1. Introduction
Excess sodium intake is related to high blood pressure, cardiovascular disease and stroke in the general population [
1,
2]. In patients on chronic hemodialysis, excess sodium intake is also associated to thirst and consequently to high interdialytic weight gain (IDWG). High IDWG is associated with higher risk of all-cause and cardiovascular death and increased morbidity, such as ventricular hypertrophy and major adverse cardiac and cerebrovascular events [
3,
4,
5,
6,
7,
8,
9]. In addition, it leads to supplementary weekly dialysis sessions with consequent deterioration of quality of life and increased costs [
10].
The American Heart Association recommends a daily sodium intake <1500 mg [
11]. The average daily sodium intake among dialysis patients has been reported to be significantly higher [
12,
13,
14,
15,
16,
17,
18]. Sodium intake of patients on chronic hemodialysis varies according to the country, being higher especially where the diet is rich in processed foods [
12,
13,
14,
15,
16,
17].
Nephrologists routinely recommend restriction of salt, but unfortunately it is difficult to obtain in daily clinical practice. Adherence to a low-salt diet of hemodialysis patients is poor [
18] as well as in patients with other chronic diseases such as heart failure, hypertension, and cirrhosis [
19,
20,
21,
22,
23,
24,
25,
26,
27]. Many factors contribute to such poor adherence such as lack of knowledge, interference with socialization, low education level, low socioeconomic status, and lack of food selections [
10]. It must also be considered that hemodialysis patients are continuously instructed to follow a restricted diet because of potassium and phosphorus concerns, and such further restrictions may lead to a diet poorly acceptable in terms of palatability and pleasantness.
Recently, it has been suggested that that sodium restriction may be beneficial as long as optimal nutritional status and food intake are not compromised [
28]. Indeed, malnutrition and the risk of protein-energy wasting may occur following a sodium-restricted diet because sodium is widely used in the foods [
28]. It has also been suggested that the efforts to intensify sodium restriction might increase the risk of compromising energy intake further [
17].
The present study aims to compare the intake of nutrients, minerals, trace elements, and vitamins in patients who had a daily sodium intake below or above the value of 1500 mg recommended by the American Heart Association.
3. Results
One-hundred-and-twenty-seven patients were included in the study. Their demographic, clinical and laboratory characteristics as well as the causes of ESRD are shown in
Table 1.
The mean sodium intake (mg) was 1295.9 ± 812.3. The mean sodium intake per body weight was 20.1 ± 14 mg/kg. Eighty seven (68.5%) patients had a daily sodium intake <1500 mg (group 1) and 40 (31.5%) ≥ 1500 mg (group 2).
The mean sodium intake was similar in dialysis and non-dialysis days. The correlation between sodium intake and age was negative and statistically significant (
r = −0.203 [−0.365–0.029];
p < 0.0001). The mean age of patients of group 1 and 2 did not differ significantly (
Table 2).
The daily sodium intake was significantly higher in patients <40 years (2324 ± 1666) than in patients of 40–60 years (1319 ± 475) or older (1220 ± 787) (p = 0.005). However, the difference between the latter two groups was not statistically significant.
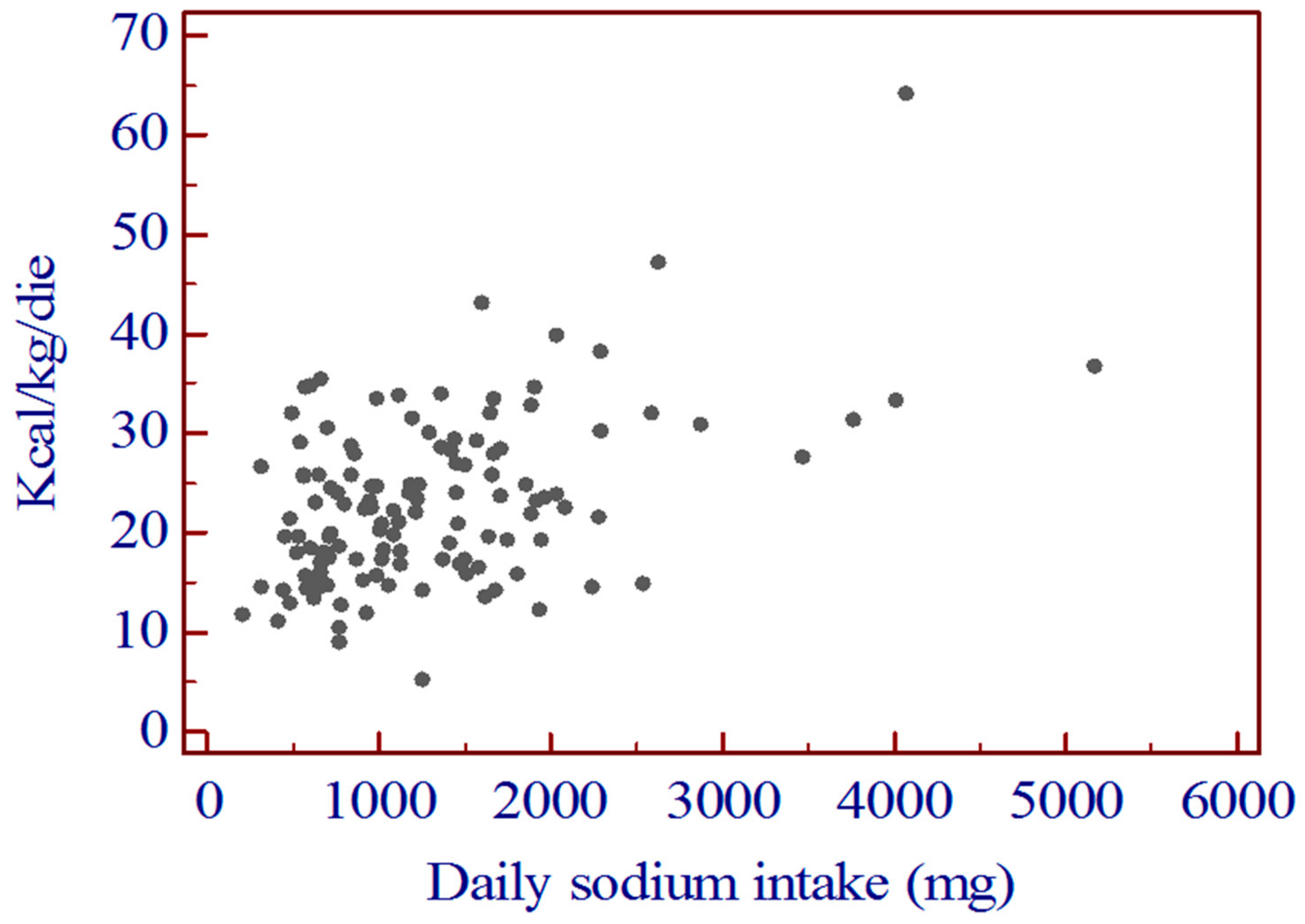
The correlation between daily sodium intake and daily calorie intake was highly significant (
Figure 1).
The daily calorie intake was significantly lower in group 1 than in group 2 (
p = 0.0001). (
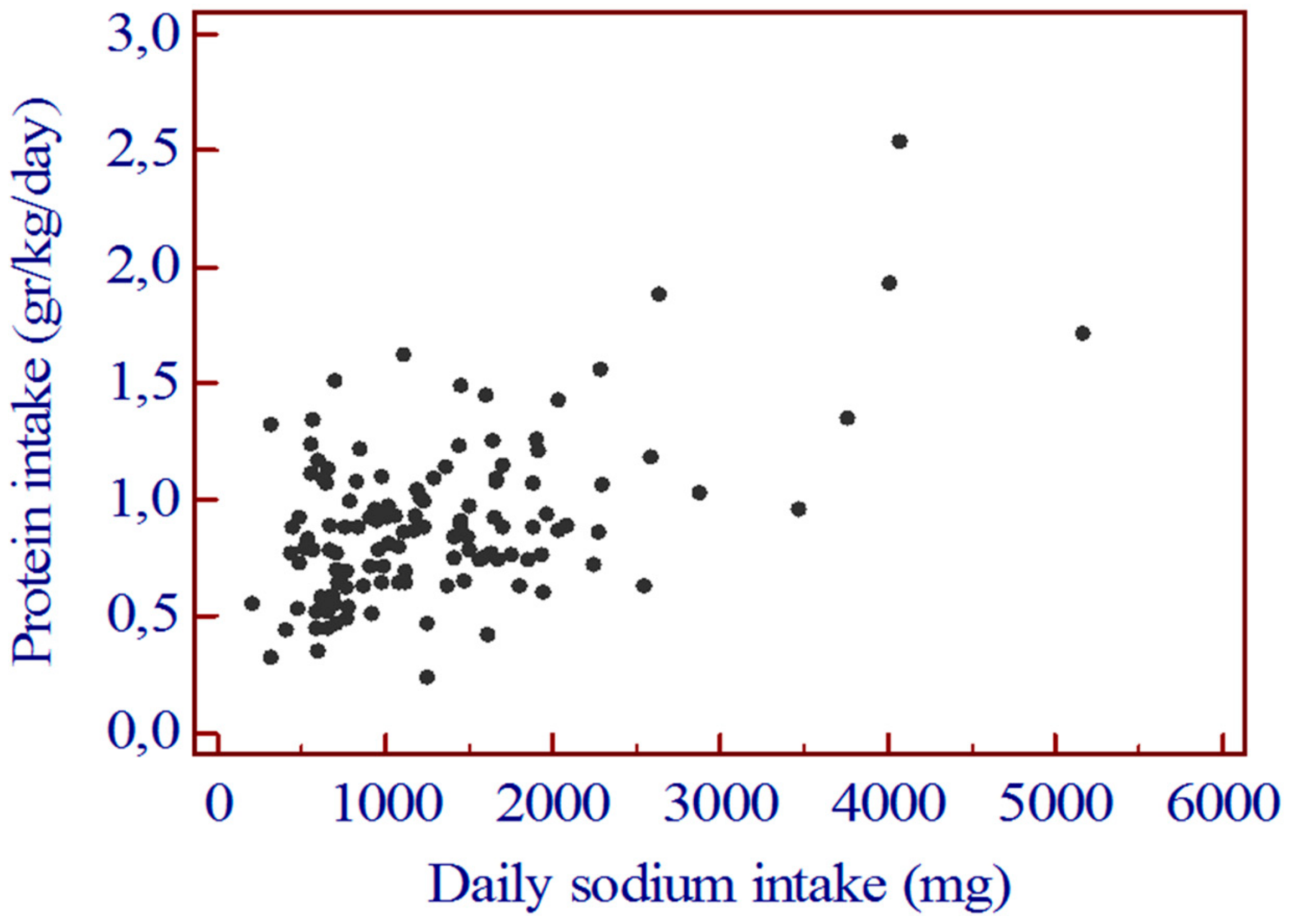
Table 2). Similarly, the correlation between daily sodium intake and daily protein intake was highly significant (
Figure 2).
The daily protein intake was significantly lower in group 1 than in group 2 (
p = 0.0003) (
Table 2).
The correlation between daily sodium intake and daily carbohydrate intake was highly significant (
r = 0.415 [0.260–0.549]:
p < 0.0001). The daily carbohydrate intake was significantly lower in group 1 than in group 2 (
Table 2). The correlation between daily sodium intake and daily lipid intake was highly significant (
r = 0.421 [0.267–0.555];
p < 0.0001). The daily lipid intake was significantly lower in group 1 than in group 2 (
Table 2).
The correlation between daily sodium intake and daily phosphate intake was highly significant (
Figure 3). The daily intake of phosphate was significantly higher in group 2 than in group 1 (
Table 2). The correlation between daily sodium intake and daily potassium intake was highly significant. The daily intake of potassium was significantly higher in group 2 than in group 1 (
Table 2).
The correlations between daily sodium intake and daily intake of magnesium, copper, iron, zinc, and selenium were significant (data not shown). The daily intake of magnesium, copper, iron, zinc, and selenium was significantly lower in group 1 than in group 2 (
Table 3).
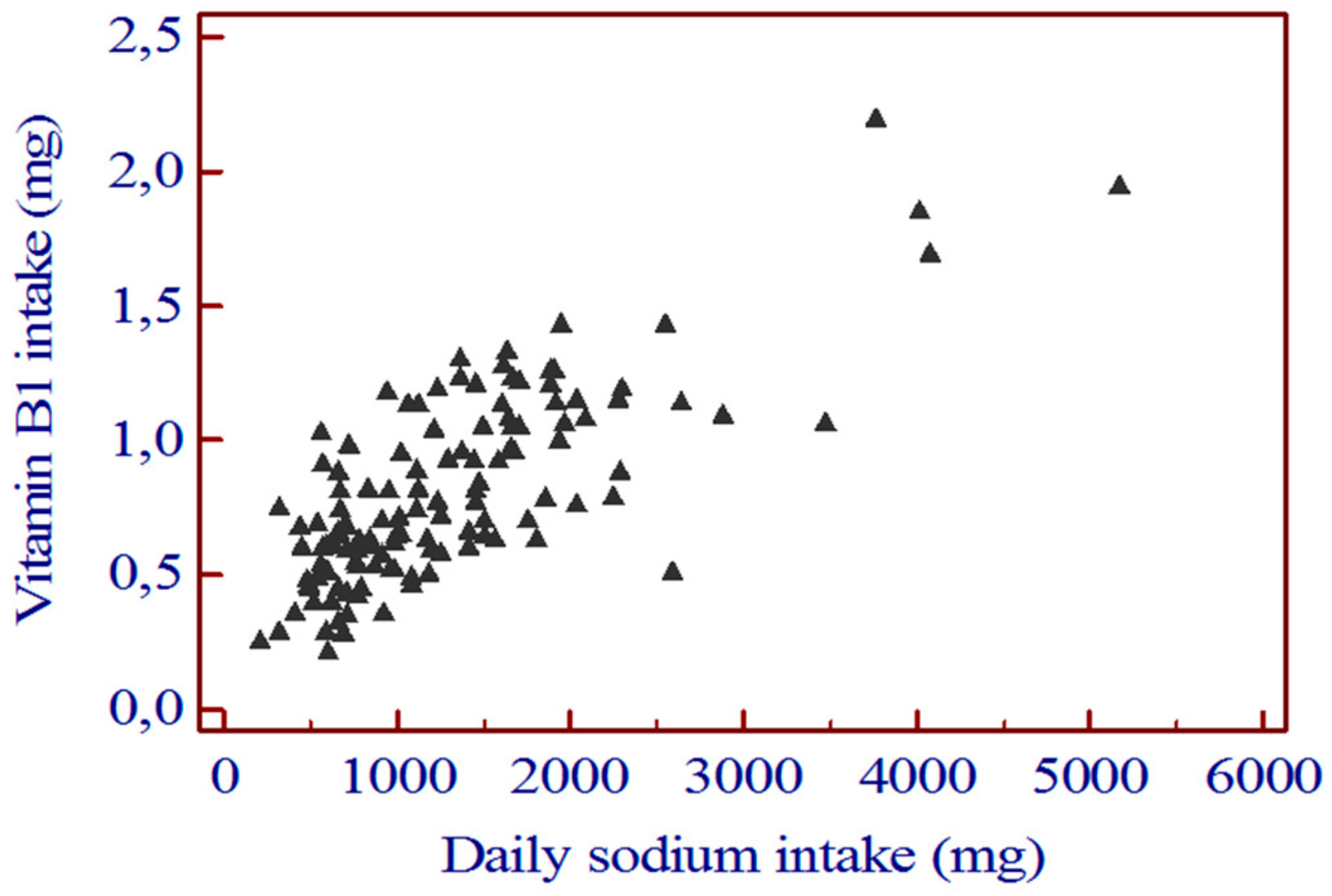
The daily intake of vitamin A, B2, B3, and C did not differ significantly between group 1 and group 2. The correlation between daily sodium intake and daily vitamin B1 intake was highly significant (
r = 0.763 [0.679 to 0.827];
p < 0.0001) (
Figure 3).
The daily intake of vitamin B1 was significantly lower in group 1 than in group 2 (
Table 4).
We then compared patients of group 1 and group 2 in terms of percentage of patients within the recommended value of nutrients intakes. The percentage of patients with intakes of calories and proteins (
Table 5) target value were significantly lower in group 1 than in group 2.
Similarly, the percentage of patients with intakes of iron and zinc (
Table 6) and vitamin B1 (
Table 7) within the target value were significantly lower in group 1 than in group 2. Conversely, the percentage of patients with adequate potassium intake was significantly higher in group 1 than in group 2 (
Table 5).
4. Discussion
More than two thirds of patients included in the present study had a sodium intake <1500 mg/day, and thus were within the value recommended by the American Heart Association [
11]. It is possible that these good results are a consequence of the habit of the patients of our country to consume fresh foods and avoid, as much as possible, the use of fast and/or processed foods. The average daily salt intake among dialysis patients has been reported to be high, ranging from 7.9 to 14.1 g/day [
12,
13,
14,
15,
16,
17]. Recently, Luis et al., that referred to the recommendations of 2000–2300 mg/day of the European Best Practice Guideline on Nutrition and Chronic Kidney Disease, found that only 15% of patients were within the target value [
29]. Similarly, in the study of Xie et al., more than half of the patients exceeded the recommended sodium intake of 1840–2300 mg/day of the New Zealand Dietitians Guidelines [
17].
In patients on chronic hemodialysis, a diet with a low sodium intake is associated with an improvement of xerostomia, a better control of blood pressure and with a lower interdialytic weight gain [
35,
36], as well as with a reduction of the risk of all-cause and cardiovascular death and morbidity, such as ventricular hypertrophy and major adverse cardiac and cerebrovascular events [
3,
4,
5,
6,
7,
8,
9].
However, the present study also shows that patients with a daily sodium intake lower than 1500 mg, with respect to those with an intake ≥1500 mg, had a significantly greater risk to have an inadequate calorie and protein intake as well as of a low intake of iron and zinc. This in accordance with the study of Xie et al. who appropriately suggested that the efforts to intensify sodium restriction might increase the risk of compromising energy intake further [
17]. Inadequate low calorie and protein intakes put the patients at risk of protein energy wasting and to its consequences. However, the results of the present study do not mean that patients should increase their calorie and protein intakes while disregarding the daily sodium intake. Instead, our study suggests that much attention should be paid to the nutritional education of patients on chronic hemodialysis with the aim to stimulate them to increase their food intake and, at the same time, limit as much as possible the daily sodium consumption. Undoubtedly, this is not an easy task. Adherence to a low-salt diet of hemodialysis patients is poor [
18,
19] as well as in patients with other chronic diseases [
20,
21,
22,
23,
24,
25,
26,
27,
28], even though a high percentage of patients on hemodialysis recognize that salty food is not good for them [
18,
37,
38]. Sevick et al. showed that nutritional counseling and a technology-supported behavioral intervention resulted in reduced dietary sodium intake at 8 weeks, however, it was not sustained at 16 weeks [
39]. Conversely, 48-month nutritional counseling resulted in a significant decrease of salt and water intake (from 13.3 ± 2.7 to 11.8 ± 2.4 g/day and 2528 ± 455 to 2332 ± 410 mL/day, respectively) [
39]. In addition, it is usually difficult to combine an adequate calorie and protein intake with a low sodium intake. Interestingly, in all the studies cited above the intake of macronutrients and micronutrients was never reported. Nevertheless, in the randomized, controlled study by Rodrigues-Telini, sodium intake was reduced by 2 g/day for 16 weeks without a reduction in total caloric or protein intake as a consequence of adequate nutritional counselling [
39].
The lower percentage of patients within the recommended value of iron and zinc intake, observed in the group with a sodium intake <1500 mg, requires attention also. Iron is essential for erythropoiesis, and zinc deficiency is associated with delayed wound healing, immune deficiency, dysgeusia, decreased cognitive function, anorexia, and increased risk of infection [
32,
40]. Attention should be paid to stimulate the patients to consume food rich in zinc (such as bread, cereals, leguminous plant seeds and mushrooms, red meat) and in iron (red meat, chicken, turkey, pork, ham, veal, fish, raw, and cooked spinach).
The percentage of patients within the target value of vitamins intake was low both in patients with daily sodium intake <1500 mg and in those with an intake ≥1500. However, the difference between the two groups was highly significant with regard to vitamin B1 intake, with only 8% and 50% of patients with a sodium intake <1500 or ≥1500 mg within the target value, respectively. Low vitamin B1 intake can lead to low serum levels and associated complications as Wernicke’s encephalopathy [
41,
42].
Overall, the correlation between sodium intake and age was significant and the daily sodium intake was significantly higher in patients <40 years than in patients of 40–60 years or older, although the calorie intake was similar in the three groups. Similar observations have been reported by other authors [
19]. Conversely, in the study of Gkza et al., older patients consumed more sodium than the middle-age cohort and this was due, according to the authors, to the fact that many elderly patients that were no longer able to cook fresh food increasingly relied on ready and prepared meals that have higher sodium content and also because elderly patients residing in nursing or residential homes did not receive low-sodium meals [
16]. In the present study, all old patients lived at home and consumed food prepared by themselves or by relatives. Overall, the observation that younger patients consume more sodium may be useful in the clinical practice because it allows to identify a specific population at risk of high sodium intake that needs to be offered adequate nutritional counselling.
The present study has a limitation. We used a 3-day food diary to assess sodium intake, a method that may imply inherent errors of dietary assessment and can be the cause of under- and over-reporting. Nevertheless, there is large recent evidence that the 3-day diet diary is a simple, useful, and effective method to measure the intake of macro- and micro-nutrients in patients on chronic hemodialysis [
43,
44,
45,
46,
47]. The strength is that we included patients of different towns of Italy and consequently the data can be considered representative of the Italian population of patients on chronic hemodialysis.
In conclusion, the results of the present study suggests practically that low sodium intake is associated with a low intake of calorie, protein, iron, zinc, and vitamin B. This finding implies and strongly suggests that all nutritional counselling aimed at reducing the daily intake of sodium in patients on chronic hemodialysis should not disregard an adequate intake of macro- and micronutrients, otherwise the risk of protein and energy wasting as well as the deficit of some trace elements and vitamins may be high.

 ,
, 



{kind=link}
{kind=link}
{kind=link}