Effect of Tomato Nutrient Complex on Blood Pressure: A Double Blind, Randomized Dose–Response Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Materials
2.3. Procedure
2.4. Steady-State Bioavailability of Tomato Carotenoids TNC Dose–Response
2.5. Statistical Methods
3. Results
3.1. Demographics and Baseline Characteristics
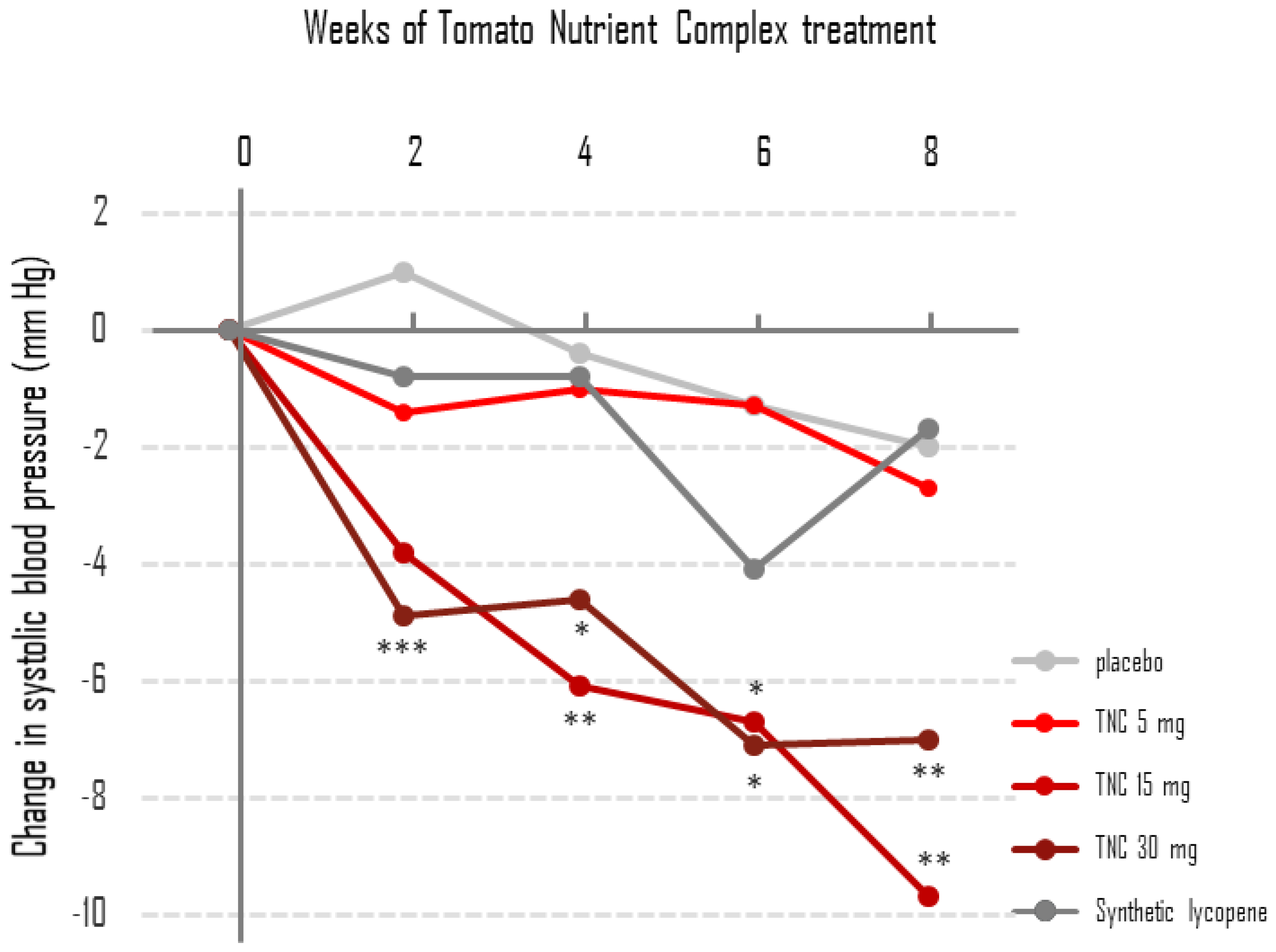
3.2. Changes in BP Values during the 8-Week Double-Blind Placebo-Controlled Treatment Phase
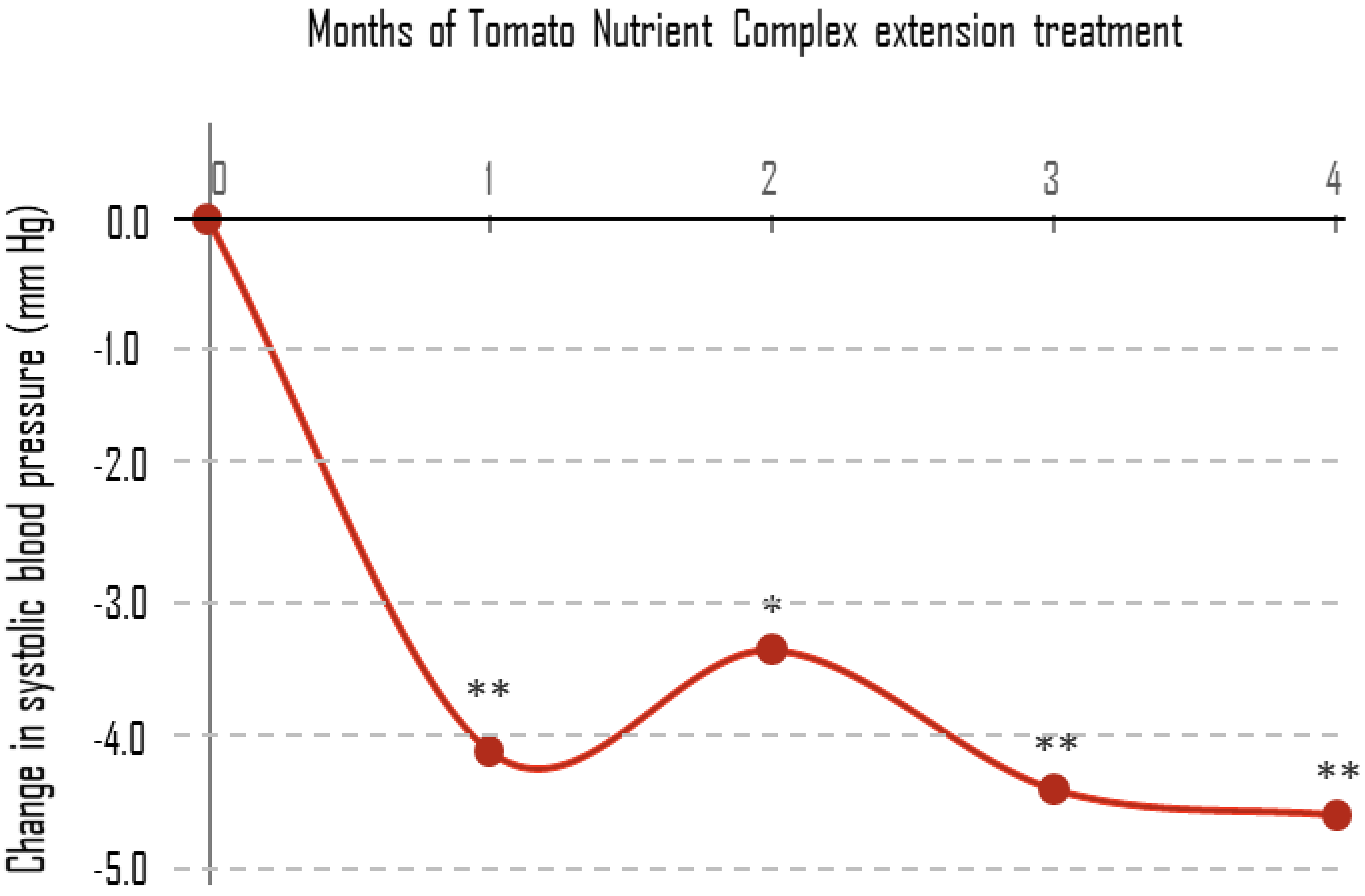
3.3. Changes in BP Values during the Single-Blind 16-Week Study Extension
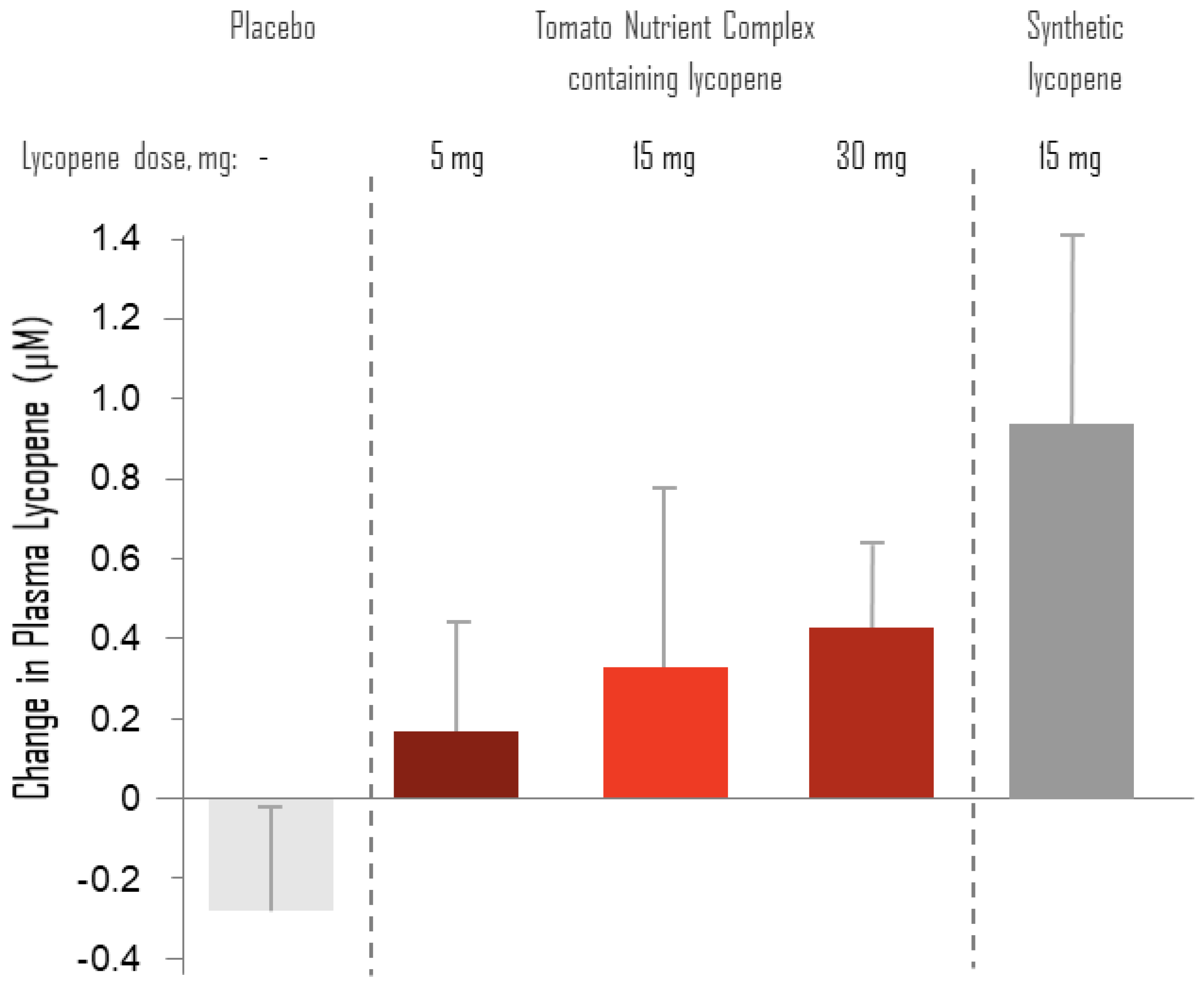
3.4. Changes from Baseline of Plasma Levels of Lycopene
3.5. Bioavailability of Tomato Carotenoids during 4 Weeks of Daily TNC Supplementation—A Dose– Response Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thies, F.; Masson, L.F.; Rudd, A.; Vaughan, N.; Tsang, C.; Brittenden, J.; Simpson, W.G.; Duthie, S.; Horgan, G.W.; Duthie, G. Effect of a tomato-rich diet on markers of cardiovascular disease risk in moderately overweight, disease-free, middle-aged adults: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Yeh, G.Y.; Davis, R.B.; Phillips, R.S. Use of complementary therapies in patients with cardiovascular disease. Am. J. Cardiol. 2006, 98, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The jnc 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Simons-Morton, D.; Vollmer, W.M.; Appel, L.J.; Conlin, P.R.; Ryan, D.H.; Ard, J.; Kennedy, B.M. Effects of dietary patterns on blood pressure: Subgroup analysis of the dietary approaches to stop hypertension (dash) randomized clinical trial. Arch. Intern. Med. 1999, 159, 285–293. [Google Scholar] [CrossRef]
- John, J.H.; Ziebland, S.; Yudkin, P.; Roe, L.S.; Neil, H.A.; Oxford, F.; Vegetable Study, G. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: A randomised controlled trial. Lancet 2002, 359, 1969–1974. [Google Scholar] [CrossRef]
- Engelhard, Y.N.; Gazer, B.; Paran, E. Natural antioxidants from tomato extract reduce blood pressure in patients with grade-1 hypertension: A double-blind, placebo-controlled pilot study. Am. Heart J. 2006, 151, 100. [Google Scholar] [CrossRef]
- Kim, J.Y.; Paik, J.K.; Kim, O.Y.; Park, H.W.; Lee, J.H.; Jang, Y.; Lee, J.H. Effects of lycopene supplementation on oxidative stress and markers of endothelial function in healthy men. Atherosclerosis 2011, 215, 189–195. [Google Scholar] [CrossRef]
- Ried, K.; Frank, O.R.; Stocks, N.P. Dark chocolate or tomato extract for prehypertension: A randomised controlled trial. BMC Complement. Altern. Med. 2009, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Paran, E.; Novack, V.; Engelhard, Y.N.; Hazan-Halevy, I. The effects of natural antioxidants from tomato extract in treated but uncontrolled hypertensive patients. Cardiovasc. Drugs Ther. 2009, 23, 145–151. [Google Scholar] [CrossRef]
- Hozawa, A.; Jacobs, D.R., Jr.; Steffes, M.W.; Gross, M.D.; Steffen, L.M.; Lee, D.H. Circulating carotenoid concentrations and incident hypertension: The coronary artery risk development in young adults (cardia) study. J. Hypertens. 2009, 27, 237–242. [Google Scholar] [CrossRef]
- Itsiopoulos, C.; Brazionis, L.; Kaimakamis, M.; Cameron, M.; Best, J.D.; O’Dea, K.; Rowley, K. Can the mediterranean diet lower hba1c in type 2 diabetes? Results from a randomized cross-over study. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 740–747. [Google Scholar] [CrossRef]
- Upritchard, J.E.; Sutherland, W.H.; Mann, J.I. Effect of supplementation with tomato juice, vitamin e, and vitamin c on ldl oxidation and products of inflammatory activity in type 2 diabetes. Diabetes Care 2000, 23, 733–738. [Google Scholar] [CrossRef]
- Paterson, E.; Gordon, M.H.; Niwat, C.; George, T.W.; Parr, L.; Waroonphan, S.; Lovegrove, J.A. Supplementation with fruit and vegetable soups and beverages increases plasma carotenoid concentrations but does not alter markers of oxidative stress or cardiovascular risk factors. J. Nutr. 2006, 136, 2849–2855. [Google Scholar] [CrossRef]
- Ried, K.; Fakler, P. Protective effect of lycopene on serum cholesterol and blood pressure: Meta-analyses of intervention trials. Maturitas 2011, 68, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, J. Lycopene supplement and blood pressure: An updated meta-analysis of intervention trials. Nutrients 2013, 5, 3696–3712. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 acc/aha/aapa/abc/acpm/ags/apha/ash/aspc/nma/pcna guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar]
- Walfisch, Y.; Walfisch, S.; Agbaria, R.; Levy, J.; Sharoni, Y. Lycopene in serum, skin and adipose tissues after tomato-oleoresin supplementation in patients undergoing haemorrhoidectomy or peri-anal fistulotomy. Br. J. Nutr. 2003, 90, 759–766. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, S.; Mathur, S.; Basu, A.; Aung, H.H.; Vasu, V.T.; Meyers, S.; Jialal, I. A dose-response study on the effects of purified lycopene supplementation on biomarkers of oxidative stress. J. Am. Coll. Nutr. 2008, 27, 267–273. [Google Scholar] [CrossRef]
- Linnewiel-Hermoni, K.; Khanin, M.; Danilenko, M.; Zango, G.; Amosi, Y.; Levy, J.; Sharoni, Y. The anti-cancer effects of carotenoids and other phytonutrients resides in their combined activity. Arch. Biochem. Biophys. 2015, 572, 28–35. [Google Scholar] [CrossRef]
- Aust, O.; Stahl, W.; Sies, H.; Tronnier, H.; Heinrich, U. Supplementation with tomato-based products increases lycopene, phytofluene, and phytoene levels in human serum and protects against uv-light-induced erythema. Int. J. Vitam Nutr. Res. 2005, 75, 54–60. [Google Scholar] [CrossRef]
- Di Tomo, P.; Canali, R.; Ciavardelli, D.; Di Silvestre, S.; De Marco, A.; Giardinelli, A.; Pipino, C.; Di Pietro, N.; Virgili, F.; Pandolfi, A. Beta-carotene and lycopene affect endothelial response to tnf-alpha reducing nitro-oxidative stress and interaction with monocytes. Mol. Nutr. Food Res. 2012, 56, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Ben-Dor, A.; Steiner, M.; Gheber, L.; Danilenko, M.; Dubi, N.; Linnewiel, K.; Zick, A.; Sharoni, Y.; Levy, J. Carotenoids activate the antioxidant response element transcription system. Mol. Cancer Ther. 2005, 4, 177–186. [Google Scholar] [PubMed]
- Linnewiel, K.; Ernst, H.; Caris-Veyrat, C.; Ben-Dor, A.; Kampf, A.; Salman, H.; Danilenko, M.; Levy, J.; Sharoni, Y. Structure activity relationship of carotenoid derivatives in activation of the electrophile/antioxidant response element transcription system. Free Radic. Biol. Med. 2009, 47, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Khachik, F.; Goli, M.B.; Beecher, G.R.; Holden, J.; Lusby, W.R.; Tenorio, M.D.; Barrera, M.R. Effect of food preparation on qualitative and quantitative distribution of major carotenoid constituents of tomatoes and several green vegetables. J. Agric. Food Chem. 1992, 40, 390–398. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | TNC 5 mg | TNC 15 mg | TNC 30 mg | Synthetic Lycopene 15 mg | Placebo | All |
|---|---|---|---|---|---|---|
| Age (years) 1 | 53.5 ± 8.0 (12) | 54.0 ± 8.6 (12) | 51.0 ± 10.1 (13) | 52.1 ± 8.4 (12) | 51.8 ± 6.3 (12) | 52.4 ± 8.2 (61) |
| Males (%) | 66.7% (8) | 75.0% (9) | 69.2% (9) | 66.7% (8) | 83.3% (10) | 72.1% (44) |
| Females (%) | 33.3% (4) | 25.0% (3) | 30.8 (4) | 33.3% (4) | 16.7% (2) | 27.9% (17) |
| SBP (mmHg) 1 | 133.6 ± 7.8 (12) | 137.4 ± 5.6 (12) | 136.4 ± 7.8 (13) | 132.8 ± 9.3 (12) | 135.7 ± 6.0 (12) | 135.2 ± 7.4 (61) |
| DBP (mmHg) 1 | 82.9 ± 9.3 (12) | 83.8 ± 6.3 (12) | 77.5 ± 21 (13) | 82.3 ± 6.1 (12) | 83.7 ± 8.7 (12) | 82.0 ± 11.7 (61) |
| Plasma lycopene (µM) | 0.97 ± 0.49 (7) | 1.55 ± 0.86 (7) | 0.80 ± 0.74 (10) | 0.91 ± 0.95 (8) | 1.01 ± 1.24 (10) | 0.93 ± 0.68 (42) |
| TG (mg/dL) | 152.0 ± 70.4 (11) | 164.3 ± 65.3 (10) | 124.5 ± 75.3 (12) | 115.1 ± 50.5 (10) | 166.0 ± 103.1 (12) | |
| HDL chol (mg/dL) | 52.0 ± 12.2 (10) | 49.5 ± 10.1 (10) | 54.4 ± 10.0 (12) | 59.1 ± 18.2 (10) | 52.1 ± 11.7 (11) | |
| LDL chol (mg/dL) | 142.1 ± 34.6 (10) | 107.4 ± 26.0 (9) | 104.8 ± 31.1 (11) | 134.2 ± 29.5 (10) | 112.9 ± 30.1 (9) |
| SBP 1 (mmHg) | TNC 5 mg | TNC 15 mg | TNC 30 mg | Synthetic Lycopene 15 mg | Placebo |
|---|---|---|---|---|---|
| Baseline | 133.6 ± 7.8 (12) | 137.4 ± 5.6 (12) | 136.4 ± 7.8 (13) | 132.8 ± 9.3 (12) | 135.7 ± 6.0 (12) |
| Week 2 | 132.7 ± 8.9 (10) | 133.7 ± 5.3 (12) | 131.5 ± 8.0 (13) | 133.2 ± 8.9 (11) | 137.1 ± 10.3 (11) |
| Week 4 | 133.1 ± 9.2 (9) | 130.7 ± 4.7 (10) | 131.7 ± 10.5 (11) | 133.4 ± 7.2 (9) | 134.5 ± 8.7 (10) |
| Week 6 | 132.8 ± 9.2 (9) | 130.2 ± 10.6 (9) | 129.9 ± 13.9 (10) | 130.1 ± 9.8 (9) | 133.7 ± 9.9 (9) |
| Week 8 | 131.4 ± 7.7 (9) | 127.2 ± 6.3 (9) | 130.0 ± 13.0 (10) | 132.6 ± 5.1 (9) | 133.0 ± 6.7 (9) |
| DBP 1 (mmHg) | TNC 5 mg | TNC 15 mg | TNC 30 mg | Synthetic Lycopene 15 mg | Placebo |
|---|---|---|---|---|---|
| Baseline | 82.9 ± 9.3 (12) | 83.8 ± 6.3 (12) | 77.5 ± 21 (13) | 82.3 ± 6.1 (12) | 83.7 ± 8.7 (12) |
| Week 2 | 81.4 ± 8.2 (10) | 80.7 ± 7.1 (12) | 80.5 ± 7.9 (13) | 84.5 ± 6.1 (11) | 84.2 ± 8.2 (11) |
| Week 4 | 82.8 ± 9.9 (9) | 81.3 ± 3.9 (10) | 82.6 ± 9.1 (11) | 84.9 ± 6.6 (9) | 83.0 ± 8.8 (10) |
| Week 6 | 82.6 ± 6.4 (9) | 78.8 ± 7.5 (9) | 72.3 ± 23 (10) | 81.6 ± 6.0 (9) | 83.2 ± 7.9 (9) |
| Week 8 | 81.7 ± 7.9 (9) | 78.6 ± 7.9 (9) | 74.4 ± 23 (10) | 84.6 ± 5.0 (9) | 85.3 ± 7.0 (9) |
| DBP (mmHg) | TNC 5 mg | TNC 15 mg | TNC 30 mg | Synthetic Lycopene 15 mg | Placebo |
|---|---|---|---|---|---|
| Mean ± SD (p 1) | Mean ± SD (p) | Mean ± SD (p) | Mean ± SD (p) | Mean ± SD (p) | |
| Week 2 | −2.9 ± 7.7 (0.265) | −3.2 ± 4.5 (0.032) | 3.0 ± 4.9 (0.672) | 0.9 ± 2.9 (0.331) | 0.0 ± 5.0 (1.000) |
| Week 4 | −0.9 ± 5.1 (0.613) | −1.9 ± 5.1 (0.268) | 6.8 ± 7.0 (0.422) | 1.2 ± 4.6 (0.449) | −0.4 ± 8.6 (0.887) |
| Week 6 | −1.1 ± 5.8 (0.582) | −3.9 ± 6.5 (0.112) | −3.5 ± 5.9 (0.092) | −2.1 ± 4.5 (0.198) | −1.4 ± 9.8 (0.671) |
| Week 8 | −2.0 ± 6.3 (0.371) | −4.1 ± 5.0 (0.038) | −1.4 ± 5.7 (0.454) | 0.9 ± 5.6 (0.645) | 0.7 ± 5.8 (0.740) |
| SBP (mmHg) 1 | Change of SBP 1 from Baseline (mmHg) | p-Value for Change | DBP (mmHg) 1 | Change of DBP 1 from Baseline (mmHg) | p-Value for Change | |
|---|---|---|---|---|---|---|
| Baseline | 135.1 ± 8.76 | 85.1 ± 6.6 | ||||
| Month 1 | 130.9 ± 8.6 | −4.2 ± 6.5 | 0.0024 | 84.3 ± 6.2 | −0.9 ± 5.7 | 0.422 |
| Month 2 | 131.7 ± 10 | −3.5 ± 7.4 | 0.0211 | 81.6 ± 15.5 | −3.6 ± 15.8 | 0.252 |
| Month 3 | 130.6 ± 8.8 | −4.5 ± 7.0 | 0.0024 | 82.7 ± 7.7 | −2.4 ± 6.3 | 0.056 |
| Month 4 | 130.4 ± 10.9 | −4.7 ±6.7 | 0.0012 | 83.9 ± 7.3 | −1.4 ± 4.3 | 0.362 |
| SBP 1 (mmHg) | TNC 5 mg | TNC 15 mg | TNC 30 mg | Synthetic Lycopene 15 mg | Placebo |
|---|---|---|---|---|---|
| Baseline | 0.97 ± 0.49 (7) | 1.55 ± 0.86 (7) | 0.80 ± 0.74 (9) | 0.91 ± 0.95 (7) | 1.01 ± 1.24 (9) |
| Week 8 | 1.13 ± 0.97 (7) | 1.89 ± 1.22 (7) | 1.23 ±1.07 (9) | 1.84 ± 1.14 (7) | 0.72 ± 0.72 (9) |
| Carotenoid Plasma Concentration (µM) | Baseline Mean ± SD | Week 2 Mean ± SD (p) 1 | Week 3 Mean ± SD (p) 1 | Week 4 Mean ± SD (p) 1 |
|---|---|---|---|---|
| Lycopene | ||||
| TNC 2 mg 2 | 1.021 ± 0.437 | 1.483 ± 0.481 (0.001) | 1.354 ± 0.408 (0.009) | 1.656 ± 0.537 (<0.000x) |
| TNC 5 mg 2 | 1.149 ± 0.322 | 1.629 ± 0.444 (<0.000x) | 1.677 ± 0.470 (<0.000x) | 1.767 ± 0.473 (<0.000x) |
| TNC 15 mg 2 | 1.036 ± 0.398 | 1.794 ± 0.453 (<0.000x) | 1.754 ± 0.449 (<0.000x) | 2.008 ± 0.627 (<0.000x) |
| Phytofluene | ||||
| TNC 2 mg 2 | 0.310 ± 0.147 | 0.382 ± 0.211 (0.171) | 0.300 ± 0.126 (0.805) | 0.398 ± 0.242 (0.128) |
| TNC 5 mg 2 | 0.354 ± 0.130 | 0.429 ± 0.190 (0.120) | 0.456 ± 0.201 (0.046) | 0.530 ± 0.263 (0.005) |
| TNC 15 mg 2 | 0.270 ± 0.111 | 0.503 ± 0.235 (<0.000x) | 0.536 ± 0.228 (<0.000x) | 0.650 ± 0.275 (<0.000x) |
| Phytoene | ||||
| TNC 2 mg 2 | 0.057 ± 0.040 | 0.073 ± 0.060 (0.300) | 0.059 ± 0.037 (0.868) | 0.091 ± 0.061 (0.028) |
| TNC 5 mg 2 | 0.046 ± 0.032 | 0.096 ± 0.050 (<0.000x) | 0.092 ± 0.057 (0.001) | 0.124 ± 0.058 (<0.000x) |
| TNC 15 mg 2 | 0.048 ± 0.031 | 0.133 ± 0.062 (<0.000x) | 0.127 ± 0.068 (<0.000x) | 0.158 ± 0.091 (<0.000x) |
| β-carotene | ||||
| TNC 2 mg 2 | 0.842 ± 0.391 | 0.975 ± 0.484 (0.289) | 0.872 ± 0.486 (0.811) | 0.998 ± 0.502 (0.224) |
| TNC 5 mg 2 | 0.947 ± 0.598 | 0.954 ± 0.580 (0.965) | 0.919 ± 0.473 (0.866) | 1.037 ± 0.533 (0.590) |
| TNC 15 mg 2 | 0.885 ± 0.534 | 0.968 ± 0.609 (0.618) | 0.970 ± 0.553 (0.587) | 1.057 ± 0.631 (0.315) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolak, T.; Sharoni, Y.; Levy, J.; Linnewiel-Hermoni, K.; Stepensky, D.; Paran, E. Effect of Tomato Nutrient Complex on Blood Pressure: A Double Blind, Randomized Dose–Response Study. Nutrients 2019, 11, 950. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11050950
Wolak T, Sharoni Y, Levy J, Linnewiel-Hermoni K, Stepensky D, Paran E. Effect of Tomato Nutrient Complex on Blood Pressure: A Double Blind, Randomized Dose–Response Study. Nutrients. 2019; 11(5):950. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11050950
Chicago/Turabian StyleWolak, Talia, Yoav Sharoni, Joseph Levy, Karin Linnewiel-Hermoni, David Stepensky, and Esther Paran. 2019. "Effect of Tomato Nutrient Complex on Blood Pressure: A Double Blind, Randomized Dose–Response Study" Nutrients 11, no. 5: 950. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11050950