The Influence of Caffeine Expectancies on Simulated Soccer Performance in Recreational Individuals

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Pre-Experimental Procedures
2.3. VO2MAX and Brief Familiarisation
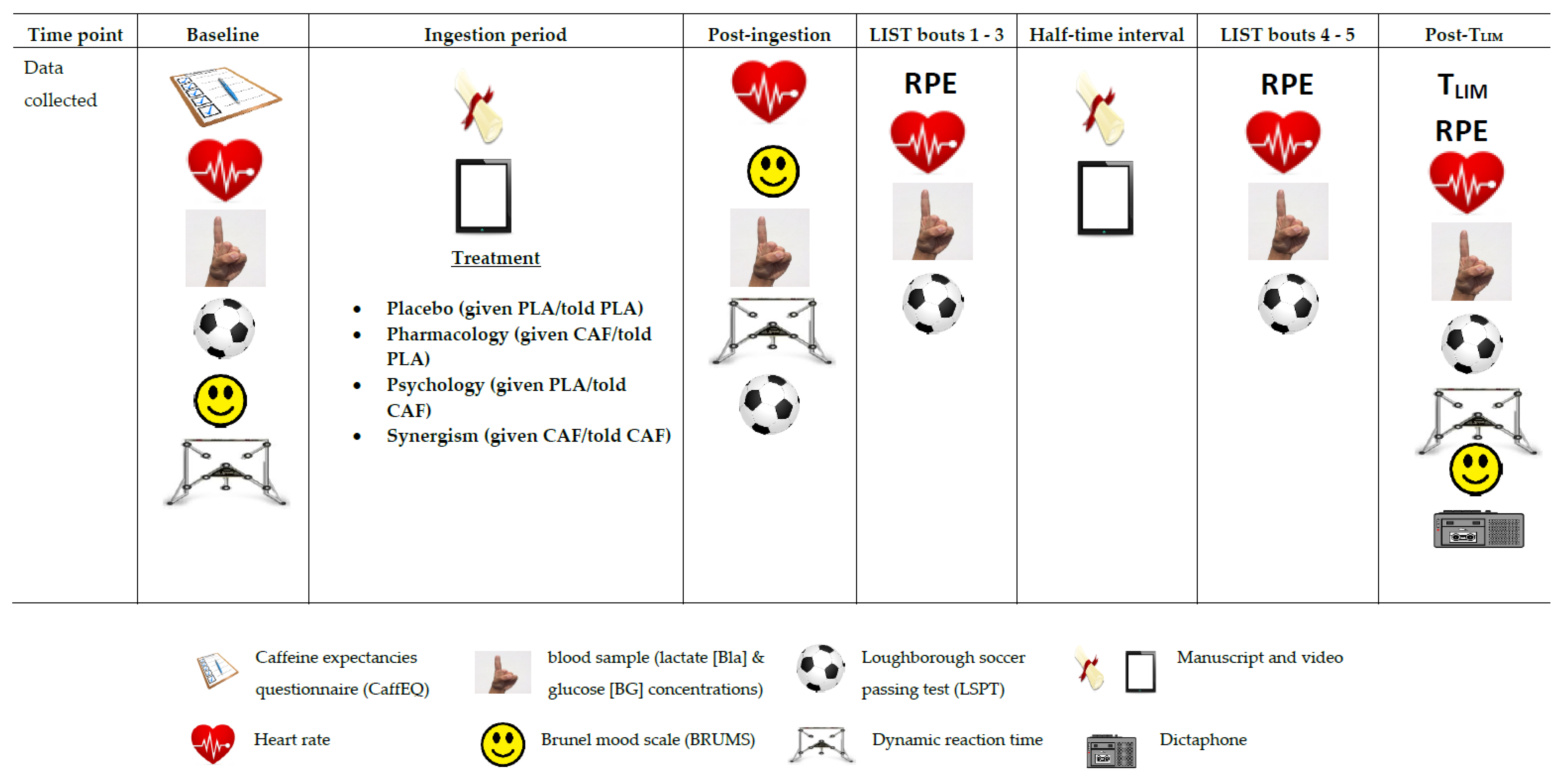
2.4. Full Familiarisation and Experimental Trials
2.5. Treatments
2.6. Dynamic Reaction Time (DRT)
2.7. Brunel Mood Scale (BRUMS)
2.8. Caffeine Expectancies Questionnaire (CaffEQ)
2.9. Dictaphone
2.10. Qualitative Analysis
- (1)
- An in-depth description of the data collection and analysis procedure.
- (2)
- Involvement of A.H and M.F.H in guiding the qualitative process, by making implicit enquiries to the lead researcher (A.S) about the data collection/analysis procedure. This assisted in minimising biases, whilst improving the clarity of interpretations.
- (3)
2.11. Statistical Analysis
3. Results
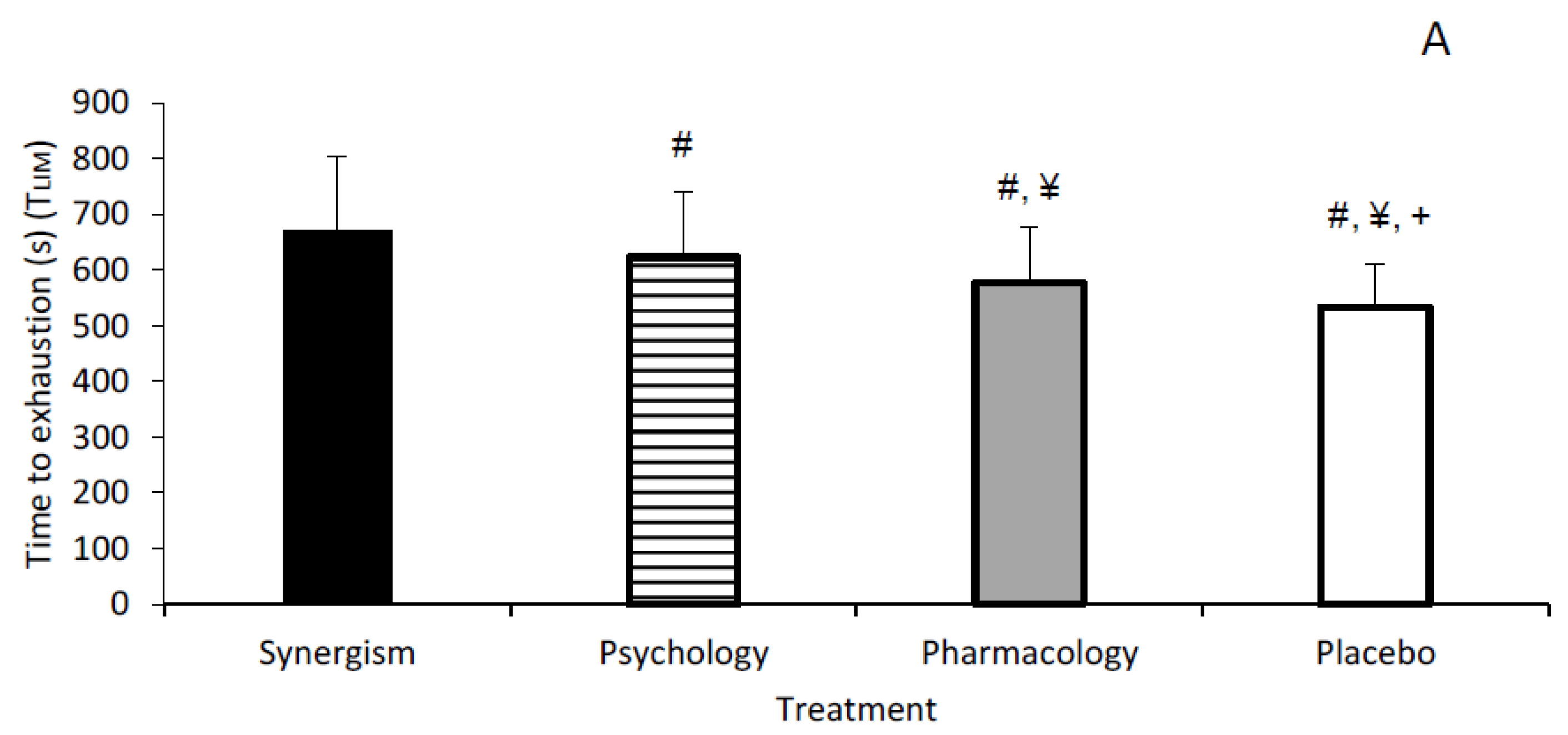
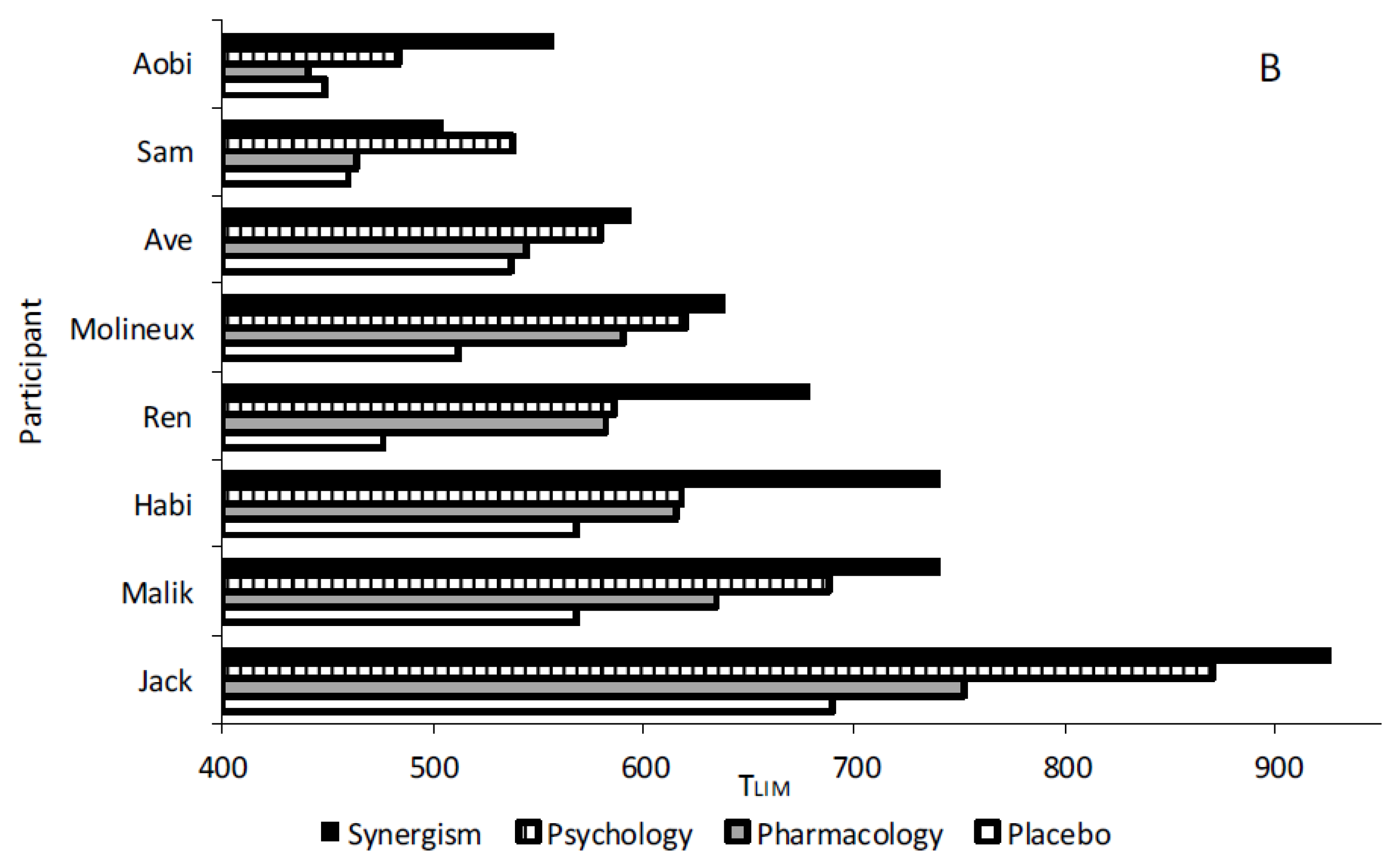
3.1. Endurance Capacity (TLIM)
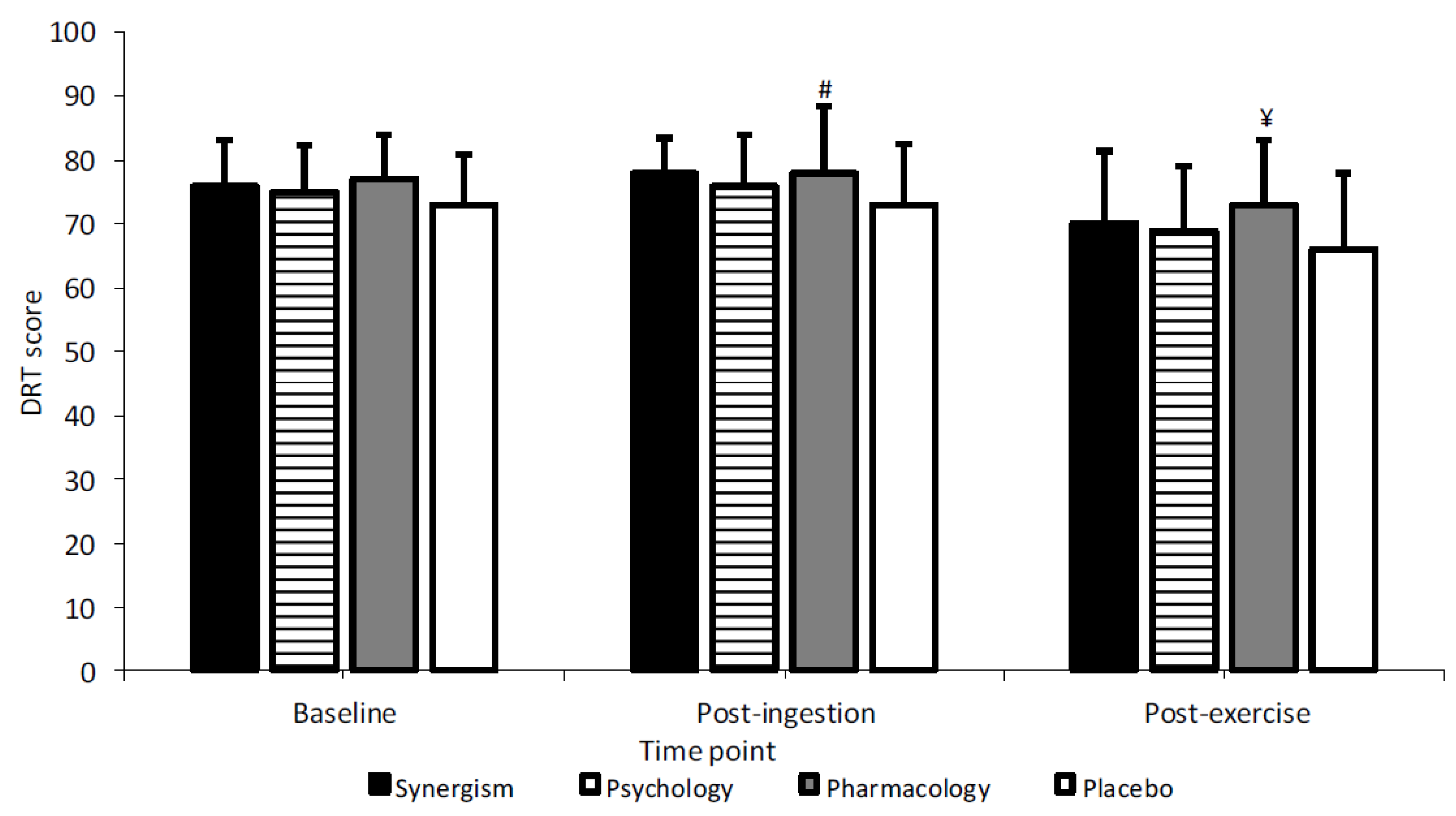
3.2. Dynamic Reaction Time (DRT)
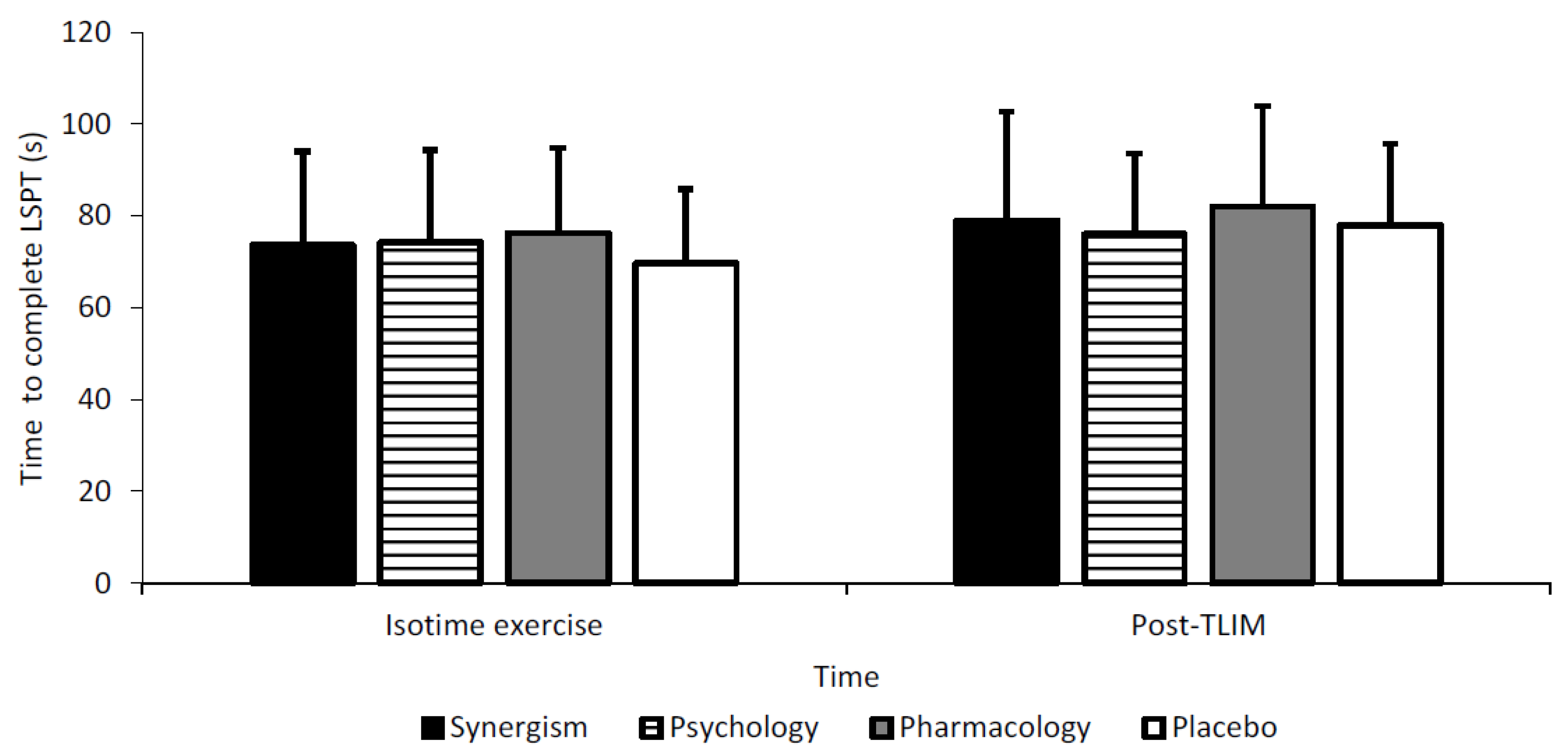
3.3. Loughborough Soccer Passing Test (LSPT)
3.4. Heart Rate
3.5. Blood Variables
3.6. BRUMS
3.7. CaffEQ
4. Qualitative Findings
5. Discussion
5.1. Qualitative Implications
5.1.1. TLIM
5.1.2. DRT and LSPT
5.2. Broader Applications
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bloms, L.P.; Fitzgerald, J.S.; Short, M.W.; Whitehead, J.R. The Effects of Caffeine on Vertical Jump Height and Execution in Collegiate Athletes. J. Strength Cond. Res. 2016, 30, 1855–1861. [Google Scholar] [CrossRef] [PubMed]
- Glaister, M.; Muniz-Pumares, D.; Patterson, S.D.; Foley, P.; McInnes, G. Caffeine supplementation and peak anaerobic power output. Eur. J. Sport Sci. 2015, 15, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Del Coso, J.; Munoz-Fernandez, V.E.; Munoz, G.; Fernandez-Elias, V.E.; Ortega, J.F.; Hamouti, N.; Barbero, J.C.; Munoz-Guerra, J. Effects of a Caffeine-Containing Energy Drink on Simulated Soccer Performance. PLoS ONE 2012, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lara, B.; Gonzalez-Millan, C.; Salinero, J.J.; Abian-Vicen, J.; Areces, F.; Barbero-Alvarez, J.C.; Munoz, V.; Portillo, L.J.; Gonzalez-Rave, J.M.; Del Coso, J. Caffeine-containing energy drink improves physical performance in female soccer players. Amino Acids 2014, 46, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.R.; Ziegenfuss, T.; Kalman, D.; Kreider, R.; Campbell, B.; Wilborn, C.; Taylor, L.; Willougby, D.; Stout, J.; Graves, B.S.; et al. International society of sports nutrition position stand: Caffeine and performance. J. Int. Soc. Sports Nutr. 2010, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.; Kingsley, M. The efficacy of acute nutritional interventions on soccer skill performance. Sports Med. 2014, 44, 957–970. [Google Scholar] [CrossRef] [PubMed]
- Foskett, A.; Ali, A.; Gant, N. Caffeine enhances cognitive function and skill performance during simulated soccer activity. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 410–423. [Google Scholar] [CrossRef]
- Jordan, J.B.; Korgaokar, A.; Farley, R.S.; Coons, J.M.; Caputo, J.L. Caffeine supplementation and reactive agility in elite youth soccer players. Pediatric Exerc. Sci. 2014, 26, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Fredholm, B.B.; Battig, K.; Holmen, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 1990, 51, 83–133. [Google Scholar]
- Pickering, C.; Kiely, J. Are the Current Guidelines on Caffeine Use in Sport Optimal for Everyone? Inter-individual Variation in Caffeine Ergogenicity, and a Move Towards Personalised Sports Nutrition. Sports Med. 2018, 48, 7–16. [Google Scholar] [CrossRef]
- Reilly, T.; Thomas, V. A motion analysis of work-rate in different positional roles in professional football match-play. J. Hum. Mov. Stud. 1976, 2, 87–89. [Google Scholar]
- Mohr, M.; Krustrup, P.; Bangsbo, J. Match performance of high-standard soccer players with special reference to development of fatigue. J. Sports Sci. 2003, 21, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolen, T.; Chamari, K.; Castagna, C.; Wisloff, U. Physiology of soccer: An update. Sports Med. 2005, 35, 501–536. [Google Scholar] [CrossRef] [PubMed]
- Vescovi, J.D.; Favero, T.G. Motion characteristics of women’s college soccer matches: Female Athletes in Motion (FAiM) study. Int. J. Sports Physiol. Perform. 2014, 9, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on exercise testing: A meta-analysis. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 626–646. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Grgic, J. Caffeine and Exercise: What Next? Sports Med. 2019, 49, 1007–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, F.G.; Iaia, M.; Arcelli, E.; Cavaggioni, L.; Rampinini, E. Goal scoring patterns in major European soccer leagues. Sport Sci. Health 2013, 9, 151–153. [Google Scholar] [CrossRef]
- Shabir, A.; Hooton, A.; Tallis, J.; Higgins, M.F. The Influence of Caffeine Expectancies on Sport, Exercise, and Cognitive Performance. Nutrients 2018, 10, 1528. [Google Scholar] [CrossRef] [PubMed]
- Saunders, B.; de Oliveira, L.F.; da Silva, R.P.; de Salles Painelli, V.; Goncalves, L.S.; Yamaguchi, G.; Mutti, T.; Maciel, E.; Roschel, H.; Artioli, G.G.; et al. Placebo in sports nutrition: A proof-of-principle study involving caffeine supplementation. Scand. J. Med. Sci. Sports 2017, 27, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Beedie, C.J.; Foad, A.J. The placebo effect in sports performance: A brief review. Sports Med. 2009, 39, 313–329. [Google Scholar] [CrossRef]
- Beedie, C.J.; Stuart, E.M.; Coleman, D.A.; Foad, A.J. Placebo effects of caffeine on cycling performance. Med. Sci. Sports Exerc. 2006, 38, 2159–2164. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Lyons, M.; Hankey, J. Placebo effects of caffeine on short-term resistance exercise to failure. Int. J. Sport Physiol. 2009, 4, 244–253. [Google Scholar] [CrossRef]
- Harrell, P.T.; Juliano, L.M. Caffeine expectancies influence the subjective and behavioral effects of caffeine. Psychopharmacology 2009, 207, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Denson, T.F.; Jacobsen, M.; von Hippel, W.; Kemp, R.I.; Mak, T. CAF expectancies but not CAF reduce depletion-induced aggression. Psychol. Addict. Behav. 2012, 26, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Pollo, A.; Carlino, E.; Benedetti, F. The top-down influence of ergogenic placebos on muscle work and fatigue. Eur. J. Neurosci. 2008, 28, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Tallis, J.; Muhammad, B.; Islam, M.; Duncan, M.J. Placebo effects of caffeine on maximal voluntary concentric force of the knee flexors and extensors. Muscle Nerve 2016, 54, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Foad, A.J.; Beedie, C.J.; Coleman, D.A. Pharmacological and psychological effects of caffeine ingestion in 40-km cycling performance. Med. Sci. Sports Exerc. 2008, 40, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, C.; Asano, R.Y.; Russi de Lima, F.D.; Pinheiro, F.A.; Alvarenga, F.; Ugrinowitsch, C.; Pires, F.O. Caffeine effects on VO2max test outcomes investigated by a placebo perceived-as-caffeine design. Nutr. Health 2017, 23, 231–238. [Google Scholar] [CrossRef]
- Pires, F.O.; dos Anjos, C.A.S.; Covolan, R.J.M.; Fontes, E.B.; Noakes, T.D.; Gibson, A.S.C.; Magalhaes, F.H.; Ugrinowitsch, C. Caffeine and placebo Improved Maximal Exercise Performance Despite Unchanged Motor Cortex Activation and Greater Prefontal Cortex Deoxygenation. Front. Physiol. 2018. [Google Scholar] [CrossRef]
- Dawkins, L.; Shahzad, F.Z.; Ahmed, S.S.; Edmonds, C.J. Expectation of having consumed caffeine can improve performance and mood. Appetite 2011, 57, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Oei, A.; Hartley, L.R. The effects of caffeine and expectancy on attention and memory. Hum. Psychopharmacol. 2005, 20, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Fillmore, M.; Vogel-Sprott, M. Expected effect of caffeine on motor performance predicts the type of response to placebo. Psychopharmacology 1992, 106, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Burke, T.M.; Markwald, R.R.; McHill, A.W.; Chinoy, E.D.; Snider, J.A.; Bessman, S.C.; Jung, C.M.; O’Neill, J.S.; Wright, K.P., Jr. Effects of caffeine on the human circadian clock in vivo and in vitro. Sci. Transl. Med. 2015, 16, 305. [Google Scholar] [CrossRef] [PubMed]
- Schicatano, E.J.; Blumenthal, T.D. The effects of different doses of caffeine on habituation of the human acoustic startle reflex. Pharmacol. Biochem. Behav. 1995, 52, 231–236. [Google Scholar] [CrossRef]
- Svenningsson, P.; Nomikos, G.G.; Fredholm, B.B. The stimulatory action and the development of tolerance to caffeine is associated with alterations in gene expression in specific brain regions. J. Neurosci. 1999, 19, 4011–4022. [Google Scholar] [CrossRef] [PubMed]
- Pickering, G.; Kiely, J. What Should We Do About Habitual Caffeine Use in Athletes? Sports Med. 2019, 49, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, C.W.; Nuttall, F.E.; Williams, C. The Loughborough Intermittent Shuttle Test: A field test that simulates the activity pattern of soccer. J. Sports Sci. 2000, 18, 97–104. [Google Scholar] [CrossRef]
- Elliman, N.A.; Ash, J.; Green, M.W. Pre-existent expectancy effects in the relationship between caffeine and performance. Appetite 2010, 55, 355–358. [Google Scholar] [CrossRef]
- Van Soeren, M.H.; Graham, T.E. Effect of caffeine on metabolism, exercise endurance, and catecholamine responses after withdrawal. J. Appl. Physiol. 1998, 85, 1493–1501. [Google Scholar] [CrossRef] [Green Version]
- Irwin, C.; Desbrow, B.; Ellis, A.; O’Keeffe, B.; Grant, G.; Leveritt, M. Caffeine withdrawal and high-intensity endurance cycling performance. J. Sports Sci. 2011, 29, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, A.L.; Lopes-Silva, J.P.; Bertuzzi, R.; Casarini, D.E.; Arita, D.Y.; Bishop, D.J.; Lima-Silva, A.E. Effect of Time of Day on Performance, Hormonal and Metabolic Response during a 1000-m Cycling Time Trial. PLoS ONE 2014, 9, e109954. [Google Scholar] [CrossRef]
- Strasbourg. Testing Physical Fitness, Eurofit Experimental Battery Provisional Handbook, Sports Section of the Council of Europe; Bitworks Design and Consultancy: Cheltenham, UK, 1983. [Google Scholar]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- McGregor, S.J.; Nicholas, C.W.; Lakomy, H.K.A.; Williams, C. The influence of intermittent high intensity shuttle running and fluid ingestion on the performance of a soccer skill. J. Sports Sci. 1990, 17, 895–903. [Google Scholar] [CrossRef]
- Online Tone Generator. Available online: http://www.szynalski.com/tone-generator/ (accessed on 1 July 2017).
- Lane, A.M.; Lane, H.J. Predictive effectiveness of mood measures. Percept. Mot. Ski. 2002, 94, 785–791. [Google Scholar] [CrossRef]
- Graham, T.E.; Spriet, L.L. Metabolic, catecholamine, and exercise performance responses to various doses of caffeine. J. Appl. Physiol. 1995, 78, 867–874. [Google Scholar] [CrossRef]
- The Science of Caffeine: The Worlds Most Popular Drug. Available online: https://www.youtube.com/watch?v=YuJOhpNS0IY (accessed on 1 July 2017).
- Fat Albert “JATO” Take-Off 2009. Available online: https://www.youtube.com/watch?v=VHOvoO-6nWQ (accessed on 1 July 2017).
- Huntley, E.D.; Juliano, L.M. Caffeine Expectancy Questionnaire (CaffEQ): Construction, psychometric properties, and associations with caffeine use, caffeine dependence, and other related variables. Psychol. Assess 2011, 24, 592–607. [Google Scholar] [CrossRef]
- Ando, S.; Kida, N.; Oda, S. Central and peripheral visual reaction time of soccer players and nonathletes. Percept. Mot. Ski. 2001, 92, 786–794. [Google Scholar] [CrossRef]
- Ricotti, L.; Rigosa, J.; Niosi, A.; Menciassi, A. Analysis of balance, rapidity, force and reaction times of soccer players at different levels of competition. PLoS ONE 2013, 8, e77264. [Google Scholar] [CrossRef]
- Ellison, P.H.; Sparks, S.A.; Murphy, P.N.; Carnegie, E.; Marchant, D.C. Determining eye-hand coordination using the sport vision trainer: An evaluation of test-retest reliability. Res. Sports Med. 2014, 22, 36–48. [Google Scholar] [CrossRef]
- Terry, P.C.; Lane, A.M.; Fogarty, G.J. Construct Validity of the POMS-A for use with adults. J. Sport Exerc. Psychol. 2003, 4, 125–139. [Google Scholar] [CrossRef]
- Brooks, J.; McCluskey, S.; Turley, E.; King, N. The Utility of Template Analysis in Qualitative Psychology Research. Qual. Res. Psychol. 2015, 12, 202–222. [Google Scholar] [CrossRef]
- Weber, R.P. Basic Content Analysis; Sage: Beverly Hills, CA, USA, 1990. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Publishing Company: Chicago, IL, USA, 1967. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Jackson, S.A. Factors influencing the occurrence of flow state in elite athletes. J. Appl. Sport Psychol. 1995, 4, 161–180. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publication: Newbury Park, CA, USA, 1985. [Google Scholar]
- Patton, M. Qualitative Evaluation and Research Methods; Sage: Beverly Hills, CA, USA, 1990. [Google Scholar]
- van Manen, M. Researching Lived Experience: Human Science for and Action Sensitive Pedagogy; SUNY Press: Albany, NY, USA, 1990. [Google Scholar]
- Field, A. (Ed.) Reliability Analysis, 2nd ed.; Discovering Statistics Using SPSS; Sage Publication: London, UK, 2005. [Google Scholar]
- Armstrong, R.A. When to use the Bonferroni correction. Ophalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. Camb. Philos. Soc. 2007, 82, 591–605. [Google Scholar] [CrossRef]
- Ivarsson, A.; Johnson, U.; Podlog, L. Psychological predictors of injury occurrence: A prospective investigation of professional Swedish soccer players. J. Sport Rehabil. 2013, 22, 19–26. [Google Scholar] [CrossRef]
- Higgins, M.F.; Wilson, S.; Hill, C.; Price, M.J.; Duncan, M.; Tallis, J. Evaluating the effects of caffeine and sodium bicarbonate, ingested individually or in combination, and a taste-matched placebo on high-intensity cycling capacity in healthy males. Appl. Physiol. Nutr. Metab. 2016, 41, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Higgins, M.F.; James, R.S.; Price, M.J. Familiarisation to and reproducibility of cycling at 110% peak power output. J. Sports Med. Phys. Fit. 2014, 54, 139–146. [Google Scholar]
- Benedetti, F.; Mayberg, H.S.; Wager, T.D.; Stohler, C.S.; Zubieta, J.K. Neurobiological mechanisms of the placeo effect. J. Neurosci. 2005, 25, 10390–10402. [Google Scholar] [CrossRef]
- Pageaux, B.; Lepers, R.; Dietz, K.C.; Marcora, S.M. Response inhibition impairs subsequent self-paced endurance performance. Eur. J. Appl. Physiol. 2014, 114, 1095–1105. [Google Scholar] [CrossRef]
- Pageaux, B.; Lepers, R. Fatigue Induced by Physical and Mental Exertion Increases Perception of Effort and Impairs Subsequent Endurance Performance. Front. Physiol. 2016, 7, 587. [Google Scholar] [CrossRef] [PubMed]
- Broelz, E.K.; Enck, P.; Niess, A.M.; Schneeweiss, P.; Wolf, S.; Weimer, K. The neurobiology of placebo effects in sports: EEG frontal alpha asymmetry increases in response to a placebo ergogenic aid. Sci. Rep. 2019, 9, 2381. [Google Scholar] [CrossRef] [PubMed]
- Smirmaul, B.P.C.; Dantas, J.L.; Nakamura, F.Y.; Pereira, G. The psychobiological model: A new explanation to intensity regulation and (in)tolerance in endurance exercise. Rev. Bras. Educ. Fís. 2013, 27, 333–340. [Google Scholar] [CrossRef]
- Meeusen, R.; Roelands, B.; Spriet, L.L. Caffeine, exercise and the brain. Nestle Nutr. Inst. Workshop Ser. 2013, 76, 1–12. [Google Scholar] [PubMed]
- Duvnjak-Zaknich, D.M.; Dawson, B.T.; Wallman, K.E.; Henry, G. Effect of caffeine on reactive agility time when fresh and fatigued. Med. Sci. Sports Exerc. 2011, 43, 1523–1530. [Google Scholar] [CrossRef]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef]
- Plaskett, C.J.; Cafarelli, E. Caffeine increases endurance and attenuates force sensation during submaximal isometric contractions. J. Appl. Physiol. 2001, 91, 1535–1544. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L. Clinical pharmacology of caffeine. Annu. Rev. Med. 1990, 41, 277–288. [Google Scholar] [CrossRef]
- Gant, N.; Ali, A.; Foskett, A. The influence of caffeine and carbohydrate coingestion on simulated soccer performance. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 191–197. [Google Scholar] [CrossRef]
- Coyle, E.F. Physiological determinants of endurance exercise performance. J. Sci. Med. Sport 1999, 2, 181–189. [Google Scholar] [CrossRef]
- Sahlin, K. Muscle glucose metabolism during exercise. Ann. Med. 1990, 22, 85–89. [Google Scholar] [PubMed]
- Burton, D.A.; Stokes, K.; Hall, G.M. Physiological effects of exercise. BJA Educ. 2004, 4, 185–188. [Google Scholar] [CrossRef]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neurol. 1908, 18, 459–482. [Google Scholar] [CrossRef] [Green Version]
- Bchir, F.; Dogui, M.; Ben Fradj, R.; Arnaud, M.J.; Saguem, S. Differences in pharmacokinetic and electroencephalographic responses to caffeine in sleep-sensitive and non-sensitive subjects. Comptes Rendus Biol. 2006, 329, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Hartley, T.R.; Sung, B.H.; Pincomb, G.A.; Whitsett, T.L.; Wilson, M.F.; Lovallo, W.R. Hypertension risk status and effect of caffeine on blood pressure. Hypertension 2000, 36, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Green, P.J.; Kirby, R.; Suls, J. The effects of caffeine on blood pressure and heart rate: A review. Ann. Behav. Med. 1996, 18, 201–216. [Google Scholar] [CrossRef]
- Abraham, J.; Mudd, J.O.; Kapur, N.K.; Klein, K.; Champion, H.C.; Wittstein, I.S. Stress cardiomyopathy after intravenous administration of catecholamines and beta-receptor agonists. J. Am. Coll. Cardiol. 2009, 53, 1320–1325. [Google Scholar] [CrossRef]
- Lane, J.D.; Pieper, C.F.; Phillips-Bute, B.G.; Bryant, J.E.; Kuhn, C.M. Caffeine affects cardiovascular and neuroendocrine activation at work and home. Psychosom. Med. 2002, 64, 595–603. [Google Scholar]
- Van Soeren, M.; Mohr, T.; Kjaer, M.; Graham, T.E. Acute effects of caffeine ingestion at rest in humans with impaired epinephrine responses. J. Appl. Physiol. 1996, 80, 999–1005. [Google Scholar] [CrossRef]
- Southward, K.; Rutherfurd-Markwick, K.; Badenhorst, C.; Ali, A. The Role of Genetics in Moderating the Inter-Individual Differences in the Ergogenicity of Caffeine. Nutrients 2018, 10, 1352. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Palmer, A.A.; de Wit, H. Genetics of caffeine consumption and responses to caffeine. Psychopharmacology 2010, 211, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | 1 min | 2 min | 3 min | 4 min | 5 min | 6 min | 7 min | Post-Exercise (Placebo) | Post-Exercise (Pharmacology) | Post-Exercise (Psychology) | Post-Exercise (Synergism) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Synergism | 2 | 3 | 5 | 6 | 8 | 10 | 11 | 14 | 15 | 17 | 18* |
| Psychology | 2 | 3 | 5 | 7 | 9 | 10 | 12 | 15 | 16 | 18* | - |
| Pharmacology | 2 | 4 | 6 | 8 | 10 | 11 | 13 | 17 | 18* | - | - |
| Placebo | 2 | 4 | 6 | 8 | 10 | 12 | 14 | 18* | - | - | - |
| Treatment | Post-Exercise (Placebo) | Post-Exercise (Pharmacology) | Post-Exercise (Psychology) | Post-Exercise (Synergism) |
|---|---|---|---|---|
| Heart Rate (HR; bpm−1) | ||||
| Synergism | 147 | 159 | 172 | 185* |
| Psychology | 160 | 173 | 187* | |
| Pharmacology | 172 | 186* | - | - |
| Placebo | 184* | - | - | - |
| Blood Lactate (BLa; mmol/L) | ||||
| Synergism | 6.8 | 7.3 | 7.9 | 8.5* |
| Psychology | 7.4 | 7.9 | 8.6* | |
| Pharmacology | 8.4 | 9.0* | - | - |
| Placebo | 8.6* | - | - | - |
| Blood Glucose (BG; mmol/L) | ||||
| Synergism | 3.5 | 3.8 | 4.1 | 4.4* |
| Psychology | 3.4 | 3.7 | 4.0* | - |
| Pharmacology | 3.8 | 4.1* | - | - |
| Placebo | 4.0* | - | - | - |
| Participant | Responses Based on |
|---|---|
| 1-Jack | Caffeine in general |
| 2-Malik | Energy drinks |
| 3-Habi | Soft drinks |
| 4-Ren | Energy drinks |
| 5-Molineux | Other (not specified) |
| 6-Ave | Caffeine in general |
| 7-Sam | Energy drinks |
| 8-Aobi | Coffee, soft drinks and tea |
| Withdrawal | Energy | Mood Enhancement | Appetite Suppression | Physical Performance Enhancement | Anxiety/Negative Physical Effects | Sleep Disturbances | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participant | T1 | T3 | T1 | T3 | T1 | T3 | T1 | T3 | T1 | T3 | T1 | T3 | T1 | T3 |
| Jack | 2 | 2 | 3 | 3 | 3 | 3 | 2 | 2 | 3 | 3 | 2 | 1 | 1 | 1 |
| Malik | 0 | 0 | 2 | 2 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 |
| Habi | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ren | 3 | 2 * | 4 | 4 | 4 | 3 | 3 | 2 * | 4 | 4 | 1 | 3 * | 3 | 3 |
| Molineux | 2 | 3 * | 2 | 3 * | 1 | 2 | 2 | 3 * | 3 | 3 | 2 | 3 * | 1 | 2 |
| Ave | 0 | 1 | 2 | 2 | 1 | 1 | 0 | 3 * | 2 | 3 * | 0 | 1 | 0 | 2 * |
| Sam | 1 | 0 | 3 | 2 * | 1 | 1 | 0 | 1 | 2 | 3 * | 0 | 0 | 0 | 0 |
| Aobi | 2 | 1 | 3 | 3 | 2 | 2 | 2 | 2 | 2 | 3 * | 3 | 2 * | 3 | 2 * |
| General Perceptions | |
|---|---|
| Themes | Supporting Statements |
| Expectancies facilitated perceptions |
|
| |
| |
| Told PLA treatments had minimal effect |
|
| |
| |
| Dynamic reaction time (DRT) | |
| Expectancies > told PLA treatments |
|
| |
| |
| |
| |
| LSPT and TLIM | |
| Synergism > all other Treatments |
|
| |
| |
| LIST | |
| Debilitative psychology |
|
| |
| |
| |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabir, A.; Hooton, A.; Spencer, G.; Storey, M.; Ensor, O.; Sandford, L.; Tallis, J.; Saunders, B.; Higgins, M.F. The Influence of Caffeine Expectancies on Simulated Soccer Performance in Recreational Individuals. Nutrients 2019, 11, 2289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102289
Shabir A, Hooton A, Spencer G, Storey M, Ensor O, Sandford L, Tallis J, Saunders B, Higgins MF. The Influence of Caffeine Expectancies on Simulated Soccer Performance in Recreational Individuals. Nutrients. 2019; 11(10):2289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102289
Chicago/Turabian StyleShabir, Akbar, Andy Hooton, George Spencer, Mitch Storey, Olivia Ensor, Laura Sandford, Jason Tallis, Bryan Saunders, and Matthew F. Higgins. 2019. "The Influence of Caffeine Expectancies on Simulated Soccer Performance in Recreational Individuals" Nutrients 11, no. 10: 2289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102289