Association between 25-Hydroxyvitamin D Status and Components of Body Composition and Glucose Metabolism in Older Men and Women

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Assessment of Serum 25(OH)D Concentration
2.3. Assessment of Participant Characteristics and Covariates
2.4. Assessment of Measures of Insulin Resistance
2.5. Assessment of Body Composition
2.6. Statistics
3. Results
3.1. Participants’ Characteristics
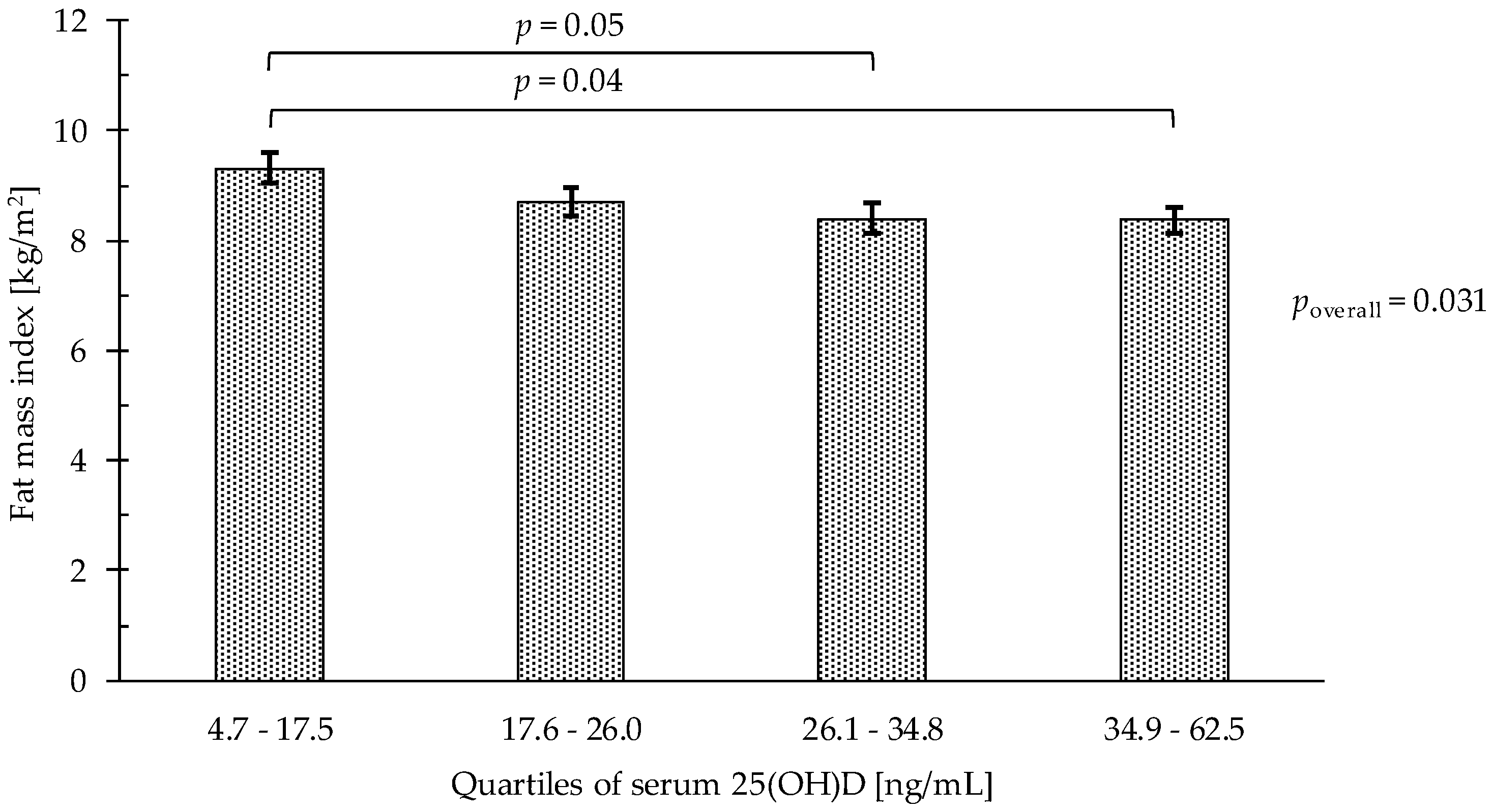
3.2. Association between Quartiles of Serum 25(OH)D and Fat Mass (FMI)
3.3. Association between Quartiles of Serum 25(OH)D and Muscle Mass (ALMI)
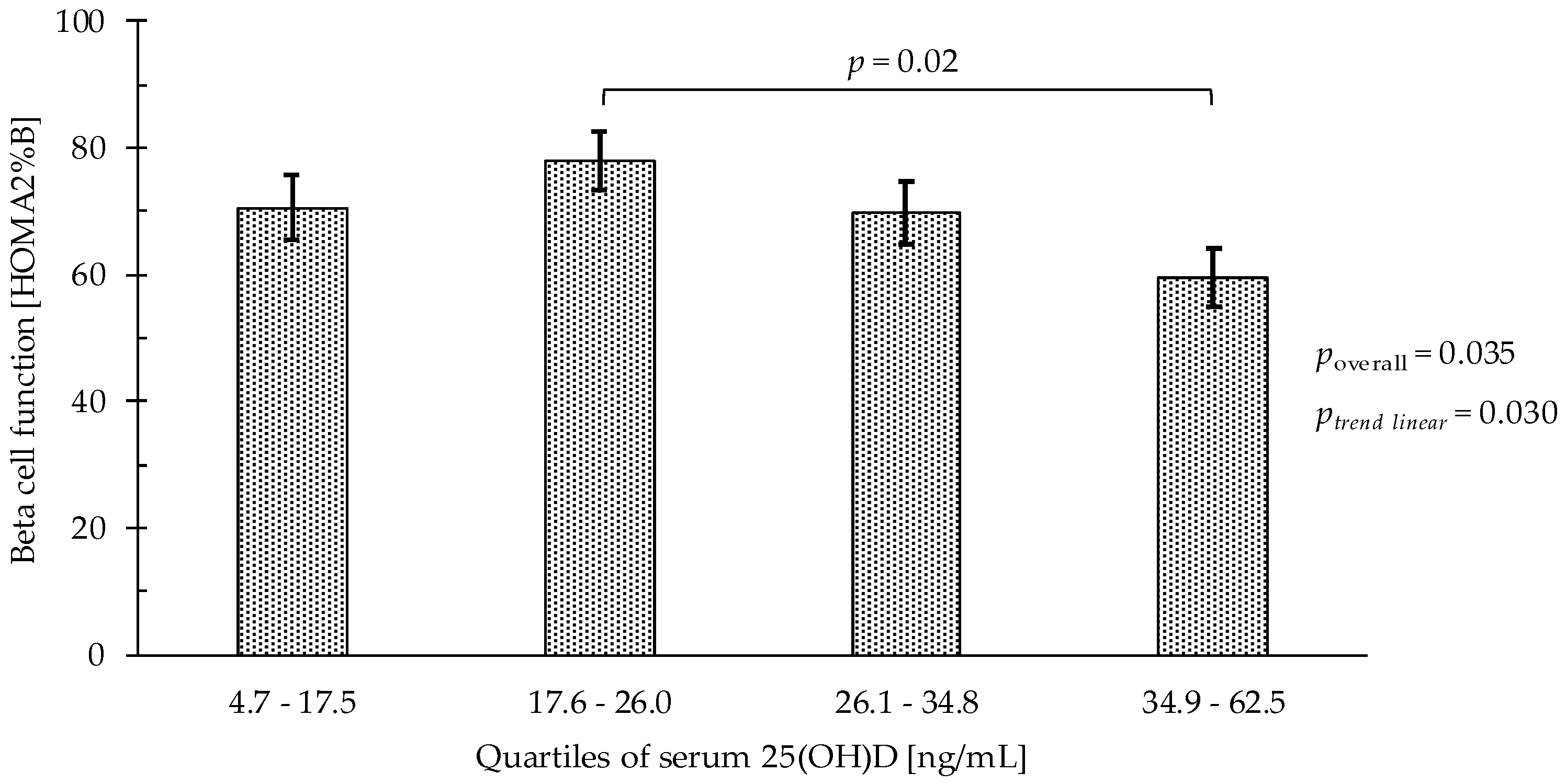
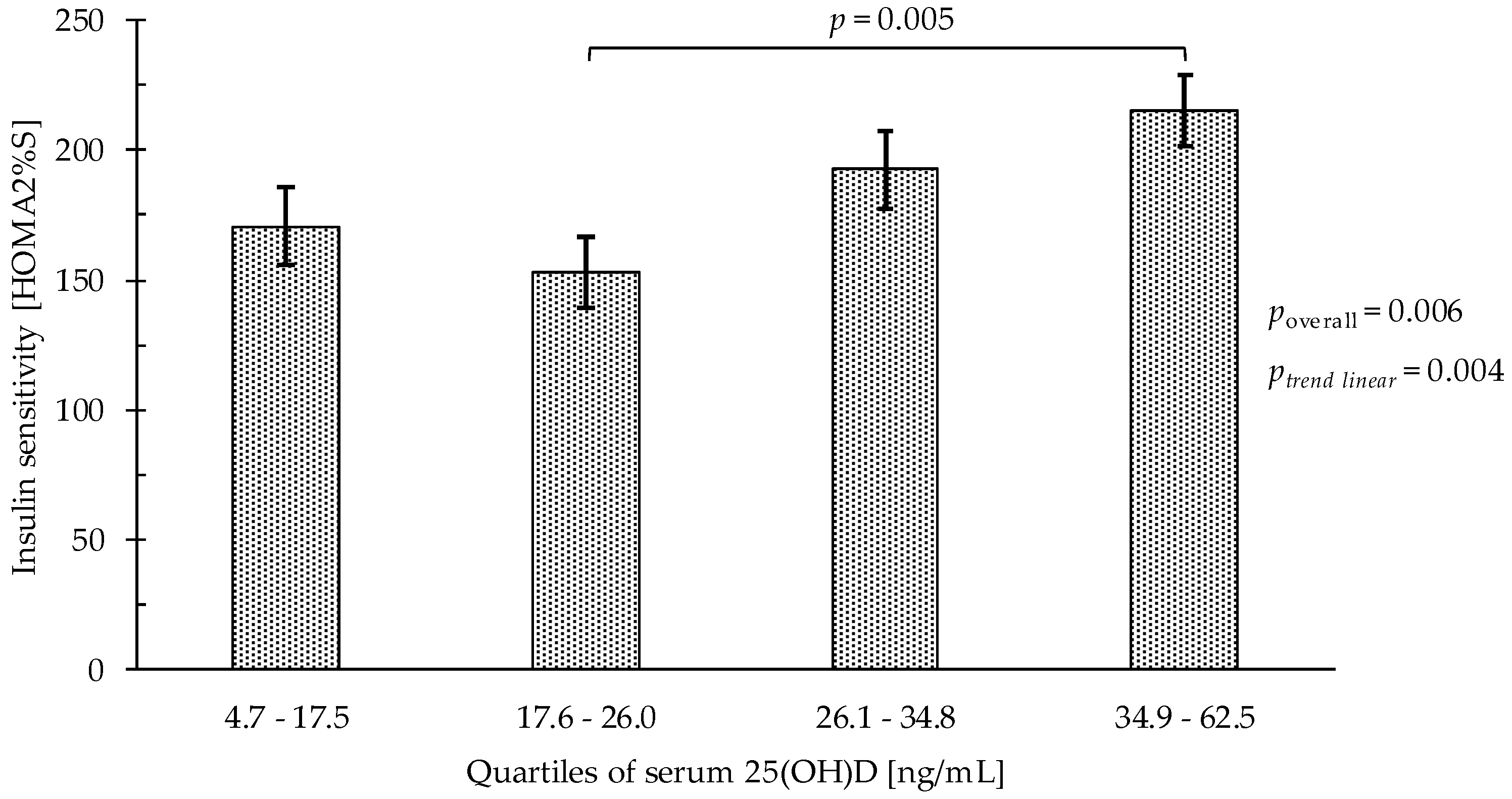
3.4. Association between Quartiles of Serum 25(OH)D and Glucose Metabolism
3.5. Serum 25(OH)D Status and Prevalence of Insulin Resistance and Diabetes
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Roubenoff, R. Sarcopenic obesity: The confluence of two epidemics. Obes. Res. 2004, 12, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N. Body composition in healthy aging. Ann. N. Y. Acad. Sci. 2000, 904, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Cleasby, M.E.; Jamieson, P.M.; Atherton, P.J. Insulin resistance and sarcopenia: Mechanistic links between common co-morbidities. J. Endocrinol. 2016, 229, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Wayne, S.J.; Waters, D.L.; Janssen, I.; Gallagher, D.; Morley, J.E. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes. Res. 2004, 12, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Wells, J.C.; Smith, S.R.; Stephan, B.C.; Siervo, M. Sarcopenic obesity: A Critical appraisal of the current evidence. Clin. Nutr. 2012, 31, 583–601. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Skrabakova, Z.; Gonzalez-Gross, M.; Valtuena, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Molgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H. Relevance of vitamin D in bone and muscle health of cancer patients. Anticancer Agents Med. Chem. 2013, 13, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Oliai Araghi, S.; van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; Enneman, A.W.; Sohl, E.; Swart, K.M.; van der Zwaluw, N.L.; van Wijngaarden, J.P.; Dhonukshe-Rutten, R.A.; et al. BMI and body fat mass is inversely associated with Vitamin D levels in older individuals. J. Nutr. Health Aging 2015, 19, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Shantavasinkul, P.C.; Phanachet, P.; Puchaiwattananon, O.; Chailurkit, L.O.; Lepananon, T.; Chanprasertyotin, S.; Ongphiphadhanakul, B.; Warodomwichit, D. Vitamin D status is a determinant of skeletal muscle mass in obesity according to body fat percentage. Nutrition 2015, 31, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Tosunbayraktar, G.; Bas, M.; Kut, A.; Buyukkaragoz, A.H. Low serum 25(OH)D levels are associated to higher BMI and metabolic syndrome parameters in adult subjects in Turkey. Afr. Health Sci. 2015, 15, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, H.A.; Borchers, M.; Gudat, F.; Duermueller, U.; Theiler, R.; Stahelin, H.B.; Dick, W. In situ detection of 1,25-dihydroxyvitamin D3 receptor in human skeletal muscle tissue. Histochem. J. 2001, 33, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Borchers, M.; Gudat, F.; Durmuller, U.; Stahelin, H.B.; Dick, W. Vitamin D receptor expression in human muscle tissue decreases with age. J. Bone Miner Res. 2004, 19, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Ceglia, L.; da Silva Morais, M.; Park, L.K.; Morris, E.; Harris, S.S.; Bischoff-Ferrari, H.A.; Fielding, R.A.; Dawson-Hughes, B. Multi-step immunofluorescent analysis of vitamin D receptor loci and myosin heavy chain isoforms in human skeletal muscle. J. Mol. Histol. 2010, 41, 137–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceglia, L.; Niramitmahapanya, S.; da Silva Morais, M.; Rivas, D.A.; Harris, S.S.; Bischoff-Ferrari, H.; Fielding, R.A.; Dawson-Hughes, B. A randomized study on the effect of vitamin D(3) supplementation on skeletal muscle morphology and vitamin D receptor concentration in older women. J. Clin. Endocrinol. Metab. 2013, 98, E1927–E1935. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Gao, D.; Wilding, J.; Trayhurn, P.; Bing, C. Vitamin D signalling in adipose tissue. Br. J. Nutr. 2012, 108, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Norman, A.W.; Okamura, W.H.; Sen, A.; Zemel, M.B. 1alpha,25-Dihydroxyvitamin D3 modulates human adipocyte metabolism via nongenomic action. FASEB J. 2001, 15, 2751–2753. [Google Scholar] [CrossRef] [PubMed]
- Mitri, J.; Dawson-Hughes, B.; Hu, F.B.; Pittas, A.G. Effects of vitamin D and calcium supplementation on pancreatic beta cell function, insulin sensitivity, and glycemia in adults at high risk of diabetes: The Calcium and Vitamin D for Diabetes Mellitus (CaDDM) randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Pittas, A.G.; Harris, S.S.; Stark, P.C.; Dawson-Hughes, B. The effects of calcium and vitamin D supplementation on blood glucose and markers of inflammation in nondiabetic adults. Diabetes Care 2007, 30, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.J.; Yun, S.; Oh, K.; Kim, K. Relation of serum 25-hydroxyvitamin D status with skeletal muscle mass by sex and age group among Korean adults. Br. J. Nutr. 2015, 114, 1838–1844. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Deeg, D.J.; Lips, P. Longitudinal Aging Study A: Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): The Longitudinal Aging Study Amsterdam. J. Clin. Endocrinol. Metab. 2003, 88, 5766–5772. [Google Scholar] [CrossRef] [PubMed]
- Al-Shoha, A.; Qiu, S.; Palnitkar, S.; Rao, D.S. Osteomalacia with bone marrow fibrosis due to severe vitamin D deficiency after a gastrointestinal bypass operation for severe obesity. Endocr. Pract. 2009, 15, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.J.; Hu, F.B.; Zhang, Y.; Karlson, E.W.; Dawson-Hughes, B. Higher 25-hydroxyvitamin D concentrations are associated with better lower-extremity function in both active and inactive persons aged > or = 60 year. Am. J. Clin. Nutr. 2004, 80, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.J.; Chan She Ping-Delfos, W.; Ghanbari, M.H. Calcium and vitamin D for obesity: A review of randomized controlled trials. Eur. J. Clin. Nutr. 2011, 65, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Maunsell, Z.; Wright, D.J.; Rainbow, S.J. Routine isotope-dilution liquid chromatography-tandem mass spectrometry assay for simultaneous measurement of the 25-hydroxy metabolites of vitamins D2 and D3. Clin. Chem. 2005, 51, 1683–1690. [Google Scholar] [CrossRef] [PubMed]
- Saenger, A.K.; Laha, T.J.; Bremner, D.E.; Sadrzadeh, S.M. Quantification of serum 25-hydroxyvitamin D(2) and D(3) using HPLC-tandem mass spectrometry and examination of reference intervals for diagnosis of vitamin D deficiency. Am. J. Clin. Pathol. 2006, 125, 914–920. [Google Scholar] [CrossRef] [PubMed]
- The National Institute of Standards and Technology (NIST); The National Institutes of Health (NIH). Vitamin D Metabolites Quality Assurance Program. Available online: http://www.nist.gov/mml/analytical/vitdqap.cfm (accessed on 1 November 2016).
- Resnick, B.; Nahm, E.S.; Orwig, D.; Zimmerman, S.S.; Magaziner, J. Measurement of activity in older adults: Reliability and validity of the Step Activity Monitor. J. Nurs. Meas. 2001, 9, 275–290. [Google Scholar] [CrossRef] [PubMed]
- White, D.K.; Tudor-Locke, C.; Zhang, Y.; Fielding, R.; LaValley, M.; Felson, D.T.; Gross, K.D.; Nevitt, M.C.; Lewis, C.E.; Torner, J.; et al. Daily walking and the risk of incident functional limitation in knee osteoarthritis: An observational study. Arthritis Care Res. 2014, 66, 1328–1336. [Google Scholar] [CrossRef] [PubMed]
- Geloneze, B.; Vasques, A.C.; Stabe, C.F.; Pareja, J.C.; Rosado, L.E.; Queiroz, E.C.; Tambascia, M.A.; Investigators, B. HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome: Brazilian Metabolic Syndrome Study (BRAMS). Arq. Bras. Endocrinol. Metabol. 2009, 53, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jungert, A.; Neuhauser-Berthold, M. Sex-specific determinants of serum 25-hydroxyvitamin D3 concentrations in an elderly German cohort: A cross-sectional study. Nutr. Metab. (Lond) 2015, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Moschonis, G.; Tanagra, S.; Koutsikas, K.; Nikolaidou, A.; Androutsos, O.; Manios, Y. Association between serum 25-hydroxyvitamin D levels and body composition in postmenopausal women: The postmenopausal Health Study. Menopause 2009, 16, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.A.; Cho, H.; Eun, C.R.; Yoo, H.J.; Kim, S.G.; Choi, K.M.; Baik, S.H.; Choi, D.S.; Park, M.H.; Han, C.; et al. Association between visceral obesity and sarcopenia and vitamin D deficiency in older Koreans: The Ansan Geriatric Study. J. Am. Geriatr. Soc. 2012, 60, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Cao, Z.B.; Tanisawa, K.; Ito, T.; Oshima, S.; Higuchi, M. The relationship between serum 25-hydroxyvitamin D concentration, cardiorespiratory fitness, and insulin resistance in Japanese men. Nutrients 2014, 7, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Esteghamati, A.; Aryan, Z.; Esteghamati, A.; Nakhjavani, M. Vitamin D deficiency is associated with insulin resistance in nondiabetics and reduced insulin production in type 2 diabetics. Horm. Metab. Res. 2015, 47, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Peng, S. The relationship between serum vitamin D and HOMA-IR in overweight elderly patients. Int. J. Cardiol. 2014, 177, 1100–1102. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Meigs, J.B.; Pittas, A.G.; McKeown, N.M.; Economos, C.D.; Booth, S.L.; Jacques, P.F. Plasma 25-hydroxyvitamin D is associated with markers of the insulin resistant phenotype in nondiabetic adults. J. Nutr. 2009, 139, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Brouwer-Brolsma, E.M.; Feskens, E.J.; Steegenga, W.T.; de Groot, L.C. Associations of 25-hydroxyvitamin D with fasting glucose, fasting insulin, dementia and depression in European elderly: The SENECA study. Eur. J. Nutr. 2013, 52, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Song, B.M.; Kim, H.C.; Choi, D.P.; Oh, S.M.; Suh, I. Association between serum 25-hydroxyvitamin D level and insulin resistance in a rural population. Yonsei Med. J. 2014, 55, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Yetley, E.A. Assessing the vitamin D status of the US population. Am. J. Clin. Nutr. 2008, 88, S558–S564. [Google Scholar] [CrossRef] [PubMed]
- Hypponen, E.; Power, C. Hypovitaminosis D in British adults at age 45 year: Nationwide cohort study of dietary and lifestyle predictors. Am. J. Clin. Nutr. 2007, 85, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.S.; Dawson-Hughes, B. Reduced sun exposure does not explain the inverse association of 25-hydroxyvitamin D with percent body fat in older adults. J. Clin. Endocrinol. Metab. 2007, 92, 3155–3157. [Google Scholar] [CrossRef] [PubMed]
- Drincic, A.T.; Armas, L.A.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity 2012, 20, 1444–1448. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marantes, I.; Achenbach, S.J.; Atkinson, E.J.; Khosla, S.; Melton, L.J., 3rd; Amin, S. Is vitamin D a determinant of muscle mass and strength? J. Bone Miner Res. 2011, 26, 2860–2871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Ham, J.O.; Lee, B.K. A positive association of vitamin D deficiency and sarcopenia in 50 year old women, but not men. Clin. Nutr. 2014, 33, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Brouwer-Brolsma, E.M.; Nienaber-Rousseau, C.; van Loon, L.J.; De Groot, L.C. Low vitamin D status is associated with reduced muscle mass and impaired physical performance in frail elderly people. Eur. J. Clin. Nutr. 2013, 67, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Gumieiro, D.N.; Murino Rafacho, B.P.; Buzati Pereira, B.L.; Cavallari, K.A.; Tanni, S.E.; Azevedo, P.S.; Polegato, B.F.; Mamede Zornoff, L.A.; Dinhane, D.I.; Innocenti Dinhane, K.G.; et al. Vitamin D serum levels are associated with handgrip strength but not with muscle mass or length of hospital stay after hip fracture. Nutrition 2015, 31, 931–934. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Unit | Men | Women | Sex Difference (p) | Total Participants |
|---|---|---|---|---|---|
| Subjects | [n (%)] | 126 (46.5) | 145 (53.5) | 0.25 | 271 |
| Age | [year] | 70.3 (6.9) | 70.3 (6.0) | 0.94 | 70.3 (6.4) |
| Height | [m] | 1.8 (0.1) | 1.6 (0.1) | <0.0001 | 1.7 (0.1) |
| Weight | [kg] | 85.3 (12.4) | 70.7 (11.3) | <0.0001 | 77.5 (13.9) |
| BMI | [kg/m2] | 27.6 (3.8) | 26.9 (4.1) | 0.14 | 27.2 (3.9) |
| Not overweight (BMI <25 kg/m2) | [n (%)] | 30 (23.8) | 54 (37.2) | 0.002 | 84 (31.0) |
| Overweight (BMI ≥25–29.99 kg/m2) | 76 (60.3) | 56 (38.6) | 132 (48.7) | ||
| Obese (BMI ≥30) | 20 (15.9) | 35 (24.2) | 55 (20.3) | ||
| Physical activity | [min MVPA/day] | 45.1 (22.8) | 38.0 (21.2) | 0.01 | 41.3 (22.2) |
| Smoking status | |||||
| Non-smoker | [n (%)] | 38 (30.2) | 98 (67.6) | <0.0001 | 136 (50.2) |
| Past smoker | 69 (54.7) | 41 (28.3) | 110 (40.6) | ||
| Current smoker | 19 (15.1) | 6 (4.1) | 25 (9.2) | ||
| Baseline 25-hydroxyvitamin D | [ng/mL] | 26.3 (11.3) | 28.2 (13.3) | 0.20 | 27.3 (12.4) |
| <10 | [n (%)] | 7 (5.6) | 10 (6.9) | 0.65 | 17 (6.3) |
| <20 | 38 (30.2) | 47 (32.4) | 0.69 | 85 (31.4) | |
| Glucose metabolism | |||||
| Glucose | [mmol/L] | 5.9 (1.4) | 5.3 (0.6) | <0.0001 | 5.6 (1.1) |
| Insulin | [mU/L] | 9.0 (8.8) | 7.0 (6.1) | 0.03 | 7.9 (7.5) |
| Beta cell function | [HOMA2%B] | 75.3 (38.5) | 71.7 (38.2) | 0.45 | 73.3 (38.3) |
| Insulin sensitivity | [HOMA2%S] | 143.3 (105.9) | 195.7 (129.5) | 0.0005 | 171.1 (121.6) |
| Insulin resistance | [HOMA2 IR] | 1.2 (1.2) | 0.9 (0.7) | 0.005 | 1.1 (1.0) |
| Prevalent diabetes | [n (%)] | 10 (8.0) | 0 (0) | 0.0004 | 10 (3.7) |
| DXA variables | |||||
| Total lean mass | [kg] | 59.3 (6.8) | 42.0 (4.8) | <0.0001 | 50.1 (10.4) |
| [%] | 70.0 (4.6) | 60.0 (5.3) | <0.0001 | 64.7 (7.0) | |
| Lean mass index | [kg/m2] | 19.2 (1.8) | 16.0 (1.6) | <0.0001 | 17.5 (2.3) |
| Appendicular lean mass | [kg] | 26.3 (5.1) | 17.7 (2.4) | <0.0001 | 21.7 (5.8) |
| [%] | 31.0 (4.5) | 25.3 (2.6) | <0.0001 | 27.9 (4.6) | |
| Appendicular lean mass index | [kg/m2] | 8.5 (1.5) | 6.7 (0.8) | <0.0001 | 7.6 (1.5) |
| Total fat mass | [kg] | 23.2 (7.0) | 27.1 (7.7) | <0.0001 | 25.3 (7.6) |
| [%] | 26.7 (4.9) | 37.7 (5.5) | <0.0001 | 32.6 (7.6) | |
| Fat mass index | [kg/m2] | 7.5 (2.3) | 10.3 (2.9) | <0.0001 | 9.0 (3.0) |
| Parameter | Q1 (4.7–17.5) (n = 67) | Q2 (17.6–26.0) (n = 69) | Q3 (26.1–34.8) (n = 67) | Q4 (34.9–62.5) (n = 68) |
|---|---|---|---|---|
| Fat mass index [kg/m2] | ||||
| LSM (95% CI) | 9.31 (8.77, 9.84) | 8.69 (8.17, 9.20) | 8.40 (7.87, 8.94) | 8.37 (7.88, 8.87) |
| p† | Ref | 0.28 | 0.049 | 0.04 |
| poverall‡ | 0.03 | |||
| ptrend linear | 0.65 | |||
| Appendicular lean mass index [kg/m2] | ||||
| LSM (95% CI) | 7.74 (7.54, 7.95) | 7.68 (7.48, 7.87) | 7.80 (7.59, 8.00) | 7.54 (7.35, 7.73) |
| p† | Ref | 0.96 | 0.98 | 0.46 |
| poverall‡ | 0.26 | |||
| ptrend linear | 0.06 |
| Parameter | Q1 (4.7–17.5) | Q2 (17.6–26.0) | Q3 (26.1–34.8) | Q4 (34.9–62.5) |
|---|---|---|---|---|
| Fasting glucose [mmol/L] | (n = 63) | (n = 66) | (n = 64) | (n = 67) |
| LSM (95% CI) | 5.46 (5.17, 5.75) a | 5.47 (5.21,5.74) a | 5.76 (5.48, 6.05) a | 5.54 (5.28, 5.81) a |
| p† | Ref | 1.00 | 0.36 | 0.97 |
| poverall‡ | 0.31 | |||
| ptrend linear | 0.44 | |||
| Fasting insulin [mU/L] | (n = 66) | (n = 69) | (n = 66) | (n = 56) |
| LSM (95% CI) | 7.40 (5.57, 9.23) a | 8.21 (6.49, 9.93) a | 8.33 (6.51, 10.16) a | 5.64 (3.93, 7.35) a |
| p† | Ref | 0.90 | 0.86 | 0.48 |
| poverall‡ | 0.09 | |||
| ptrend linear | 0.13 | |||
| Beta cell function [HOMA2%B] | (n = 63) | (n = 66) | (n = 63) | (n = 64) |
| LSM (95% CI) | 70.6 (60.7, 80.5) ab | 77.9 (68.7, 87.1) a | 69.8 (60.0, 79.5) ab | 59.6 (50.5, 68.7) b |
| p† | Ref | 0.65 | 1.00 | 0.34 |
| poverall‡ | 0.04 | |||
| ptrend linear | 0.03 | |||
| Insulin sensitivity [HOMA2%S] | (n = 63) | (n = 66) | (n = 63) | (n = 64) |
| LSM (95% CI) | 170.7 (141.1, 200.2) ab | 152.8 (125.4, 180.2) a | 192.6 (163.5, 221.8) ab | 215.3 (188.2, 242.5) b |
| p† | Ref | 0.78 | 0.66 | 0.10 |
| poverall‡ | 0.01 | |||
| ptrend linear | 0.004 |
| Q1 (4.7–17.5) | Q2 (17.6–26.0) | Q3 (26.1–34.8) | Q4 (34.9–62.5) | Total Participants | |
|---|---|---|---|---|---|
| Unadjusted model | |||||
| Insulin resistance (HOMA2 IR ≥ 1.8) | |||||
| n (%) | 15 (23.8) | 14 (21.2) | 12 (19.0) | 4 (6.3) | 45 |
| poverall† | 0.05 | ||||
| p‡ | 0.01 | ||||
| p§ | 0.02 | ||||
| Diabetes (fasting glucose >7.0 mmol/L) | |||||
| n (%) | 3 (4.8) | 2 (3.0) | 4 (6.3) | 1 (1.5) | 10 |
| poverall† | 0.57 | ||||
| p‡ | 0.31 | ||||
| p§ | 0.56 | ||||
| Adjusted model | |||||
| Insulin resistance (HOMA2 IR ≥ 1.8) | |||||
| % (95% CI) | 9.4 (3.8, 21.2) | 14.6 (7.2, 27.1) | 11.9 (5.3, 24.4) | 4.8 (1.6, 13.7) | |
| poverall† | 0.29 | ||||
| p‡ | 0.29 | ||||
| p§ | 0.06 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathieu, S.-V.; Fischer, K.; Dawson-Hughes, B.; Freystaetter, G.; Beuschlein, F.; Schietzel, S.; Egli, A.; Bischoff-Ferrari, H.A. Association between 25-Hydroxyvitamin D Status and Components of Body Composition and Glucose Metabolism in Older Men and Women. Nutrients 2018, 10, 1826. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121826
Mathieu S-V, Fischer K, Dawson-Hughes B, Freystaetter G, Beuschlein F, Schietzel S, Egli A, Bischoff-Ferrari HA. Association between 25-Hydroxyvitamin D Status and Components of Body Composition and Glucose Metabolism in Older Men and Women. Nutrients. 2018; 10(12):1826. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121826
Chicago/Turabian StyleMathieu, Svea-Vivica, Karina Fischer, Bess Dawson-Hughes, Gregor Freystaetter, Felix Beuschlein, Simeon Schietzel, Andreas Egli, and Heike A. Bischoff-Ferrari. 2018. "Association between 25-Hydroxyvitamin D Status and Components of Body Composition and Glucose Metabolism in Older Men and Women" Nutrients 10, no. 12: 1826. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121826