Prevalence and Associated Factors of Caesarean Section and its Impact on Early Initiation of Breastfeeding in Abu Dhabi, United Arab Emirates


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Study Instrument
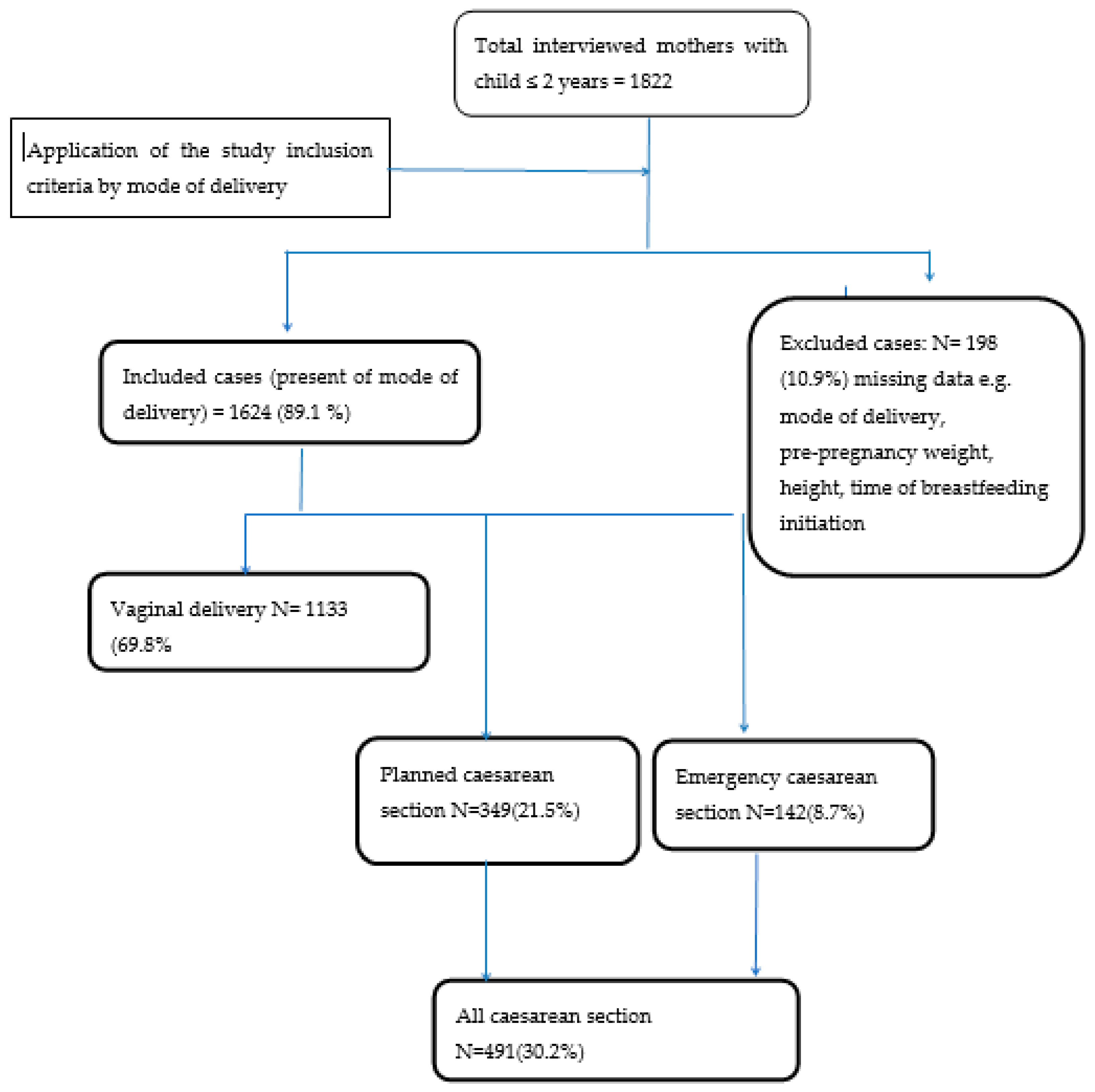
2.3. Study Inclusion and Exclusion Criteria
2.4. Statistical Analysis
2.5. Ethics
2.6. Definitions
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The World Health Report 2005 Statistical Annex; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. World health Statistics 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. WHO Statement on Caesarean Section Rates; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Smith, L.J. Impact of birthing practices on the breastfeeding dyad. J. Midwifery Womens Health 2007, 52, 621–630. [Google Scholar] [CrossRef]
- Procianoy, R.S.; Fernandes-Filho, P.H.; Lazaro, L.; Sartori, N.C. Factors affecting breastfeeding: The influence of caesarean section. J. Trop. Pediatr. 1984, 30, 39–42. [Google Scholar] [CrossRef]
- Jaafar, S.H.; Ho, J.J.; Lee, K.S. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst. Rev. 2016, Cd006641. [Google Scholar] [CrossRef]
- Bodner, K.; Wierrani, F.; Grunberger, W.; Bodner-Adler, B. Influence of the mode of delivery on maternal and neonatal outcomes: A comparison between elective cesarean section and planned vaginal delivery in a low-risk obstetric population. Arch. Gynecol. Obstet. 2011, 283, 1193–1198. [Google Scholar] [CrossRef]
- Wax, J.R. Maternal request cesarean versus planned spontaneous vaginal delivery: Maternal morbidity and short term outcomes. Semin. Perinatol. 2006, 30, 247–252. [Google Scholar] [CrossRef]
- Karlstrom, A.; Lindgren, H.; Hildingsson, I. Maternal and infant outcome after caesarean section without recorded medical indication: Findings from a Swedish case-control study. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 479–486; discussion 486. [Google Scholar] [CrossRef]
- Rowe-Murray, H.J.; Fisher, J.R. Baby friendly hospital practices: Cesarean section is a persistent barrier to early initiation of breastfeeding. Birth 2002, 29, 124–131. [Google Scholar] [CrossRef]
- Watt, S.; Sword, W.; Sheehan, D.; Foster, G.; Thabane, L.; Krueger, P.; Landy, C.K. The effect of delivery method on breastfeeding initiation from the The Ontario Mother and Infant Study (TOMIS) III. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, 728–737. [Google Scholar] [CrossRef]
- Esteves, T.M.; Daumas, R.P.; Oliveira, M.I.; Andrade, C.A.; Leite, I.C. Factors associated to breastfeeding in the first hour of life: Systematic review. Rev. Saude Publica 2014, 48, 697–708. [Google Scholar] [CrossRef]
- Meedya, S.; Fahy, K.; Kable, A. Factors that positively influence breastfeeding duration to 6 months: A literature review. Women Birth 2010, 23, 135–145. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization and United Nations Children’s Fund (UNICEF). Baby-Friendly Hospital Initiative Revised, Updated and Expanded for Integrated Care; World Health Organization and United Nations Children’s Fund: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003; pp. 1–30. [Google Scholar]
- Moore, E.R.; Bergman, N.; Anderson, G.C.; Medley, N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst. Rev. 2016, 11, Cd003519. [Google Scholar] [CrossRef]
- Patel, R.R.; Liebling, R.E.; Murphy, D.J. Effect of operative delivery in the second stage of labor on breastfeeding success. Birth 2003, 30, 255–260. [Google Scholar] [CrossRef]
- Zanardo, V.; Pigozzo, A.; Wainer, G.; Marchesoni, D.; Gasparoni, A.; Di Fabio, S.; Cavallin, F.; Giustardi, A.; Trevisanuto, D. Early lactation failure and formula adoption after elective caesarean delivery: Cohort study. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F37–F41. [Google Scholar] [CrossRef]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess. 2007, 153, 1–186. [Google Scholar]
- Yan, J.; Liu, L.; Zhu, Y.; Huang, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef]
- Victora, C.G.; Horta, B.L.; Loret de Mola, C.; Quevedo, L.; Pinheiro, R.T.; Gigante, D.P.; Goncalves, H.; Barros, F.C. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: A prospective birth cohort study from Brazil. Lancet Glob. Health 2015, 3, e199–e205. [Google Scholar] [CrossRef]
- Taha, Z. Trends of breastfeeding in the United Arab Emirates (UAE). Arab. J. Nutr. Exerc. 2017, 2, 152–159. [Google Scholar] [CrossRef]
- Taha, Z.; Garemo, M.; Nanda, J. Patterns of breastfeeding practices among infants and young children in Abu Dhabi, United Arab Emirates. Int Breastfeed. J. 2018, 13, 48. [Google Scholar] [CrossRef]
- Perez-Rios, N.; Ramos-Valencia, G.; Ortiz, A.P. Cesarean delivery as a barrier for breastfeeding initiation: The Puerto Rican experience. J. Hum. Lact. 2008, 24, 293–302. [Google Scholar] [CrossRef]
- Prior, E.; Santhakumaran, S.; Gale, C.; Philipps, L.H.; Modi, N.; Hyde, M.J. Breastfeeding after cesarean delivery: A systematic review and meta-analysis of world literature. Am. J. Clin. Nutr. 2012, 95, 1113–1135. [Google Scholar] [CrossRef]
- Perez-Escamilla, R.; Maulen-Radovan, I.; Dewey, K.G. The association between cesarean delivery and breast-feeding outcomes among Mexican women. Am. J. Public Health 1996, 86, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Jordan, S. Impact of birth complications on breastfeeding duration: An internet survey. J. Adv. Nurs. 2013, 69, 828–839. [Google Scholar] [CrossRef] [PubMed]
- Albokhary, A.A.; James, J.P. Does cesarean section have an impact on the successful initiation of breastfeeding in Saudi Arabia? Saudi. Med. J. 2014, 35, 1400–1403. [Google Scholar] [PubMed]
- Badaya, N.; Jain, S.; Kumar, N. Time of initiation of breastfeeding in various modes of delivery and to observe the effect of low birth weight and period of gestation on initiation of breastfeeding. Int. J. Contemp. Pediatr. 2018, 5, 1509–1517. [Google Scholar] [CrossRef] [Green Version]
- Regan, J.; Thompson, A.; DeFranco, E. The influence of mode of delivery on breastfeeding initiation in women with a prior cesarean delivery: A population-based study. Breastfeed. Med. 2013, 8, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kiani, S.N.; Rich, K.M.; Herkert, D.; Safon, C.; Perez-Escamilla, R. Delivery mode and breastfeeding outcomes among new mothers in Nicaragua. Matern. Child. Nutr. 2018, 14, e12474. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.A.; Taha, Z.; Ahmed, M.A.A.; Ali, A.A.A.; Adam, I. Assessment of initiation of breastfeeding practice in Kassala, Eastern Sudan: A community-based study. Int. Breastfeed. J. 2018, 13, 34. [Google Scholar] [CrossRef]
- Rabiepoor, S.; Sadeghi, E.; Hamidiazar, P. The relationship between type of delivery and successful breastfeeding. Int. J. Paediatr. 2017, 5, 4899–4907. [Google Scholar]
- Palla, H.; Kitsantas, P. Mode of delivery and breastfeeding practices. Int. J. Pregnancy Child Birth 2017, 2, 167–172. [Google Scholar]
- Grajeda, R.; Perez-Escamilla, R. Stress during labor and delivery is associated with delayed onset of lactation among urban Guatemalan women. J. Nutr. 2002, 132, 3055–3060. [Google Scholar] [CrossRef]
- Abu Dhabi Government. Abu Dhabi Emirate: Facts and Figures; Abu Dhabi Government: Abu Dhabi, UAE, 2018.
- World Health Organization. Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Ghadeer, Z.; Abdullah, A.; Afnan, B.; Abdullah, A.; Abrar, H.; Hanoof, A.; Aeshah, A.; Fatimah, A.; Duaa, F.; Amair, A. Prevalence of caesarean section and its indicating factors among pregnant women attending delivery at King Abdulaziz University Hospital, Jeddah city during 2016. EC Gynaecol. 2018, 7, 43–51. [Google Scholar]
- Elmugabil, A.; Rayis, D.A.; Hassan, A.A.; Ali, A.A.A.; Adam, I. Epidemiology of cesarean delivery in Kassala, Eastern Sudan: A community-based study 2014–2015. Sudan JMS 2016, 11, 49–54. [Google Scholar]
- Khan, M.N.; Islam, M.M.; Shariff, A.A.; Alam, M.M.; Rahman, M.M. Socio-demographic predictors and average annual rates of caesarean section in Bangladesh between 2004 and 2014. PLoS ONE 2017, 12, e0177579. [Google Scholar] [CrossRef] [PubMed]
- Barros, F.C.; Rabello Neto, D.L.; Villar, J.; Kennedy, S.H.; Silveira, M.F.; Diaz-Rossello, J.L.; Victora, C.G. Caesarean sections and the prevalence of preterm and early-term births in Brazil: Secondary analyses of national birth registration. BMJ Open 2018, 8, e021538. [Google Scholar] [CrossRef]
- Boatin, A.A.; Schlotheuber, A.; Betran, A.P.; Moller, A.B.; Barros, A.J.D.; Boerma, T.; Torloni, M.R.; Victora, C.G.; Hosseinpoor, A.R. Within country inequalities in caesarean section rates: Observational study of 72 low and middle income countries. BMJ 2018, 360, k55. [Google Scholar] [CrossRef]
- Al Rifai, R. Rising cesarean deliveries among apparently low-risk mothers at university teaching hospitals in Jordan: Analysis of population survey data, 2002–2012. Glob. Health Sci. Pract. 2014, 2, 195–209. [Google Scholar] [CrossRef]
- Einarsdottir, K.; Haggar, F.; Pereira, G.; Leonard, H.; de Klerk, N.; Stanley, F.J.; Stock, S. Role of public and private funding in the rising caesarean section rate: A cohort study. BMJ Open 2013, 3, e002789. [Google Scholar] [CrossRef]
- Delnord, M.; Blondel, B.; Drewniak, N.; Klungsoyr, K.; Bolumar, F.; Mohangoo, A.; Gissler, M.; Szamotulska, K.; Lack, N.; Nijhuis, J.; et al. Varying gestational age patterns in cesarean delivery: An international comparison. BMC Pregnancy Childbirth 2014, 14, 321. [Google Scholar] [CrossRef]
- Cavazos-Rehg, P.A.; Krauss, M.J.; Spitznagel, E.L.; Bommarito, K.; Madden, T.; Olsen, M.A.; Subramaniam, H.; Peipert, J.F.; Bierut, L.J. Maternal age and risk of labor and delivery complications. Matern. Child. Health J. 2015, 19, 1202–1211. [Google Scholar] [CrossRef]
- Fuchs, F.; Monet, B.; Ducruet, T.; Chaillet, N.; Audibert, F. Effect of maternal age on the risk of preterm birth: A large cohort study. PLoS ONE 2018, 13, e0191002. [Google Scholar] [CrossRef]
- Waldenstrom, U.; Cnattingius, S.; Vixner, L.; Norman, M. Advanced maternal age increases the risk of very preterm birth, irrespective of parity: A population-based register study. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Apanga, P.A.; Awoonor-Williams, J.K. Predictors of caesarean section in northern Ghana: A case-control study. Pan Afr. Med. J. 2018, 29, 20. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, J.A.; Campbell, O.M.; De Silva, M.J.; Slaymaker, E.; Filippi, V. Maternal obesity and Caesarean delivery in sub-Saharan Africa. Trop. Med. Int. Health 2016, 21, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Ovesen, P.; Rasmussen, S.; Kesmodel, U. Effect of prepregnancy maternal overweight and obesity on pregnancy outcome. Obstet. Gynecol. 2011, 118, 305–312. [Google Scholar] [CrossRef]
- Tsvieli, O.; Sergienko, R.; Sheiner, E. Risk factors and perinatal outcome of pregnancies complicated with cephalopelvic disproportion: A population-based study. Arch. Gynecol. Obstet. 2012, 285, 931–936. [Google Scholar] [CrossRef]
- Donath, S.M.; Amir, L.H. Maternal obesity and initiation and duration of breastfeeding: Data from the longitudinal study of Australian children. Matern. Child. Nutr. 2008, 4, 163–170. [Google Scholar] [CrossRef]
- Ramji, N.; Quinlan, J.; Murphy, P.; Crane, J.M. The impact of maternal obesity on breastfeeding. J. Obstet. Gynaecol. Can. 2016, 38, 703–711. [Google Scholar] [CrossRef]
- Verret-Chalifour, J.; Giguere, Y.; Forest, J.-C.; Croteau, J.; Zhang, P.; Marc, I. Breastfeeding initiation: Impact of obesity in a large Canadian perinatal cohort study. PLoS ONE 2015, 10, e0117512. [Google Scholar] [CrossRef]
- Isik, Y.; Dag, Z.O.; Tulmac, O.B.; Pek, E. Early postpartum lactation effects of cesarean and vaginal birth. Ginekol. Pol. 2016, 87, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Yan, Y.; Gao, X.; Xiang, S.; He, Q.; Zeng, G.; Liu, S.; Sha, T.; Li, L. Influences of Cesarean Delivery on Breastfeeding Practices and Duration: A Prospective Cohort Study. J. Hum. Lact. 2018, 34, 526–534. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mode of Delivery | ||||||
|---|---|---|---|---|---|---|---|
| Total (n = 1624) | Vaginal (n = 1133) | CS (n = 491) | |||||
| Mean (SD), range | Mean (SD) | Mean (SD) | p-Value | ||||
| Maternal age, years | 30.1(5.2) | 29.9(5.3) | 31.0(4.8) | <0.001 | |||
| Child age, months (median 6, interquartile range 9) | 8.1(5.9) | 8.3(6.0) | 7.6(5.7) | 0.042 | |||
| Gestational age, weeks | 39.1(1.9) | 39.4(1.7) | 38.6(2.1) | <0.001 | |||
| Birth weight, grams | 3079(518) | 3110(463) | 3008(621) | <0.001 | |||
| Mother pre-pregnancy BMI | 23.9(3.8), (15.2, 64.9) | 23.7(3.7) | 24.3(4.2) | 0.002 | |||
| N | % | N | % | N | % | ||
| Child Gender | |||||||
| Male Female | 799 | 49.2 | 560 | 49.4 | 239 | 48.7 | 0.781 |
| 825 | 50.8 | 573 | 50.6 | 252 | 51.3 | ||
| Nationality by category | |||||||
| Arab Non-Arab | 1056 | 65.0 | 757 | 66.7 | 299 | 60.9 | 0.049 |
| 568 | 35.0 | 376 | 33.3 | 192 | 39.1 | ||
| Marital status | |||||||
| Married Unmarried | 1602 | 98.6 | 1116 | 98.5 | 486 | 99.0 | 0.440 |
| 22 | 1.4 | 17 | 1.5 | 5 | 1.0 | ||
| Initiation of breastfeeding | |||||||
| Delayed initiated Early initiated | 609 | 37.5 | 329 | 29.0 | 280 | 57.0 | < 0.001 |
| 1015 | 62.5 | 804 | 71.0 | 211 | 43.0 | ||
| Rooming-in | |||||||
| Yes No | 1562 | 96.2 | 1101 | 97.2 | 461 | 93.9 | 0.002 |
| 62 | 3.8 | 32 | 2.8 | 30 | 6.1 | ||
| Mother’s education | |||||||
| <Secondary level ≥secondary level | 65 | 4.0 | 53 | 4.7 | 12 | 2.4 | 0.035 |
| 1559 | 96.0 | 1080 | 95.3 | 479 | 97.6 | ||
| Father’s education | |||||||
| <Secondary level ≥secondary level | 31 | 1.9 | 23 | 2.0 | 8 | 1.6 | 0.588 |
| 1593 | 98.1 | 1110 | 98.0 | 483 | 98.4 | ||
| Mother occupation | |||||||
| Housewives Employed | 1008 | 62.1 | 695 | 61.3 | 313 | 63.7 | 0.533 |
| 616 | 37.9 | 438 | 38.7 | 178 | 36.3 | ||
| Child order | |||||||
| 1st order >1st order | 1038 | 63.9 | 399 | 35.2 | 187 | 38.1 | 0.269 |
| 1038 | 63.9 | 304 | 61.9 | 304 | 61.9 | ||
| Variable | Adjusted Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|
| Advanced maternal age, years | 1.04 | 1.02, 1.07 | < 0.001 | |
| Gestational age, weeks | 0.80 | 0.75, 0.86 | <0.001 | |
| Child’s birth weight, grams | 1.00 | 1.00, 1.00 | 0.283 | |
| Nationality | Non-Arab | 1.36 | 1.08, 1.71 | 0.009 |
| Arab | Reference | |||
| Maternal education | ≥Secondary | 1.88 | 0.94, 3.75 | 0.072 |
| <Secondary | Reference | |||
| Mother pre-pregnancy BMI | Underweight (<18.5) | 1.12 | 0.56, 2.26 | 0.746 |
| Normal (18.5–24.9) | Reference | |||
| Overweight (25–29.9) | 1.10 | 0.85, 1.42 | 0.477 | |
| Obese (≥30) | 1.79 | 1.15, 2.79 | 0.010 | |
| Mode of Delivery | 95% Confidence Interval (CI) | p-Value | AOR 1 (95% CI) | p-Value | AOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Vaginal delivery | 4.5 (3.16, 6.61) | < 0.001 | 2.78 (2.17, 3.56) | < 0.001 | Reference | |
| Planned CS | 1.64 (1.09, 2.46) | 0.017 | Reference | 0.36 (0.28, 046) | < 0.001 | |
| Emergency CS | Reference | 0.61 (0.41, 0.91) | 0.017 | 0.22 (0.15, 0.32) | < 0.001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taha, Z.; Ali Hassan, A.; Wikkeling-Scott, L.; Papandreou, D. Prevalence and Associated Factors of Caesarean Section and its Impact on Early Initiation of Breastfeeding in Abu Dhabi, United Arab Emirates. Nutrients 2019, 11, 2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112723
Taha Z, Ali Hassan A, Wikkeling-Scott L, Papandreou D. Prevalence and Associated Factors of Caesarean Section and its Impact on Early Initiation of Breastfeeding in Abu Dhabi, United Arab Emirates. Nutrients. 2019; 11(11):2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112723
Chicago/Turabian StyleTaha, Zainab, Ahmed Ali Hassan, Ludmilla Wikkeling-Scott, and Dimitrios Papandreou. 2019. "Prevalence and Associated Factors of Caesarean Section and its Impact on Early Initiation of Breastfeeding in Abu Dhabi, United Arab Emirates" Nutrients 11, no. 11: 2723. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112723