Glucose Response during the Night Is Suppressed by Wheat Albumin in Healthy Participants: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Consent to Participate
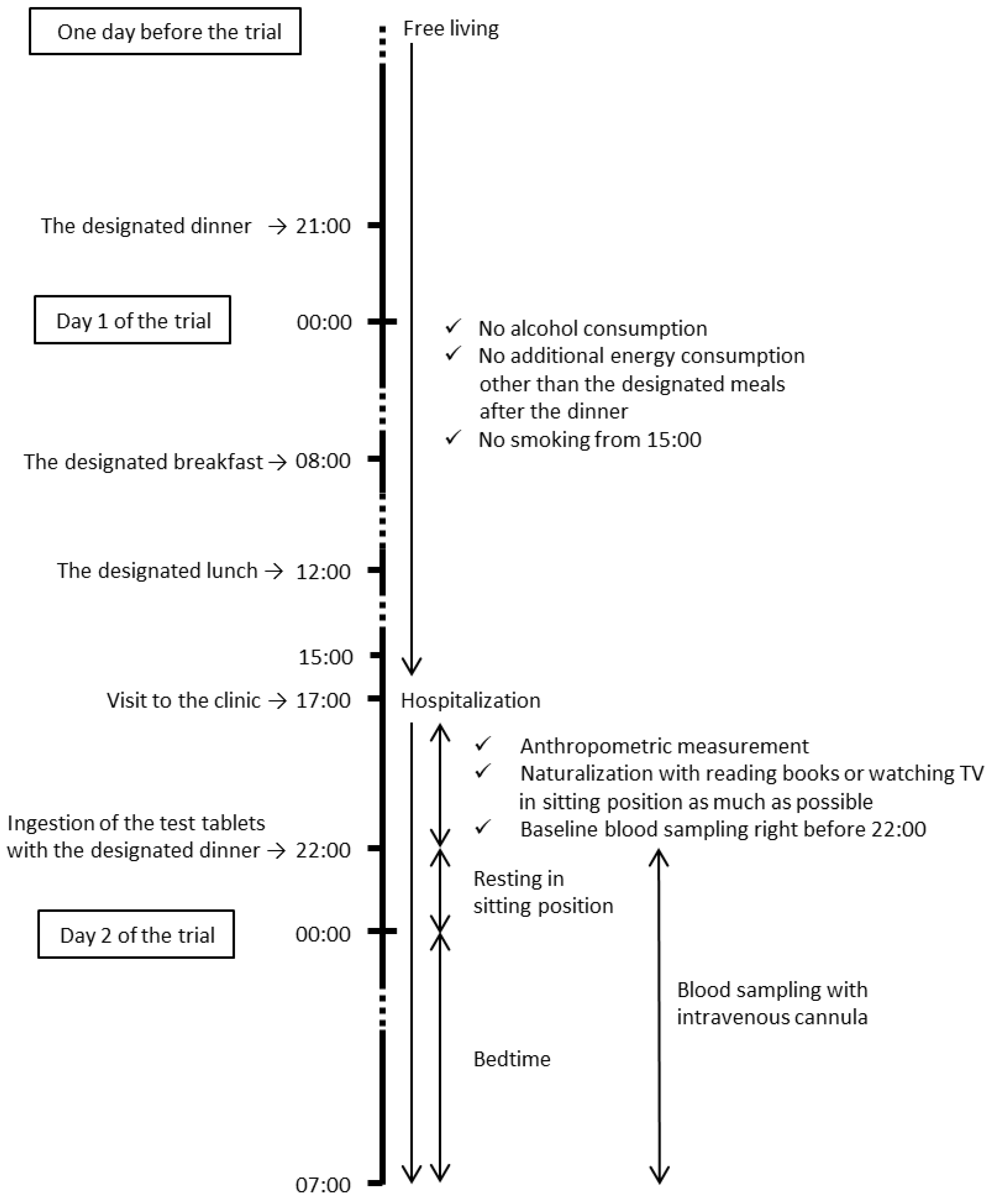
2.2. Study Design
2.3. Participants
2.4. Test Tablets and Meals
2.5. Laboratory Measurements
2.6. Statistics
3. Results
3.1. Characteristics of the Participants
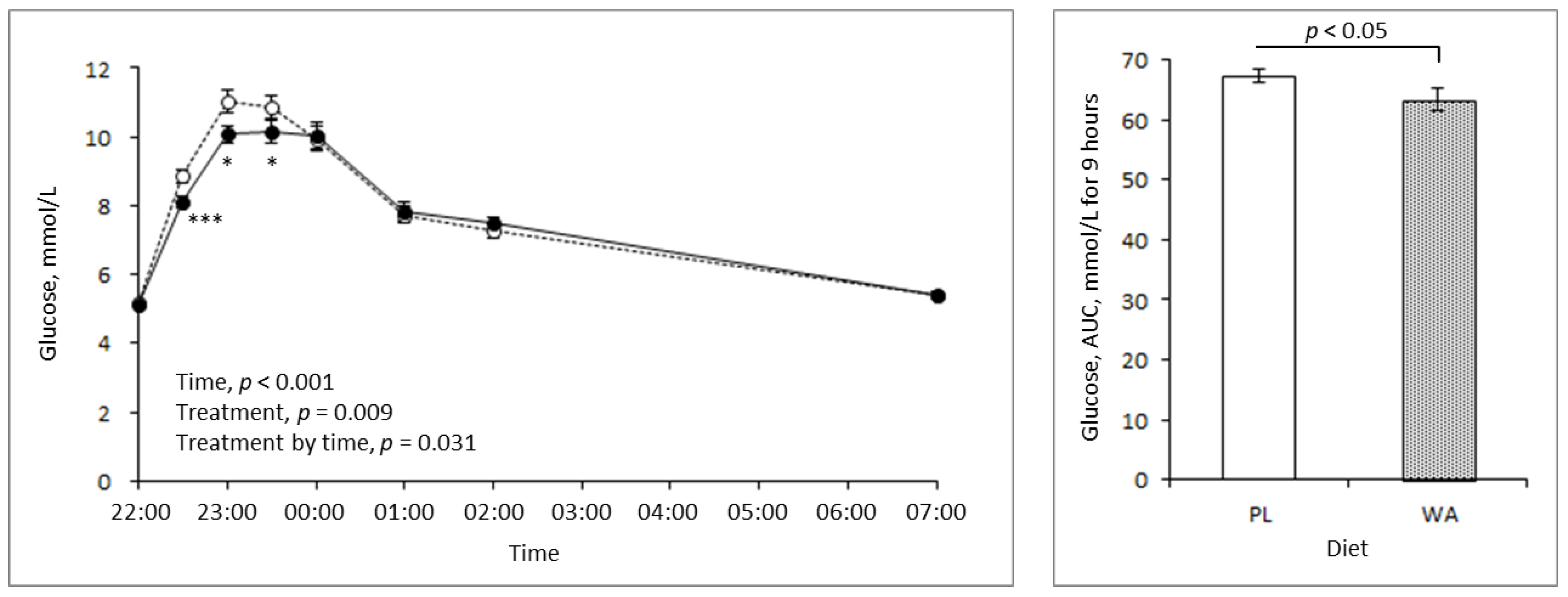
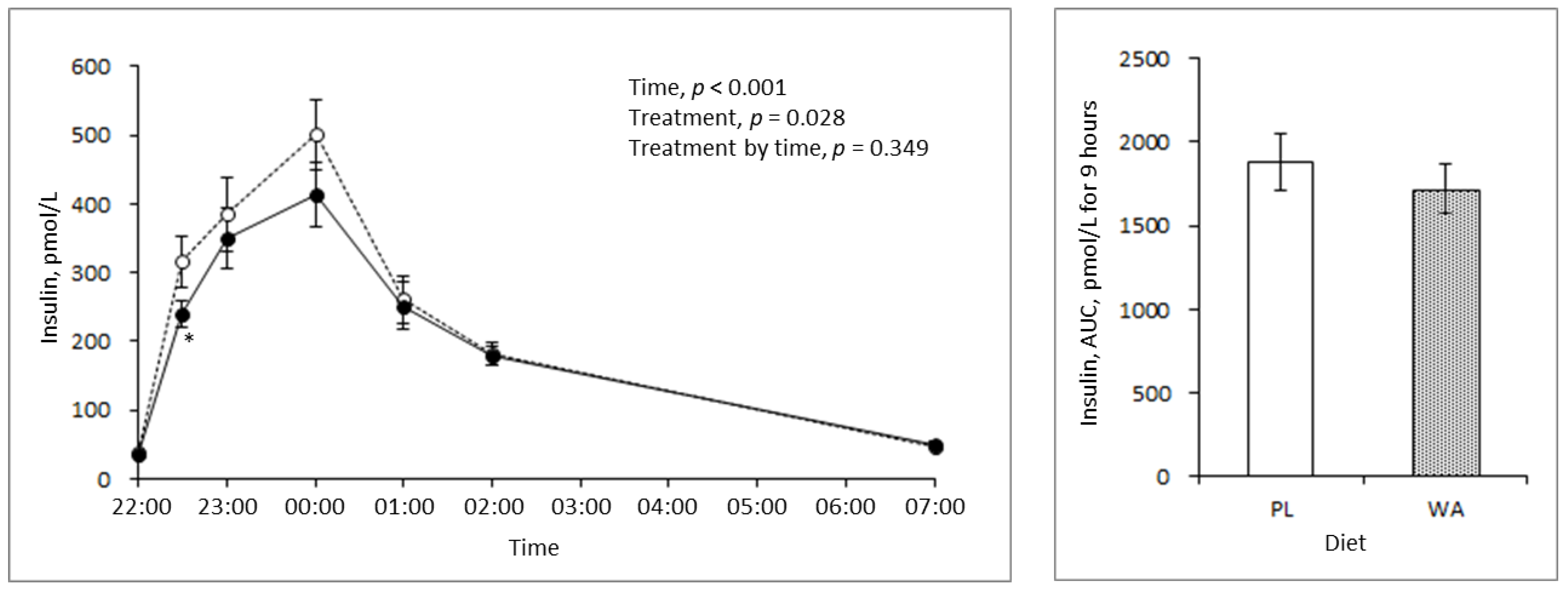
3.2. Effects of WA on Blood Glucose, Insulin, and Triglyceride Response during Night
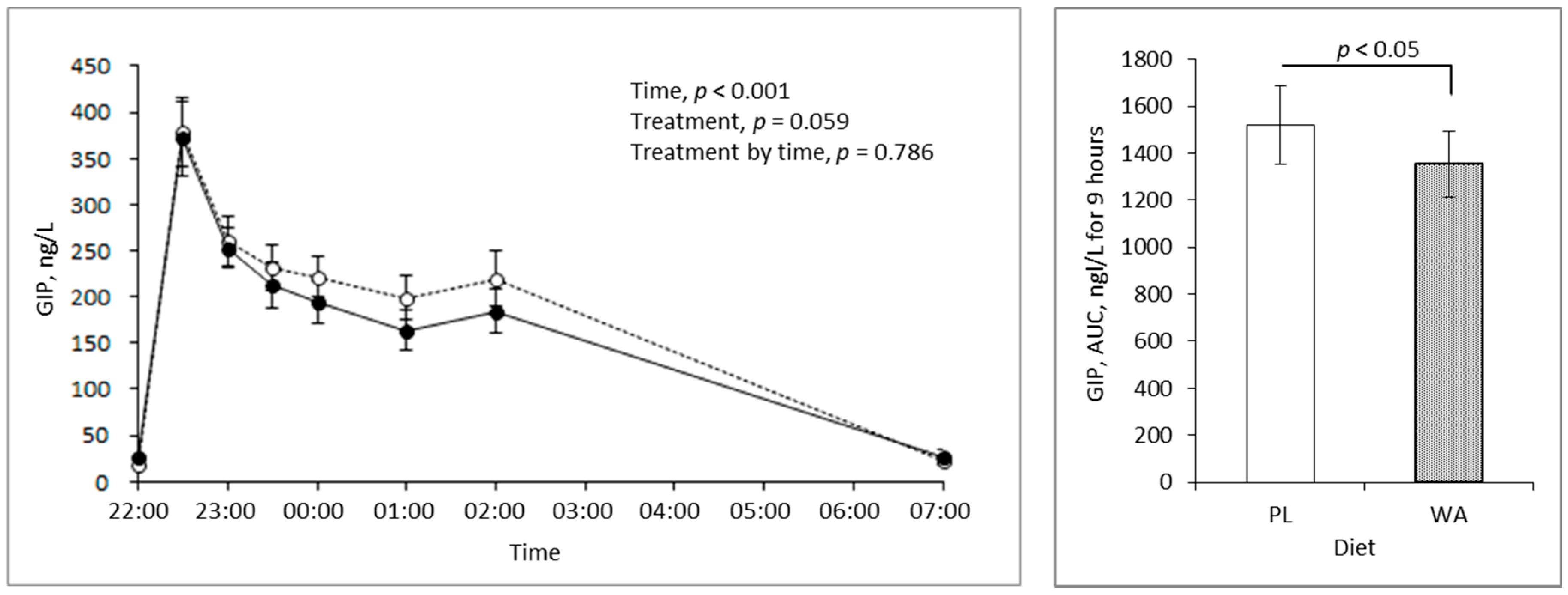
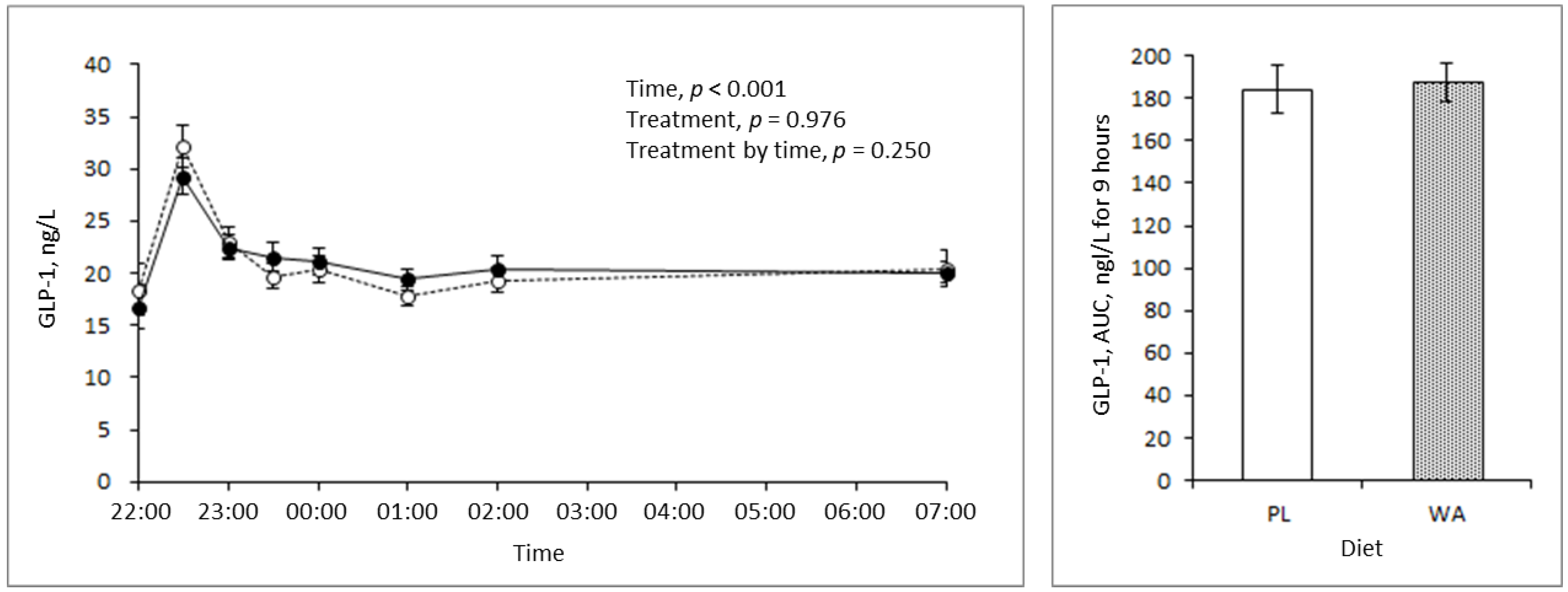
3.3. Effects of WA on Incretins during the Night
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Gerstein, H.C. Dysglycemia, not just diabetes, is a continuous risk factor for cardiovascular disease. Evid.-Based Cardiovasc. Med. 1997, 1, 87–88. [Google Scholar] [CrossRef]
- Punthakee, Z.; Werstuck, G.H.; Gerstein, H.C. Diabetes and cardiovascular disease: Explaining the relationship. Rev. Cardiovasc. Med. 2007, 8, 145–153. [Google Scholar]
- Ceriello, A.; Hanefeld, M.; Leiter, L.; Monnier, L.; Moses, A.; Owens, D.; Tajima, N.; Tuomilehto, J. The International Prandial Glucose Regulation (PGR) Study Group. Postprandial Glucose Regulation and Diabetic Complications. Arch. Intern. Med. 2004, 164, 2090–2095. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Hein, R.J.; Holman, R.R.; Sherwin, R.; Zinman, B. Management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy: A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2006, 29, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. The glucose triad and its role in comprehensive glycaemic control: Current status, future management. Int. J. Clin. Pract. 2010, 64, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. Guideline for Management of PostMeal Glucose in Diabetes; International Diabetes Federation: Brussels, Belgium, 2011. [Google Scholar]
- Jarrett, R.J.; Baker, I.A.; Keen, H.; Oakly, N.W. Diurnal variation in oral glucose tolerance, blood sugar, and plasma insulin levels in the morning, afternoon, and evening. Br. Med. J. 1972, 1, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.F.; Nestel, P.L. Diurnal variation in glucose tolerance and in insulin secretion in man. Diabetes 1973, 22, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.Z.; Well, J.R.; Rome, R.; Stimmler, L.; Jarrett, J.R. Diurnal variation in glucose tolerance and associated changes in plasma insulin, growth hormone, and esterified fatty acids. Br. Med. J. 1974, 1, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, N.J.; Puchulu, F.E.; Gagliardino, J.J.; Ruiz, M.; Llorens, J.M.; Ruiz, J.; Lamas, A.; De Miguel, R. Circadian variation of the blood glucose, plasma insulin, and human growth hormone levels in response to an oral glucose load in normal subjects. Diabetes 1974, 23, 132–137. [Google Scholar] [CrossRef]
- Whichelow, M.J.; Stuge, R.A.; Keen, H.; Jarrett, R.T.; Stimmler, L.; Grainger, S. Diurnal variation in response to intravenous glucose. Br. Med. J. 1974, 1, 488–491. [Google Scholar] [CrossRef]
- Sensi, S. Some aspects of circadian variation of carbohydrate metabolism and related hormones in man. Chronobiologia 1974, 1, 396–399. [Google Scholar] [PubMed]
- Jarrett, R.J.; Keen, H. Further observations on the diurnal variation in oral glucose tolerance. Br. Med. J. 1970, 4, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Baker, I.A.; Jarrett, R.J. Diurnal variation in the blood glucose and plasma insulin response to tolbutamide. Lancet 1972, 1, 945–947. [Google Scholar] [CrossRef]
- Gibson, T.; Jarrett, R.J. Diurnal variation in insulin sensitivity. Lancet 1972, 1, 947–948. [Google Scholar] [CrossRef]
- Kodama, T.; Miyazaki, T.; Kitamura, I.; Suzuki, Y.; Namba, Y.; Sakurai, J.; Torikai, Y.; Inoue, S. Effects of single and long-term administration of wheat albumin on blood glucose control: Randomized controlled clinical trials. Eur. J. Clin. Nutr. 2005, 59, 384–392. [Google Scholar] [CrossRef]
- Josse, R.G.; Chiasson, J.L.; Ryan, E.A.; Lau, D.C.W.; Ross, S.A.; Yale, J.F.; Leiter, L.A.; Maheux, P.; Tessier, D.; Wolever, T.M.S.; et al. Acarbose in the treatment of elderly patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2003, 59, 37–42. [Google Scholar] [CrossRef]
- Lu, Z.X.; Walker, K.Z.; Muir, J.G.; Mascara, T.; O’Dea, K. Arabinoxylan fiber, a byproduct of wheat flour processing, reduces the postprandial glucose response in normoglycemic subjects. Am. J. Clin. Nutr. 2000, 71, 1123–1128. [Google Scholar] [CrossRef] [Green Version]
- Maki, K.C.; Davidson, M.H.; Witchger, M.S.; Dicklin, M.R.; Subbaiah, P.V. Effects of high-fiber oat and wheat cereals on postprandial glucose and lipid responses in healthy men. Int. J. Vitam. Nutr. Res. 2007, 77, 347–356. [Google Scholar] [CrossRef]
- The University Hospital Medical Information Network (UMIN) Clinical Registry. Available online: http://www.umin.ac.jp/ctr/index.htm (accessed on 25 December 2018).
- Allen, K.V.; Frier, B.M. Nocturnal hypoglycemia: Clinical manifestations and therapeutic strategies toward prevention. Endocr. Pract. 2003, 9, 530–543. [Google Scholar] [CrossRef] [PubMed]
- Oshida, H.; Kutsuma, A.; Nakajima, K. Associations of eating a late-evening meal before bedtime with low serum amylase and unhealthy conditions. J. Diabetes Metab. Disord. 2013, 12, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Katayose, Y.; Tasaki, M.; Ogata, H.; Nakata, Y.; Tokuyama, K.; Satoh, M. Metabolic rate and fuel utilization during sleep assessed by whole-body indirect calorimetry. Metabolism 2009, 58, 920–926. [Google Scholar] [CrossRef]
- Zhou, H.; Yamada, Y.; Tsukiyama, K.; Miyawaki, K.; Hosokawa, M.; Nagashima, K.; Toyoda, K.; Naitoh, R.; Mizunoya, W.; Fushiki, T.; et al. Gastric inhibitory polypeptide modulates adiposity and fat oxidation under diminished insulin action. Biochem. Biophys. Res. Commun. 2005, 335, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Seino, Y.; Fukushima, M.; Yabe, D. GIP and GLP-1, the two incretin hormones: Similarities and differences. J. Diabetes Investig. 2010, 1, 8–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seino, Y.; Yabe, D. Glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1: Incretin actions beyond the pancreas. J. Diabetes Investig. 2013, 4, 108–130. [Google Scholar] [CrossRef] [PubMed]
- Shimotoyodome, A.; Suzuki, J.; Fukuoka, D.; Tokimitsu, I.; Hase, T. RS4-type resistant starch prevents high-fat diet-induced obesity via increased hepatic fatty acid oxidation and decreased postprandial GIP in C57BL/6J mice. Am. J. Physiol. Endocrinol. Metab. 2010, 298, E652–E662. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xue, J.; Yang, J.; Xie, M. Timed high-fat diet in the evening affects the hepatic circadian clock and PPARα-mediated lipogenic gene expressions in mice. Genes Nutr. 2013, 8, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimba, S.; Ogawa, T.; Hitosugi, S.; Ichihashi, Y.; Nakadaira, Y.; Kobayashi, M.; Tezuka, M.; Kosuge, Y.; Ishige, K.; Ito, Y.; et al. Deficient of a clock gene, brain and muscle Arnt-like protein-1 (BMAL1), induces dyslipidemia and ectopic fat formation. PLoS ONE 2011, 6, e25231. [Google Scholar] [CrossRef]
- Marcheva, B.; Ramsey, K.M.; Buhr, E.D.; Kobayashi, Y.; Su, H.; Ko, C.H.; Ivanova, G.; Omura, C.; Mo, S.; Vitaterna, M.H.; et al. Disruption of the clock components CLOCK and BMAL1 leads to hypoinsulinaemia and diabetes. Nature 2010, 466, 627–631. [Google Scholar] [CrossRef] [Green Version]
- King, D.P.; Zhao, Y.; Sangoram, A.M.; Wilsbacher, L.D.; Tanaka, M.; Antoch, M.P.; Steeves, T.D.; Vitaterna, M.H.; Kornhauser, J.M.; Lowrey, P.L.; et al. Positional cloning of the mouse circadian clock gene. Cell 1997, 89, 641–653. [Google Scholar] [CrossRef]
- Turek, F.W.; Joshu, C.; Kohsaka, A.; Lin, E.; Ivanova, G.; McDearmon, E.; Laposky, A.; Losee-Olson, S.; Easton, A.; Jensen, D.R.; et al. Obesity and metabolic syndrome in circadian Clock mutant mice. Science 2005, 308, 1043–1045. [Google Scholar] [CrossRef]
- Bunger, M.K.; Wilsbacher, L.D.; Moran, S.M.; Clendenin, C.; Radcliffe, L.A.; Hogenesch, J.B.; Simon, M.C.; Takahashi, J.S.; Bradfield, C.A. Mop3 is an essential component of the master circadian pacemaker in mammals. Cell 2000, 103, 1009–1017. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Number of participants (male/female) | 20 (20/0) |
| Age, years | 51 ± 1 |
| Body weight, kg | 75.8 ± 1.7 |
| Body mass index, kg/m2 | 26.0 ± 0.4 |
| Systolic blood pressure, mmHg | 116 ± 2 |
| Diastolic blood pressure, mmHg | 76 ± 2 |
| Glucose, mmol/L | 5.19 ± 0.05 |
| Insulin, pmol/L | 39 ± 4 |
| Triglyceride, mg/dL | 1.61 ± 0.16 |
| HbA1c, % | 5.6 ± 0.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, S.; Oishi, S.; Shudo, A.; Sugiura, Y.; Yasunaga, K. Glucose Response during the Night Is Suppressed by Wheat Albumin in Healthy Participants: A Randomized Controlled Trial. Nutrients 2019, 11, 187. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010187
Saito S, Oishi S, Shudo A, Sugiura Y, Yasunaga K. Glucose Response during the Night Is Suppressed by Wheat Albumin in Healthy Participants: A Randomized Controlled Trial. Nutrients. 2019; 11(1):187. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010187
Chicago/Turabian StyleSaito, Shinichiro, Sachiko Oishi, Aiko Shudo, Yoko Sugiura, and Koichi Yasunaga. 2019. "Glucose Response during the Night Is Suppressed by Wheat Albumin in Healthy Participants: A Randomized Controlled Trial" Nutrients 11, no. 1: 187. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010187