Effects of Long-Term Physical Activity and Diet on Skin Glycation and Achilles Tendon Structure

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Questionnaire
2.4. Skin Autofluorescence
2.5. Ultrasonography
2.6. Statistics
3. Results
3.1. Participant Characteristics
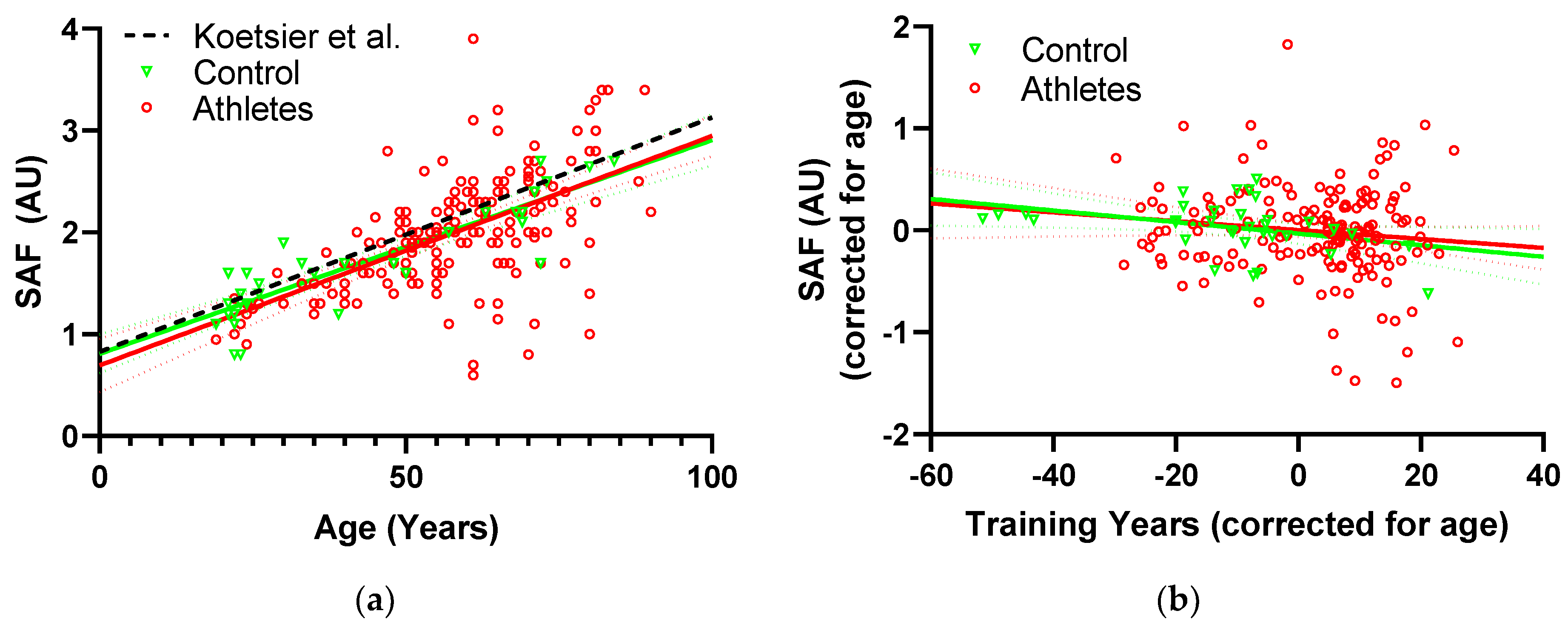
3.2. SAF
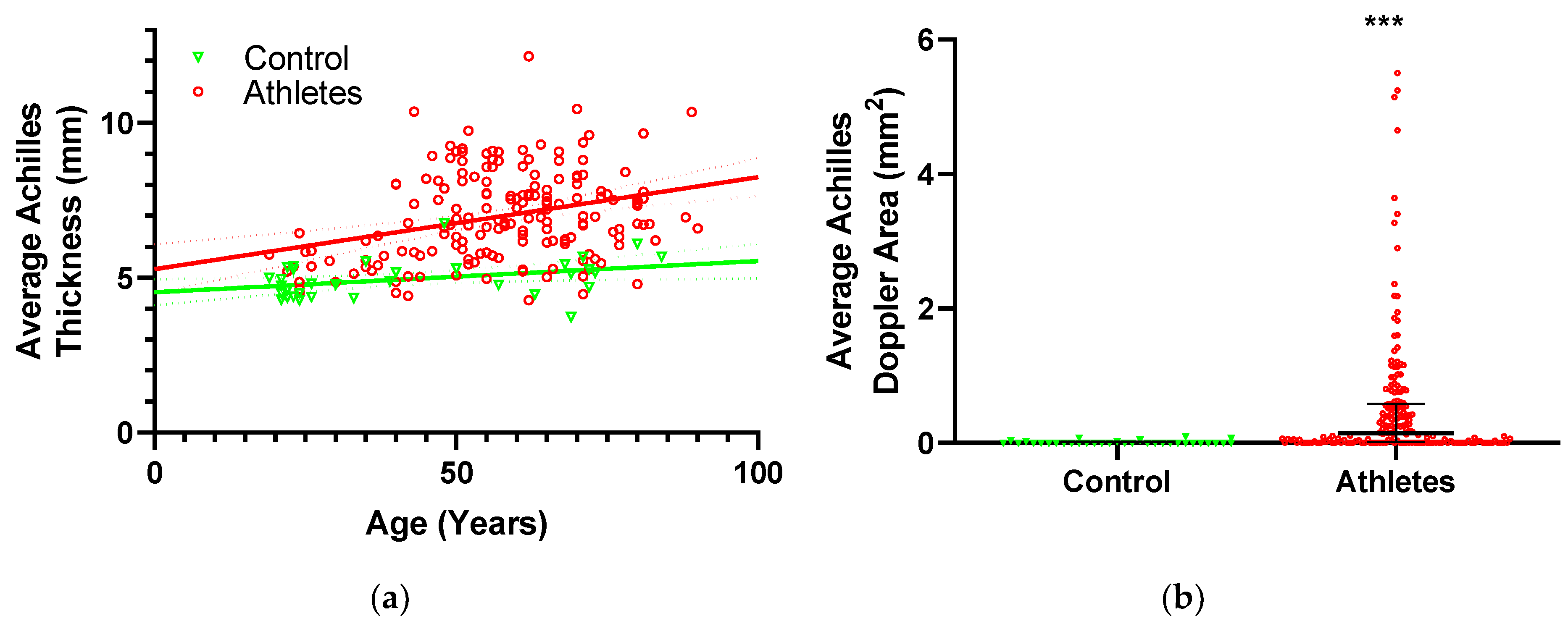
3.3. Tendon Structure
4. Discussion
4.1. SAF and Diet
4.2. SAF, Exercise and Aging
4.3. SAF and Biometrics
4.4. Tendon Structure, SAF and Aging
4.5. Tendon Structure and Diet
4.6. Tendon Structure and Exercise
4.7. Tendon Structure and Biometrics
4.8. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Monnier, V.M.; Mustata, G.T.; Biemel, K.L.; Reihl, O.; Lederer, M.O.; Zhenyu, D.; Sell, D.R. Cross-linking of the extracellular matrix by the maillard reaction in aging and diabetes: An update on “a puzzle nearing resolution”. Ann. N. Y. Acad. Sci. 2005, 1043, 533–544. [Google Scholar] [CrossRef]
- Meerwaldt, R.; Graaff, R.; Oomen, P.H.N.; Links, T.P.; Jager, J.J.; Alderson, N.L.; Thorpe, S.R.; Baynes, J.W.; Gans, R.O.B.; Smit, A.J. Simple non-invasive assessment of advanced glycation endproduct accumulation. Diabetologia 2004, 47, 1324–1330. [Google Scholar] [CrossRef] [Green Version]
- Sell, D.R.; Monnier, V.M. Molecular basis of arterial stiffening: Role of glycation-a mini-review. Gerontology 2012, 58, 227–237. [Google Scholar] [CrossRef]
- Komi, P.V.; Fukashiro, S.; Jarvinen, M. Biomechanical loading of Achilles tendon during normal locomotion. Clin. Sports Med. 1992, 11, 521–531. [Google Scholar]
- Fukashiro, S.; Komi, P.V.; Jarvinen, M.; Miyashita, M. In Vivo Achilles tendon loading during jumping in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 71, 453–458. [Google Scholar] [CrossRef]
- Heinemeier, K.M.; Schjerling, P.; Heinemeier, J.; Magnusson, S.P.; Kjaer, M. Lack of tissue renewal in human adult Achilles tendon is revealed by nuclear bomb (14)C. FASEB J. 2013, 27, 2074–2079. [Google Scholar] [CrossRef]
- Kujala, U.M.; Sarna, S.; Kaprio, J. Cumulative incidence of achilles tendon rupture and tendinopathy in male former elite athletes. Clin. J. Sport Med. 2005, 15, 133–135. [Google Scholar] [CrossRef]
- De Jonge, S.; van den Berg, C.; de Vos, R.J.; van der Heide, H.J.; Weir, A.; Verhaar, J.A.; Bierma-Zeinstra, S.M.; Tol, J.L. Incidence of midportion Achilles tendinopathy in the general population. Br. J. Sports Med. 2011, 45, 1026–1028. [Google Scholar] [CrossRef] [Green Version]
- Gautieri, A.; Passini, F.S.; Silvan, U.; Guizar-Sicairos, M.; Carimati, G.; Volpi, P.; Moretti, M.; Schoenhuber, H.; Redaelli, A.; Berli, M.; et al. Advanced glycation end-products: Mechanics of aged collagen from molecule to tissue. Matrix Biol. 2017, 59, 95–108. [Google Scholar] [CrossRef] [Green Version]
- James, V.J.; Delbridge, L.; McLennan, S.V.; Yue, D.K. Use of X-ray diffraction in study of human diabetic and aging collagen. Diabetes 1991, 40, 391–394. [Google Scholar] [CrossRef]
- Li, Y.; Fessel, G.; Georgiadis, M.; Snedeker, J.G. Advanced glycation end-products diminish tendon collagen fiber sliding. Matrix Biol. 2013, 32, 169–177. [Google Scholar] [CrossRef]
- Fessel, G.; Li, Y.; Diederich, V.; Guizar-Sicairos, M.; Schneider, P.; Sell, D.R.; Monnier, V.M.; Snedeker, J.G. Advanced glycation end-products reduce collagen molecular sliding to affect collagen fibril damage mechanisms but not stiffness. PLoS ONE 2014, 9, e110948. [Google Scholar] [CrossRef]
- Grasa, J.; Calvo, B.; Delgado-Andrade, C.; Navarro, M.P. Variations in tendon stiffness due to diets with different glycotoxins affect mechanical properties in the muscle-tendon unit. Ann. Biomed. Eng. 2013, 41, 488–496. [Google Scholar] [CrossRef]
- Eriksen, C.; Svensson, R.B.; Scheijen, J.; Hag, A.M.F.; Schalkwijk, C.; Praet, S.F.E.; Schjerling, P.; Kjaer, M.; Magnusson, S.P.; Couppe, C. Systemic stiffening of mouse tail tendon is related to dietary advanced glycation end products but not high-fat diet or cholesterol. J. Appl. Physiol. 2014, 117, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, E.A.; Schaible, E.; Bale, H.; Barth, H.D.; Tang, S.Y.; Reichert, P.; Busse, B.; Alliston, T.; Ager, J.W., 3rd; Ritchie, R.O. Age-related changes in the plasticity and toughness of human cortical bone at multiple length scales. Proc. Natl. Acad. Sci. USA 2011, 108, 14416–14421. [Google Scholar] [CrossRef] [Green Version]
- Couppe, C.; Svensson, R.B.; Grosset, J.-F.; Kovanen, V.; Nielsen, R.H.; Olsen, M.R.; Larsen, J.O.; Praet, S.F.E.; Skovgaard, D.; Hansen, M.; et al. Life-long endurance running is associated with reduced glycation and mechanical stress in connective tissue. Age 2014, 36, 9665. [Google Scholar] [CrossRef]
- Couppe, C.; Svensson, R.B.; Kongsgaard, M.; Kovanen, V.; Grosset, J.-F.; Snorgaard, O.; Bencke, J.; Larsen, J.O.; Bandholm, T.; Christensen, T.M.; et al. Human Achilles tendon glycation and function in diabetes. J. Appl. Physiol. 2016, 120, 130–137. [Google Scholar] [CrossRef]
- Craig, M.E.; Duffin, A.C.; Gallego, P.H.; Lam, A.; Cusumano, J.; Hing, S.; Donaghue, K.C. Plantar fascia thickness, a measure of tissue glycation, predicts the development of complications in adolescents with type 1 diabetes. Diabetes Care 2008, 31, 1201–1206. [Google Scholar] [CrossRef]
- D’Ambrogi, E.; Giurato, L.; D’Agostino, M.A.; Giacomozzi, C.; Macellari, V.; Caselli, A.; Uccioli, L. Contribution of plantar fascia to the increased forefoot pressures in diabetic patients. Diabetes Care 2003, 26, 1525–1529. [Google Scholar] [CrossRef]
- Sell, D.R.; Sun, W.; Gao, X.; Strauch, C.; Lachin, J.M.; Cleary, P.A.; Genuth, S.; Group, D.E.R.; Monnier, V.M. Skin collagen fluorophore LW-1 versus skin fluorescence as markers for the long-term progression of subclinical macrovascular disease in type 1 diabetes. Cardiovasc. Diabetol. 2016, 15, 30. [Google Scholar] [CrossRef] [Green Version]
- Orchard, T.J.; Lyons, T.J.; Cleary, P.A.; Braffett, B.H.; Maynard, J.; Cowie, C.; Gubitosi-Klug, R.A.; Way, J.; Anderson, K.; Barnie, A.; et al. The association of skin intrinsic fluorescence with type 1 diabetes complications in the DCCT/EDIC study. Diabetes Care 2013, 36, 3146–3153. [Google Scholar] [CrossRef]
- Noordzij, M.J.; Lefrandt, J.D.; Loeffen, E.A.; Saleem, B.R.; Meerwaldt, R.; Lutgers, H.L.; Smit, A.J.; Zeebregts, C.J. Skin autofluorescence is increased in patients with carotid artery stenosis and peripheral artery disease. Int. J. Cardiovasc. Imaging 2012, 28, 431–438. [Google Scholar] [CrossRef]
- DeChristopher, L.R. Perspective: The Paradox in Dietary Advanced Glycation End Products Research-The Source of the Serum and Urinary Advanced Glycation End Products Is the Intestines, Not the Food. Adv. Nutr. 2017, 8, 679–683. [Google Scholar] [CrossRef]
- Uribarri, J.; Cai, W.; Ramdas, M.; Goodman, S.; Pyzik, R.; Chen, X.; Zhu, L.; Striker, G.E.; Vlassara, H. Restriction of advanced glycation end products improves insulin resistance in human type 2 diabetes: Potential role of AGER1 and SIRT1. Diabetes Care 2011, 34, 1610–1616. [Google Scholar] [CrossRef]
- Koschinsky, T.; He, C.J.; Mitsuhashi, T.; Bucala, R.; Liu, C.; Buenting, C.; Heitmann, K.; Vlassara, H. Orally absorbed reactive glycation products (glycotoxins): An environmental risk factor in diabetic nephropathy. Proc. Natl. Acad. Sci. USA 1997, 94, 6474–6479. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, B.P.; Owan, T.E.; Mohammed, S.F.; Meyer, D.M.; Mills, L.D.; Schalkwijk, C.G.; Redfield, M.M. Advanced glycation end products accumulate in vascular smooth muscle and modify vascular but not ventricular properties in elderly hypertensive canines. Circulation 2008, 118, 1002–1010. [Google Scholar] [CrossRef]
- Skovgaard, D.; Svensson, R.B.; Scheijen, J.; Eliasson, P.; Mogensen, P.; Hag, A.M.F.; Kjaer, M.; Schalkwijk, C.G.; Schjerling, P.; Magnusson, S.P.; et al. An advanced glycation endproduct (AGE)-rich diet promotes accumulation of AGEs in Achilles tendon. Physiol. Rep. 2017, 5, e13215. [Google Scholar] [CrossRef]
- Kellow, N.J.; Coughlan, M.T.; Reid, C.M. Association between habitual dietary and lifestyle behaviours and skin autofluorescence (SAF), a marker of tissue accumulation of advanced glycation endproducts (AGEs), in healthy adults. Eur. J. Nutr. 2018, 57, 2209–2216. [Google Scholar] [CrossRef]
- Van Waateringe, R.P.; Slagter, S.N.; van der Klauw, M.M.; van Vliet-Ostaptchouk, J.V.; Graaff, R.; Paterson, A.D.; Lutgers, H.L.; Wolffenbuttel, B.H.R. Lifestyle and clinical determinants of skin autofluorescence in a population-based cohort study. Eur. J. Clin. Investig. 2016, 46, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Chakravarty, E.F.; Hubert, H.B.; Lingala, V.B.; Fries, J.F. Reduced disability and mortality among aging runners: A 21-year longitudinal study. Arch. Intern. Med. 2008, 168, 1638–1646. [Google Scholar] [CrossRef]
- Sell, D.R.; Monnier, V.M. Structure elucidation of a senescence cross-link from human extracellular matrix. Implication of pentoses in the aging process. J. Biol. Chem. 1989, 264, 21597–21602. [Google Scholar]
- Malliaras, P.; Richards, P.J.; Garau, G.; Maffulli, N. Achilles tendon Doppler flow may be associated with mechanical loading among active athletes. Am. J. Sports Med. 2008, 36, 2210–2215. [Google Scholar] [CrossRef]
- Koetsier, M.; Lutgers, H.L.; de Jonge, C.; Links, T.P.; Smit, A.J.; Graaff, R. Reference values of skin autofluorescence. Diabetes Technol. Ther. 2010, 12, 399–403. [Google Scholar] [CrossRef]
- Eny, K.M.; Orchard, T.J.; Miller, R.G.; Maynard, J.; Grant, D.M.; Costacou, T.; Cleary, P.A.; Braffett, B.H.; Paterson, A.D. Caffeine Consumption Contributes to Skin Intrinsic Fluorescence in Type 1 Diabetes. Diabetes Technol. Ther. 2015, 17, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Botros, N.; Sluik, D.; van Waateringe, R.P.; de Vries, J.H.M.; Geelen, A.; Feskens, E.J.M. Advanced glycation end-products (AGEs) and associations with cardio-metabolic, lifestyle, and dietary factors in a general population: The NQplus study. Diabetes Metab. Res. Rev. 2017, 33, e2892. [Google Scholar] [CrossRef]
- Uribarri, J.; Woodruff, S.; Goodman, S.; Cai, W.; Chen, X.; Pyzik, R.; Yong, A.; Striker, G.E.; Vlassara, H. Advanced glycation end products in foods and a practical guide to their reduction in the diet. J. Am. Diet. Assoc. 2010, 110, 911–916. [Google Scholar] [CrossRef]
- Scheijen, J.L.J.M.; Clevers, E.; Engelen, L.; Dagnelie, P.C.; Brouns, F.; Stehouwer, C.D.A.; Schalkwijk, C.G. Analysis of advanced glycation endproducts in selected food items by ultra-performance liquid chromatography tandem mass spectrometry: Presentation of a dietary AGE database. Food Chem. 2016, 190, 1145–1150. [Google Scholar] [CrossRef]
- Hull, G.L.J.; Woodside, J.V.; Ames, J.M.; Cuskelly, G.J. N-epsilon-(carboxymethyl)lysine content of foods commonly consumed in a Western style diet. Food Chem. 2012, 131, 170–174. [Google Scholar] [CrossRef]
- Forster, A.; Kuhne, Y.; Henle, T. Studies on absorption and elimination of dietary maillard reaction products. Ann. N. Y. Acad. Sci. 2005, 1043, 474–481. [Google Scholar] [CrossRef]
- den Engelsen, C.; van den Donk, M.; Gorter, K.J.; Salome, P.L.; Rutten, G.E. Advanced glycation end products measured by skin autofluorescence in a population with central obesity. Dermatoendocrinology 2012, 4, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Jochemsen, B.M.; Van Doormaal, J.J.; Mulder, G.; Volmer, M.; Graaff, R.; Smit, A.J.; Mulder, D.J. Relation between food and drinking habits, and skin autofluorescence and intima media thickness in subjects at high cardiovascular risk. J. Food Nutr. Res. Bratisl. 2009, 48, 51–58. [Google Scholar]
- Boor, P.; Celec, P.; Behuliak, M.; Grancic, P.; Kebis, A.; Kukan, M.; Pronayova, N.; Liptaj, T.; Ostendorf, T.; Sebekova, K. Regular moderate exercise reduces advanced glycation and ameliorates early diabetic nephropathy in obese Zucker rats. Metab. Clin. Exp. 2009, 58, 1669–1677. [Google Scholar] [CrossRef]
- Momma, H.; Niu, K.; Kobayashi, Y.; Guan, L.; Sato, M.; Guo, H.; Chujo, M.; Otomo, A.; Yufei, C.; Tadaura, H.; et al. Skin advanced glycation end product accumulation and muscle strength among adult men. Eur. J. Appl. Physiol. 2011, 111, 1545–1552. [Google Scholar] [CrossRef]
- Tabara, Y.; Ikezoe, T.; Yamanaka, M.; Setoh, K.; Segawa, H.; Kawaguchi, T.; Kosugi, S.; Nakayama, T.; Ichihashi, N.; Tsuboyama, T.; et al. Advanced Glycation End Product Accumulation Is Associated With Low Skeletal Muscle Mass, Weak Muscle Strength, and Reduced Bone Density: The Nagahama Study. J. Gerontol. A Biol. Sci. Med. Sci. 2018. [Google Scholar] [CrossRef]
- Kongsgaard, M.; Kovanen, V.; Aagaard, P.; Doessing, S.; Hansen, P.; Laursen, A.H.; Kaldau, N.C.; Kjaer, M.; Magnusson, S.P. Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand. J. Med. Sci. Sports 2009, 19, 790–802. [Google Scholar] [CrossRef]
- Monami, M.; Lamanna, C.; Gori, F.; Bartalucci, F.; Marchionni, N.; Mannucci, E. Skin autofluorescence in type 2 diabetes: Beyond blood glucose. Diabetes Res. Clin. Pract. 2008, 79, 56–60. [Google Scholar] [CrossRef]
- Giacomozzi, C.; D’Ambrogi, E.; Uccioli, L.; Macellari, V. Does the thickening of Achilles tendon and plantar fascia contribute to the alteration of diabetic foot loading? Clin. Biomech. 2005, 20, 532–539. [Google Scholar] [CrossRef]
- Slane, L.C.; Thelen, D.G. Non-uniform displacements within the Achilles tendon observed during passive and eccentric loading. J. Biomech. 2014, 47, 2831–2835. [Google Scholar] [CrossRef] [Green Version]
- Thorpe, C.T.; Udeze, C.P.; Birch, H.L.; Clegg, P.D.; Screen, H.R. Capacity for sliding between tendon fascicles decreases with ageing in injury prone equine tendons: A possible mechanism for age-related tendinopathy? Eur. Cell. Mater. 2013, 25, 48–60. [Google Scholar] [CrossRef]
- Franz, J.R.; Thelen, D.G. Imaging and simulation of Achilles tendon dynamics: Implications for walking performance in the elderly. J. Biomech. 2016, 49, 1403–1410. [Google Scholar] [CrossRef] [Green Version]
- De Jonge, S.; Rozenberg, R.; Vieyra, B.; Stam, H.J.; Aanstoot, H.-J.; Weinans, H.; van Schie, H.T.M.; Praet, S.F.E. Achilles tendons in people with type 2 diabetes show mildly compromised structure: An ultrasound tissue characterisation study. Br. J. Sports Med. 2015, 49, 995–999. [Google Scholar] [CrossRef]
- Abate, M.; Salini, V. Mid-portion Achilles tendinopathy in runners with metabolic disorders. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 697–703. [Google Scholar] [CrossRef]
- Gaida, J.E.; Ashe, M.C.; Bass, S.L.; Cook, J.L. Is adiposity an under-recognized risk factor for tendinopathy? A systematic review. Arthritis Rheum. 2009, 61, 840–849. [Google Scholar] [CrossRef]
- Scott, A.; Zwerver, J.; Grewal, N.; de Sa, A.; Alktebi, T.; Granville, D.J.; Hart, D.A. Lipids, adiposity and tendinopathy: Is there a mechanistic link? Critical review. Br. J. Sports Med. 2015, 49, 984–988. [Google Scholar] [CrossRef]
- Siegel, R.C.; Pinnell, S.R.; Martin, G.R. Cross-linking of collagen and elastin. Properties of lysyl oxidase. Biochemistry 1970, 9, 4486–4492. [Google Scholar] [CrossRef]
- Stone, N.; Meister, A. Function of ascorbic acid in the conversion of proline to collagen hydroxyproline. Nature 1962, 194, 555–557. [Google Scholar] [CrossRef]
- Farup, J.; Rahbek, S.K.; Vendelbo, M.H.; Matzon, A.; Hindhede, J.; Bejder, A.; Ringgard, S.; Vissing, K. Whey protein hydrolysate augments tendon and muscle hypertrophy independent of resistance exercise contraction mode. Scand. J. Med. Sci. Sports 2014, 24, 788–798. [Google Scholar] [CrossRef]
- Barbosa, A.W.C.; Benevides, G.P.; Alferes, L.M.T.; Salomao, E.M.; Gomes-Marcondes, M.C.C.; Gomes, L. A leucine-rich diet and exercise affect the biomechanical characteristics of the digital flexor tendon in rats after nutritional recovery. Amino Acids 2012, 42, 329–336. [Google Scholar] [CrossRef]
- Roncero-Ramos, I.; Niquet-Leridon, C.; Strauch, C.; Monnier, V.M.; Tessier, F.J.; Navarro, M.P.; Delgado-Andrade, C. An advanced glycation end product (AGE)-rich diet promotes Nepsilon-carboxymethyl-lysine accumulation in the cardiac tissue and tendons of rats. J. Agric. Food Chem. 2014, 62, 6001–6006. [Google Scholar] [CrossRef]
- Iqbal, M.; Kenney, P.B.; Al-Humadi, N.H.; Klandorf, H. Relationship between mechanical properties and pentosidine in tendon: Effects of age, diet restriction, and aminoguanidine in broiler breeder hens. Poult. Sci. 2000, 79, 1338–1344. [Google Scholar] [CrossRef]
- Reiser, K.M. Influence of age and long-term dietary restriction on enzymatically mediated crosslinks and nonenzymatic glycation of collagen in mice. J. Gerontol. 1994, 49, B71–B79. [Google Scholar] [CrossRef] [PubMed]
- Korntner, S.; Kunkel, N.; Lehner, C.; Gehwolf, R.; Wagner, A.; Augat, P.; Stephan, D.; Heu, V.; Bauer, H.-C.; Traweger, A.; et al. A high-glucose diet affects Achilles tendon healing in rats. Sci. Rep. 2017, 7, 780. [Google Scholar] [CrossRef] [PubMed]
- Kongsgaard, M.; Aagaard, P.; Kjaer, M.; Magnusson, S.P. Structural Achilles tendon properties in athletes subjected to different exercise modes and in Achilles tendon rupture patients. J. Appl. Physiol. 2005, 99, 1965–1971. [Google Scholar] [CrossRef] [Green Version]
- Arampatzis, A.; Karamanidis, K.; Albracht, K. Adaptational responses of the human Achilles tendon by modulation of the applied cyclic strain magnitude. J. Exp. Biol. 2007, 210, 2743–2753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenroth, L.; Peltonen, J.; Cronin, N.J.; Sipila, S.; Finni, T. Age-related differences in Achilles tendon properties and triceps surae muscle architecture In Vivo. J. Appl. Physiol. 2012, 113, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Stenroth, L.; Cronin, N.J.; Peltonen, J.; Korhonen, M.T.; Sipila, S.; Finni, T. Triceps surae muscle-tendon properties in older endurance-and sprint-trained athletes. J. Appl. Physiol. 2016, 120, 63–69. [Google Scholar] [CrossRef]
- Magnusson, S.P.; Beyer, N.; Abrahamsen, H.; Aagaard, P.; Neergaard, K.; Kjaer, M. Increased cross-sectional area and reduced tensile stress of the Achilles tendon in elderly compared with young women. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 123–127. [Google Scholar] [CrossRef]
- Ohberg, L.; Lorentzon, R.; Alfredson, H. Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 233–238. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls | Athletes | Combined | |
|---|---|---|---|
| Age (year) | 42 ± 22 | 57 ± 15 *** | 54 ± 18 |
| Waist (cm) | 89.7 ± 11.8 | 82.7 ± 6.2 ** | 83.9 ± 7.8 |
| Height (cm) | 180.3 ± 5.5 | 178.2 ± 6.7 | 178.6 ± 6.6 |
| Weight (kg) | 81.0 ± 12.3 | 73.8 ± 8.5 ** | 74.9 ± 9.6 |
| BMI (kg/m2) | 25.0 ± 3.8 | 23.2 ± 2.2 * | 23.5 ± 2.6 |
| Training years (years) | 13 ± 18 | 36 ± 15 *** | 32 ± 18 |
| High intense activity (hours/week) 1 | 0.17 ± 0.38 | 4.57 ± 4.04 *** | 3.86 ± 4.04 |
| Controls | Athletes | |
|---|---|---|
| Fruit (pieces) | 7.9 ± 7.1 | 15.3 ± 9.8 *** |
| Vegetables (100g portions) | 9.7 ± 9.0 | 13.5 ± 8.7 * |
| Fish (100g portions) | 1.2 ± 1.6 | 2.1 ± 3.4 * |
| Rye or wholegrain bread (slices) | 16 ± 11 | 16 ± 12 |
| Oat or wholegrain cereals (1 dL servings) | 4.1 ± 5.2 | 5.7 ± 5.9 |
| Coffee (cups) | 16 ± 14 | 16 ± 12 |
| Wine (glasses) | 5.0 ± 9.5 | 4.2 ± 8.0 |
| Beer (bottles) | 4.2 ± 7.8 | 2.6 ± 5.8 |
| Liquors and spirits (drinks) | 1.6 ± 4.2 | 0.4 ± 2.2 |
| Total fluid (liters) | 17.3 ± 5.5 | 18.0 ± 6.9 |
| Pure water (liters) | 9.1 ± 5.6 | 9.8 ± 5.8 |
| “Western” diet currently (%) | 46 ± 25 | 28 ± 21 *** |
| “Western” diet prior to 18 years (%) | 56 ± 21 | 44 ± 25 ** |
| Pearson | Spearman | ||||||
|---|---|---|---|---|---|---|---|
| Coefficient | R2 | p-Value | 95%-CI | rho | p-Value | ||
| Age (year) | 0.022 | 0.441 | <0.001 *** | 0.018 | 0.025 | 0.681 | <0.001 *** |
| Fruit (pieces) | 0.001 | <0.001 | 0.841 | −0.007 | 0.009 | 0.055 | 0.427 |
| Vegetables (100g portions) | −0.006 | 0.008 | 0.193 | −0.015 | 0.003 | −0.056 | 0.422 |
| Fish (100g portions) | 0.018 | 0.011 | 0.138 | −0.006 | 0.043 | 0.112 | 0.105 |
| Rye or wholegrain bread (slices) | 0.0004 | <0.001 | 0.896 | −0.006 | 0.007 | 0.025 | 0.722 |
| Oat or wholegrain cereals (1 dL servings) | −0.009 | 0.009 | 0.186 | −0.023 | 0.004 | −0.076 | 0.273 |
| Coffee (cups) | 0.008 | 0.033 | 0.008 ** | 0.002 | 0.014 | 0.229 | <0.001 *** |
| Wine (glasses) | 0.013 | 0.036 | 0.006 ** | 0.004 | 0.023 | 0.215 | 0.002 ** |
| Beer (bottles) | −0.007 | 0.005 | 0.310 | −0.020 | 0.006 | 0.011 | 0.881 |
| Liquors and spirits (drinks) | 0.035 | 0.026 | 0.021 * | 0.005 | 0.064 | 0.146 | 0.036 * |
| Total fluid (liters) | −0.009 | 0.012 | 0.119 | −0.021 | 0.002 | −0.132 | 0.063 |
| Pure water (liters) | −0.015 | 0.024 | 0.027 * | −0.029 | −0.002 | −0.182 | 0.009 ** |
| “Western” diet currently (%) | −0.001 | 0.002 | 0.512 | −0.005 | 0.002 | −0.083 | 0.233 |
| “Western” diet prior to 18 years (%) | −0.001 | 0.001 | 0.609 | −0.004 | 0.002 | −0.039 | 0.573 |
| Coefficient | SE | p-Value | Semi-Partial R2 (%) | ||
|---|---|---|---|---|---|
| SAF (AU). Model parameters: Age, exercise-group, waist circumference, height, weight, BMI, training years and high intense activity. | |||||
| Resulting model: n = 201, p < 0.0001, R2 = 45.9%. | |||||
| Intercept | 0.728 | 0.099 | <0.0001 | ||
| Age (years) | 0.0248 | 0.0022 | <0.0001 | 35.1 | |
| Training years (years) | −0.0044 | 0.0021 | 0.041 | 1.2 | |
| SAF (AU). Model parameters: Age, exercise-group, fruit, vegetables, fish, bread, cereals, coffee, wine, beer, liqueurs, total fluid, pure water, “Western” diet currently and “Western” diet prior to 18 years. | |||||
| Resulting model: n = 195, p < 0.0001, R2 = 42.7%. | |||||
| Intercept | 0.58 | 0.13 | <0.0001 | ||
| Age (years) | 0.0219 | 0.0018 | <0.0001 | 42.7 | |
| “Western” diet prior to 18 years (%) | 0.0031 | 0.0013 | 0.021 | 1.6 | |
| Achilles tendon thickness (mm). Model parameters: Age, exercise-group, waist circumference, height, weight, BMI, training years, high intense activity and SAF. | |||||
| Resulting model: n = 197, p < 0.0001, R2 = 33.8%. | |||||
| Intercept | −3.6 | 2.8 | 0.21 | ||
| Age (years) | 0.0288 | 0.0059 | <0.0001 | 8.2 | |
| Exercise-group (athlete) | 1.64 | 0.25 | <0.0001 | 14.8 | |
| Height (cm) | 0.041 | 0.015 | 0.0075 | 2.5 | |
| Achilles tendon Doppler (mm2) Model parameters: Age, exercise-group, waist circumference, height, weight, BMI, training years, high intense activity and SAF | |||||
| Resulting model: n = 197, p = 0.0023, R2 = 4.65%. | |||||
| Intercept | 0.01 | 0.16 | 0.94 | ||
| Exercise-group (athlete) | 0.53 | 0.17 | 0.0023 | 4.65 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hjerrild, J.N.; Wobbe, A.; Stausholm, M.B.; Larsen, A.E.; Josefsen, C.O.; Malmgaard-Clausen, N.M.; Dela, F.; Kjaer, M.; Magnusson, S.P.; Hansen, M.; et al. Effects of Long-Term Physical Activity and Diet on Skin Glycation and Achilles Tendon Structure. Nutrients 2019, 11, 1409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061409
Hjerrild JN, Wobbe A, Stausholm MB, Larsen AE, Josefsen CO, Malmgaard-Clausen NM, Dela F, Kjaer M, Magnusson SP, Hansen M, et al. Effects of Long-Term Physical Activity and Diet on Skin Glycation and Achilles Tendon Structure. Nutrients. 2019; 11(6):1409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061409
Chicago/Turabian StyleHjerrild, Joachim Nymann, Alexander Wobbe, Martin B. Stausholm, Anne Ellegaard Larsen, Christian Ohrhammer Josefsen, Nikolaj M. Malmgaard-Clausen, Flemming Dela, Michael Kjaer, S. Peter Magnusson, Mette Hansen, and et al. 2019. "Effects of Long-Term Physical Activity and Diet on Skin Glycation and Achilles Tendon Structure" Nutrients 11, no. 6: 1409. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061409