The Relationship between Maternal Nutrition during Pregnancy and Offspring Kidney Structure and Function in Humans: A Systematic Review

 ,
,
Abstract
:1. Introduction
- What is known about the relationship between maternal nutrition during pregnancy and offspring kidney structure and function?
- Which areas of research have not been addressed in the current literature?
2. Methods
2.1. Study Identification
2.2. Inclusion Criteria
2.2.1. Types of Participants
2.2.2. Types of Studies
2.2.3. Types of Exposures/Interventions
2.2.4. Types of Outcome Measures
2.3. Study Selection
2.4. Study Quality
2.5. Data Extraction and Synthesis
3. Results
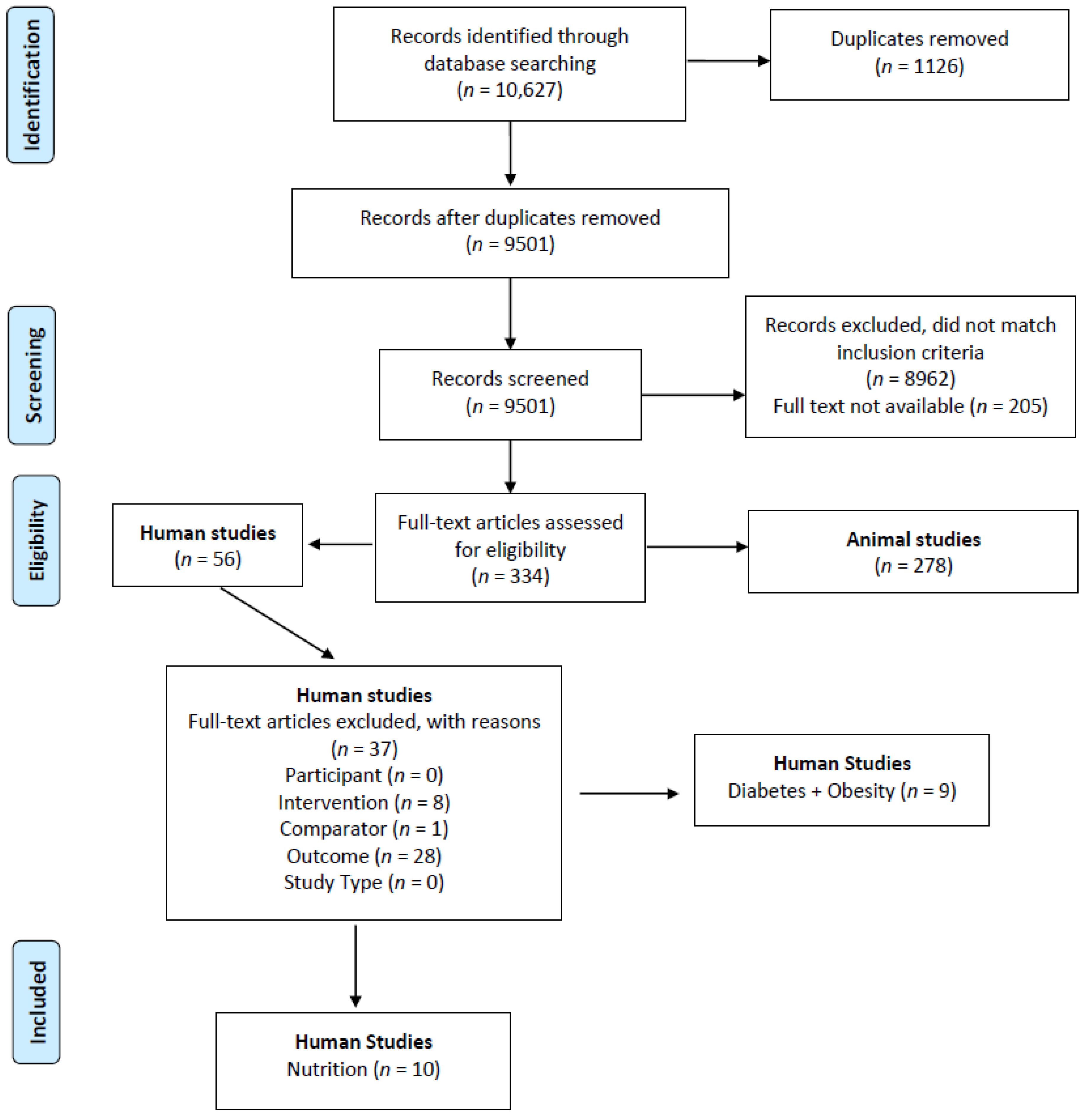
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
3.4. Relationship between Maternal Nutrition during Pregnancy and Offspring Kidney Structure or Function (Table 3 and Table 4)
3.4.1. Vitamin A
3.4.2. Folate & Vitamin B12
3.4.3. Vitamin D
3.4.4. Iron
3.4.5. Famine
3.4.6. Protein
4. Discussion
4.1. Maternal Nutrition and Offspring Kidney Structure or Function
4.1.1. Maternal Micronutrient Deficiencies
4.1.2. Maternal Energy and Protein Restriction
4.2. Quality of Included Studies
4.3. Strengths and Limitations
4.4. Implication for Practice
4.5. Implication for Research
- Prospective studies should be designed to ensure accurate assessment of maternal nutritional status and dietary intake at specific times in gestation;
- High quality longitudinal studies with longer follow-ups beyond childhood are needed;
- Consideration of the use of common outcomes for maternal and offspring kidney health to facilitate meta-analysis of results across studies.
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Barker, D.J.P. Intrauterine programming of adult disease. Mol. Med. Today 1995, 4, 18–23. [Google Scholar] [CrossRef]
- Barker, D.J.P. Developmental origins of adult health and disease. J. Epidemiol. Community Health 2004, 58, 114–115. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Osmond, C.; Law, C.M. The intrauterine and early postnatal origins of cardiovascular disease and chronic bronchitis. J. Epidemiol. Community Health 1989, 43, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, S.C. Developmental programming of health and disease. Proc. Nutr. Soc. 2006, 65, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Wood-Bradley, R.J.; Barrand, S.; Giot, A.; Armitage, J.A. Understanding the role of maternal diet on kidney development; an opportunity to improve cardiovascular and renal health for future generations. Nutrients 2015, 7, 1881–1905. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.L.; Ingelfinger, J.R.; Nyengaard, J.R.; Rasch, R. Maternal protein restriction suppresses the newborn renin-angiotensin system and programs adult hypertension in rats. Pediatr. Res. 2001, 49, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.L.; Ingelfinger, J.R.; Rasch, R. Modest maternal protein restriction fails to program adult hypertension in female rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R1131–R1136. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, S.C.; Welham, S.J.; Jackson, A.A. Fetal exposure to a maternal low protein diet impairs nephrogenesis and promotes hypertension in the rat. Life Sci. 1999, 64, 965–974. [Google Scholar] [CrossRef]
- Lelievre-Pegorier, M.; Vilar, J.; Ferrier, M.L.; Moreau, E.; Freund, N.; Gilbert, T.; Merlet-Bénichou, C. Mild vitamin A deficiency leads to inborn nephon deficit in the rat. Kidney Int. 1998, 54, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Lisle, S.J.; Lewis, R.M.; Petry, C.J.; Ozanne, S.E.; Hales, C.N.; Forhead, A.J. Effect of maternal iron restriction during pregnancy on renal morphology in the adult rat offspring. Br. J. Nutr. 2003, 90, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.Y.; Taylor, P.D.; Dekou, V.; Seed, P.T.; Lakasing, L.; Graham, D.; Dominiczak, A.F.; Hanson, M.A.; Poston, L. Gender-linked hypertension in offspring of lard-fed pregnant rats. Hypertension 2003, 41, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.D.; Khan, I.Y.; Lakasing, L.; Dekou, V.; O’Brien-Coker, I.; Mallet, A.I.; Hanson, M.A.; Poston, L. Uterine artery function in pregnant rats fed a diet supplemented with animal lard. Exp. Physiol. 2003, 88, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Armitage, J.A.; Lakasing, L.; Taylor, P.D.; Balachandran, A.A.; Jensen, R.I.; Dekou, V.; Ashton, N.; Nyengaard, J.R.; Poston, L. Developmental programming of aortic and renal structure in offspring of rats fed fat-rich diets in pregnancy. J. Physiol. 2005, 565, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Bayol, S.A.; Farrington, S.J.; Stickland, N.C. A maternal ‘junk food’ diet in pregnancy and lactation promotes an exacerbated taste for ‘junk food’ and a greater propensity for obesity in rat offspring. Br. J. Nutr. 2007, 98, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Benkalfat, N.B.; Merzouk, H.; Bouanane, S.; Merzouk, S.A.; Bellenger, J.; Gresti, J.; Tessier, C.; Narce, M. Altered adipose tissue metabolism in offspring of dietary obese rat dams. Clin. Sci. 2011, 121, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Parente, L.B.; Aguila, M.B.; Mandarim-de-Lacerda, C.A. Deleterious effects of high-fat diet on perinatal and postweaning periods in adult rat offspring. Clin. Nutr. 2008, 27, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Katewa, S.D.; Palaniyappan, A.; Pandya, J.D.; Patel, M.S. Maternal high-fat diet consumption results in fetal malprogramming predisposing to the onset of metabolic syndrome-like phenotype in adulthood. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E792–E799. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.M.; Alexander., B.T.; Roach, L.; Haggerty, D.; Marbury, D.C.; Hutchens, Z.M.; Flynn, E.R.; Maric-Bilkan, C. Exposure to maternal overnutrition and a high-fat diet during early postnatal development increases susceptibility to renal and metabolic injury later in life. Am. J. Physiol. Renal Physiol. 2012, 302, F774–F783. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.K.; Smith, R.; Simpson, S.J.; Giles, W.B.; Raubenheimer, D.; Collins, C.E. Dietary balance during pregnancy is associated with fetal adiposity and fat distribution. Am. J. Clin. Nutr. 2012, 96, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Nowson, C.; Hure, A.J.; Smith, R.; Simpson, S.J.; Raubenheimer, D.; MacDonald-Wicks, L.; Collins, C.E. Lower protein-to-carbohydrate ratio in maternal diet is associated with higher childhood systolic blood pressure up to age four years. Nutrients 2015, 7, 3078–3093. [Google Scholar] [CrossRef] [PubMed]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; University of York: New York, NY, USA, 2008. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PG. preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- American Dietetic Association. ADA Quality Criteria Checklist: Primary Research; American Dietetic Association: Chicago, IL, USA, 2008. [Google Scholar]
- Hawkesworth, S.; Wagatsuma, Y.; Kahn, A.I.; Hawlader, M.D.; Fulford, A.J.; Arifeen, S.E.; Persson, L.Å.; Moore, S.E. Combined food and micronutrient supplements during pregnancy have limited impact on child blood pressure and kidney function in rural Bangladesh. J. Nutr. 2013, 143, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.P.; Christian, P.; Schulze, K.J.; Leclerq, S.C.; West, K.P., Jr.; Khatry, S.K. Antenatal micronutrient supplementation reduces metabolic syndrome in 6 to 8 year-old children in rural Nepal. J. Nutr. 2009, 139, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.P.; Christian, P.; Katz, J.; Schulze, K.J.; Wu, L.S.; LeClerq, S.C.; Shakya, T.R.; Khatry, S.K.; West, K.P. Maternal supplementation with vitamin A or beta-carotene and cardiovascular risk factors among pre-adolescent children in rural Nepal. J. Dev. Orig. Health Dise 2010, 1, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Guo, C.; Nichols, C.; Chen, S.; Martorell, R. Elevated levels of protein in urine in adulthood after exposure to the Chinese famine of 1959–1961 during gestation and the early postnatal period. Int. J. Epidemiol. 2014, 43, 1806–1814. [Google Scholar] [CrossRef] [PubMed]
- Painter, R.C.; Roseboom, T.J.; van Montfrans, G.A.; Bossuyt, P.M.; Krediet, R.T.; Osmond, C.; Barker, D.J.; Bleker, O.P. Microalbuminuria in adults after prenatal exposure to the Dutch famine. J. Am. Soc. Nephrol: JASN 2005, 16, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Miliku, K.; Voortman, T.; van den Hooven, E.H.; Hofman, A.; Franco, O.H.; Jaddoe, V.W. First-trimester maternal protein intake and childhood kidney outcomes: The Generation R Study. Am. J. Clin. Nutr. 2015, 102, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Miliku, K.; Voortman, T.; Franco, O.H.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Hofman, A.; Tiemeier, H.; Jaddoe, V.W. Vitamin D status during fetal life and childhood kidney outcomes. Eur. J. Clin. Nutr. 2016, 70, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Miliku, K.; Mesu, A.; Franco, O.H.; Hofman, A.; Steegers, E.A.; Jaddoe, V.W. Maternal and fetal folate, vitamin B12, and homocysteine concentrations and childhood kidney outcomes. Am. J. Kidney Dis. 2017, 69, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Goodyer, P.; Kurpad, A.; Rekha, S.; Muthayya, S.; Dwarkanath, P.; Iyengar, A.; Philip, B.; Mhaskar, A.; Benjamin, A.; Maharaj, S.; et al. Effects of maternal vitamin A status on kidney development: A pilot study. Pediatr. Nephrol. 2007, 22, 209–214. [Google Scholar] [CrossRef] [PubMed]
- El-Khashab, E.K.; Hamdy, A.M.; Maher, K.M.; Fouad, M.A.; Abbas, G.Z. Effect of maternal vitamin A deficiency during pregnancy on neonatal kidney size. J. Perinat. Med. 2013, 41, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Bertram, J.F.; Douglas-Denton, R.N.; Diouf, B.; Hughson, M.D.; Hoy, W.E. Human nephron number: Implications for health and disease. Pediatr. Nephrol. 2011, 26, 1529. [Google Scholar] [CrossRef] [PubMed]
- Hughson, M.; Farris, A.B., 3rd.; Douglas-Denton, R.; Hoy, W.E.; Bertram, J.F. Glomerular number and size in autopsy kidneys: The relationship to birth weight. Kidney Int. 2003, 63, 2113–2122. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A.; Bertram, J.F.; Brenner, B.M.; Fall, C.; Hoy, W.E.; Ozanne, S.E.; Vikse, B.E. Effect of fetal and child health on kidney development and long-term risk of hypertension and kidney disease. Lancet 2013, 382, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Luyckx, V.A.; Perico, N.; Somaschini, M.; Manfellotto, D.; Valensise, H.; Cetin, I.; Simeoni, U.; Allegaert, K.; Vikse, B.E.; Steegers, E.A.; et al. A developmental approach to the prevention of hypertension and kidney disease: A report from the Low Birth Weight and Nephron Number Working Group. Lancet 2017, 390, 424–428. [Google Scholar] [CrossRef]
- Dorey, E.S.; Pantaleon, M.; Weir, K.A.; Moritz, K.M. Adverse prenatal environment and kidney development: Implications for programing of adult disease. Reproduction 2014, 147, R189–R198. [Google Scholar] [CrossRef] [PubMed]
- Merlet-Benichou, C.; Vilar, J.; Lelievre-Pegorier, M.; Gilbert, T. Role of retinoids in renal development: Pathophysiological implication. Curr. Opin. Nephrol. Hypertens. 1999, 8, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Global prevalence of vitamin A deficiency in populations at risk 1995–2005: WHO global database on Vitamin A deficiency. Available online: http://apps.who.int/iris/bitstream/10665/44110/1/9789241598019_eng.pdf (accessed on 20 March 2017).
- Lee, L.M.; Leung, C.Y.; Tang, W.W.; Choi, H.L.; Leung, Y.C.; McCaffery, P.J.; Wang, C.C.; Woolf, A.S.; Shum, A.S. A paradoxical teratogenic mechanism for retinoic acid. Proc. Natl. Acad. Sci. USA 2012, 109, 13668–13673. [Google Scholar] [CrossRef] [PubMed]
- Stoltzfus, R.J. Iron deficiency: Global prevalence and consequences. Food Nutr. Bull. 2003, 24, S99–S103. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, C.J.; Antipatis, C. Micronutrient programming of development throughout gestation. Reproduction 2001, 122, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Selhub, J.; Bostom, A.G.; Wilson, P.W.; Rosenberg, I.H. The effect of folic acid fortification on plasma folate and total homocysteine concentrations. N. Engl. J. Med. 1999, 340, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, G.; Bogdarina, I.G.; Stupka, E.; Clark, A.J.; Langley-Evans, S. Genome-wide methylation and gene expression changes in newborn rats following maternal protein restriction and reversal by folic acid. PLoS ONE 2013, 8, e82989. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Lou, X.; Zou, Z.; Mou, N.; Wu, W.; Huang, X.; Tan, H. Folic acid attenuates hyperhomocysteinemia-induced glomerular damage in rats. Microvasc. Res. 2013, 89, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Levi, A.; Cohen, E.; Levi, M.; Goldberg, E.; Garty, M.; Krause, I. Elevated serum homocysteine is a predictor of accelerated decline in renal function and chronic kidney disease: A historical prospective study. Eur. J. Inter. Med. 2014, 25, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Maka, N.; Makrakis, J.; Parkington, H.C.; Tare, M.; Morley, R.; Black, M.J. Vitamin D deficiency during pregnancy and lactation stimulates nephrogenesis in rat offspring. Pediatr. Nephrol. 2008, 23, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, F.A.; Ceciliano, T.C.; Aguila, M.B.; Mandarim-de-Lacerda, C.A. Maternal vitamin D deficiency delays glomerular maturity in F1 and F2 offspring. PLoS ONE 2012, 7, e41740. [Google Scholar] [CrossRef] [PubMed]
- Richard, A.; Rohrmann, S.; Quack Lotscher, K.C. Prevalence of vitamin D deficiency and its associations with skin color in pregnant women in the first trimester in a sample from Switzerland. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Aljohani, N.; Al-Attas, O.S.; Krishnaswamy, S.; Alfawaz, H.; Al-Ajlan, A.; Alokail, M.S. Dairy products consumption and serum 25-hydroxyvitamin D level in Saudi children and adults. Int. J. Clin. Exp. pathol. 2015, 8, 8480–8486. [Google Scholar] [PubMed]
- Al-Faris, N.A. High prevalence of vitamin D deficiency among pregnant Saudi women. Nutrients 2016, 8, 77. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Simhan, H.N.; Powers, R.W.; Frank, M.P.; Cooperstein, E.; Roberts, J.M. High prevalence of vitamin D insufficiency in black and white pregnant women residing in the northern United States and their neonates. J. Nutr. 2007, 137, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Sullivan, A.F.; Mansbach, J.M.; Camargo, C.A., Jr. Vitamin D insufficiency in pregnant and nonpregnant women of childbearing age in the United States. Am. J. Obstet. Gynecol. 2010, 202, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, C.C.; Evans, R.G.; Bertram, J.F.; Moritz, K.M. Effects of dietary protein restriction on nephron number in the mouse. Am. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R1768–R1774. [Google Scholar] [CrossRef] [PubMed]
- Nwagwu, M.O.; Cook, A.; Langley-Evans, S.C. Evidence of progressive deterioration of renal function in rats exposed to a maternal low-protein diet in utero. Br. J. Nutr. 2000, 83, 79–85. [Google Scholar] [PubMed]
- Vehaskari, V.M.; Aviles, D.H.; Manning, J. Prenatal programming of adult hypertension in the rat. Kidney Int. 2001, 59, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.L.; Weeks, D.A.; Rasch, R. Programming of adult blood pressure by maternal protein restriction: Role of nephrogenesis. Kidney Int. 2004, 65, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.; Yosypiv, I.V. Developmental programming of hypertension and kidney disease. Int. J. Nephrol. 2012, 2012, 760580. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, A.J.; Langley-Evans, S.C. Relationship between maternal nutrient intakes in early and late pregnancy and infants weight and proportions at birth: Prospective cohort study. J. R. Soc. Promot. Health 2003, 123, 210–216. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| References | Setting | Aims, Design | Sample size | Details of Intervention | Intervention Length | Offspring Age at Follow-Up (Years), Sex |
|---|---|---|---|---|---|---|
| Intervention Studies (n = 3) | ||||||
| Stewart et al. 2010 [26] | Rural, low-lying Sarlahi District of Nepal | Aim: To determine the effect of maternal Vitamin A or β-Carotene supplementation from pre-pregnancy through the post-partum period on childhood cardiovascular risk factors Design: Cluster-Randomized, double blind, placebo-controlled trial of vitamin A or β-Carotene supplementation. |
| Women were randomized by ward to receive weekly supplementation with: 1. Placebo 2. 7000 mg retinol equivalents of preformed vitamin A (23,300 IU retinyl palmitate) 3. 7000 mg retinol equivalents of β-Carotene (42 mg) | Before, during and after pregnancy | Mean ± SD: 10.4 ± 0.71 Males (Placebo: 51.4%, Vitamin A: 50.9%, β-Carotene: 51.1%) Females (Placebo: 48.6%, Vitamin A: 49.1%, β-Carotene: 48.9%) |
| Stewart et al. 2009 [25] | Rural, low-lying Sarlahi District of Nepal | Aim: To examine the impact of antenatal micronutrient supplementation on cardio-metabolic risk in the offspring at 6–8 years. Design: Community-based, cluster randomized, controlled trial of antenatal micronutrient supplementation. |
| Pregnant women were provided with daily supplements: 1. Vitamin A alone (Control) 2. Folic acid (400 mg) 3. Folic acid + iron (60mg) 4. Folic acid + iron + zinc (30 mg) 5. MMS containing folic acid, iron, zinc, and an additional 11 vitamins and minerals All supplements contained 1 mg retinol equivalents of vitamin A in the form of retinyl acetate. | From the time of enrolment (early pregnancy) through 3 months postpartum | Mean: 7.5 Numbers for each sex not specified. |
| Hawkesworth et al. 2013 [24] | International Centre for Diarrheal Disease Research, Bangladesh. | Aim: To assess the association between prenatal food and micronutrient supplementation and childhood blood pressure and kidney function Design: Follow up study of infants at 4.5 years from mothers who participated in the Maternal and Infant Nutrition Interventions, MatLab (MINIMat) Randomised Control Trial. |
| 2 separate nutritional interventions in pregnancy: 1. Food supplementation Food supplements (608kcal/day energy and 18 g/day of vegetable protein) were provided either: (a) early in pregnancy (~ 9 week gestation; early food) or (b) late in pregnancy (~ 20 week gestation; late food). 2. Micronutrient supplementation (a) 30mg of iron and 400μg of folate (Fe30F)/day (b) 60mg of iron and 400μg of folate (Fe60F)/day (c) 15 micronutrients ≥ the RDA, including 30mg iron and 400μg folate (MMS)/day | Early Food: 21 weeks (around 9 week of gestation to week 30 gestation) Late Food: 10 weeks (around 20 week of gestation to week 30 gestation) | Mean ± SD: 4.6 ± 0.1 Male (50.5%) Female (49.5%) |
| References | Setting | Aims, Design | Inclusion/Exclusion Criteria | Study Population | Offspring Age at Follow-Up (Years), Sex |
|---|---|---|---|---|---|
| Observational Studies (n = 7) | |||||
| Goodyer et al. 2007 [32] | St. John’s Medical College Hospital, Bangalore, India and Royal Victoria Hospital, Montreal, Canada | Aim: To determine the prevalence of maternal vitamin A deficiency and its relationship to offspring nephron endowment from normal pregnant women from Bangalore (India) and Montreal (Canada) Design: Prospective cohort. | Inclusion: Healthy women with uncomplicated pregnancies Exclusion: Mothers on vitamin A supplements, high risk and medically complicated pregnancies, twin, diabetic and growth restricted pregnancies, significant fetal structural or genetic abnormalities, fetuses with significant pyelectasis or renal anomalies and pregnancies delivered <32 weeks of gestation. | Montreal: 48 Bangalore: 46 | 2–6 weeks of age Numbers for each sex not specified. |
| El-Khashab et al. 2013 [33] | Gynecology and Obstetrics Hospital, Ain Shams University, Cairo, Egypt | Aim: To assess the Vitamin A status of a cohort of Egyptian pregnant women and their newborns and to determine the potential effect of maternal Vitamin A deficiency during pregnancy on the neonatal kidney size. Design: Cross-sectional. | Inclusion: Healthy mothers, aged 19–39 years, with singleton uncomplicated pregnancy. Full term, healthy offspring with no morbidities. Exclusion: 1. Mothers with a history of exposure to teratogens, high-risk and complicated pregnancies, multiple gestations, antenatal diagnosis of intrauterine growth restriction, renal anomalies, fetal structural abnormalities, on vitamin A supplementation. 2. Offspring born <37 weeks, birth weight <2.5 kg, birth asphyxia, congenital anomalies or dysmorphic features. | Vitamin A deficiency: serum retinol concentration ≤0.7 umol/L (n = 16) Vitamin A sufficient: serum retinol concentration >0.7 umol/L (n = 64) | ≤3 days Numbers for each sex not specified. |
| Miliku, K. et al. 2017 [31] | Generation R study: Population-based prospective cohort study from fetal life onward in Rotterdam, Netherlands | Aim: To examine the associations of folate, vitamin B12, and homocysteine concentrations during first trimester of pregnancy and at birth with kidney outcomes in school-aged children Design: Prospective cohort study. | Inclusion: Singleton live-born children from mothers with nutritional data and with at least one kidney measurement. | 4226 mothers-child pairs Maternal venous blood samples were collected in early-pregnancy (median gestational age 13.2 weeks, range 12.2–14.8 weeks). Deficient folate <7 nmol/L Normal folate ≥7 nmol/L | Median (95% range): 6.0 (5.9–6.3) Deficient folate Male (51.3%) Female (48.7%) Normal folate Male (49.9%) Female (50.1%) |
| Miliku, K. et al. 2016 [30] | Generation R study: Population-based prospective cohort study from fetal life onward in Rotterdam, Netherlands | Aim: To examine the associations of circulating vitamin 25-hydroxyvitamin D (25(OH)D) levels during mid-pregnancy and in cord blood at birth with childhood kidney outcomes Design: Prospective cohort study. | Inclusion: Singletons with available information on maternal vitamin D blood levels during mid-pregnancy and have measurements on kidney ultrasound, creatinine and cystatin C from blood, and albumin and creatinine from urine samples at the age of 6 years. Exclusion: Children with evidence of congenital kidney abnormalities on ultrasound examination or with abnormally high urinary albumin–creatinine ratio | 4212 mothers-child pairs Maternal venous blood samples were collected in mid-pregnancy (median gestational age 20.3 weeks, range 18.5–23.3 weeks). Total 25(OH)D was reported as the sum of 25(OH)D2 and 25(OH)D3 measured in plasma. Maternal vitamin D status: severely deficient <25.0 nmol/L deficient 25–49.9 nmol/L Sufficient 50.0–74.9 nmol/L Optimal ⩾75.0 nmol/L | Median (95% range): 6.0 (5.6–7.4) Male (49.6%) Female (50.4%) |
| Huang et al. 2014 [27] | Chinese famine of 1959–1961 | Aim: To describe the long term effects of exposure to the Chinese famine of 1959–1961 during gestation and early postnatal life on the levels of proteinuria in adulthood Design: Retrospective cohort. | Inclusion: Restricted study to women born from 1957 to 1965 and living in Hebei, Zhejiang and Jiangsu provinces. Exclusion: 18.3% of rural sample, 12.9% of urban sample due to missing data on outcome variable. Famine (<1500 calories daily per capita) | Rural: n = 51,978 (i) Pre-famine (1957–1958): n = 2050 (ii) Famine (1959–1961): n = 6396 (iii) Post-famine (1962–1963): n = 24,739 (iv) Unexposed group (1964–1965): n = 18,793 Urban: n = 4563 (i) Pre-famine (1957–1958): n = 241 (ii) Famine (1959–1961): n = 518 (iii) Post-famine (1962–1963): n = 1594 (iv) Unexposed group (1964–1965): n = 2210 | Approx. 30 All female only |
| Painter et al. 2005 [28] | The Dutch Famine Birth Cohort study, the Netherlands | Aim: To describe the long-term effects of prenatal exposure to famine on microalbuminuria and renal function Design: Retrospective cohort. | Inclusion: Exposed: Infants born in 1945 and were exposed to famine in utero. Unexposed: Infants born before or conceived after the famine. Famine <1000 calories daily | 288 (40%) of the 724 participants studied had been exposed to famine in utero. Exposed (n = 288): 3 groups; 16-week periods Early gestation: n = 65 Mid gestation: n = 104 Late gestation: n = 119 Unexposed (n = 506): Born before: n = 207 Conceived after: n = 229 | Mean (95% range): 50 (48–53) Male Early: 46% Mid: 42% Late: 47% Female Early: 54% Mid: 58% Late: 53% |
| Miliku, K. et al. 2015 [29] | Generation R study: Population-based prospective cohort study from fetal life onward in Rotterdam, Netherlands | Aim: To assess the associations between first-trimester maternal total, animal and vegetable protein intake during pregnancy and offspring kidney outcomes at 6 years Design: Prospective cohort study. | Inclusion: 1. Living in the study area at delivery 2. Delivery between April 2002 and January 2006 Exclusion: 1. Twin pregnancies 2. Loss to follow-up 3. Withdrawal of consent | 3650 mother-child pairs (78%) of the 4658 children with maternal nutritional data available and who attended follow-up at age 6 with successful kidney outcome measures | Median (95% range): 6.1 (5.6–7.3) Male (49.9%) Female (50.1%) |
| References | Offspring Kidney-Related Outcomes Reported | Conclusion, Limitations & Recommendations | ||
|---|---|---|---|---|
| Measures | Significant difference between Groups | Results | ||
| Intervention Studies (n = 3) | ||||
| Stewart et al. 2010 [26] | BP (mmHg) | No significant difference between vitamin A or β-Carotene groups and placebo group (in crude model or after adjustment for child’s age or gender) | Adjusted difference (Mean (S.D.)) Systolic BP Vitamin A: −0.19 (−0.94, 0.56) β-Carotene: −0.21 (−1.00, 0.58) Diastolic BP Vitamin A: −0.03 (−0.90, 0.83) β-Carotene: −0.19 (−1.07, 0.70) | Limitations 1. High percentage of missing data for some biochemical measures reduced power to detect differences between groups. 2. The prevalence of hypertension and micro-albuminuria was only 5%, reflecting a low disease risk and power to detect risk factors. 3. Observations only applicable to rural population Strengths 1. Presents data from a large cohort of more than 13,000 children 2. More than half of all women consumed >80% of their intended supplements 3. A high rate of follow-up was achieved, with no differential losses and a high degree of comparability across groups. 4. Study design minimized the risk of confounders Conclusion No evidence of an overall effect of maternal supplementation with vitamin A or β-Carotene on BP or risk of microalbuminuria. |
| Risk of hypertension | No overall difference between supplement groups | Adjusted OR (95%) Vitamin A: 1.14 (0.72, 1.79) β-Carotene: 0.81 (0.46, 1.44) | ||
| Risk of microalbuminuria (≥30 microalbumin/creatinine mg/g) | No overall difference between supplement groups | Adjusted OR (95%) Vitamin A: (0.40, 3.71) β-Carotene: 0.68 (0.20, 2.30) | ||
| Stewart et al. 2009 [25] | BP (mmHg) | No difference between intervention groups and control for both systolic and diastolic BP | - | Limitations High numbers of missing data, decreased the sample size and power to find significant differences among treatment groups. Strengths This study provides unique data for the effects of micronutrient supplementation during pregnancy on risk factors for chronic disease from a RCT with high compliance and a high rate of follow-up. Conclusion 1. No impact of antenatal MMS on BP. 2. 36% reduction in the risk of microalbuminuria when all supplementation groups containing folic acid were compared with the control, suggesting a protective role of folic acid on kidney function. |
| Risk of microalbuminuria (≥3.4 albumin/creatinine mg/mmol) | Significant reduction among mothers in the folic acid and folic acid + iron + zinc groups compared with the control | OR (95% CI) Folic acid:0.56 (0.33, 0.93) Folic acid + iron: 0.77 (0.49, 1.22) Folic acid + iron + zinc: 0.53 (0.32, 0.89) Multiple micronutrient: 0.70 (0.44, 1.11) | ||
| Hawkesworth et al. 2013 [24] | Diastolic BP (mmHg) | Lower in early food than late food (p = 0.01) | Mean difference of 0.74 (95% CI: 0.18, 1.30) | Limitations 1. Women only randomly assigned to encouragement to food supplementation rather than provided with food supplementation itself. 2. The study lacked control arms and a MMS arm that also contained iron. 3. Age of offspring may be too young to see differences in renal or cardiovascular outcomes. Strengths Large sample size, good retention of participants Conclusion Overall there was limited evidence for long-lasting impacts of pregnancy supplementation on offspring blood pressure or markers of kidney function. |
| Higher in MMS compared with iron and folate (p = 0.03) | Mean difference of 0.65 (95% CI: 0.06, 1.24) | |||
| No difference between high and low iron intervention | - | |||
| Systolic BP (mmHg) | No effect of food or nutritional supplementation | - | ||
| Kidney Volume (cm3/m2) | No effect of food or nutritional supplementation | - | ||
| eGFR from plasma Cystatin C (ml/(min × 1.73 m2) | No difference between early or late food | - | ||
| Higher in offspring whose mothers received 60mg of iron during pregnancy vs. 30mg (p = 0.04) | Mean difference of 4.98 (95% CI: 0.30, 9.67) | |||
| References | Offspring Kidney-Related Outcome Reported | Conclusion, Limitations & Recommendations | ||
|---|---|---|---|---|
| Measures | Significance of Results | Results | ||
| Observational Studies (n = 7) | ||||
| Goodyer et al. 2007 [32] | Mean combined renal volume (ml) at 1 month | Significantly smaller in Bangalore (VAD) than that in Montreal (VAS) (p < 0.001) | 22.3 ± 7.0 vs. 40.1 ± 11.0 | Conclusion Vitamin A deficiency has an additional effect on nephron number as reflected in kidney volume. Recommendations 1. Future study should target the assessment of renal volume during the immediate newborn period prior to discharge from hospital. 2. Cord cystatin C measurements might be used to estimate fetal renal function mass. |
| Mean combined renal volume/Body surface area (ml/m2) | Significantly lower in Bangalore (VAD) than that in Montreal (VAS) (p < 0.01) | 113.7 ± 33.3 vs. 184.2 ± 43.6 | ||
| Mean maternal retinol + renal size at 1 month in Bangalore newborns | No significant correlation (p > 0.4) | r = 0.159 (n = 25 only) | ||
| El-Khashab et al. 2013 [33] | Mean longitudinal axis (cm) | Significantly lower in both kidneys of newborns delivered to VAD mothers compared with the newborns delivered to VAS mothers (Right: p = 0.005; Left: p = 0.008) | Right Kidney VAD: 3.12 ± 0.96 VAS: 3.86 ± 0.51 Left Kidney VAD: 3.25 ± 1.11 VAS: 3.92 ± 0.41 | Conclusion Maternal VAD during pregnancy may decrease the renal size in the infant at birth. Limitation 1. Did not include the follow-up of renal size and the effect on renal functions of the infants 2. Small sample size Recommendations Longitudinal studies on larger scale needed to validate the results and to explore the effect on renal functions |
| Mean transverse axis (cm) | Significantly lower in both kidneys of newborns delivered to VAD mothers compared with the newborns delivered to VAS mothers (Right: p = 0.008; Left: p = 0.05) | Right Kidney VAD: 1.57 ± 0.44 VAS: 1.94 ± 0.31 Left Kidney VAD: 1.63 ± 0.44 VAS: 1.92 ± 0.33 | ||
| Mean renal volume (cm3) | Significantly lower in both kidneys of newborns delivered to VAD mothers compared with the newborns delivered to VAS mothers (Right: p = 0.002; Left: p = 0.002) | Right Kidney VAD: 7.42 ± 2.45 VAS: 9.5 ± 2.31 Left Kidney VAD: 7.95 ± 1.36 VAS: 9.96 ± 2.41 | ||
| Combined renal volume (cm3) | Significantly lower in newborns delivered to VAD mothers compared with the newborns delivered to VAS mothers (p = 0.001) | VAD: 15.95 ± 2.47 VAS: 19.01 ± 3.49 | ||
| Combined renal volume and maternal serum retinol concentrations | Significant positive correlation (p = 0.001) | r = 0.48 | ||
| Miliku, K. et al. 2017 [31] | Combined kidney volume (cm3) | Higher maternal folate concentration was associated with a larger childhood combined kidney volume. (p < 0.01) | Difference: 1.16 (95% CI: 0.47, 1.85) per 1 SD in folate | Limitations Results apply to a relatively healthy sample of pregnant women and children, generalizability of results to other populations should be interpreted with caution. Strengths 1. The largest prospective population-based cohort study examining the associations of folate, vitamin B12 and homocysteine concentrations during fetal life with childhood kidney outcomes. 2. Detailed measurements on kidney outcomes were obtained. Conclusion 1. Maternal higher folate and lower homocysteine concentrations are associated with larger childhood combined kidney volume. 2. Maternal higher vitamin B12 and lower homocysteine concentrations were associated with higher childhood eGFRcystC. 3. No association between folic acid supplement intake and kidney outcomes. 4. Effect sizes presented are small. Recommendations These findings should be considered as hypothesis generating and require further replication. Additional follow-up studies are warranted to examine the long term consequences for the risk of kidney diseases in later life. |
| Maternal vitamin B12 concentration was not associated with childhood combined kidney volume. | Difference: 0.47 (95% CI: −0.17, 1.11) per 1 SD in vitamin B12 | |||
| Higher maternal homocysteine concentration was associated with a smaller childhood combined kidney volume. (p < 0.01) | Difference: −1.44 (95% CI: −2.09, −0.79) per 1 SD in homocysteine | |||
| No association between maternal folic acid supplement intake during pregnancy and childhood combined kidney volume. | - | |||
| eGFRcreat (ml/min per 1.73 m2) | Maternal folate, vitamin B12 and homocysteine concentration were not associated with childhood eGFRcreat. | Folate Difference: 0.01 (95% CI: −0.65, 0.67) per 1 SD in folate Vitamin B12 Difference: 0.20 (95% CI: −0.43, 0.83) per 1 SD in vitamin B12 Homocysteine Difference: −0.55 (95% CI: −1.15, 0.05) per 1 SD in homocysteine | ||
| No association between maternal folic acid supplements intake during pregnancy and childhood eGFRcreat. | - | |||
| eGFRcystC (ml/min per 1.73 m2) | Maternal folate concentration was not associated with childhood eGFRcystC. | Difference: −0.03 (95% CI: −0.63, 0.58) per 1 SD in folate | ||
| Higher maternal vitamin B12 concentration was associated with a higher childhood eGFRcystC. (p < 0.01) | Difference: 1.00 (95% CI: 0.43, 1.57) per 1 SD in vitamin B12 | |||
| Higher maternal homocysteine concentration was associated with a lower childhood eGFRcystC. (p < 0.05) | Difference: −0.57 (95% CI: −1.13, −0.02) per 1 SD in homocysteine | |||
| No association between maternal folic acid supplement intake during pregnancy and childhood eGFRcystC. | - | |||
| Microalbuminuria | Maternal folate, vitamin B12 and homocysteine concentration were not associated with risk of microalbuminuria. | Folate OR 0.97 (95% CI: 0.85, 1.10) per 1 SD in folate Vitamin B12 OR 1.06 (95% CI: 0.95, 1.19) per 1 SD in vitamin B12 Homocysteine OR 1.08 (95% CI: 0.98, 1.20) per 1 SD in homocysteine | ||
| No association between maternal folic acid supplement intake during pregnancy and risk of microalbuminuria. | - | |||
| Miliku, K. et al. 2016 [30] | Combined kidney volume (cm3) | Larger in children of mothers who were vitamin D deficient during pregnancy compared with children of mothers who had optimal 25(OH)D levels. (p < 0.05) | Difference: 1.92 (95% CI: 0.11, 3.74) | Limitations 1. Mothers of the children who were lost to follow-up had on average lower 25(OH)D levels and were on average lower educated, suggesting that the study population had a bias toward a more healthy population. 2. Same cut-offs of 25(OH)D were used for pregnant woman as the documented levels for general population 3. Childhood dietary data at the age of 6 years were not available. 4. Microalbuminuria was evaluated using urine albumin–creatinine ratio from a random urine sample, instead of first-morning void samples. 5. Residual confounding by other lifestyle factors might be present. Strengths 1. Prospective design from fetal life onward within a large population-based cohort. 2. 25(OH)D levels were used, which are the best and the most widely used indicator of vitamin D status. 3. Well-established methods were used to measure kidney size and function. Conclusion 1. Mothers who were 25(OH)D deficient had children with larger combined kidney volumes. 2. Lower maternal 25(OH)D levels were associated with an increased eGFRcreat in school-age children. Recommendations Further studies are needed to replicate the observations, examine the underlying mechanisms and to identify the long-term clinical consequences. |
| eGFRcreat (ml/min per 1.73 m2) | Maternal 25(OH)D levels were inversely associated with lower childhood eGFRcreat. (p = 0.02) | Difference: −0.94 (95% CI: −1.73, −0.15) per 1 SD in 25(OH)D | ||
| eGFRcystC (ml/min per 1.73 m2) | Maternal 25(OH)D levels were not associated with eGFRcystC. | Difference: − 0.29 (95% CI: −0.99, 0.41) per 1 SD in 25(OH)D | ||
| Microalbuminuria | Maternal 25(OH)D levels were not associated with risk of microalbuminuria. | OR: 0.93 (95% CI: 0.80, 1.09) per 1 SD in 25(OH)D | ||
| Creatinine levels from blood (μmol/L) | Maternal 25(OH)D levels were associated with higher childhood creatinine levels. (p < 0.05) | 0.32 (95% CI: 0.07, 0.58) per 1 SD in 25(OH)D | ||
| Cystatin C levels from blood (μg/L) | Maternal 25(OH)D levels were not associated with childhood cystatin C levels. | 2.32 (95% CI: −1.55, 6.19) per 1 SD in 25(OH)D | ||
| Huang et al. 2014 [27] | Proteinuria | Rural: Famine exposure was associated with 54% higher odds of having a higher concentration of protein in the urine compared with the unexposed group (p = 0.029) | OR: 1.54 (95% CI: 1.04, 2.28) | Limitations 1. Dipstick test of urine specimens is less sensitive and accurate than other methods. 2. Assumption that women were living in the same country as when they were born. 3. Famine cohort may represent a more selective and robust population compared with post-famine cohorts. May result in underestimation of the effects of famine exposure on adult health outcomes. 4. The long and imprecise duration of the Chinese famine of 1959–61 did not permit isolation of prenatal and postnatal exposures. Strengths First study to examine the effects of the Chinese famine of 1959–1961 on renal function. Conclusion Exposure to the Chinese famine of 1959–1961 during gestation was associated with higher level of proteinuria three decades later after the exposure in rural residents, but the effect size was small. |
| Rural: No association between famine exposure and the concentration of protein in urine for the pre-famine group (p = 0.380) | OR: 1.29 (95% CI: 0.73, 2.26) | |||
| Rural: No significant difference in the levels of proteinuria between post-famine and unexposed group (p = 0.051) | OR: 1.26 (95% CI: 0.99, 1.59) | |||
| Urban: No significant difference in the occurrence of proteinuria in the pre-famine, famine and post-famine group when compared with the unexposed group | - | |||
| Painter et al. 2005 [28] | Prevalence of Microalbuminuria | Significantly higher in those who were exposed to famine in mid gestation than in people who were not exposed prenatally (p = 0.05) | 12% vs. 7% | Limitations 1. Conclusions are based on non-invasive outcome measures only. 2. Small number of individuals in each of the exposure groups limited the ability to make firm statements about the precise timing of the effects 3. Small sample size. Conclusion Exposure to famine in mid-gestation is linked to a 3.2-fold increase in occurrence of microalbuminuria in adulthood and a 10% decrease in creatinine clearance. |
| Not significantly increased in early (p = 0.3) or late gestation (p = 0.8) | - | |||
| Mean creatinine clearance (mL/min) | Decreased in those exposed to famine in mid-gestation compared to those conceived after (p < 0.01) | Decrease of 11.9 (95% CI: 4.0, 19.8) | ||
| Those conceived after famine had the highest mean clearance | - | |||
| A gender- and age-adjusted decrease in those born before the famine compared to those conceived after (p < 0.01) | Decrease of 16.4 (95% CI: 7.4, 25.4) | |||
| Miliku, K. et al. 2015 [29] | eGFRcreat (mL × min−1 × 1.73 m−2) | Higher with higher first trimester maternal total protein intake (p < 0.05) | Difference: 0.06/g total protein intake (95% CI: 0.01, 0.12) | Limitations FFQ validated only in Dutch elderly women (55–75 years old), not specifically in pregnancy. Strengths Prospective design from fetal life onward within a large population-based cohort Conclusion 1. A higher maternal intake of total and vegetable protein, but not animal protein, during the first trimester of pregnancy is associated with higher eGFRcreat but not with kidney size, eGFRcyst C, or microalbuminuria in school-aged children. 2. First-trimester maternal protein intake was positively associated with eGFRcreat in 6 year-old children. 3. The associations with eGFR were stronger for vegetable than for animal protein intake during pregnancy. 4. Child protein intake at the age of 1 year does not affect the association between maternal protein intake and childhood kidney health. Recommendations Follow-up studies are needed to explore whether protein intake in pregnancy affects the risk of kidney diseases in adulthood. Further studies are needed to investigate the underlying mechanisms. |
| Strongly associated with first trimester maternal vegetable protein intake (p < 0.05) | Difference: 0.22/g vegetable protein intake (95% CI: 0.10, 0.35) | |||
| Not significantly associated with first trimester maternal animal protein intake | - | |||
| eGFRcystC (mL × min−1 × 1.73 m−2) | Not associated with first trimester maternal total protein intake | - | ||
| Kidney volume (cm3) | Not associated with first trimester maternal total protein intake | - | ||
| Microalbuminuria | Not associated with first trimester maternal total protein intake | - | ||
| Serum creatinine (umol/L) | First trimester maternal total protein intake associated with lower concentrations of creatinine | −0.02/g total protein intake (95% CI: −0.04, −0.01) | ||
| First trimester maternal vegetable protein intake associated with lower concentrations of creatinine | −0.07/g vegetable protein intake (95% CI: −0.11, −0.03) | |||
| Serum cystatin C (ug/L) | Not associated with first trimester maternal total protein intake | - | ||
| Not associated with first trimester maternal vegetable protein intake | - | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.Q.; Collins, C.E.; Gordon, A.; Rae, K.M.; Pringle, K.G. The Relationship between Maternal Nutrition during Pregnancy and Offspring Kidney Structure and Function in Humans: A Systematic Review. Nutrients 2018, 10, 241. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020241
Lee YQ, Collins CE, Gordon A, Rae KM, Pringle KG. The Relationship between Maternal Nutrition during Pregnancy and Offspring Kidney Structure and Function in Humans: A Systematic Review. Nutrients. 2018; 10(2):241. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020241
Chicago/Turabian StyleLee, Yu Qi, Clare E. Collins, Adrienne Gordon, Kym M. Rae, and Kirsty G. Pringle. 2018. "The Relationship between Maternal Nutrition during Pregnancy and Offspring Kidney Structure and Function in Humans: A Systematic Review" Nutrients 10, no. 2: 241. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020241