No Association between Glucocorticoid Diurnal Rhythm in Breastmilk and Infant Body Composition at 3 Months

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Data Collection
2.2.1. Peripartum
2.2.2. One Month Postpartum
2.2.3. Three Months Postpartum
2.3. Laboratory Analysis
2.4. Statistics
- The maximum GC concentration, as a proxy for peak concentrations;
- The delta between maximum and minimum GC concentrations, as a measure of rhythm variability; and
- Area under the curve (AUC) ground (g) and increase (i), using the trapezoid rule [17].Calculations were corrected for total sampling time, since this differed between mothers. AUCg is a measure of total GC exposure, while AUCi provides information on GC variability.
3. Results
3.1. Population
3.2. Linear Regression Analyses
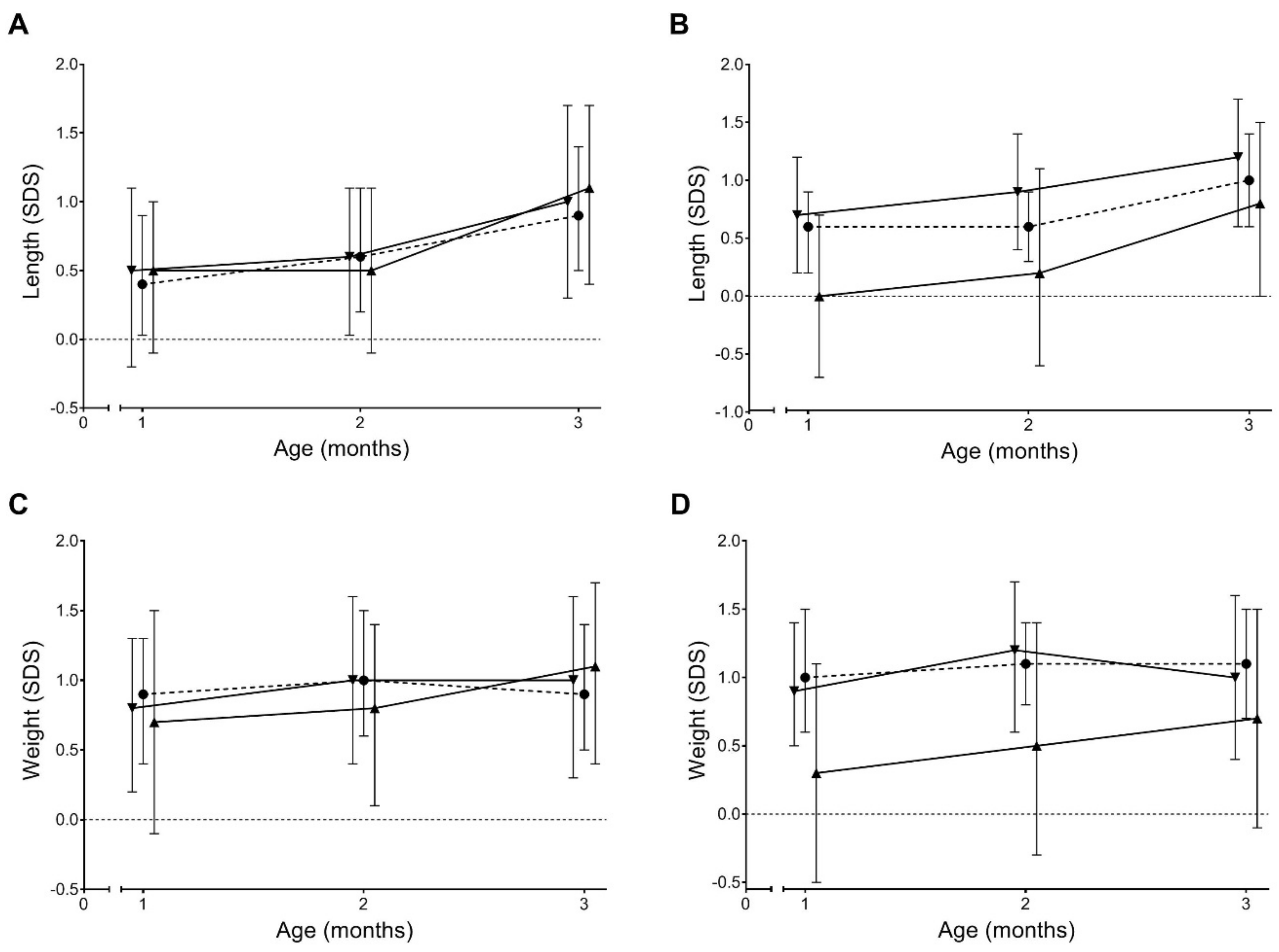
3.3. Growth Trajectories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barker, D.J.; Osmond, C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet 1986, 1, 1077–1081. [Google Scholar] [CrossRef]
- Finken, M.J.; van der Voorn, B.; Heijboer, A.C.; de Waard, M.; van Goudoever, J.B.; Rotteveel, J. Glucocorticoid Programming in Very Preterm Birth. Horm. Res. Paediatr. 2016, 85, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Rosmond, R.; Bjorntorp, P. The hypothalamic-pituitary-adrenal axis activity as a predictor of cardiovascular disease, type 2 diabetes and stroke. J. Intern. Med. 2000, 247, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Drake, A.J.; Tang, J.I.; Nyirenda, M.J. Mechanisms underlying the role of glucocorticoids in the early life programming of adult disease. Clin. Sci. 2007, 113, 219–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Entringer, S. Impact of stress and stress physiology during pregnancy on child metabolic function and obesity risk. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Angelucci, L.; Patacchioli, F.R.; Scaccianoce, S.; Di Sciullo, A.; Cardillo, A.; Maccari, S. A model for later-life effects of perinatal drug exposure: Maternal hormone mediation. Neurobehav. Toxicol. Teratol. 1985, 7, 511–517. [Google Scholar]
- Hinde, K.; Skibiel, A.L.; Foster, A.B.; Rosso, L.D.; Mendoza, S.P.; Capitanio, J.P. Cortisol in mother’s milk across lactation reflects maternal life history and predicts infant temperament. Behav. Ecol. 2015, 26, 269–281. [Google Scholar] [CrossRef]
- Hahn-Holbrook, J.; Le, T.B.; Chung, A.; Davis, E.P.; Glynn, L.M. Cortisol in human milk predicts child BMI. Obesity (Silver Spring) 2016, 24, 2471–2474. [Google Scholar] [CrossRef] [Green Version]
- Van der Voorn, B.; de Waard, M.; van Goudoever, J.B.; Rotteveel, J.; Heijboer, A.C.; Finken, M.J. Breast-Milk Cortisol and Cortisone Concentrations Follow the Diurnal Rhythm of Maternal Hypothalamus-Pituitary-Adrenal Axis Activity. J. Nutr. 2016, 146, 2174–2179. [Google Scholar] [CrossRef] [Green Version]
- Adam, E.K.; Quinn, M.E.; Tavernier, R.; McQuillan, M.T.; Dahlke, K.A.; Gilbert, K.E. Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 83, 25–41. [Google Scholar] [CrossRef]
- Ruttle, P.L.; Javaras, K.N.; Klein, M.H.; Armstrong, J.M.; Burk, L.R.; Essex, M.J. Concurrent and longitudinal associations between diurnal cortisol and body mass index across adolescence. J. Adolesc. Health 2013, 52, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Wirix, A.J.; Finken, M.J.; von Rosenstiel-Jadoul, I.A.; Heijboer, A.C.; Nauta, J.; Groothoff, J.W.; Chinapaw, M.J.; Kist-van Holthe, J.E. Is There an Association Between Cortisol and Hypertension in Overweight or Obese Children? J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Patacchioli, F.; Cigliana, G. Maternal plasma and milk free cortisol during the first 3 days of breast-feeding following spontaneous delivery or elective cesarean section. Gynecolog. Obstet. Invest. 1992, 34, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Voorn, B.; Martens, F.; Peppelman, N.S.; Rotteveel, J.; Blankenstein, M.A.; Finken, M.J.; Heijboer, A.C. Determination of cortisol and cortisone in human mother’s milk. Clin. Chim. Acta 2015, 444, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Kyle, U.G.; Schutz, Y.; Dupertuis, Y.M.; Pichard, C. Body composition interpretation. Contributions of the fat-free mass index and the body fat mass index. Nutrition 2003, 19, 597–604. [Google Scholar] [CrossRef]
- TNO. De Vijfde Landelijke Groeistudie; TNO: Hague, The Netherlands, 2010. [Google Scholar]
- Schonbeck, Y.; Talma, H.; van Dommelen, P.; Bakker, B.; Buitendijk, S.E.; HiraSing, R.A.; van Buuren, S. The world’s tallest nation has stopped growing taller: The height of Dutch children from 1955 to 2009. Pediatr. Res. 2013, 73, 371–377. [Google Scholar] [CrossRef]
- Figueiras, A.; Domenech-Massons, J.M.; Cadarso, C. Regression models: Calculating the confidence interval of effects in the presence of interactions. Stat. Med. 1998, 17, 2099–2105. [Google Scholar] [CrossRef]
- De Weerth, C.; Zijl, R.H.; Buitelaar, J.K. Development of cortisol circadian rhythm in infancy. Early Hum. Dev. 2003, 73, 39–52. [Google Scholar] [CrossRef]
- Ackermans, M.T.; Endert, E. LC-MS/MS in endocrinology: What is the profit of the last 5 years? Bioanalysis 2014, 6, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Koontz, M.B.; Gunzler, D.D.; Presley, L.; Catalano, P.M. Longitudinal changes in infant body composition: Association with childhood obesity. Pediatr. Obes. 2014, 9, e141–e144. [Google Scholar] [CrossRef]
- Blair, J.; Adaway, J.; Keevil, B.; Ross, R. Salivary cortisol and cortisone in the clinical setting. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Savas, M.; Wester, V.L.; de Rijke, Y.B.; Rubinstein, G.; Zopp, S.; Dorst, K.; van den Berg, S.A.A.; Beuschlein, F.; Feelders, R.A.; Reincke, M.; et al. Hair glucocorticoids as biomarker for endogenous Cushing’s syndrome: Validation in two independent cohorts. Neuroendocrinology 2019, 109, 171–178. [Google Scholar] [CrossRef]
- Smith, R.E.; Maguire, J.A.; Stein-Oakley, A.N.; Sasano, H.; Takahashi, K.; Fukushima, K.; Krozowski, Z.S. Localization of 11 beta-hydroxysteroid dehydrogenase type II in human epithelial tissues. J. Clin. Endocrinol. Metab. 1996, 81, 3244–3248. [Google Scholar] [CrossRef]
- Macfarlane, A.J.; Blondel, B.; Mohangoo, A.D.; Cuttini, M.; Nijhuis, J.; Novak, Z.; Olafsdottir, H.S.; Zeitlin, J.; Euro-Peristat Scientific Committee. Wide differences in mode of delivery within Europe: Risk-stratified analyses of aggregated routine data from the Euro-Peristat study. BJOG 2016, 123, 559–568. [Google Scholar] [CrossRef]


{kind=link}
| Unit | Mean ± SD or n (%) | |
|---|---|---|
| Gestational Age | Weeks | 39.9 ± 1.3 |
| Birth weight | grams | 3561 ± 498 |
| SDS | 0.2 ± 1.0 | |
| Birth length * | cm | 52.0 ± 2.6 |
| SDS | 1.0 ± 1.6 | |
| Male sex | 25 (59.5) | |
| Primiparity | 23 (54.8) | |
| Caesarian section | 21 (51.2) | |
| HAS and/or HDS ≥ 8 at 1-month pp | 6 (14.6) | |
| Pre-pregnancy maternal BMI | kg/m2 | 22.3 ± 2.8 |
| Weight gain during pregnancy | kg | 13.1 ± 3.2 |
| Maternal age | years | 36.0 ± 4.7 |
| Non-Caucasian ethnicity | 8 (20.0) | |
| Socioeconomic status | SDS | 0.6 ± 1.2 |
| >80% breastfed at 3 months of age | 35 (87.5) | |
| Age at breastmilk sampling | days | 30.8 ± 2.6 |
| Age at Pea Pod measurement ** | days | 90.5 ± 7.0 |
| Length | Weight | BMI | FMI | FFMI | Fat % | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | ||
| Cortisol | Maximum | 0.006 | (−0.04 to 0.05) | 0.022 | (−0.02 to 0.07) | 0.022 | (−0.02 to 0.06) | 0.003 | (−0.04 to 0.05) | −0.006 | (−0.04 to 0.03) | 0.048 | (−0.17 to 0.27) |
| Delta | 0.006 | (−0.04 to 0.05) | 0.024 | (−0.02 to 0.07) | 0.025 | (−0.02 to 0.07) | 0.003 | (−0.04 to 0.05) | −0.004 | (−0.04 to 0.03) | 0.043 | (−0.18 to 0.26) | |
| AUCi | 0.025 | (−0.15 to 0.20 | 0.101 | (−0.07 to 0.28) | 0.1 | (−0.06 to 0.26) | 0.06 | (−0.10 to 0.23) | −0.095 | (−0.23 to 0.04) | 0.53 | (−0.34 to 1.39) | |
| AUCg | 0.029 | (−0.13 to 0.19) | 0.06 | (−0.11 to 0.23) | 0.046 | (−0.11 to 0.20) | 0.06 | (−0.10 to 0.22) | −0.107 | (−0.24 to 0.02) | 0.53 | (−0.28 to 1.33) | |
| Cortison | Maximum | −0.002 | (−0.04 to 0.03) | 0.01 | (−0.03 to 0.05) | 0.014 | (−0.02 to 0.05) | –0.006 | (−0.04 to 0.03) | –0.006 | (−0.04 to 0.02) | –0.007 | (−0.19 to 0.18) |
| Delta | −0.002 | (−0.04 to 0.04) | 0.018 | (−0.02 to 0.06) | 0.024 | (−0.01 to 0.06) | –0.003 | (−0.04 to 0.03) | –0.001 | (−0.03 to 0.03) | 0.005 | (−0.19 to 0.20) | |
| AUCi | −0.005 | (−0.09 to 0.08) | 0.042 | (−0.05 to 0.13) | 0.055 | (−0.02 to 0.14) | 0.002 | (−0.08 to 0.09) | –0.008 | (−0.08 to 0.06) | 0.034 | (−0.41 to 0.48) | |
| AUCg | −0.001 | (−0.07 to 0.07) | 0.003 | (−0.07 to 0.07) | 0.004 | (−0.06 to 0.07) | –0.013 | (−0.08 to 0.05) | –0.02 | (−0.08 to 0.04) | –0.02 | (−0.37 to 0.33) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollanders, J.; Dijkstra, L.R.; van der Voorn, B.; Kouwenhoven, S.M.P.; Toorop, A.A.; van Goudoever, J.B.; Rotteveel, J.; Finken, M.J.J. No Association between Glucocorticoid Diurnal Rhythm in Breastmilk and Infant Body Composition at 3 Months. Nutrients 2019, 11, 2351. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102351
Hollanders J, Dijkstra LR, van der Voorn B, Kouwenhoven SMP, Toorop AA, van Goudoever JB, Rotteveel J, Finken MJJ. No Association between Glucocorticoid Diurnal Rhythm in Breastmilk and Infant Body Composition at 3 Months. Nutrients. 2019; 11(10):2351. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102351
Chicago/Turabian StyleHollanders, Jonneke, Lisette R. Dijkstra, Bibian van der Voorn, Stefanie M.P. Kouwenhoven, Alyssa A. Toorop, Johannes B. van Goudoever, Joost Rotteveel, and Martijn J.J. Finken. 2019. "No Association between Glucocorticoid Diurnal Rhythm in Breastmilk and Infant Body Composition at 3 Months" Nutrients 11, no. 10: 2351. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102351