, G.; Buonsenso, D.; Chiaretti, A.; Hardie, L.; et al. Experimental study of deoxynivalenol biomarkers in urine. EFSA Support. Publ. 2015, 12. [Google Scholar] [CrossRef]
- Norwegian Food Safety Authority. Matvaretabellen [The Norwegian Food Database]. Available online: http://www.matvaretabellen.no/ (accessed on 10 December 2015).
- Lauritsen, J. FoodCalc; Data Program from the Project “Diet, Cancer and Health” at the Danish Cancer Society. Available online: http://www.ibt.ku.dk/jesper/foodcalc (accessed on 1 February 2005).
- NNR12 Project Group. Iodine. In Nordic Nutrition Recommendations 2012 Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- EFSA, NDA Panel (EFSA Panel on Dietetic Products Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for Iodine. EFSA J. 2014, 12. [Google Scholar] [CrossRef] [Green Version]
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Institute of Medicine. DRI Dietary Reference Intakes: Applications in Dietary Assessment, part III, Chapter 4: Using the Estimated Average Requirement for Nutrient Assessment of Groups; National Academies Press: Washington, DC, USA, 2000; pp. 71–143. [Google Scholar]
- Joseph, M.L.; Carriquiry, A. A measurement error approach to assess the association between dietary diversity, nutrient intake, and mean probability of adequacy. J. Nutr. 2010, 140, 2094s–2101s. [Google Scholar] [CrossRef] [PubMed]
- Le Cook, B.; Manning, W.G. Thinking beyond the mean: A practical guide for using quantile regression methods for health services research. Shanghai Arch. Psychiatry 2013, 25, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fields, C.; Borak, J. Iodine Deficiency in Vegetarian and Vegan Diets: Evidence-Based Review of the World’s Literature on Iodine Content in Vegetarian Diets. In Comprehensive Handbook of Iodine; Preedy, V., Burrow, G., Watson, R., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Li, M.; Eastman, C.J. The changing epidemiology of iodine deficiency. Nat. Rev. Endocrinol. 2012, 8, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Garnweidner-Holme, L.; Aakre, I.; Lilleengen, A.M.; Brantsaeter, A.L.; Henjum, S. Knowledge about Iodine in Pregnant and Lactating Women in the Oslo Area, Norway. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Ystrom, E.; Caspersen, I.H.; Meltzer, H.M.; Aase, H.; Torheim, L.E.; Askeland, R.B.; Reichborn-Kjennerud, T.; Brantsæter, A.L. Maternal Iodine Intake and Offspring Attention-Deficit/Hyperactivity Disorder: Results from a Large Prospective Cohort Study. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Berg, G.; Eggertsen, R.; Filipsson, H.; Gramatkovski, E.; Hansson, M.; Hulthen, L.; Milakovic, M.; Nystrom, E. Adequate iodine nutrition in Sweden: A cross-sectional national study of urinary iodine concentration in school-age children. Eur. J. Clin. Nutr. 2009, 63, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Costa Leite, J.; Keating, E.; Pestana, D.; Cruz Fernandes, V.; Maia, M.L.; Norberto, S.; Pinto, E.; Moreira-Rosario, A.; Sintra, D.; Moreira, B.; et al. Iodine Status and Iodised Salt Consumption in Portuguese School-Aged Children: The Iogeneration Study. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Beckford, K.; Grimes, C.A.; Margerison, C.; Riddell, L.J.; Skeaff, S.A.; Nowson, C.A. Iodine Intakes of Victorian Schoolchildren Measured Using 24-h Urinary Iodine Excretion. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Granfors, M.; Andersson, M.; Stinca, S.; Akerud, H.; Skalkidou, A.; Poromaa, I.S.; Wikstrom, A.K.; Nystrom, H.F. Iodine deficiency in a study population of pregnant women in Sweden. Acta Obstet. Gynecol. Scand. 2015, 94, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Travers, C.A.; Guttikonda, K.; Norton, C.A.; Lewis, P.R.; Mollart, L.J.; Wiley, V.; Wilcken, B.; Eastman, C.J.; Boyages, S.C. Iodine status in pregnant women and their newborns: Are our babies at risk of iodine deficiency? Med. J. Aust. 2006, 184, 617–620. [Google Scholar] [PubMed]
- Andersen, S.L.; Sorensen, L.K.; Krejbjerg, A.; Moller, M.; Laurberg, P. Iodine deficiency in Danish pregnant women. Dan. Med. J. 2013, 60, A4657. [Google Scholar] [PubMed]
- Leitzmann, C. Vegetarian nutrition: Past, present, future. Am. J. Clin. Nutr. 2014, 100, 496s–502s. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Hill, S.; Infante, H.G.; Elghul, S.; Nezianya, C.J.; Rayman, M.P. Iodine concentration of milk-alternative drinks available in the UK in comparison with cows' milk. Br. J. Nutr. 2017, 118, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Lightowler, H.J.; Davies, G.J. Iodine intake and iodine deficiency in vegans as assessed by the duplicate-portion technique and urinary iodine excretion. Br. J. Nutr. 1998, 80, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Krajcovicova-Kudlackova, M.; Buckova, K.; Klimes, I.; Sebokova, E. Iodine deficiency in vegetarians and vegans. Ann. Nutr. Metab. 2003, 47, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Elorinne, A.L.; Alfthan, G.; Erlund, I.; Kivimaki, H.; Paju, A.; Salminen, I.; Turpeinen, U.; Voutilainen, S.; Laakso, J. Food and Nutrient Intake and Nutritional Status of Finnish Vegans and Non-Vegetarians. PLoS ONE 2016, 11, e0148235. [Google Scholar] [CrossRef] [PubMed]
- Schupbach, R.; Wegmuller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Lamar, A.; He, X.; Braverman, L.E.; Pearce, E.N. Iodine status and thyroid function of Boston-area vegetarians and vegans. J. Clin. Endocrinol. Metab. 2011, 96, E1303–E1307. [Google Scholar] [CrossRef] [PubMed]
- Ovesen, L.; Boeing, H. The use of biomarkers in multicentric studies with particular consideration of iodine, sodium, iron, folate and vitamin D. Eur. J. Clin. Nutr. 2002, 56, S12–S17. [Google Scholar] [CrossRef] [PubMed]
- Als, C.; Helbling, A.; Peter, K.; Haldimann, M.; Zimmerli, B.; Gerber, H. Urinary iodine concentration follows a circadian rhythm: A study with 3023 spot urine samples in adults and children. J. Clin. Endocrinol. Metab. 2000, 85, 1367–1369. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.D.; Smith, T.E.; Butler, K.A.; Packer, M.A. An evaluation of urinary measures of iodine and selenium status. J. Trace Elem. Med. Biol. 1996, 10, 214–222. [Google Scholar] [CrossRef]
- Andersen, S.; Karmisholt, J.; Pedersen, K.M.; Laurberg, P. Reliability of studies of iodine intake and recommendations for number of samples in groups and in individuals. Br. J. Nutr. 2008, 99, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Haddow, J.E.; McClain, M.R.; Palomaki, G.E.; Hollowell, J.G. Urine iodine measurements, creatinine adjustment, and thyroid deficiency in an adult United States population. J. Clin. Endocrinol. Metab. 2007, 92, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Update on iodine status worldwide. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Frisoli, T.M.; Schmieder, R.E.; Grodzicki, T.; Messerli, F.H. Salt and hypertension: Is salt dietary reduction worth the effort? Am. J. Med. 2012, 125, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.; Probst, Y.; Kiene, G. Dietary Iodine Intake of the Australian Population after Introduction of a Mandatory Iodine Fortification Programme. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; de Benoist, B.; Delange, F.; Zupan, J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: Conclusions and recommendations of the Technical Consultation. Public Health Nutr. 2007, 10, 1606–1611. [Google Scholar] [PubMed]
- Gowachirapant, S.; Jaiswal, N.; Melse-Boonstra, A.; Galetti, V.; Stinca, S.; Mackenzie, I.; Thomas, S.; Thomas, T.; Winichagoon, P.; Srinivasan, K.; et al. Effect of iodine supplementation in pregnant women on child neurodevelopment: A randomised, double-blind, placebo-controlled trial. Lancet 2017, 5, 853–863. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroups | n | Sex (Male) n (%) | Age, Years Mean ± SD | Weight, kg Mean ± SD | Supplementary Iodine n (%) |
|---|---|---|---|---|---|
| Age and life-stage groups | |||||
| Children 3–9 years | 47 | 30 (64) | 6.3 ± 1.9 | 23 ± 5.6 | 0 |
| Adolescents 10–17 years | 46 | 17 (37) | 13.4 ± 2.3 | 50 ± 12.7 | 1 (2.2) |
| Adults 18–64 years | 71 | 34 (48) | 42.1 ± 11.4 | 73 ± 12.7 | 2 (2.8) |
| Elderly 65+ years | 23 | 11 (48) | 70.7 ± 6.7 | 72 ± 11.3 | 2 (8.7) |
| Pregnant women | 45 | 33.0 ± 4.6 | 66 ± 8.2 | 11 (24) | |
| Vegetarians combined | 44 | 14 (32) | 34.2 ± 13.1 | 66 ± 15.1 | 10 (23) |
| Vegetarian groups | |||||
| Ovo-Lacto vegetarians 1 | 25 | 11 (44) | 37.2 ± 15.7 | 64 ± 15.9 | 5 (20) |
| Vegans 2 | 19 | 3 (16) | 30.1 ± 7.1 | 67 ± 14.4 | 5 (16) |
| Subgroup | n | UIC 1 µg/L | UIC1 µg/g Creatinine | Inadequate Iodine Intake 2 | Excessive Iodine Intake 3 |
|---|---|---|---|---|---|
| Median (95% CI) | Median (95% CI) | n (%) | n (%) | ||
| All participants | 276 | 101 (90, 110) | 92 (85, 100) | 148 (54) | 12 (4.3) |
| Children 3–9 years | 47 | 148 (129, 145) | 143 (130, 174) | 5 (11) | 3 (6.4) |
| Adolescents 10–17 years | 46 | 109 (90, 123) | 76 (64, 92) | 19 (41) | 3 (6.5) |
| Adults 18–64 years | 71 | 96 (81, 113) | 77 (66, 89) | 38 (54) | 3 (4.2) |
| Elderly 65+ years | 23 | 62 (51, 97) | 91 (74, 127) | 16 (70) | 0 |
| Pregnant women | 45 | 84 (62, 107) | 101 (78, 135) | 40 (89) | 0 |
| Ovo-Lacto Vegetarians | 25 | 105 (50, 129) | 84 (63, 101) | 12 (48) | 2 (8.0) |
| Vegans | 19 | 46 (32, 62) | 47 (25, 48) | 18 (95) | 1 (5.3) |
| Subgroup | n | Iodine from Food Only 1 | Total Iodine 2 | Total Iodine below RDI 3 |
|---|---|---|---|---|
| Median (P25, P75) | Median (P25, P75) | n (%) | ||
| All participants | 276 | 103 (69, 150) | 112 (77, 175) | 182 (66) |
| Children 3–9 years | 47 | 93 (72, 139) | 93 (72, 139) | 27 (57) |
| Adolescents 10–17 years | 46 | 106 (68, 150) | 108 (68, 151) | 33 (72) |
| Adults 18–64 years | 71 | 116 (80, 195) | 117 (81, 195) | 47 (66) |
| Elderly 65+ years | 23 | 107 (85, 161) | 107 (85, 161) | 16 (70) |
| Pregnant women | 45 | 118 (90, 176) | 154 (105, 228) | 26 (58) |
| Ovo-Lacto Vegetarians | 25 | 86 (50, 134) | 116 (85, 194) | 16 (64) |
| Vegans | 19 | 26 (15, 42) | 31 (15, 88) | 17 (90) |
| Subgroup | n | Estimated Usual Iodine Intake, µg/d | Probability of Adequacy (%) 2 | |
|---|---|---|---|---|
| Median (P25, P75) | Mean (SD) | Mean (SD) | ||
| All participants | 276 | 101 (75, 150) | 119 (66) | 60 (41) |
| Children 3–9 years | 47 | 89 (77, 120) | 100 (34) | 82 (28) |
| Adolescents 10–17 years | 46 | 92 (67, 133) | 115 (74) | 61 (43) |
| Adults 18–64 years | 71 | 109 (76, 149) | 122 (63) | 63 (39) |
| Elderly 65+ years | 23 | 112 (76, 168) | 121 (58) | 61 (37) |
| Pregnant women | 45 | 154 (107, 225) | 161 (73) | 47 (42) |
| Ovo-Lacto Vegetarians | 25 | 102 (64, 175) | 119 (65) | 60 (41) |
| Vegans | 19 | 57 (15, 90) | 64 (59) | 14 (32) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brantsæter, A.L.; Knutsen, H.K.; Johansen, N.C.; Nyheim, K.A.; Erlund, I.; Meltzer, H.M.; Henjum, S. Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample. Nutrients 2018, 10, 230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020230
Brantsæter AL, Knutsen HK, Johansen NC, Nyheim KA, Erlund I, Meltzer HM, Henjum S. Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample. Nutrients. 2018; 10(2):230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020230
Chicago/Turabian StyleBrantsæter, Anne Lise, Helle Katrine Knutsen, Nina Cathrine Johansen, Kristine Aastad Nyheim, Iris Erlund, Helle Margrete Meltzer, and Sigrun Henjum. 2018. "Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample" Nutrients 10, no. 2: 230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020230