Dietary Fiber Intake and Endometrial Cancer Risk: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Methods
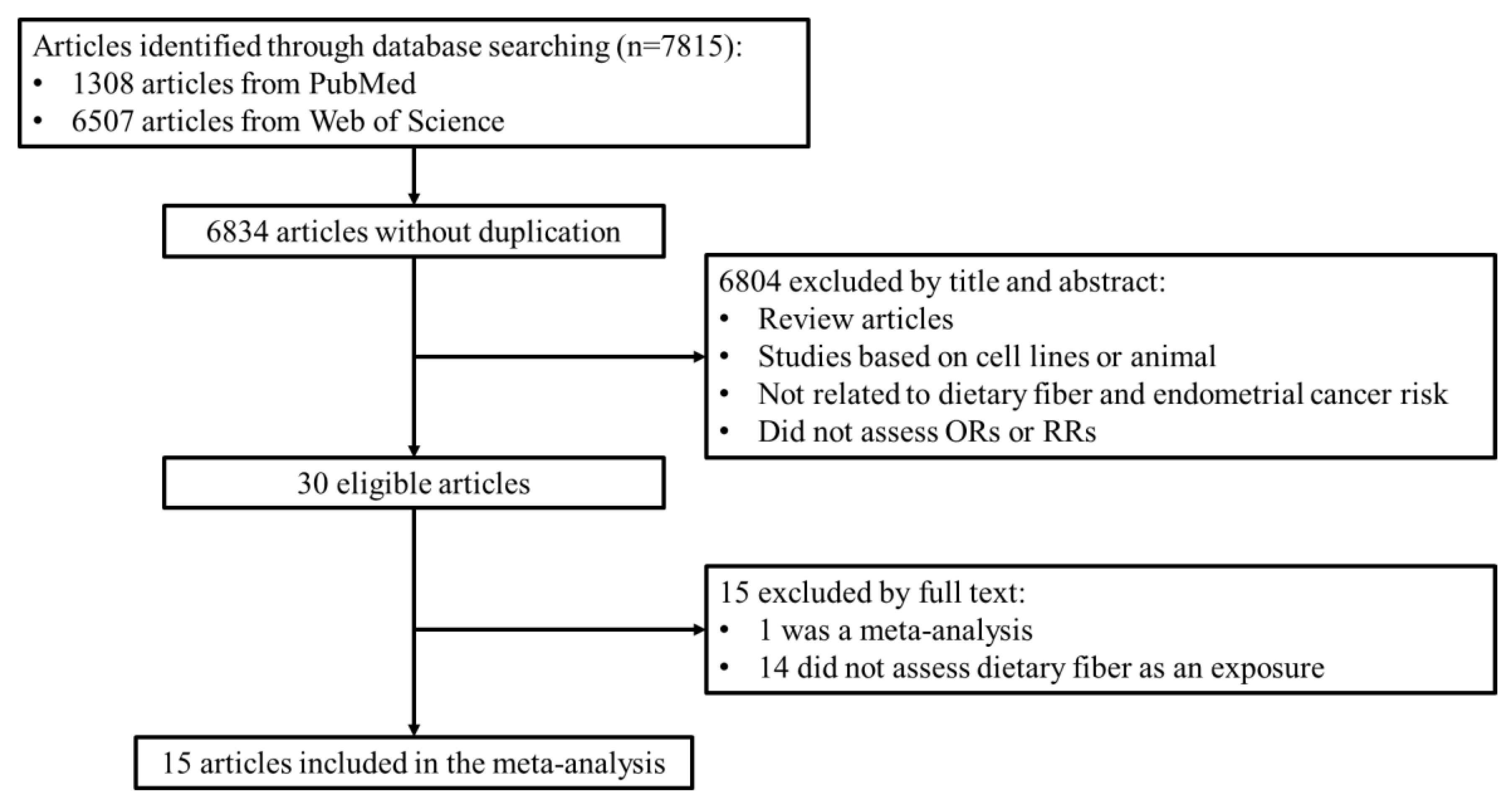
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
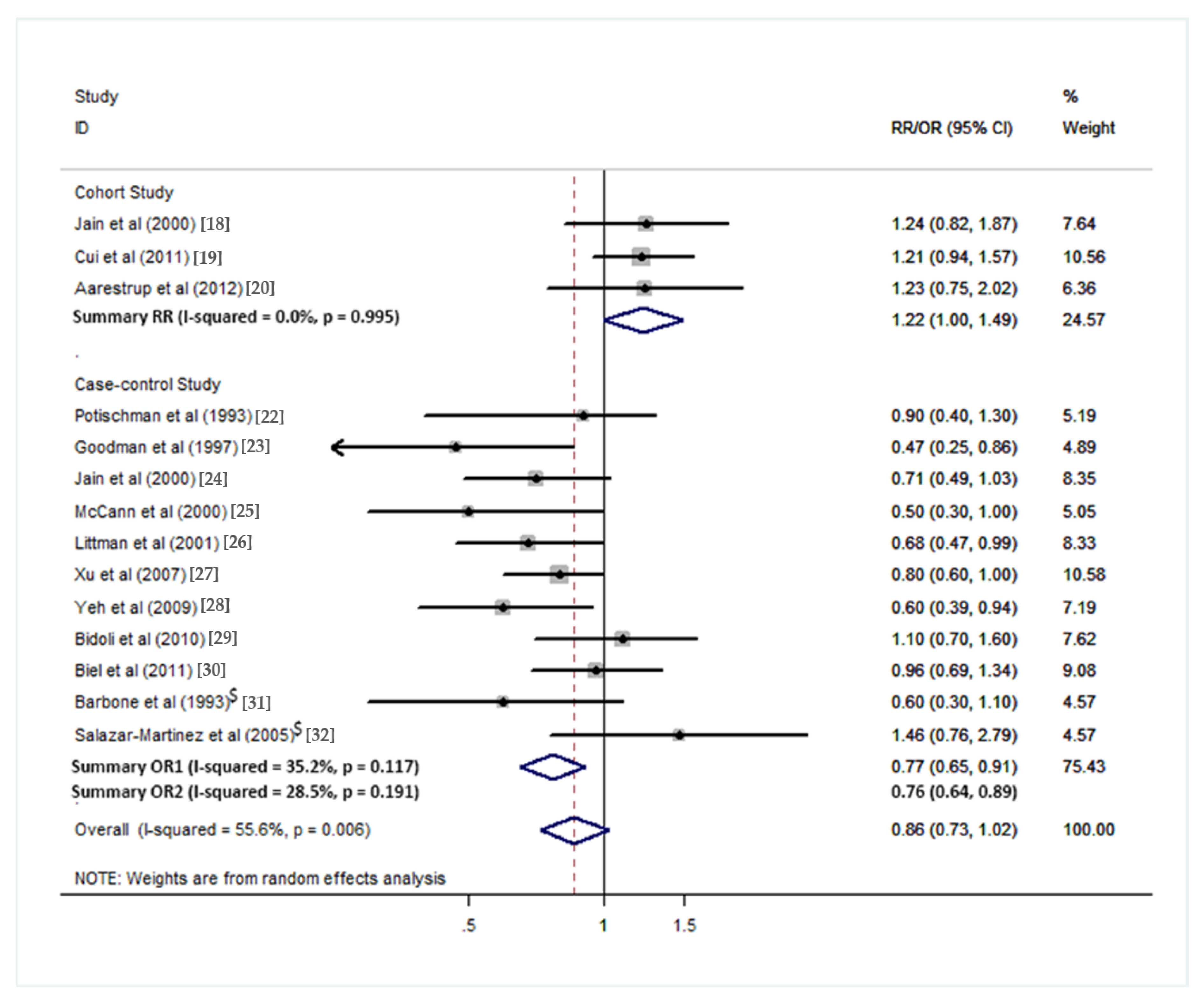
3.1. Total Dietary Fiber
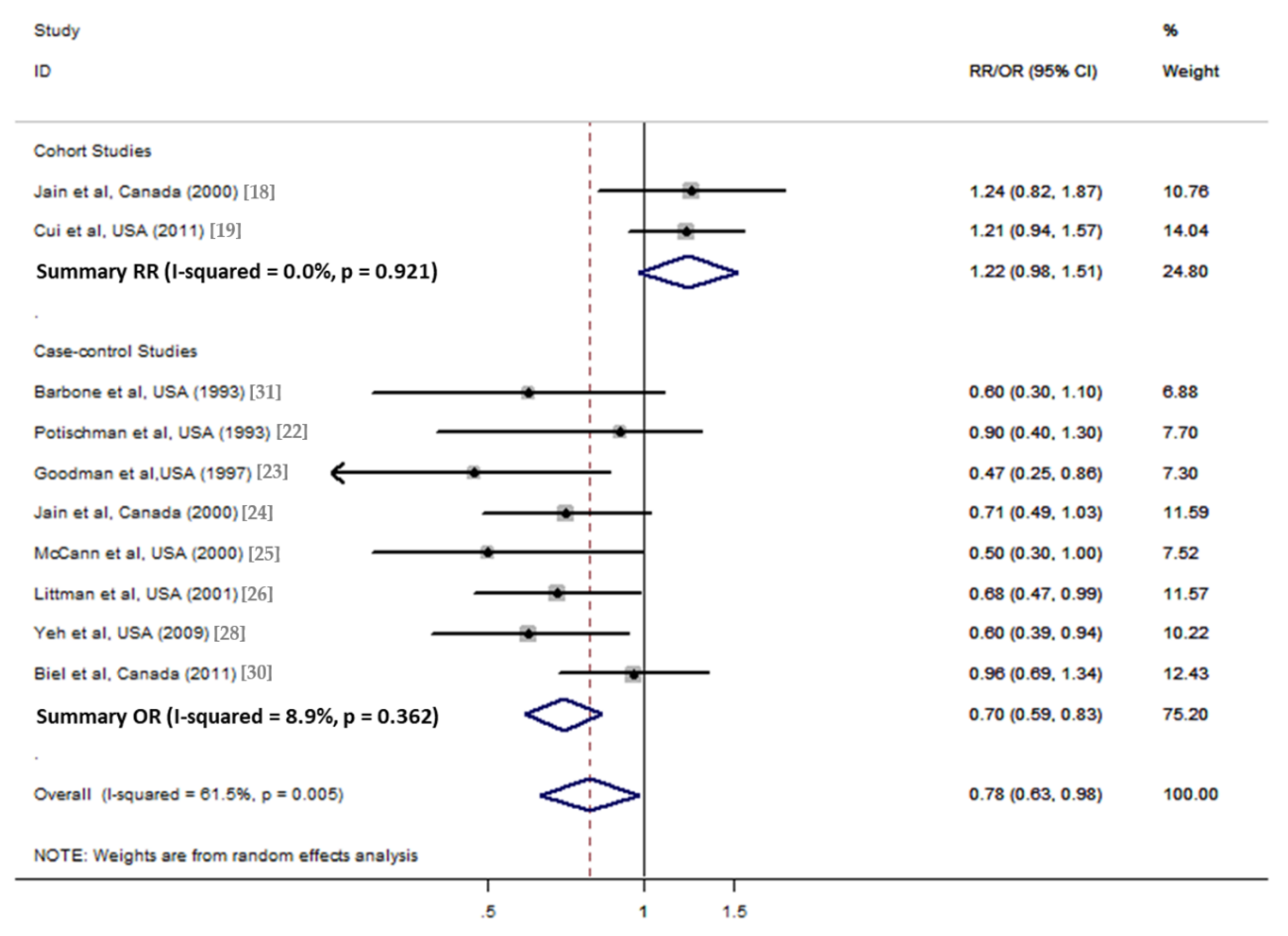
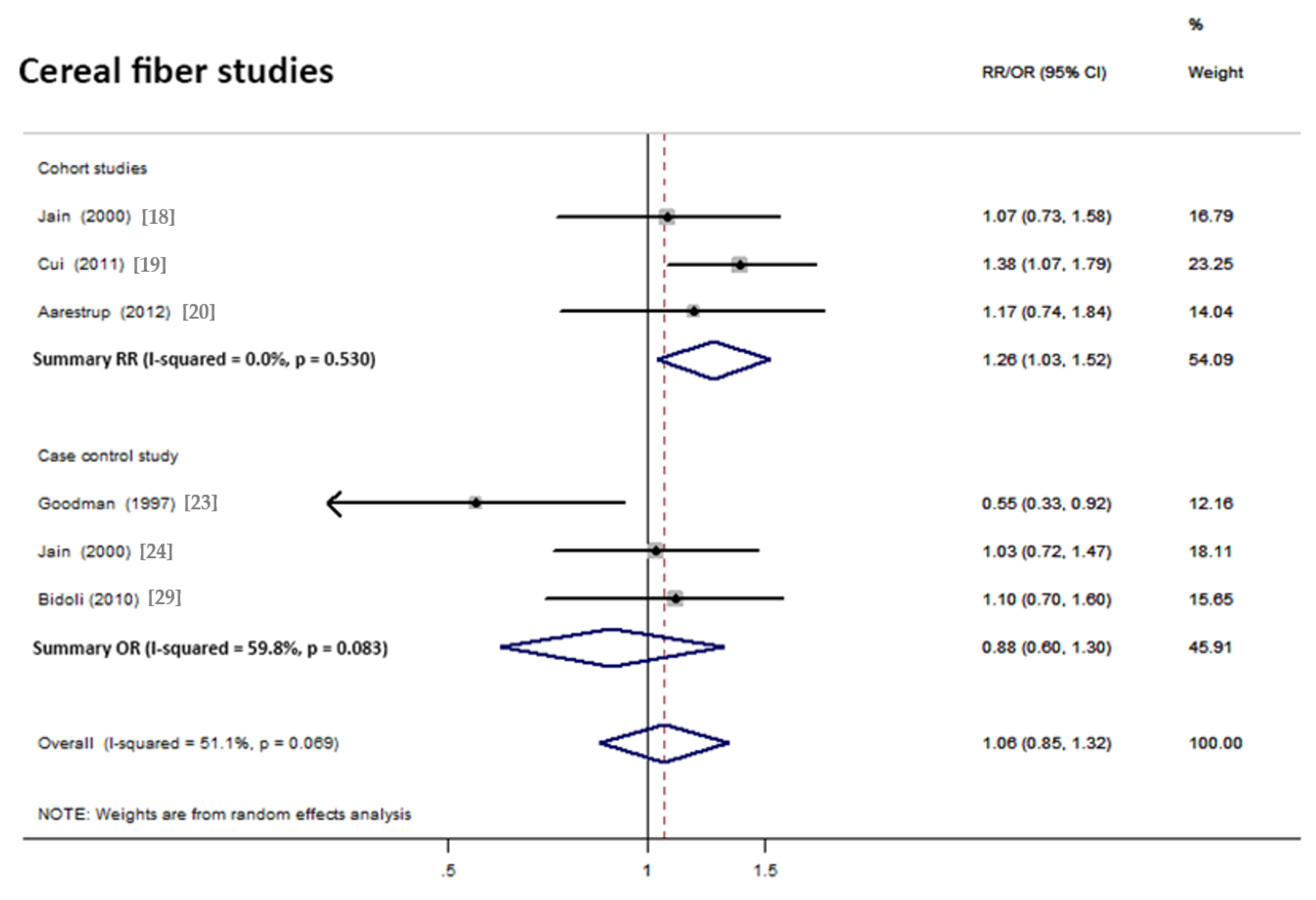
3.2. Cereal Fiber Intake
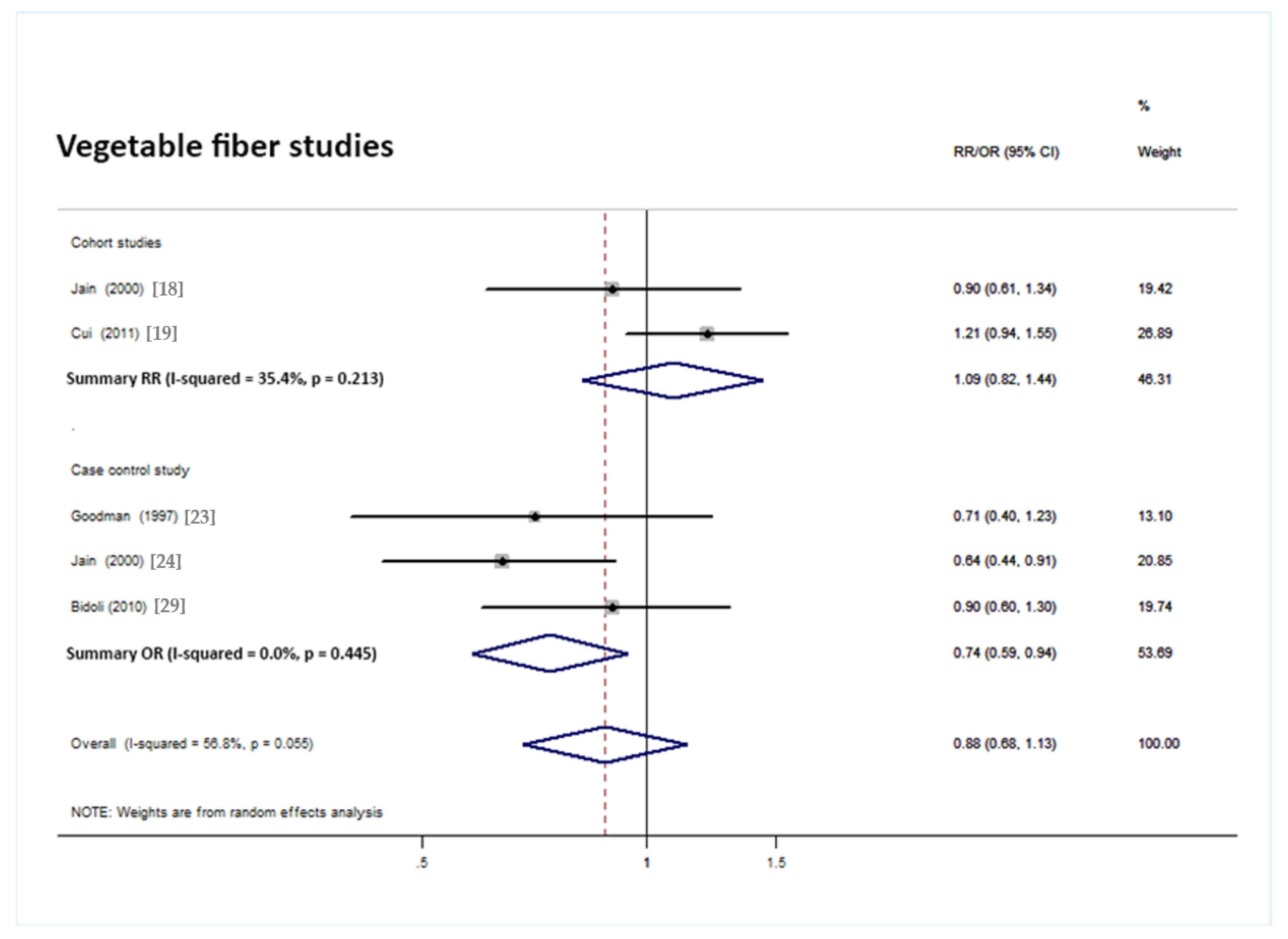
3.3. Vegetable Fiber Intake
3.4. Fruit Fiber Intake and Insoluble Fiber Intake
4. Discussion
4.1. Total Dietary Fiber and Endometrial Cancer Risk
4.2. Subtypes of Dietary Fiber and Endometrial Cancer Risk
4.2.1. Cereal Fiber
4.2.2. Vegetable Fiber, Fruit Fiber, and Insoluble Fiber
4.3. Biochemical Constituents of Dietary Fiber
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, A.L.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; van Limbergen, E.; Vergote, I. Endometrial Cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef]
- Aune, D.; Chan, D.S.M.; Greenwood, D.C.; Vieira, A.R.; Rosenblatt, D.A.N.; Vieira, R.; Norat, T. Dietary Fiber and Breast Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Ann. Oncol. 2012, 23, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.M.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary Fibre, Whole Grains, and Risk of Colorectal Cancer: Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Br. Med. J. 2011, 343. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Qiao, C.; Wang, R.-C.; Zhou, W.-P. Dietary Fiber Intake and Pancreatic Cancer Risk: A Meta-Analysis of Epidemiologic Studies. Sci. Rep. 2015, 5, 10834. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and Prebiotics: Mechanisms and Health Benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Rosenblatt, D.A.N.; Chan, D.S.M.; Vingeliene, S.; Abar, L.; Vieira, A.R.; Greenwood, D.C.; Bandera, E.V.; Norat, T. Anthropometric Factors and Endometrial Cancer Risk: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Ann. Oncol. 2015, 26, 1635–1648. [Google Scholar] [CrossRef] [PubMed]
- Lattimer, J.M.; Haub, M.D. Effects of Dietary Fiber and Its Components on Metabolic Health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food, Nutrition, Physical Activity, and the Prevention of Endometrial Cancer 2013; World Cancer Research Fund/American Institute for Cancer Research; Continuous Update Project Report; Available online: http://www.dietandcancerreport.org (accessed on 22 July 2018).
- Bandera, E.V.; Kushi, L.H.; Moore, D.F.; Gifkins, D.M.; McCullough, M.L. Association between Dietary Fiber and Endometrial Cancer: A Dose-Response Meta-Analysis. Am. J. Clin. Nutr. 2007, 86, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLOS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-Analysis of Observational Studies in Epidemiology—A Proposal for Reporting. J. Am. Med. Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Zhao, J.; Chen, L.; Gao, J.; Du, L.; Shan, B.; Zhang, H.; Wang, Hu.; Gao, Y. Dietary Fat Intake and Endometrial Cancer Risk a Dose Response Meta-Analysis. Medicine 2016, 95. [Google Scholar] [CrossRef]
- Bandera, E.V.; Kushi, L.H.; Moore, D.F.; Gifkins, D.M.; McCullough, M.L. Consumption of Animal Foods and Endometrial Cancer Risk: A Systematic Literature Review and Meta-Analysis. Cancer Causes Control 2007, 18, 967–988. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of Random Effects Meta-Analyses. Br. Med. J. 2011, 342. [Google Scholar] [CrossRef] [PubMed]
- Dersimonian, R.; Laird, N. Metaanalysis in Clinical-Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.G.; Rohan, T.E.; Howe, G.R.; Miller, A.B. A Cohort Study of Nutritional Factors and Endometrial Cancer. Eur. J. Epidemiol. 2000, 16, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Rosner, B.; Willett, W.C.; Hankinson, S.E. Dietary Fat, Fiber, and Carbohydrate Intake in Relation to Risk of Endometrial Cancer. Cancer Epidemiol. Biomark. Prev. 2011, 20, 978–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarestrup, J.; Kyro, C.; Christensen, J.; Kristensen, M.; Wurtz, A.M.L.; Johnsen, N.F.; Overvad, K.; Tjonneland, A.; Olsen, A. Whole Grain, Dietary Fiber, and Incidence of Endometrial Cancer in a Danish Cohort Study. Nutr. Cancer Int. J. 2012, 64, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.O.; Zheng, W.; Potischman, N.; Brinton, L.A.; Hatch, M.C.; Gao, T.; Fraumeni, J.F., Jr. A Population-Based Case-Control Study of Dietary Factors and Endometrial Cancer in Shanghai, People's Republic of China. Am. J. Epidemiol. 1993, 137, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Potischman, N.; Swanson, C.A.; Brinton, L.A.; McAdams, M.; Barrett, R.J.; Berman, M.L.; Mortel, R.; Twiggs, L.B.; Wilbanks, G.D.; Hoover, R.N. Dietary Associations in a Case-Control Study of Endometrial Cancer. Cancer Causes Control 1993, 4, 239–250. [Google Scholar] [PubMed]
- Goodman, M.T.; Wilkens, L.R.; Hankin, J.H.; Lyu, L.C.; Wu, A.H.; Kolonel, L.N. Association of Soy and Fiber Consumption with the Risk of Endometrial Cancer. Am. J. Epidemiol. 1997, 146, 294–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, M.G.; Howe, G.R.; Rohan, T.E. Nutritional Factors and Endometrial Cancer in Ontario, Canada. Cancer Control 2000, 7, 288–296. [Google Scholar] [CrossRef] [PubMed]
- McCann, S.E.; Freudenheim, J.L.; Marshall, J.R.; Brasure, J.R.; Swanson, M.K.; Graham, S. Diet in the Epidemiology of Endometrial Cancer in Western New York (United States). Cancer Causes Control 2000, 11, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Littman, A.J.; Beresford, S.A.A.; White, E. The Association of Dietary Fat and Plant Foods with Endometrial Cancer (United States). Cancer Causes Control 2001, 12, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.-H.; Dai, Q.; Xiang, Y.B.; Zhao, G.M.; Ruan, Z.X.; Cheng, J.R.; Zheng, W.; Shu, X.O. Nutritional Factors in Relation to Endometrial Cancer: A Report from a Population-Based Case-Control Study in Shanghai, China. Int. J. Cancer 2007, 120, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.; Moysich, K.B.; Jayaprakash, V.; Rodabaugh, K.J.; Graham, S.; Brasure, J.R.; McCann, S.E. Higher Intakes of Vegetables and Vegetable-Related Nutrients Are Associated with Lower Endometrial Cancer Risks. J. Nutr. 2009, 139, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Bidoli, E.; Pelucchi, C.; Zucchetto, A.; Negri, E.; Maso, L.D.; Polesel, J.; Montella, M.; Franceschi, S.; Serraino, D.; la Vecchia, C.; et al. Fiber Intake and Endometrial Cancer Risk. Acta Oncol. 2010, 49, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Biel, R.K.; Csizmadi, I.; Cook, L.S.; Courneya, K.S.; Magliocco, A.M.; Friedenreich, C.M. Risk of Endometrial Cancer in Relation to Individual Nutrients from Diet and Supplements. Public Health Nutr. 2011, 14, 1948–1960. [Google Scholar] [CrossRef] [PubMed]
- Barbone, F.; Austin, H.; Partridge, E.E. Diet and Endometrial Cancer—A Case-Control Study. Am. J. Epidemiol. 1993, 137, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Martinez, E.; Lazcano-Ponce, E.; Sanchez-Zamorano, L.M.; Gonzalez-Lira, G.; Escudero-DE Los Rios, P.; Hernandez-Avila, M. Dietary Factors and Endometrial Cancer Risk. Results of a Case-Control Study in Mexico. Int. J. Gynecol. Cancer 2005, 15, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Baird, P.; Davis, R.H., Jr.; Ferreri, S.; Knudtson, M.; Koraym, A.; Waters, V.; Williams, C.L. Health Benefits of Dietary Fiber. Nutr. Rev. 2009, 67, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Stewart, M.L. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J. Acad. Nutr. Diet. 2015, 115, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Bingham, S. Definitions and Intakes of Dietary Fiber. Am. J. Clin. Nutr. 1987, 45, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, Lifestyle, and the Risk of Type 2 Diabetes Mellitus in Women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hullar, M.A.J.; Burnett-Hartman, A.N.; Lampe, J.W. Gut Microbes, Diet, and Cancer. In Advances in Nutrition and Cancer; Zappia, V., Panico, S., Russo, G.L., Budillon, A., DellaRagione, F., Eds.; 2014; pp. 377–399. [Google Scholar]
- Guarner, F.; Malagelada, J.R. Gut Flora in Health and Disease. Lancet 2003, 361, 512–519. [Google Scholar] [CrossRef]
- Hague, A.D.; Elder, J.E.; Hicks, D.J.; Paraskeva, C. Apoptosis in Colorectal Tumor-Cells - Induction by the Short-Chain Fatty-Acids Butyrate, Propionate and Acetate and by the Bile-Salt Deoxycholate. Int. J. Cancer 1995, 60, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of Endometrial Carcinoma: More Than Two Types. Lancet Oncol. 2014, 15, E268–E278. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Case-Controls (Cohort) Size | Age (Years) | Dietary Assessment | Time Frame * | Exclusion of Hysterectomy | Dietary Fiber Evaluated | OR/RR (95% CI) | Covariates Considered |
|---|---|---|---|---|---|---|---|---|---|
| Cohort studies | |||||||||
| Jain et al. [18], 2000 | Canada | 221/3697 | 40–59 | FFQ 86 items | 1 month period | Yes | Dietary fiber: >23.2 vs. <15.1 g/day Insoluble fiber Soluble fiber Cereal fiber: >4.8 vs. <2.7 g/day Fruit fiber: >5.7 vs. <2.2 g/day Vegetable fiber: >9.6 vs. <5.5 g/day | 1.24 (0.82, 1.87) 1.1 (0.74, 1.63) 1.09 (0.72, 1.65) 1.07 (0.73, 1.58) 1.08 (0.73, 1.61) 0.9 (0.61, 1.34) | A.B.E.S.H.R |
| Cui et al. [19], 2011 | USA | 669/68070 | 30–55 | FFQ 130 items | A 26-year period † | Yes | Total fiber: 21.3 vs. 10.7 g/day (median) Vegetable fiber: 8.5 vs. 3.2 g/day (median) Fruit fiber: 7.1 vs. 1.4 g/day (median) Cereal fiber: 6 vs. 1.9 g/day (median) | 1.21 (0.94, 1.57) 1.21 (0.94, 1.55) 0.97 (0.76, 1.25) 1.38 (1.07, 1.79) | B.E.S.H.R |
| Aarestrup et al. [20], 2012 | Denmark | 217/24418 | 50–64 | FFQ 192 items | 12 months | Yes | Total dietary fiber: >24 vs. <17 g/day Total cereal fiber: >11 vs. <7 g/day | 1.23 (0.75, 2.02) 1.17 (0.74, 1.84) | B.E.S.H.R |
| Population-based case–control studies | |||||||||
| Shu et al. [21], 1993 | China | 268/268 | 18–74 | FFQ 63 items | 10 years | Yes | Crude fiber: >4.68 vs. <2.65 g/day | 1.1 | A.B.E.R |
| Potischman et al. [22], 1993 | USA | 399/296 | 20–74 | FFQ 60 items (Block) | Past few years | No mention | Fiber: >13.6 vs. <7.7 g/day | 0.9 (0.4, 1.3) | A.B.(E).S.H.R |
| Goodman et al. [23], 1997 | USA | 332/511 | 18–84 | Dietary history 250 items | 1 year | Yes | Crude fiber: >6.04 vs. <3.01 g/day NSP: >20.6 vs. <10.2 g/day Cellulose: >5.1 vs. <2.35 g/day NCP: >15 vs. <7.27 g/day Dietary fiber: >23.9 vs. <12.3 g/day Cereal fiber: >2.51 vs. <0.01 g/day Vegetable fiber: >6.25 vs. <2.94 g/day Fruit fiber: >6.27 vs. <2.21 g/day | 0.6 (0.33, 1.09) 0.6 (0.32, 1.11) 0.59 (0.32, 1.07) 0.62 (0.34, 1.15) 0.47 (0.25, 0.86) 0.55 (0.33, 0.92) 0.71 (0.4, 1.23) 0.54 (0.32, 0.92) | (A).B.H.R |
| Jain et al. [24], 2000 | Canada | 552/562 | 30–79 | Dietary History (unknown items) | 1 year | Yes | Dietary fiber: >27.5 vs. <17.2 g/day Insoluble fiber Cereal fiber: >10.5 vs. <4.8 g/day Fruit fiber: >8.9 vs. <3.4 g/day Vegetable fiber: >12.83 vs. <6.63 g/day | 0.71 (0.49, 1.03) 0.92 (0.64, 1.33) 1.03 (0.72, 1.47) 1.34 (0.92, 1.95) 0.64 (0.44, 0.91) | A.B.E.S.H.R |
| McCann et al. [25], 2000 | USA | 232/639 | 40–85 | FFQ 172 items | 2 years | Yes | Dietary fiber: >32 vs. <20 g/day | 0.5 (0.3, 1) | A.B.E.S.H.R |
| Littman et al. [26], 2001 | USA | 679/944 | 45–74 | FFQ 98 items | 5 years | Yes | Total fiber: >10.7 vs.<5.6 g/1000 kcal per day | 0.68 (0.47, 0.99) | A.B.E.S.H |
| Xu et al. [27], 2007 | China | 1204/1212 | 30–69 | FFQ 71 items | 5 years | Yes | Dietary fiber: >8.1 vs.<4.8 g/1000 kcal per day | 0.8 (0.6, 1) | A.B.E.H.R |
| Yeh et al. [28], 2009 | USA | 541/541 | 27–96 | FFQ 44 items | Several years | Yes | Dietary fiber: >33 vs. <16 g/day | 0.6 (0.39, 0.94) | A.B.E.S.H |
| Bidoli et al. [29], 2010 | Italy | 454/908 | 18–79 | FFQ 78 items | 2 years | Yes | Total fiber: (mean = 15.3 ± 5.2 g/day) Soluble NCP: (mean = 7.7 ± 2.5 g/day) Total insoluble fiber: (mean = 7.6 ± 3.6 g/day) Cellulose: (mean = 3.6 ± 1.9 g/day) Insoluble NCP: (mean = 4 ± 1.5 g/day) Lignin: (mean = 1.5 ± 0.5 g/day) Vegetable fiber: (mean = 5.7 ± 2.2 g/day) Fruit fiber: (mean = 5.8 ± 3.6 g/day) Grain fiber: (mean = 4.5 ± 2.1 g/day) | 1.1 (0.7, 1.6) 0.7 (0.5, 1.1) 1 (0.7, 1.5) 0.9 (0.6, 1.3) 0.9 (0.6, 1.3) 0.6 (0.4, 0.9) 0.9 (0.6, 1.3) 0.8 (0.5, 1.1) 1.1 (0.7, 1.6) | A.B.E.S.H.R |
| Biel et al. [30], 2011 | Canada | 506/981 | 30–79 | Diet History Questionnaire 124 items | 1 year | No mention | Dietary fiber: >21.9 vs. <14.8 g/day Insoluble fiber: >14.3 vs. <9.5 g/day Soluble fiber: >7.5 vs. <5.1 g/day | 0.96 (0.69, 1.34) 0.95 (0.68, 1.34) 1.08 (0.77, 1.52) | A.B.E.H.R |
| Hospital-based case-control studies | |||||||||
| Barbone et al. [31], 1993 | USA | 103/236 | No mention | FFQ 116 items (Willett) | 1 year | No mention | Dietary fiber: 19.5 g/day | 0.6 (0.3, 1.1) | A.B.E.S.H.R |
| Salazar-Martinez et al. [32], 2005 | Mexico | 85/629 | 18–81 | FFQ 116 items | 1 year | Yes | Dietary fiber: >24 vs. <13 g/day | 1.46 (0.76, 2.79) | A.B.E.R |
| Reference | Country | Case–Controls (Cohort) Size | Age (Year) | Type of Study | Dietary Fibers Evaluated | OR/RR (95% CI) | Covariates Considered |
|---|---|---|---|---|---|---|---|
| Fruit fiber | |||||||
| Jain et al. [18], 2000 | Canada | 221/3697 | 40–59 | Cohort study | Fruit fiber: >5.7 vs. <2.2 g/day | 1.08 (0.73, 1.61) | A.B.E.S.H.R |
| Cui et al. [19], 2011 | USA | 669/68070 | 30–55 | Cohort study | Fruit fiber: 7.1 vs. 1.4 g/day (median) | 0.97 (0.76, 1.25) | B.E.S.H.R |
| Goodman et al. [23], 1997 | USA | 332/511 | 18–84 | Population-based case-control study | Fruit fiber: >6.27 vs. <2.21 g/day | 0.54 (0.32, 0.92) | (A).B.H.R |
| Jain et al. [24], 2000 | Canada | 552/562 | 30–79 | Population-based case–control study | Fruit fiber: >8.9 vs. <3.4 g/day | 1.34 (0.92, 1.95) | A.B.E.S.H.R |
| Bidoli et al. [29], 2010 | Italy | 454/908 | 18–79 | Population-based case–control study | Fruit fiber: (mean = 5.8 ± 3.6 g/day) | 0.8 (0.5, 1.1) | A.B.E.S.H.R |
| Insoluble fiber | |||||||
| Jain et al. [18], 2000 | Canada | 221/3697 | 40–59 | Cohort study | Insoluble fiber | 1.1 (0.74, 1.63) | A.B.E.S.H.R |
| Jain et al. [24], 2000 | Canada | 552/562 | 30–79 | Population-based case–control study | Insoluble fiber | 0.92 (0.64, 1.33) | A.B.E.S.H.R |
| Bidoli et al. [29], 2010 | Italy | 454/908 | 18–79 | Population-based case–control study | Total insoluble fiber: (mean = 7.6 ± 3.6 g/day) | 1 (0.7, 1.5) | A.B.E.S.H.R |
| Biel et al. [30], 2011 | Canada | 506/981 | 30–79 | Population-based case–control study | Insoluble fiber: >14.3 vs. <9.5 g/day | 0.95 (0.68, 1.34) | A.B.E.H.R |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.; Zhao, Q.; Li, X.; Zhao, J.; Li, P.; Lin, S.; Wang, H.; Zang, J.; Xiao, Y.; Xu, W.; et al. Dietary Fiber Intake and Endometrial Cancer Risk: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 945. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070945
Chen K, Zhao Q, Li X, Zhao J, Li P, Lin S, Wang H, Zang J, Xiao Y, Xu W, et al. Dietary Fiber Intake and Endometrial Cancer Risk: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(7):945. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070945
Chicago/Turabian StyleChen, Kangning, Qianyu Zhao, Xiaofan Li, Jing Zhao, Peiqin Li, Shuchun Lin, Hongwei Wang, Jiajie Zang, Ying Xiao, Wanghong Xu, and et al. 2018. "Dietary Fiber Intake and Endometrial Cancer Risk: A Systematic Review and Meta-Analysis" Nutrients 10, no. 7: 945. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070945