A Systematic Review and Meta-Analysis of B Vitamin Supplementation on Depressive Symptoms, Anxiety, and Stress: Effects on Healthy and ‘At-Risk’ Individuals



Abstract
:1. Introduction
2. Materials and Methods
2.1. Searches
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Data Analyses
3. Results
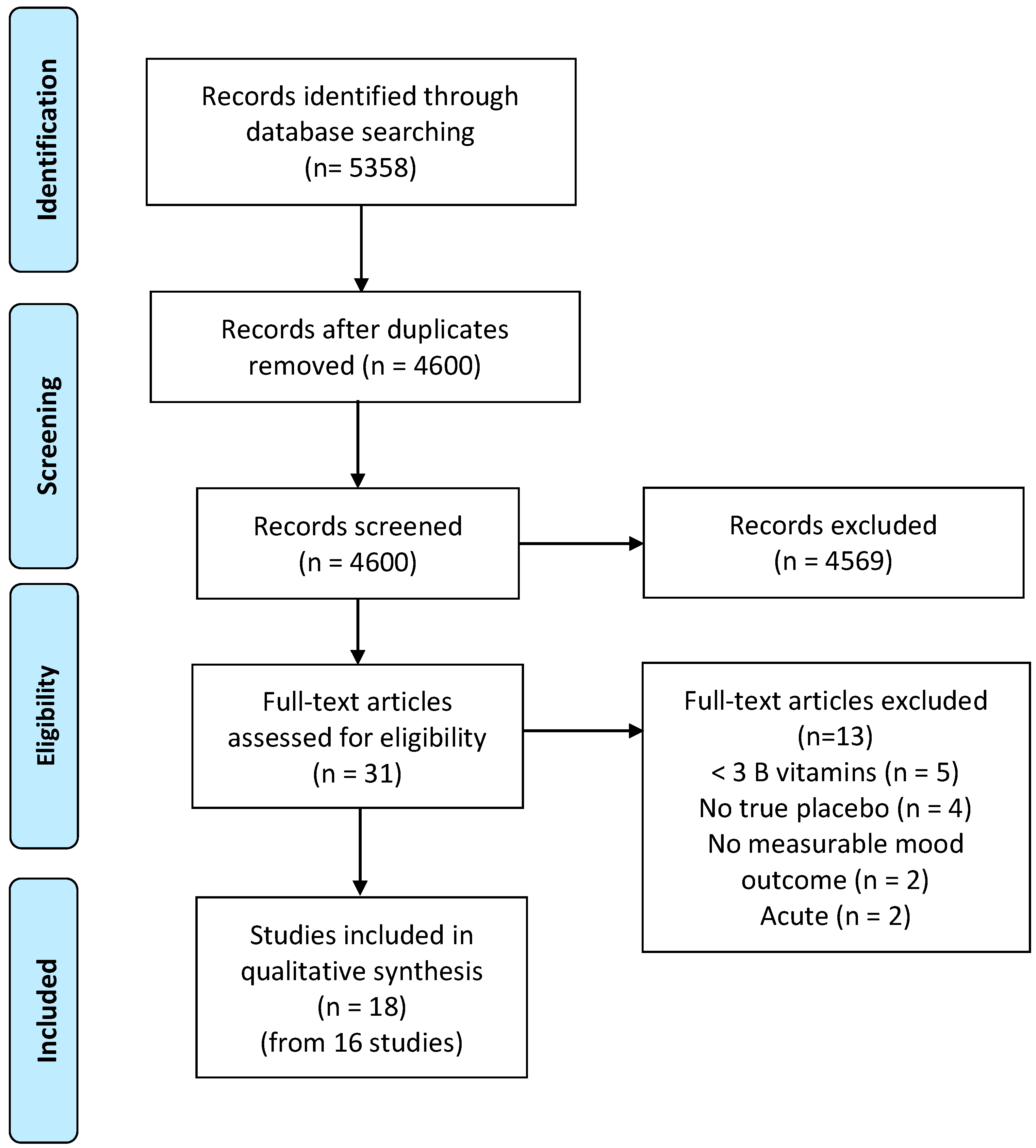
3.1. Study Selection
3.2. Constituents of Supplements
3.3. Overall Mood
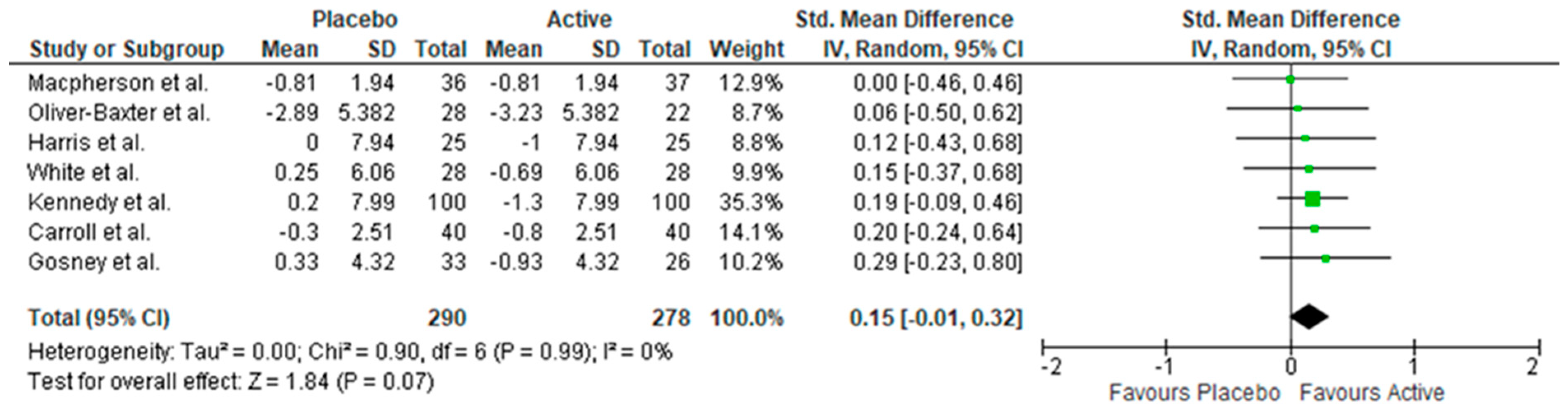
3.4. Depressive Symptoms
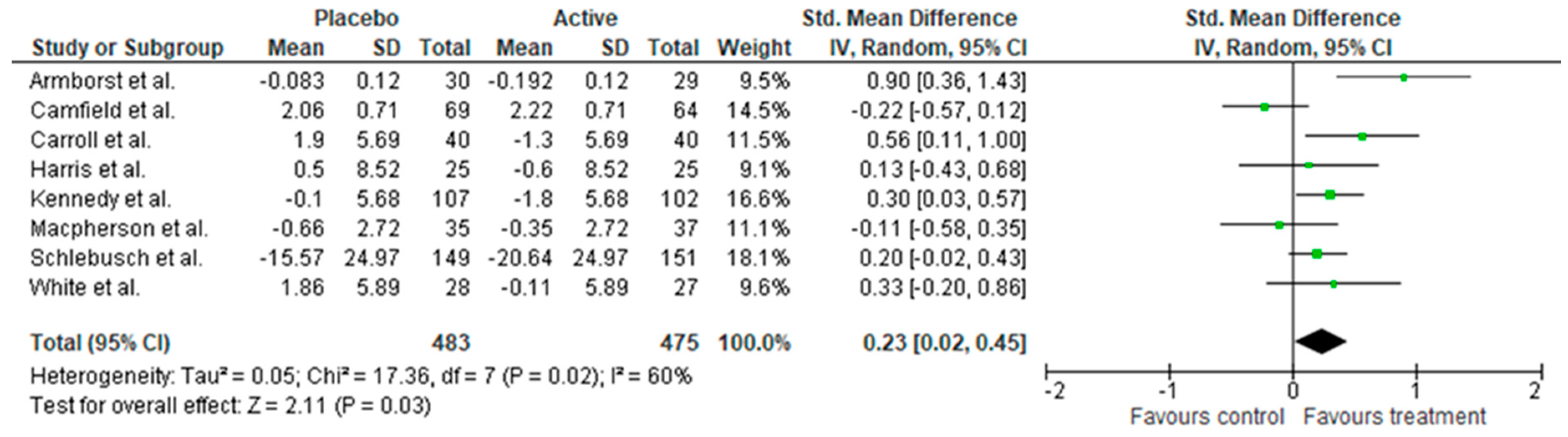
3.5. Stress
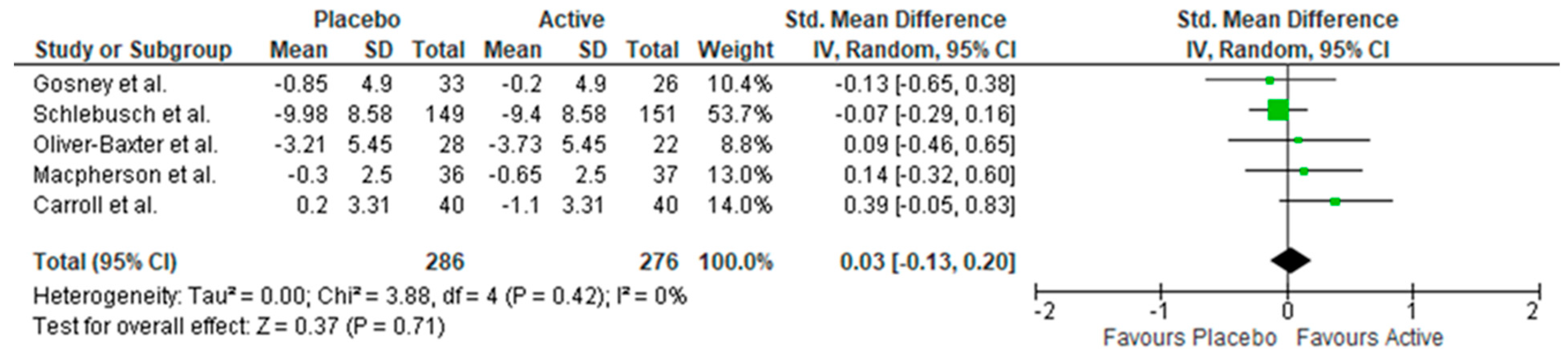
3.6. Anxiety Symptoms
3.7. Biomarkers
3.8. At-Risk Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Whiteford, H.A.; Ferrari, A.J.; Degenhardt, L.; Feigin, V.; Vos, T. The global burden of mental, neurological and substance use disorders: An analysis from the Global Burden of Disease Study 2010. PLoS ONE 2015, 10, e0116820. [Google Scholar] [CrossRef] [PubMed]
- Hariri, A.R.; Drabant, E.M.; Munoz, K.E.; Kolachana, L.S.; Mattay, V.S.; Egan, M.F.; Weinberger, D.R. A susceptibility gene for affective disorders and the response of the human amygdala. Arch. Gen. Psychiatry 2005, 62, 146–152. [Google Scholar] [CrossRef]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; Pasco, J.A.; Mykletun, A.; Williams, L.J.; Hodge, A.M.; O’Reilly, S.L.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Association of Western and Traditional Diets with Depression and Anxiety in Women. Am. J. Psychiatry 2010, 167, 305–311. [Google Scholar] [CrossRef]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy-A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O.; Haskell, C.F. Vitamins and cognition. Drugs 2011, 71, 1957–1971. [Google Scholar] [CrossRef]
- Long, S.J.; Benton, D. Effects of Vitamin and Mineral Supplementation on Stress, Mild Psychiatric Symptoms, and Mood in Nonclinical Samples: A Meta-Analysis. Psychosom. Med. 2013, 75, 144–153. [Google Scholar] [CrossRef]
- Almeida, O.P.; Ford, A.H.; Flicker, L. Systematic review and meta-analysis of randomized placebo-controlled trials of folate and vitamin B12 for depression. Int. Psychogeriatr. 2015, 27, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; Logan, A.C.; Akbaraly, T.N.; Amminger, G.P.; Balanzá-Martínez, V.; Freeman, M.P.; Hibbeln, J.; Matsuoka, Y.; Mischoulon, D.; Mizoue, T. Nutritional medicine as mainstream in psychiatry. Lancet Psychiatry 2015, 2, 271–274. [Google Scholar] [CrossRef]
- Scholey, A. Nutrients for neurocognition in health and disease: Measures, methodologies and mechanisms. Proc. Nutr. Soc. 2018, 77, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.H.; Carney, M.W.; Toone, B.K. Methylation and mood. Lancet (Lond. Engl.) 1984, 2, 196–198. [Google Scholar] [CrossRef]
- Otaegui-Arrazola, A.; Amiano, P.; Elbusto, A.; Urdaneta, E.; Martinez-Lage, P. Diet, cognition, and Alzheimer’s disease: Food for thought. Eur. J. Nutr. 2014, 53, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Bottiglieri, T.; Laundy, M.; Crellin, R.; Toone, B.K.; Carney, M.W.; Reynolds, E.H. Homocysteine, folate, methylation, and monoamine metabolism in depression. J. Neurol. Neurosurg. Psychiatry 2000, 69, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; Murphy, J.; Mischoulon, D.; Papakostas, G.I.; Fava, M.; Berk, M.; Ng, C.H. Adjunctive Nutraceuticals for Depression: A Systematic Review and Meta-Analyses. Am. J. Psychiatry 2016, 173, 575–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, O.P.; Ford, A.H.; Hirani, V.; Singh, V.; van Bockxmeer, F.M.; McCaul, K.; Flicker, L. B vitamins to enhance treatment response to antidepressants in middle-aged and older adults: Results from the B-VITAGE randomised, double-blind, placebo-controlled trial. Br. J. Psychiatry J. Ment. Sci. 2014, 205, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Rajkowska, G. Postmortem studies in mood disorders indicate altered numbers of neurons and glial cells. Biol. Psychiatry 2000, 48, 766–777. [Google Scholar] [CrossRef]
- Normann, C.; Schmitz, D.; Furmaier, A.; Doing, C.; Bach, M. Long-term plasticity of visually evoked potentials in humans is altered in major depression. Biol. Psychiatry 2007, 62, 373–380. [Google Scholar] [CrossRef]
- Laville, M.; Segrestin, B.; Alligier, M.; Ruano-Rodríguez, C.; Serra-Majem, L.; Hiesmayr, M.; Schols, A.; La Vecchia, C.; Boirie, Y.; Rath, A.; et al. Evidence-based practice within nutrition: What are the barriers for improving the evidence and how can they be dealt with? Trials 2017, 18, 425. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C. A Potential Design Flaw of Randomized Trials of Vitamin Supplements. J. Am. Med. Assoc. 2011, 305, 1348–1349. [Google Scholar] [CrossRef]
- Bowman, G.L.; Silbert, L.C.; Howieson, D.; Dodge, H.H.; Traber, M.G.; Frei, B.; Kaye, J.A.; Shannon, J.; Quinn, J.F. Nutrient biomarker patterns, cognitive function, and MRI measures of brain aging. Neurology 2012, 78, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Berti, V.; Murray, J.; Davies, M.; Spector, N.; Tsui, W.H.; Li, Y.; Williams, S.; Pirraglia, E.; Vallabhajosula, S.; McHugh, P.; et al. Nutrient patterns and brain biomarkers of Alzheimer’s disease in cognitively normal individuals. J. Nutr. Health Aging 2015, 19, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Zamroziewicz, M.K.; Barbey, A.K. Nutritional cognitive neuroscience: Innovations for healthy brain aging. Front. Neurosci. 2016, 10, 240. [Google Scholar] [CrossRef] [PubMed]
- De Souza, M.C.; Walker, A.F.; Robinson, P.A.; Boll, K. A synergistic effect of a daily supplement for 1 month of 200 mg magnesium plus 50 mg vitamin B6 for the relief of anxiety-related premenstrual symptoms: A randomized, double-blind, crossover study. J. Women’s Health Gend.-Based Med. 2000, 9, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Bryan, J.; Calvaresi, E.; Hughes, D. Short-term folate, vitamin B-12 or vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J. Nutr. 2002, 132, 1345–1356. [Google Scholar] [CrossRef]
- Williams, E.; Stewart-Knox, B.; Bradbury, I.; Rowl, I.; Pentieva, K.; Heler, A.; McNulty, H. Effect of folic acid supplementation on mood and serotonin response in healthy males. Br. J. Nutr. 2005, 94, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpley, A.L.; Hockney, R.; McPeake, L.; Geddes, J.R.; Cowen, P.J. Folic acid supplementation for prevention of mood disorders in young people at familial risk: A randomised, double blind, placebo controlled trial. J. Affect. Disord. 2014, 167, 306–311. [Google Scholar] [CrossRef]
- Popper, C.W. Single-micronutrient and broad-spectrum micronutrient approaches for treating mood disorders in youth and adults. Child Adolesc. Psychiatry Clin. N. Am. 2014, 23, 591–672. [Google Scholar] [CrossRef]
- Monti, J.M.; Moulton, C.J.; Cohen, N.J. The role of nutrition on cognition and brain health in ageing: A targeted approach. Nutr. Res. Rev. 2015, 28, 167–180. [Google Scholar] [CrossRef]
- Smith, A.D.; Refsum, H. Do we need to reconsider the desirable blood level of vitamin B12? J. Intern. Med. 2012, 271, 179–182. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Collaboration. Review Manager (RevMan), 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Veasey, R.; Watson, A.; Dodd, F.; Jones, E.; Maggini, S.; Haskell, C.F. Effects of high-dose B vitamin complex with vitamin C and minerals on subjective mood and performance in healthy males. Psychopharmacology (Berl.) 2010, 211, 55–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, D.O.; Veasey, R.C.; Watson, A.W.; Dodd, F.L.; Jones, E.K.; Tiplady, B.; Haskell, C.F. Vitamins and psychological functioning: A mobile phone assessment of the effects of a B vitamin complex, vitamin C and minerals on cognitive performance and subjective mood and energy. Hum. Psychopharmacol. 2011, 26, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Camfield, D.A.; Wetherell, M.A.; Scholey, A.B.; Cox, K.H.; Fogg, E.; White, D.J.; Sarris, J.; Kras, M.; Stough, C.; Sali, A.; et al. The effects of multivitamin supplementation on diurnal cortisol secretion and perceived stress. Nutrients 2013, 5, 4429–4450. [Google Scholar] [CrossRef] [PubMed]
- Pipingas, A.; Camfield, D.A.; Stough, C.; Cox, K.H.; Fogg, E.; Tiplady, B.; Sarris, J.; White, D.J.; Sali, A.; Wetherell, M.A.; et al. The effects of multivitamin supplementation on mood and general well-being in healthy young adults. A laboratory and at-home mobile phone assessment. Appetite 2013, 69, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Schlebusch, L.; Bosch, B.A.; Polglase, G.; Kleinschmidt, I.; Pillay, B.J.; Cassimjee, M.H. A double-blind, placebo-controlled, double-centre study of the effects of an oral multivitamin-mineral combination on stress. S. Afr. Med. J. 2000, 90, 1216–1223. [Google Scholar]
- Hallert, C.; Svensson, M.; Tholstrup, J.; Hultberg, B. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Aliment. Pharmacol. Ther. 2009, 29, 811–816. [Google Scholar] [CrossRef]
- Gosney, M.A.; Hammond, M.F.; Shenkin, A.; Allsup, S. Effect of micronutrient supplementation on mood in nursing home residents. Gerontology 2008, 54, 292–299. [Google Scholar] [CrossRef]
- Ford, A.H.; Flicker, L.; Thomas, J.; Norman, P.; Jamrozik, K.; Almeida, O.P. Vitamins B12, B6, and folic acid for onset of depressive symptoms in older men: Results from a 2-year placebo-controlled randomized trial. J. Clin. Psychiatry 2008, 69, 1203–1209. [Google Scholar] [CrossRef]
- Haskell, C.F.; Robertson, B.; Jones, E.; Forster, J.; Jones, R.; Wilde, A.; Maggini, S.; Kennedy, D.O. Effects of a multi-vitamin/mineral supplement on cognitive function and fatigue during extended multi-tasking. Hum. Psychopharmacol.-Clin. Exp. 2010, 25, 448–461. [Google Scholar] [CrossRef] [PubMed]
- Armborst, D.; Metzner, C.; Alteheld, B.; Bitterlich, N.; Rosler, D.; Siener, R. Impact of a Specific Amino Acid Composition with Micronutrients on Well-Being in Subjects with Chronic Psychological Stress and Exhaustion Conditions: A Pilot Study. Nutrients 2018, 10, 551. [Google Scholar] [CrossRef] [PubMed]
- Oliver-Baxter, J.M.; Whitford, H.S.; Turnbull, D.A.; Bond, M.J. Effects of vitamin supplementation on inflammatory markers and psychological wellbeing among distressed women: A randomized controlled trial. J. Integr. Med. 2018, 16, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.; Kirk, J.; Rowsell, R.; Vitetta, L.; Sali, A.; Scholey, A.B.; Pipingas, A. The effect of multivitamin supplementation on mood and stress in healthy older men. Hum. Psychopharmacol. 2011, 26, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Long, S.J.; Benton, D. A double-blind trial of the effect of docosahexaenoic acid and vitamin and mineral supplementation on aggression, impulsivity, and stress. Hum. Psychopharmacol.-Clin. Exp. 2013, 28, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Carroll, D.; Ring, C.; Suter, M.; Willemsen, G. The effects of an oral multivitamin combination with calcium, magnesium, and zinc on psychological well-being in healthy young male volunteers: A double-blind placebo-controlled trial. Psychopharmacology 2000, 150, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; The National Academies Press: Washington, DC, USA, 1998. [Google Scholar]
- Macpherson, H.; Rowsell, R.; Cox, K.H.M.; Reddan, J.; Meyer, D.; Scholey, A.; Pipingas, A. The Effects of Four-Week Multivitamin Supplementation on Mood in Healthy Older Women: A Randomized Controlled Trial. Evid.-Based Complementary Altern. Med. 2016, 2016, 3092828. [Google Scholar] [CrossRef]
- White, D.J.; Cox, K.H.; Peters, R.; Pipingas, A.; Scholey, A.B. Effects of Four-Week Supplementation with a Multi-Vitamin/Mineral Preparation on Mood and Blood Biomarkers in Young Adults: A Randomised, Double-Blind, Placebo-Controlled Trial. Nutrients 2015, 7, 9005–9017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stough, C.; Scholey, A.; Lloyd, J.; Spong, J.; Myers, S.; Downey, L.A. The effect of 90 day administration of a high dose vitamin B-complex on work stress. Psychopharmacology 2011, 26, 470–476. [Google Scholar] [CrossRef]
- Cockle, S.M.; Haller, J.; Kimber, S.; Dawe, R.A.; Hindmarch, I. The influence of multivitamins on cognitive function and mood in the elderly. Aging Ment. Health 2000, 4, 339–353. [Google Scholar] [CrossRef]
- Walker, J.G.; Mackinnon, A.J.; Batterham, P.; Jorm, A.F.; Hickie, I.; McCarthy, A.; Fenech, M.; Christensen, H. Mental health literacy, folic acid and vitamin B12, and physical activity for the prevention of depression in older adults: Randomised controlled trial. Br. J. Psychiatry J. Ment. Sci. 2010, 197, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sasaki, S. Dietary intake and depressive symptoms: A systematic review of observational studies. Mol. Nutr. Food Res. 2010, 54, 471–488. [Google Scholar] [CrossRef] [PubMed]
- Walters, M.; Hackett, K.; Caesar, E.; Isaacson, R.; Mosconi, L. Role of Nutrition to Promote Healthy Brain Aging and Reduce Risk of Alzheimer’s Disease. Curr. Nutr. Rep. 2017, 6, 63–71. [Google Scholar] [CrossRef]
- Barberger-Gateau, P.; Samieri, C.; Allès, B.; Féart, C. Could nutrition prevent the onset of dementia? Current evidence from epidemiological and intervention studies. Neurodegener. Dis. Manag. 2012, 2, 305–314. [Google Scholar] [CrossRef]
- Oulhaj, A.; Jernerén, F.; Refsum, H.; Smith, D.; de Jager, C.A. Omega-3 fatty acid status enhances the prevention of cognitive decline by B vitamins in mild cognitive impairment. J. Alzheimer’s Dis. 2016, 50, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Comerford, K.B. Recent developments in multivitamin/mineral research. Adv. Nutr. 2013, 4, 644–656. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size | Gender | Participant Characteristics | Age range (years) | Intervention | Length of intervention | Biomedical measures | Mood measures a | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall Mood | Depressive Symptoms | Anxiety Symptoms | Stress | |||||||||
| Armborst et al. (2018) | n = 59 tx = 29 pb = 30 | 69% female | Chronic psychological stress | 18–65 | Multivitamin | 12 weeks | N/A | PSQ, VAS | + | |||
| Camfield et al. (2013) | n = 138 tx = 56 pb = 60 | 56% female | Healthy | 20–50 | Multivitamin | 16 weeks | B6, B12, RC folate, homocysteine | PSS | n.s | |||
| Carroll et al. (2000) | n = 80 tx = 40 pb = 40 | 100% male | Healthy | 18–42 | Multivitamin | 28 days | N/A | GHQ, HADS, PSS, rating scales | + | n.s | + | + |
| Cockle et al. (2000) | n = 139 tx = 66 pb = 61 | 63% female | Healthy | 60–83 | Multivitamin | 24 weeks | B1, B2, B6, folate, B12 | POMS | n.s | |||
| Ford et al. (2008) | n = 299 tx = 118 pb = 123* | 100% male | Being treated for, or had a history of hypertension | > 75 | B vitamins only | 2 years | B12, RC folate, homocysteine | BDI | n.s | |||
| Gosney et al. (2008) | n = 73 tx = 26 pb = 33 | Not specified | nursing home residents | > 60 | Multivitamin | 8 weeks | Folate | MADRS, HADS | + b | n.s | ||
| Hallert et al. (2009) | n = 65 tx = 28 pb = 29 | 61% women | coeliac patients | 45–64 | B-group vitamins only | 6 months | Serum folate, B12, homocysteine | PGWB | + c | + c | + c | |
| Harris et al. (2011) | n = 56 tx = 25 pb = 25 | 100% male | sedentary occupation/little exercise | 50–69 | Multivitamin | 8 weeks | N/A | GHQ, DASS, PSS, POMS, VAS | + d | n.s | n.s | n.s |
| Haskell et al. (2010) | n = 226 tx = 106 pb = 110 | 100% female | occasional subjective fatigue | 25–50 | Multivitamin | 9 weeks | Hcy | Quality of life (SF36), CFS, POMS | n.s | |||
| Kennedy et al. (2010) | n = 215 tx = 103 pb = 107 | 100% male | Healthy | 30–55 | Multivitamin | 33 days | N/A | POMS, PSS, GHQ, Bond Lader, VAS | + e | n.s | + | |
| Kennedy et al. (2011) | n = 215 tx = 94 pb = 104 | 100% male | Healthy | 30–55 | Multivitamin | 28 days | N/A | Bond Lader, VAS | ||||
| Long and Benton (2013) | n = 101 tx = 43 + 41 pb = 42 | 100% male | Healthy | M= 20.9 | Multivitamin | 12 weeks | N/A | Picture frustration, Buss-Perry Aggression Scale, PSS | + | |||
| Macpherson et al. (2016) | n = 76 tx = 37 pb = 36 | 100% female | Healthy | 50–75 | Multivitamin | 4 weeks | N/A | STAI, GHQ, HADS, Bond-Lader, VAS, PSS, CFS | n.s | n.s | n.s | n.s |
| Oliver-Baxter et al. (2018) | n = 50 tx = 22 pb = 28 | 100% female | Elevated psychological distress | 25–45 | Multivitamin | 8 weeks | Folic acid | STPI | n.s | n.s | ||
| Pipingas et al. (2013) | n = 138 tx = 56 pb = 60 | 56% female | Healthy | 20–50 | Multivitamin | 16 weeks | N/A | GHQ, POMS, CFS, Bond-Lader, VAS, STAI | n.s | n.s | + f | |
| Schlebusch et al. (2000) | n = 300 tx = 151 pb = 149 | Not specified | Highly stressed employees | 18–65 | Multivitamin | 30 days | N/A | HARS, PGWB, VAS, BSI | + | + | + | |
| Stough et al. (2011) | n = 80 tx = 20 + 22 pb = 18 | 66% female | Healthy | M = 42.2 | Multivitamin | 90 days | N/A | STAI, POMS, PSQ | n.s | n.s | n.s | + |
| White et al. (2015) | n = 58 tx = 28 pb = 30 | 50% female | Healthy | 18–40 | Multivitamin | 4 weeks | B6, B12, folate, homocysteine | POMS, PSS, VAS, STAI | n.s | + | n.s | n.s |
| B1 (mg) | B2 (mg) | B3 (mg) | B5 (mg) | B6 (mg) | B7 (µg) | B9 (µg) | B12 (µg) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Other name | Thiamine | Riboflavin | Niacin, Nicotin- amide | Pantothenic acid | Biotin | Folate, Folic acid | Cyanocobalamin | ||||
| Recommended Daily Allowance (19–50 years) | 1.1 (M) 1.2 (F) | 1.3 (M) 0.9 (F) | 16 (M) 14 (F) | 5^ | 1.3 | 30^ | 400 | 2.4 | |||
| Study Daily Intake | No. of B vits | Other constituents of supplement | |||||||||
| Camfield et al. (2013) Harris et al. (2011) Pipingas et al. (2013) | M | 30 | 30 | 30 | 64.13 | 24.8 | - | 500 | 30 | 7 | Vitamins C, D, E, Choline, Calcium, Iron, Magnesium, Selenium, Zinc, Korean ginseng, Siberian ginseng, Ginkgo Biloba, Chamomile, Green Tea, St. Mary’s thistle |
| F | 50 | 50 | 50 | 68.7 | 41.14 | - | 500 | 50 | |||
| Carroll et al. (2000) Kennedy et al. (2010) Kennedy et al. (2011) | 15 | 15 | 50 | 23 | 10 | 15 | 400 | 10 | 8 | Vitamin C, Calcium, Magnesium, Zinc | |
| Armborst et al. (2018) | 25 | 25 | 100 | 100 | 25 | - | 800 | 50 | 7 | Taurine, L- ornithine, L-phenylalanine, L-tyrosine, Vitamin C, ß-carotene, Magnesium, Zinc, Selenium, Chrome, Molybdenum | |
| Cockle et al. (2000) | 14 | 16 | 180 | - | 22 | - | 4000 | 30 | 6 | Vitamins A, C | |
| Ford et al. (2008) | - | - | - | - | 25 | - | 2000 | 400 | 3 | N/A | |
| Gosney et al. (2008) | 4.8 | 5.6 | 56 | 20 | 12 | 120 | 2400 | 800 | 8 | Vitamins A, C, D, E | |
| Hallert et al. (2009) | - | - | - | - | 3 | - | 800 | 500 | 3 | N/A | |
| Haskell et al. (2010) | 4.2 | 4.7 | 54 | 18 | 6 | - | 600 | 3 | 7 | Vitamins A, C, D, E, K1, Calcium, Phosphorus, Chromium, Copper, Fluoride, Iodine, Iron, Magnesium, Manganese, Molybdenum, Selenium, Zinc | |
| Long and Benton (2013) | 1.4 | 1.75 | 20 | 7.5 | 2 | 62 | 200 | 2.5 | 8 | Vitamins A, C, D, E, K, calcium, phosphorus, magnesium, potassium, chloride, iron, iodine, copper, manganese, chromium, molybdenum, selenium, zinc, lutein. | |
| Macpherson et al. (2016) | 30 | 30 | 20 | 70 | 30 | 150 | 500 | 115 | 8 | Vitamins A, C, D, E, K, Zinc, Calcium, Magnesium, Selenium, Molybdenum, Chromium, Manganese, Iron, Copper, Iodine, L. rhamnosus, L. acidophilus, Bifidobacterium longum, Citrus bioflavonoids extract, cranberry Pacran, St. Mary’s thistle, damiana, skullcap, grape seed, nettle, Coenzyme Q10, globe artichoke, black cohosh, turmeric, ashwagandha, hawthorn, silicon, Bacopa monnieri, Lecithin, Spearmint oil, bilberry, marigold | |
| Oliver-Baxter et al. (2018) | 12.5 | 12.5 | 25 | 37.5 | 25 | 37.5 | 150 | 25 | 8 | Vitamin C, Magnesium oxide, Zinc, Withania somnifera | |
| Schlebusch et al. (2000) | 15 | 15 | 50 | 23 | 10 | 150 | - | 10 | 7 | Vitamin C, Calcium, Magnesium | |
| Stough et al. (2011) | 75 | 10 | 100 | 68.7 | 25 | 20 | 150 | 30 | 7 | Vitamins C, E, Calcium, Magnesium, Potassium, Avena sativa, Passion flower, Lecithin, Choline, Inositol | |
| White et al. (2015) | 18.54 | 15 | 50 | 23 | 10 | 15 | 400 | 10 | 7 | Vitamin C, Calcium, Magnesium, Zinc |
| Study | Group | Vitamin B6 | Folate (RC) | Folate (Serum) | Vitamin B12 | Homocysteine |
|---|---|---|---|---|---|---|
| Armborst et al. (2018) | Placebo | - | - | 9.48 (3.08) | - | - |
| Active | - | - | 9.67 (4.13) | - | - | |
| Camfield et al. (2013) | Placebo | 114.08 (10.27) | 944.96 (21.94) | - | 314.60 (14.48) | 10.6137 (0.22) |
| Active | 111.70 (9.36) | 933.27 (34.99) | - | 289.25 (12.11) | 10.8444 (0.35) | |
| Cockle et al. (2000) | Placebo Males | 235.64 (75.74) | - | 9.74 (5.66) | 304.10 (160.93) | - |
| Placebo Females | 239.02 (54.95) | - | 9.31 (4.13) | 323.44 (150.06) | - | |
| Active Males | 243.74 (50.06) | - | 8.63 (3.70) | 307.26 (86.29) | - | |
| Active Females | 230.72 (46.85) | - | 9.10 (4.76) | 365.66 (156.38) | - | |
| Ford et al. (2008) | Placebo | - | - | 24.22 (7.44) | 253.30 (115.10) | 13.06 (3.83) |
| Active | - | - | 24.00 (7.50) | 253.10 (107.50) | 13.59 (4.43) | |
| Gosney et al. (2008) | Overall | - | - | 5.88 (range 0.9–39.8) | - | - |
| Hallert et al. (2009) | Placebo | - | - | 14.8 (range 7.7–23.4) | 431 (174–734) | 11.4 (7.4–21.9) |
| Active | - | - | 12.9 (range 6.7–44) | 326 (141–510) | 11.70 (7.8–23.0) | |
| Haskell et al. (2010) | Placebo | - | - | - | - | 10.93 (0.53) |
| Active | - | - | - | - | 10.94 (0.46) | |
| Oliver-Baxter et al. (2018) | Placebo | - | - | 27.1 (13.9) | - | - |
| Active | - | - | 28.2 (16.7) | - | - | |
| White et al. (2015) | Placebo | 85.00 (34.02) | 944.25 (190.09) | - | 304.88 (75.34) | 11.43(2.24) |
| Active | 84.95 (23.73) | 954.63 (188.58) | - | 301.04 (82.22) | 11.78 (1.81) |
| Vitamin B1 | Vitamin B2 | Vitamin B6 | Vitamin B12 | Folate (RC) | Folate (serum) | Homocysteine | |
|---|---|---|---|---|---|---|---|
| Armborst et al. (2018) | + | ||||||
| Camfield et al. (2013) | + | + | + | - | |||
| Cockle et al. (2000) | + | + | + | + | +^ | ||
| Ford et al. (2008) | + | + | - | ||||
| Gosney et al. (2008) | +^ | ||||||
| Hallert et al. (2009) | + | + | - | ||||
| Haskell et al. (2010) | - | ||||||
| Oliver-Baxter et al. (2018) | + | ||||||
| White et al. (2015) | + | + | + | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, L.M.; Pipingas, A.; White, D.J.; Gauci, S.; Scholey, A. A Systematic Review and Meta-Analysis of B Vitamin Supplementation on Depressive Symptoms, Anxiety, and Stress: Effects on Healthy and ‘At-Risk’ Individuals. Nutrients 2019, 11, 2232. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092232
Young LM, Pipingas A, White DJ, Gauci S, Scholey A. A Systematic Review and Meta-Analysis of B Vitamin Supplementation on Depressive Symptoms, Anxiety, and Stress: Effects on Healthy and ‘At-Risk’ Individuals. Nutrients. 2019; 11(9):2232. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092232
Chicago/Turabian StyleYoung, Lauren M, Andrew Pipingas, David J White, Sarah Gauci, and Andrew Scholey. 2019. "A Systematic Review and Meta-Analysis of B Vitamin Supplementation on Depressive Symptoms, Anxiety, and Stress: Effects on Healthy and ‘At-Risk’ Individuals" Nutrients 11, no. 9: 2232. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092232