Diet-Induced Weight Loss Has No Effect on Psychological Stress in Overweight and Obese Adults: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
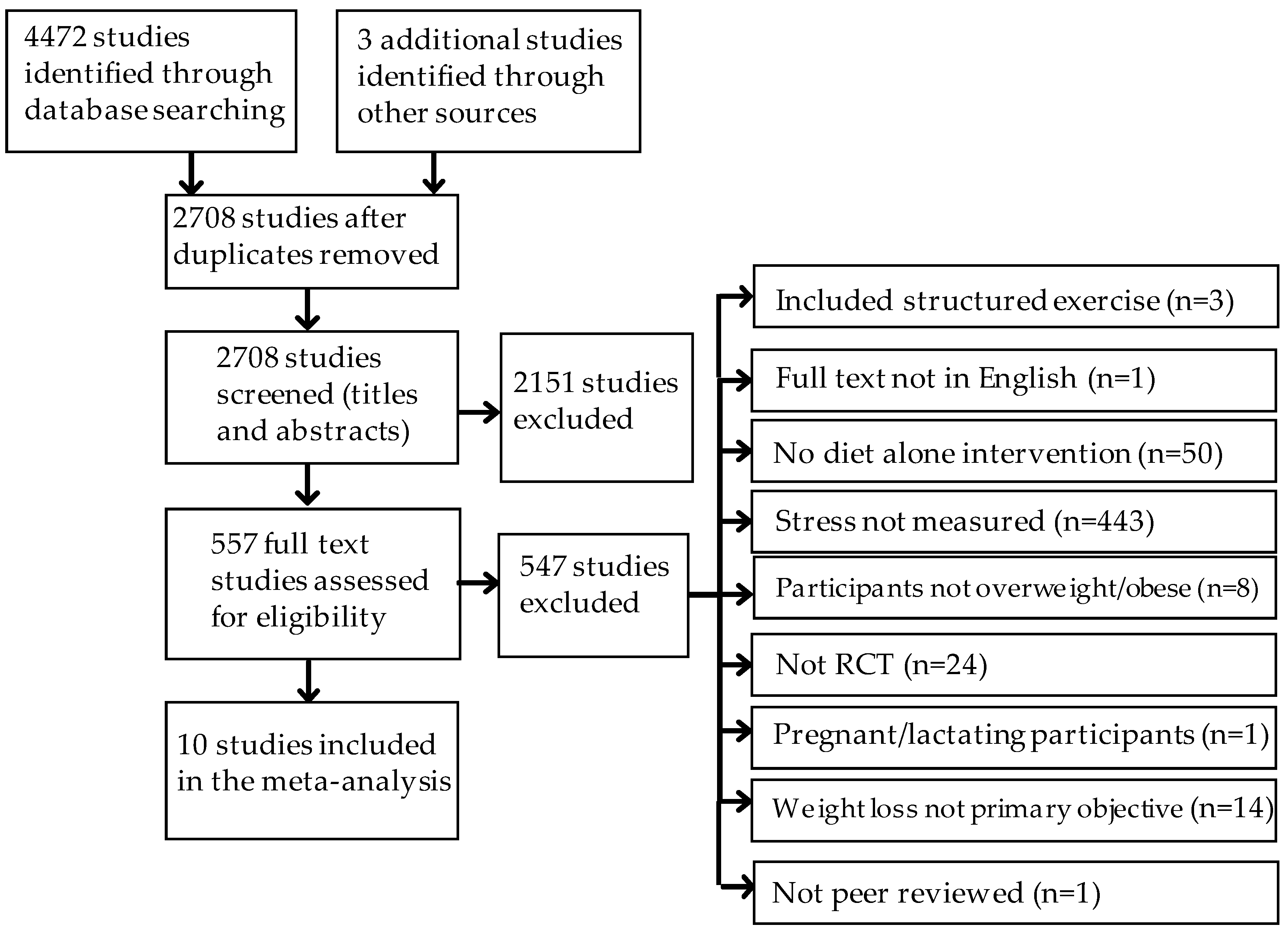
2.3. Search Results and Selection of Studies
2.4. Risk for Bias
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of the Selected Studies
3.2. Risk for Bias Assessment Summary
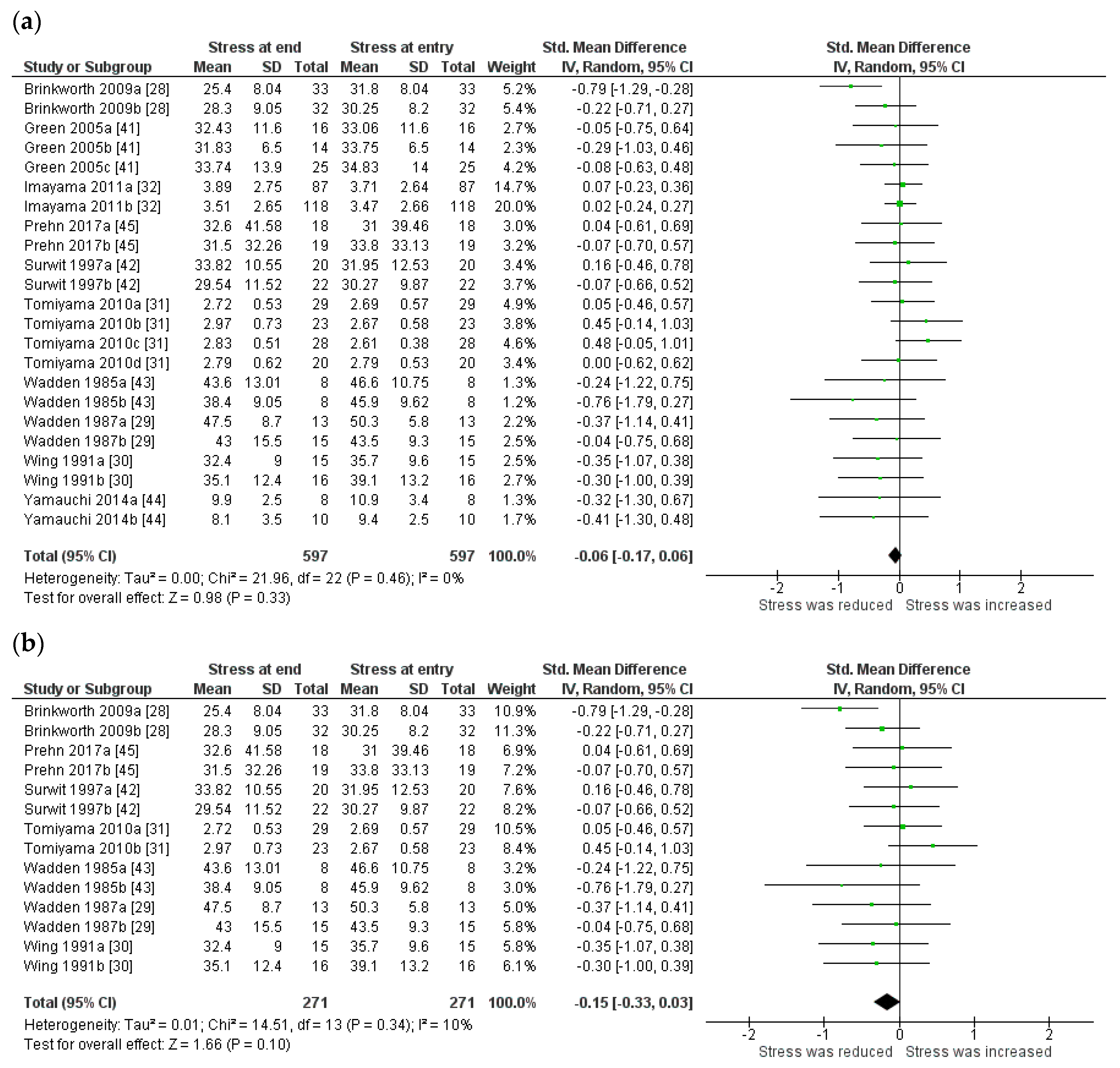
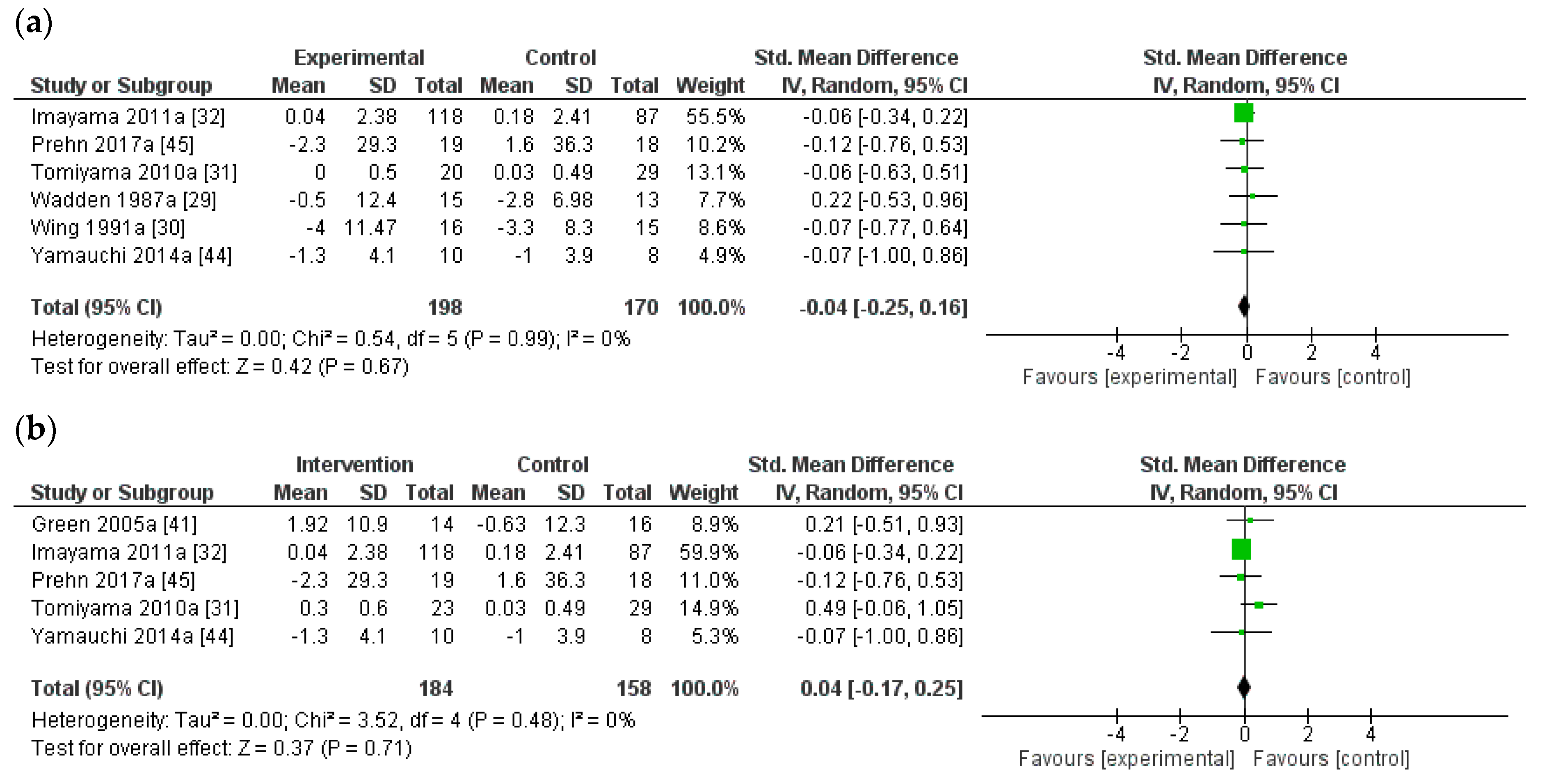
3.3. Effect of Weight Loss on Stress
3.4. Test for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- World Health Organisation. Global Strategy on Diet, Physical Activity and Health; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organisation. Obesity: Preventing and Managing the Global Epidemic; Technical Report Series 894; World Health Organisation: Geneva, Switzerland, 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Krantz, D.S.; McCeney, M.K. Effects of psychological and social factors on organic disease: A critical assessment of research on coronary heart disease. Annu. Rev. Clin. Psychol. 2002, 53, 341–369. [Google Scholar] [CrossRef] [PubMed]
- Kruk, J.; Aboul-Enein, H.Y. Psychological stress and the risk of breast cancer: A case–control study. Cancer Detect. Prev. 2004, 28, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Hammen, C. Stress and Depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Sarason, I.G.; Strelau, J.; Brebner, J.M. Stress and Anxiety; Taylor and Francis: Hoboken, NY, USA, 2014. [Google Scholar]
- Rod, N.H.; Gronbaek, M.; Schnohr, P.; Prescott, E.; Kristensen, T.S. Perceived stress as a risk factor for changes in health behaviour and cardiac risk profile: A longitudinal study. J. Intern. Med. 2009, 266, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, S.; Stubbs, B.; Ward, P.B.; Steel, Z.; Lederman, O.; Vancampfort, D. The prevalence and risk of metabolic syndrome and its components among people with posttraumatic stress disorder: A systematic review and meta-analysis. Metabolism 2015, 64, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, N.; Gyntelberg, F.; Faber, J. The appraisal of chronic stress and the development of the metabolic syndrome: A systematic review of prospective cohort studies. Endocr. Connect. 2014, 3, R55–R80. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, D.; Gamborg, M.; Gyntelberg, F.; Heitmann, B.L. Psychological workload is associated with weight gain between 1993 and 1999: Analyses based on the Danish Nurse Cohort Study. Int. J. Obes. 2004, 28, 1072–1081. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, D.; Gyntelberg, F.; Heitmann, B.L. Psychological workload and body weight: Is there an association? A review of the literature. Occup. Med. 2004, 54, 35–41. [Google Scholar] [CrossRef]
- Rippe, J.M.; Crossley, S.; Ringer, R. Obesity as a chronic disease: Modern medical and lifestyle management. J. Am. Diet. Assoc. 1998, 98, S9–S15. [Google Scholar] [CrossRef]
- Baune, B.; Aljeesh, Y. The association of psychological stress and health related quality of life among patients with stroke and hypertension in Gaza Strip. Ann. Gen. Psychiatry 2006, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, H.J.; Cole, B.M.; Geliebter, A. The benefits of body weight loss on health-related quality of life. J. Chin. Med. Assoc. 2011, 74, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kaukua, J.; Pekkarinen, T.; Sane, T.; Mustajoki, P. Health-related quality of life in obese outpatients losing weight with very-low-energy diet and behaviour modification: A 2-y follow-up study. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, K.R.; Barofsky, I.; Andersen, R.E.; Bartlett, S.J.; Wiersema, L.; Cheskin, L.J.; Franckowiak, S.C. Impact of weight loss on health-related quality of life. Qual. Life Res. 1999, 8, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Blaine, B.E.; Rodman, J.; Newman, J.M. Weight loss treatment and psychological well-being: A review and meta-analysis. J. Health Psychol. 2007, 12, 66–82. [Google Scholar] [CrossRef] [PubMed]
- Buffenstein, R.; Karklin, A.; Driver, H.S. Beneficial physiological and performance responses to a month of restricted energy intake in healthy overweight women. Physiol. Behav. 2000, 68, 439–444. [Google Scholar] [CrossRef]
- Degoutte, F.; Jouanel, P.; Begue, R.J.; Colombier, M.; Lac, G.; Pequignot, J.M.; Filaire, E. Food restriction, performance, biochemical, psychological, and endocrine changes in judo athletes. Int. J. Sports Med. 2006, 27, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Figueroa-Fankhanel, F. Measurement of stress. Psychiatr. Clin. N. Am. 2014, 37, 455–487. [Google Scholar] [CrossRef] [PubMed]
- Glinski, J.; Wetzler, S.; Goodman, E. The psychology of gastric bypass surgery. Obes. Surg. 2001, 11, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Clifton, P.M.; Noakes, M.; Brinkworth, G.D. Weight loss on a structured hypocaloric diet with or without exercise improves emotional distress and quality of life in overweight and obese patients with type 2 diabetes. J. Diabetes Investig. 2014, 5, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Brinkworth, G.D.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Wilson, C.J. Long-term effects of a very low-carbohydrate diet and a low-fat diet on mood and cognitive function. Arch. Intern. Med. 2009, 169, 1873–1880. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Stunkard, A.J.; Day, S.C.; Gould, R.A.; Rubin, C.J. Less food, less hunger: Reports of appetite and symptoms in a controlled study of a protein-sparing modified fast. Int. J. Obes. 1987, 11, 239–249. [Google Scholar] [PubMed]
- Wing, R.R.; Marcus, M.D.; Blair, E.H.; Burton, L.R. Psychological responses of obese type II diabetic subjects to very-low-calorie diet. Diabetes Care 1991, 14, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, A.J.; Mann, T.; Vinas, D.; Hunger, J.M.; Dejager, J.; Taylor, S.E. Low calorie dieting increases cortisol. Psychosom. Med. 2010, 72, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Imayama, I.; Alfano, C.M.; Kong, A.; Foster-Schubert, K.E.; Bain, C.E.; Xiao, L.; Duggan, C.; Wang, C.Y.; Campbell, K.L.; Blackburn, G.L.; et al. Dietary weight loss and exercise interventions effects on quality of life in overweight/obese postmenopausal women: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Higgins, J.P.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Rothsein, H.; Sutton, A.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; John Wiley and Sons: Chichester, UK, 2005. [Google Scholar]
- Spielberger, G.; Gorush, R.; Lusshene, R. The State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alta, CA, USA, 1970. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Shacham, S. A shortened version of the Profile of Mood States. J. Personal. Assess. 1983, 47, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Baker, F.; Denniston, M.; Zabora, J.; Polland, A.; Dudley, W.N. A POMS short form for cancer patients: Psychometric and structural evaluation. Psychooncology 2002, 11, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Green, M.W.; Elliman, N.A.; Kretsch, M.J. Weight loss strategies, stress, and cognitive function: Supervised versus unsupervised dieting. Psychoneuroendocrinology 2005, 30, 908–918. [Google Scholar] [CrossRef] [PubMed]
- Surwit, R.S.; Feinglos, M.N.; McCaskill, C.C.; Clay, S.L.; Babyak, M.A.; Brownlow, B.S.; Plaisted, C.S.; Lin, P.H. Metabolic and behavioral effects of a high-sucrose diet during weight loss. Am. J. Clin. Nutr. 1997, 65, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Stunkard, A.J.; Brownell, K.D.; Day, S.C. A comparison of two very-low-calorie diets: Protein-sparing-modified fast versus protein-formula-liquid diet. Am. J. Clin. Nutr. 1985, 41, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, K.; Katayama, T.; Yamauchi, T.; Kotani, K.; Tsuzaki, K.; Takahashi, K.; Sakane, N. Efficacy of a 3-month lifestyle intervention program using a Japanese-style healthy plate on body weight in overweight and obese diabetic Japanese subjects: A randomized controlled trial. Nutr. J. 2014, 13, 108. [Google Scholar] [CrossRef] [PubMed]
- Prehn, K.; Jumpertz von Schwartzenberg, R.; Mai, K.; Zeitz, U.; Witte, A.V.; Hampel, D.; Szela, A.M.; Fabian, S.; Grittner, U.; Spranger, J.; et al. Caloric Restriction in Older Adults-Differential Effects of Weight Loss and Reduced Weight on Brain Structure and Function. Cereb. Cortex 2017, 27, 1765–1778. [Google Scholar] [CrossRef] [PubMed]
- Eyres, S.L.; Turner, A.I.; Nowson, C.A.; Torres, S.J. Does diet-induced weight change effect anxiety in overweight and obese adults? Nutrition 2014, 30, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Laederach-Hofmann, K.; Kupferschmid, S.; Mussgay, L. Links between body mass index, total body fat, cholesterol, high-density lipoprotein, and insulin sensitivity in patients with obesity related to depression, anger, and anxiety. Int. J. Eat. Disord. 2002, 32, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Steen, S.N.; Wingate, B.J.; Foster, G.D. Psychosocial consequences of weight reduction: How much weight loss is enough? Am. J. Clin. Nutr. 1996, 63, 461S–465S. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Participants | Study Design | Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|
| Study | N | Age (mean ± SD) or range (years) | Baseline BMI (kg/m2) | Intervention | Stress measure | Duration | Weight change | Stress change |
| Brinkworth et al. 2009 [28] | 65 men and women with abdominal obesity # | 50.0 ± 8.2 | 33.7 ± 4.1 | IG: Isocaloric conventional high carbohydrate low-fat diet CG: Energy restricted very-low carbohydrate, high-fat diet | POMS STAI-ST | 12 months | IG: −13.7 kg * CG: −13.7 kg * | IG: improvement in STAI-ST vs CG p < 0.05 between groups |
| Green et al. 2005 [41] | 55 overweight women | 20–45 | IG: 29.3 ± 6.5 CG1: 28.2 ± 4.1 CG2: 26.9 ± 6.5 | IG: Hypocaloric supported diet CG1: Hypocaloric unsupported diet CG2: Usual diet | STAI-S | 8 weeks | IG: −2.7 kg * CG1: −2.2 kg * CG2: −0.05 kg * | IG: no change CG1: no change |
| Imayama et al. 2011 [32] | 205 overweight and obese women | IG: 58.1 ± 5.9 CG: 57.4 ± 4.4 | IG: 31.0 ± 3.9 CG: 30.7 ± 3.9 | IG: Reduced calorie dietary weight loss (1200–2000 kcal/day) CG: Usual diet | Perceived stress scale | 12 months | IG: −8.5% compared with CG p < 0.01 between groups | IG: no change CG: increased * |
| Prehn et al. 2017 [45] | 37 obese women | IG: 61 ± 4 CG: 61 ± 6 | IG: 35.0 (3.7) CG: 34.7 (4.3) | IG: Calorie restriction CG: Usual diet | PANAS STAI-ST | 12 weeks | IG: −12.3 kg CG: −0.2 kg CG: not reported | Positive PANAS IG: no change CG: decreased * Negative PANAS IG: no change CG: no change STAI-ST IG: no change CG: no change |
| Surwit et al. 1997 [42] | 42 women 130–200% of ideal body weight | IG: 40.6 ± 8.2 CG: 40.3 ± 7.3 | IG: 35.9 ± 4.8 CG: 34.9 ± 4.4 | IG: Low-fat, high-sucrose hypoenergetic diet CG: Low-fat, low-sucrose hypoenergetic diet | STAI-S | 6 weeks | IG: −6.9 kg * CG: −7.4 kg * | IG: no change CG: no change |
| Tomiyama et al. 2010 [31] | 99 women not underweight | NA | IG: 25.8 ± 3.6 CG1: 24.4 ± 4.0 CG2: 24.9 ± 4.5 CG3: 24.1 ± 3.4 | IG: Monitoring + restricting (1200 kcal/day) CG1: Monitoring only CG2: Restricting only (1200 kcal/day) CG3: Control | Perceived stress scale | 3 weeks | IG:-0.9 kg CG1:-1.2 kg CG2:-0.9 kg CG3:+2.2 kg p < 0.05 between groups | IG: increased * CG1:increased * CG2: no change CG3: no change |
| Wadden et al. 1985 [43] | 16 moderately overweight men and women # | 38.1 | NA | IG: Protein-sparing modified fast (450 kcal/day) CG: Protein-formula liquid diet (420 kcal/day) | STAI-ST | 4 weeks | IG: −8.7 kg * CG: −7.3 kg * | IG: decreased * CG: decreased |
| Wadden et al. 1987 [29] | Obese men (5) and women (30) | 44.1 ± 8.7 (women) 42.3 ± 11.6 (men) | NA | IG: 500 kcal protein-sparing modified fast CG: 1200 kcal balanced diet | STAI-ST | 25 weeks | IG: −20.5 kg * CG: −15.7 kg * p < 0.06 between groups | IG: no change CG: no change |
| Wing et al. 1991 [30] | 18 men and 25 women >30% above ideal body weight | 35–70 | NA | IG: VLCD: 1 to 4 weeks—1000–1500 cal/day, 5 to 12 weeks—400 cal/day, 13 to 20 weeks—1000–1500 cal/day CG: Balanced diet: 1000–1500 cal/day | STAI-ST | 20 weeks | IG: −18.6 kg * CG: −10.1 kg * p < 0.003 between groups | IG: decreased * CG: decreased * |
| Yamauchi et al. 2014 [44] | Overweight and obese men (9) and women (9) | IG: 55.8 ± 10.4 CG: 59.0 ± 11.9 | IG: 27.6 ± 3.8 CG: 28.4 ± 2.4 | IG: Lifestyle modification including healthy plate CG: Usual diet | POMS | 3 months | IG: −3.7 kg * CG: −0.1 kg p < 0.001 between groups | IG: no change CG: no change |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Brinkworth et al. 2009 [28] | Low risk | High risk | Low risk | Low risk | High risk | High risk | Low risk | High risk |
| Green et al. 2005 [41] | Low risk | High risk | Low risk | Low risk | High risk | High risk | Low risk | High risk |
| Imayama et al. 2011 [32] | High risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Prehn et al. 2017 [45] | High risk | Low risk | Low risk | Low risk | Unclear | Low risk | Low risk | Low risk |
| Surwit et al. 1997 [42] | High risk | High risk | Low risk | Low risk | High risk | High risk | Low risk | High risk |
| Tomiyama et al. 2010 [31] | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Wadden et al. 1985 [43] | High risk | High risk | Low risk | Low risk | High risk | High risk | Low risk | High risk |
| Wadden et al. 1987 [29] | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Wing et al. 1991 [30] | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Yamauchi et al. 2014 [44] | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Booth, A.O.; Wang, X.; Turner, A.I.; Nowson, C.A.; Torres, S.J. Diet-Induced Weight Loss Has No Effect on Psychological Stress in Overweight and Obese Adults: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 613. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050613
Booth AO, Wang X, Turner AI, Nowson CA, Torres SJ. Diet-Induced Weight Loss Has No Effect on Psychological Stress in Overweight and Obese Adults: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2018; 10(5):613. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050613
Chicago/Turabian StyleBooth, Alison O., Xiaodan Wang, Anne I. Turner, Caryl A. Nowson, and Susan J. Torres. 2018. "Diet-Induced Weight Loss Has No Effect on Psychological Stress in Overweight and Obese Adults: A Meta-Analysis of Randomized Controlled Trials" Nutrients 10, no. 5: 613. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050613