Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Exercise Protocol
3.4. Protocol of Nutritional Intervention
3.5. Protocols of Interventions that Combined Exercise and Nutrition
3.6. Risk of Bias in Included Studies
3.7. Effects of Exercise on Body Composition
3.8. Effects of Exercise on Metabolic and Inflammatory Biomarkers
3.9. Effects of Exercise on Muscle Strength and Walking Speed
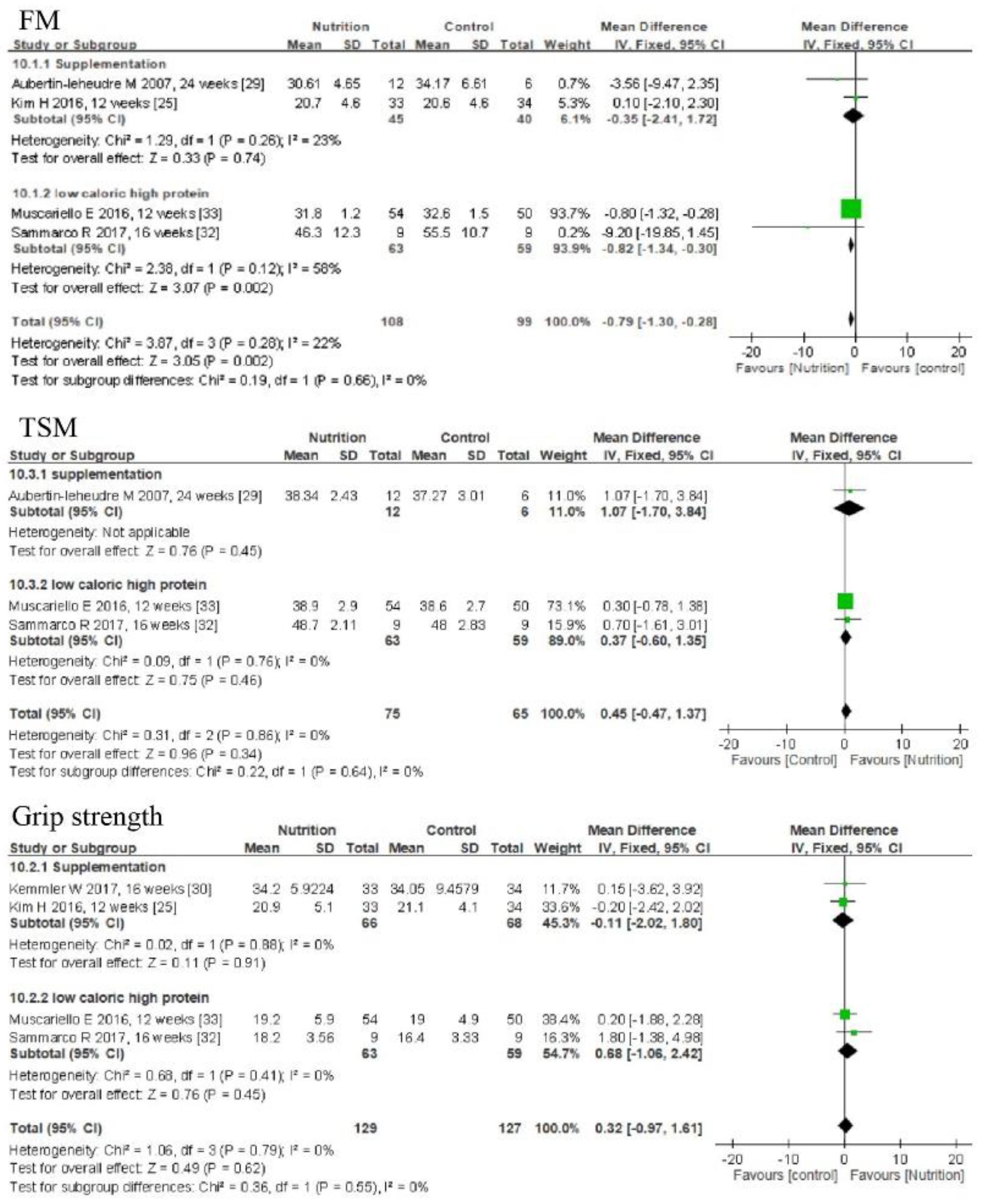
3.10. Effects of Nutritional Intervention on Body Composition
3.11. Effects of Nutrition on Muscle Strength
3.12. Additional Effects of Nutritional Supplementation on Exercise Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mijnarends, D.M.; Luiking, Y.C.; Halfens, R.J.G.; Evers, S.; Lenaerts, E.L.A.; Verlaan, S.; Wallace, M.; Schols, J.; Meijers, J.M.M. Muscle, Health and Costs: A glance at their relationship. J. Nutr. Health Aging 2018, 22, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S. Is sarcopenia associated with an increased risk of all-cause mortality and functional disability? Exp. Gerontol. 2017, 96, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lin, S.; Gao, T.; Zhong, F.; Cai, J.; Sun, Y.; Ma, A. Association between sarcopenia and metabolic syndrome in middle-aged and older non-obese adults: A systematic review and meta-analysis. Nutrients 2018, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H.; American Heart Association; Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Metabolism Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American heart association scientific statement on obesity and heart disease from the obesity committee of the council on nutrition, physical activity, and metabolism. Circulation 2006, 113, 898–918. [Google Scholar] [PubMed]
- Maffiuletti, N.A.; Jubeau, M.; Munzinger, U.; Bizzini, M.; Agosti, F.; De Col, A.; Lafortuna, C.L.; Sartorio, A. Differences in quadriceps muscle strength and fatigue between lean and obese subjects. Eur. J. Appl. Physiol. 2007, 101, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Brady, A.O.; Straight, C.R.; Evans, E.M. Body Composition, muscle Capacity, and physical function in older adults: An Integrated Conceptual Model. J. Aging Phys. Act 2014, 22, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N. Body composition in healthy aging. Ann. N. Y. Acad. Sci. 2000, 904, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.J.; Nam, G.E.; Han, K.D.; Choi, S.W.; Jung, S.W.; Bok, A.R.; Kim, Y.H.; Lee, K.S.; Han, B.D.; Kim, D.H. Sarcopenia and sarcopenic obesity and their association with dyslipidemia in Korean elderly men: The 2008–2010 Korea national health and nutrition examination survey. J. Endocrinol. Investig. 2014, 37, 247–260. [Google Scholar] [CrossRef]
- Levine, M.E.; Crimmins, E.M. The impact of insulin resistance and inflammation on the association between sarcopenic obesity and physical functioning. Obesity (Silver Spring) 2012, 20, 2101–2106. [Google Scholar] [CrossRef]
- Kim, J.H.; Cho, J.J.; Park, Y.S. Relationship between sarcopenic obesity and cardiovascular disease risk as estimated by the framingham risk score. J. Korean Med. Sci. 2015, 30, 264–271. [Google Scholar] [CrossRef]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Sarcopenic obesity and risk of cardiovascular disease and mortality: A population-based cohort study of older men. J. Am. Geriatr. Soc. 2014, 62, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Hirani, V.; Naganathan, V.; Blyth, F.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Longitudinal associations between body composition, sarcopenic obesity and outcomes of frailty, disability, institutionalisation and mortality in community-dwelling older men: The concord health and ageing in men project. Age Ageing 2017, 46, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults. Circulation 2014, 129 (Suppl. 2), S102–S138. [Google Scholar] [CrossRef] [PubMed]
- De Spiegeleer, A.; Petrovic, M.; Boeckxstaens, P.; Van Den Noortgate, N. Treating Sarcopenia in Clinical Practice: Where are We Now? Acta Clin. Belg. 2016, 71, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Makanae, Y.; Fujita, S. Role of exercise and nutrition in the prevention of sarcopenia. J. Nutr. Sci. Vitaminol. 2015, 61, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Theodorakopoulos, C.; Jones, J.; Bannerman, E.; Greig, C.A. Effectiveness of nutritional and exercise interventions to improve body composition and muscle strength or function in sarcopenic obese older adults: A systematic review. Nutr. Res. 2017, 43, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Amat, A.; Aibar-Almazan, A.; Fabrega-Cuadros, R.; Cruz-Diaz, D.; Jimenez-Garcia, J.D.; Perez-Lopez, F.R.; Achalandabaso, A.; Barranco-Zafra, R.; Hita-Contreras, F. Exercise alone or combined with dietary supplements for sarcopenic obesity in community-dwelling older people: A systematic review of randomized controlled trials. Maturitas 2018, 110, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F.; Bueno-Notivol, J.; Martinez-Amat, A.; Cruz-Diaz, D.; Hernandez, A.V.; Perez-Lopez, F.R. Effect of exercise alone or combined with dietary supplements on anthropometric and physical performance measures in community-dwelling elderly people with sarcopenic obesity: A meta-analysis of randomized controlled trials. Maturitas 2018, 116, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Aubertin-Leheudre, M.; Lord, C.; Khalil, A.; Dionne, I.J. Six months of isoflavone supplement increases fat-free mass in obese-sarcopenic postmenopausal women: A randomized double-blind controlled trial. Eur. J. Clin. Nutr. 2007, 61, 1442–1444. [Google Scholar] [CrossRef]
- Balachandran, A.; Krawczyk, S.N.; Potiaumpai, M.; Signorile, J.F. High-speed circuit training vs hypertrophy training to improve physical function in sarcopenic obese adults: A randomized controlled trial. Exp. Gerontol. 2014, 60, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.T.; Chung, Y.C.; Chen, Y.J.; Ho, S.Y.; Wu, H.J. Effects of different types of exercise on body composition, muscle strength, and IGF-1 in the Elderly with sarcopenic obesity. J. Am. Geriatr. Soc. 2017, 65, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.C.; Yang, R.S.; Yang, R.J.; Chang, S.F. Effects of resistance training on body composition and functional capacity among sarcopenic obese residents in long-term care facilities: A preliminary study. BMC Geriatr. 2018, 18, 21. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Ku, J.W.; Lin, L.F.; Liao, C.D.; Chou, L.C.; Liou, T.H. Body composition influenced by progressive elastic band resistance exercise of sarcopenic obesity elderly women: A pilot randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 556–563. [Google Scholar] [PubMed]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; Willert, S.; Bebenek, M.; Shojaa, M.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Whole-body electromyostimulation and protein supplementation favorably affect sarcopenic obesity in community-dwelling older men at risk: The randomized controlled FranSO study. Clin. Interv. Aging 2017, 12, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, M.; Kojima, N.; Fujino, K.; Hosoi, E.; Kobayashi, H.; Somekawa, S.; Niki, Y.; Yamashiro, Y.; Yoshida, H. Exercise and nutritional supplementation on community-dwelling elderly japanese women with sarcopenic obesity: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2016, 17, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Tsauo, J.Y.; Lin, L.F.; Huang, S.W.; Ku, J.W.; Chou, L.C.; Liou, T.H. Effects of elastic resistance exercise on body composition and physical capacity in older women with sarcopenic obesity: A CONSORT-compliant prospective randomized controlled trial. Medicine 2017, 96, e7115. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Huang, S.W.; Ku, J.W.; Hsiao, D.J.; Liou, T.H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef]
- Maltais, M.L.; Perreault, K.; Courchesne-Loyer, A.; Lagacé, J.-C.; Barsalani, R.; Dionne, I.J. Effect of resistance training and various sources of protein supplementation on body fat mass and metabolic profile in sarcopenic overweight older adult men: A pilot study. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 71–77. [Google Scholar] [CrossRef]
- Muscariello, E.; Nasti, G.; Siervo, M.; Di Maro, M.; Lapi, D.; D’Addio, G.; Colantuoni, A. Dietary protein intake in sarcopenic obese older women. Clin. Interv. Aging 2016, 11, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.G.; Tomeleri, C.M.; Fernandes, R.R.; Sugihara Junior, P.; Cavalcante, E.F.; Cunha, P.M.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; et al. Effect of whey protein supplementation combined with resistance training on body composition, muscular strength, functional capacity, and plasma-metabolism biomarkers in older women with sarcopenic obesity: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. ESPEN 2019, 32, 88–95. [Google Scholar] [PubMed]
- Park, J.; Kwon, Y.; Park, H. Effects of 24-week aerobic and resistance training on carotid artery intima-media thickness and flow velocity in elderly women with sarcopenic obesity. J. Atheroscler. Thromb. 2017, 24, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Sammarco, R.; Marra, M.; Di Guglielmo, M.L.; Naccarato, M.; Contaldo, F.; Poggiogalle, E.; Donini, L.M.; Pasanisi, F. Evaluation of hypocaloric diet with protein supplementation in middle-aged sarcopenic obese women: A pilot study. Obes. Facts 2017, 10, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, K.S.; Dias, J.M.; Araujo, M.C.; Pinheiro, A.C.; Moreira, B.S.; Dias, R.C. Effects of a progressive resistance exercise program with high-speed component on the physical function of older women with sarcopenic obesity: A randomized controlled trial. Braz. J. Phys. Ther. 2016, 20, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Briani, R.V.; Ferreira, A.S.; Pazzinatto, M.F.; Pappas, E.; De Oliveira Silva, D.; Azevedo, F.M. What interventions can improve quality of life or psychosocial factors of individuals with knee osteoarthritis? a systemative review with meta-analysis of primary outcomes from randomised controlled trials. Br. J. Sports Med. 2018, 52, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Kalinkovich, A.; Livshits, G. Sarcopenic obesity or obese sarcopenia: A cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res. Rev. 2017, 35, 200–221. [Google Scholar] [CrossRef] [PubMed]
- Beckwee, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; De Saint-Hubert, M.; Bautmans, I. Exercise intervention for the prevention and treatment of sarcopenia. A systematic umbrella review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Roberts, S.; Haskell, W. Comparison of aerobic exercise, diet or both on lipids and lipoproteins in adults: A meta-analysis of randomized controlled trials. Clin. Nutr. 2012, 31, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S. Aerobic exercise and lipids and lipoproteins in men: A meta-analysis of randomized controlled trials. J. Mens. Health Gend. 2006, 3, 61–70. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Tran, Z.V. Aerobic exercise and lipids and lipoproteins in women: A meta-analysis of randomized controlled trials. J. Womens Health 2004, 13, 1148–1164. [Google Scholar] [CrossRef] [PubMed]
- Pasiakos, S.M.; Cao, J.J.; Margolis, L.M.; Sauter, E.R.; Whigham, L.D.; McClung, J.P.; Rood, J.C.; Carbone, J.W.; Combs, G.F., Jr.; Young, A.J. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss: A randomized controlled trial. FASEB J. 2013, 27, 3837–3847. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.T.; Cruz-Jentoft, A.J.; Landi, F.; Hickson, M.; Zamboni, M.; Pereira, S.L.; Hustead, D.S.; Mustad, V.A. Impacts of high-protein oral nutritional supplements among malnourished men and women with sarcopenia: A multicenter, randomized, double-blinded, controlled trial. J. Am. Med. Dir. Assoc. 2016, 17, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Hanach, N.I.; McCullough, F.; Avery, A. The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: A systematic review and meta-analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Tokuda, Y. Effect of whey protein supplementation after resistance exercise on the muscle mass and physical function of healthy older women: A randomized controlled trial. Geriatr. Gerontol. Int. 2018, 18, 1398–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Country) [ref] | Study Design | Groups (Sample Size) | Age (Years) | Sex | Definition of Sarcopenic Obesity | Assessment Tool of Body Composition | Time Point of Measurement | Results | PEDro Score | |
|---|---|---|---|---|---|---|---|---|---|---|
| Sarcopenia | Obesity | |||||||||
| Aubertin-Leheudre M., 2007 (Canada) [20] | RCT | Isoflavones (12) Control (6) | 58.0 ± 5.0 | Women | SMI (ASM/Ht2) <6.87 kg/m2 | BF% >40 | DXA | Baseline: 0 week Posttest: 24 weeks | Legs FFM, ASM and SMI ↑ BW, BMI, WC, FM, TSM ⇌ | 8 |
| Balachandran A., 2014 (US) [21] | RCT | RE (9) PT (8) | 71.3 ± 8.0 | Both | SMI (TSM/Ht2) <10.76 kg/m2 in men; <6.76 kg/m2 in women | BMI >30 kg/m2 | BIA | Baseline: 0 week Posttest: 15 weeks | leg press power (PT) ↑ SPPB, 1RM of leg press and chest press ⇌ | 4 |
| Chen H.T., 2017 (Taiwan) [22] | RCT | AE (15) RE (15) CE (15) Control (15) | 68.8 ± 3.3 | Both | SMI (ASM/BW) ≤32.5% in men; ≤25.7% in women | BMI ≥25 kg/m2 and VFA ≥100 cm2 | BIA | Baseline: 0 week Posttest: 8 weeks Follow up: 12 weeks | BW (AE and CE), BMI (CE), TSM, SMI, FM, BF%, VFA and BES (AE, RE and CE), GS (RE), KES (RE and CE) ↑ | 5 |
| Chiu S.C., 2018 (Taiwan) [23] | Quasi-experimental study | RE (33) Control (31) | 79.9 ± 7.8 | Both | SMI (TSM/BW) <37.15% in men; <32.26% in women | BF% >29 in men BF% >40 in women | BIA | Baseline: 0 week Posttest: 12 weeks | GS, PS ↑ ASM, BF%, SMI ⇌ | 4 |
| Huang S.W., 2017 (Taiwan) [24] | RCT | RE (18) Control (17) | 69.2 ± 5.0 | Women | SMI (TSM/BW) <27.6% | BF% >30 | DXA | Baseline: 0 week Posttest: 12 weeks | FM, BF% ↑ BW, BMI, TSM, SMI, TG, HDL, LDL, CHOL, CRP ⇌ | 7 |
| Kemmler W., 2017 (Germany) [25] | RCT | Protein (33) Control (34) | 77.5 ± 5.1 | Men | SMI (ASM/BMI) <0.789 | BF% >27 | BIA | Baseline: 0 week Posttest: 16 weeks | BF%, SMI ↑ GS ⇌ | 8 |
| Kim H., 2016 (Japan) [26] | RCT | EN (36) E (35) N (34) Control (34) | 81.1 ± 4.6 | Women | SMI (ASM/Ht2) <5.67kg/m2 or GS <17 kg or WS <1m/s | BF% >32 | BIA | Baseline: 0 week Posttest: 12 weeks | FM (EN), TFM, stride and step length (E) ↑ BF%, ASM, SMI, GS, KES, WS, SBP, CHOL, TG, CRP, IL-6 and HBA1c ⇌ | 6 |
| Liao C.D., 2017 (Taiwan) [27] | RCT | RE (25) Control (21) | 67.3 ± 5.1 | Women | SMI (TSM/Ht2) <7.15 kg/m2 | BF% >30 | DXA | Baseline: 0 week Posttest: 12 weeks | TSM, FM, BF%, SLS, WS, TUG, TCR, GS ↑ | 8 |
| Liao C.D., 2018 (Taiwan) [28] | RCT | RE (30) Control (20) | 67.3 ± 5.1 | Women | SMI (TSM/BW) <27.6% | BF% >30 | BIA | Baseline: 0 week Posttest: 12 weeks Follow up: 36 weeks | BF%, TSM, ASM, SMI, SLS, WS, TUG, TCR ↑ | 9 |
| Maltais M.L., 2016 (Canada) [29] | RCT | RE + Nondairy shake (8) RE+Dairy shake (8) RE (10) | 65.2 ± 4.8 | Men | SMI (ASM/Ht2) <10.75 kg/m2 | BMI >30 kg/m2 | DXA | Baseline: 0 week Posttest: 16 weeks | FM (RE+Dairy shake and RE+Nondairy shake) ↑ BMI, TSM, GLU, insulin, CHOL, TG, HDL, LDL, leptin, TNF-a, IL-6 and CRP ⇌ | 6 |
| Muscariello E., 2016 (Italy) [30] | RCT | LCNP (50) LCHP (54) | 66.7 ± 4.9 | Women | SMI (TSM/Ht2) <7.3 kg/m2 | BMI >30 kg/m2 | BIA | Baseline: 0 week Posttest: 12 weeks | BMI, WC, FM, TSM, SMI, GS ⇌ | 6 |
| Nabuco H.C.G., 2019 (Brazil) [31] | RCT | RE + protein (13) RE (13) | 69.0 ± 4.1 | Women | ASM <15.02 kg | BF% >35 | DXA | Baseline: 0 week Posttest: 16 weeks | TSM, ASM, FM, BF% and IL-6 (RE+protein) ↑ WC, CHOL, TG, HDL, LDL, GLU, insulin, HOMA-IR, TNF-a, CRP, SBP ⇌ | 8 |
| Park J., 2017 (Korea) [32] | RCT | CE (25) Control (25) | 74.1 ± 6.1 | Women | SMI (ASM/BW) <25.1% | BMI >25 kg/m2 | BIA | Baseline: 0 week Posttest: 24 weeks | WC, BF%, GS, TCR, SBP, CHOL, LDL ↑ ASM, TG, HDL, CRP ⇌ | 7 |
| Sammarco R., 2017 (Italy) [33] | RCT | LCNP (9) LCHP (9) | 55.0 ± 9.6 | Women | <90% of ideal FFMa | BF% >34.8 | BIA | Baseline: 0 week Posttest: 16 week | TSM (LCHP) ↑ BW, FM, BF%, GS, SPPB ⇌ | 5 |
| Vasconcelos K.S., 2016 (Brazil) [34] | RCT | RE (14) Control (14) | 72.0 ± 4.1 | Women | GS ≤21 kg | BMI ≥30 kg/m2 | NA | Baseline: 0 week Posttest: 10 week | WS, SPPB, KES, KEP ⇌ | 8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, K.-J.; Liao, C.-D.; Tsai, M.-W.; Chen, C.-N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092163
Hsu K-J, Liao C-D, Tsai M-W, Chen C-N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients. 2019; 11(9):2163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092163
Chicago/Turabian StyleHsu, Kuo-Jen, Chun-De Liao, Mei-Wun Tsai, and Chiao-Nan Chen. 2019. "Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis" Nutrients 11, no. 9: 2163. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092163