Angiotensin Converting Enzyme (ACE): A Marker for Personalized Feedback on Dieting

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
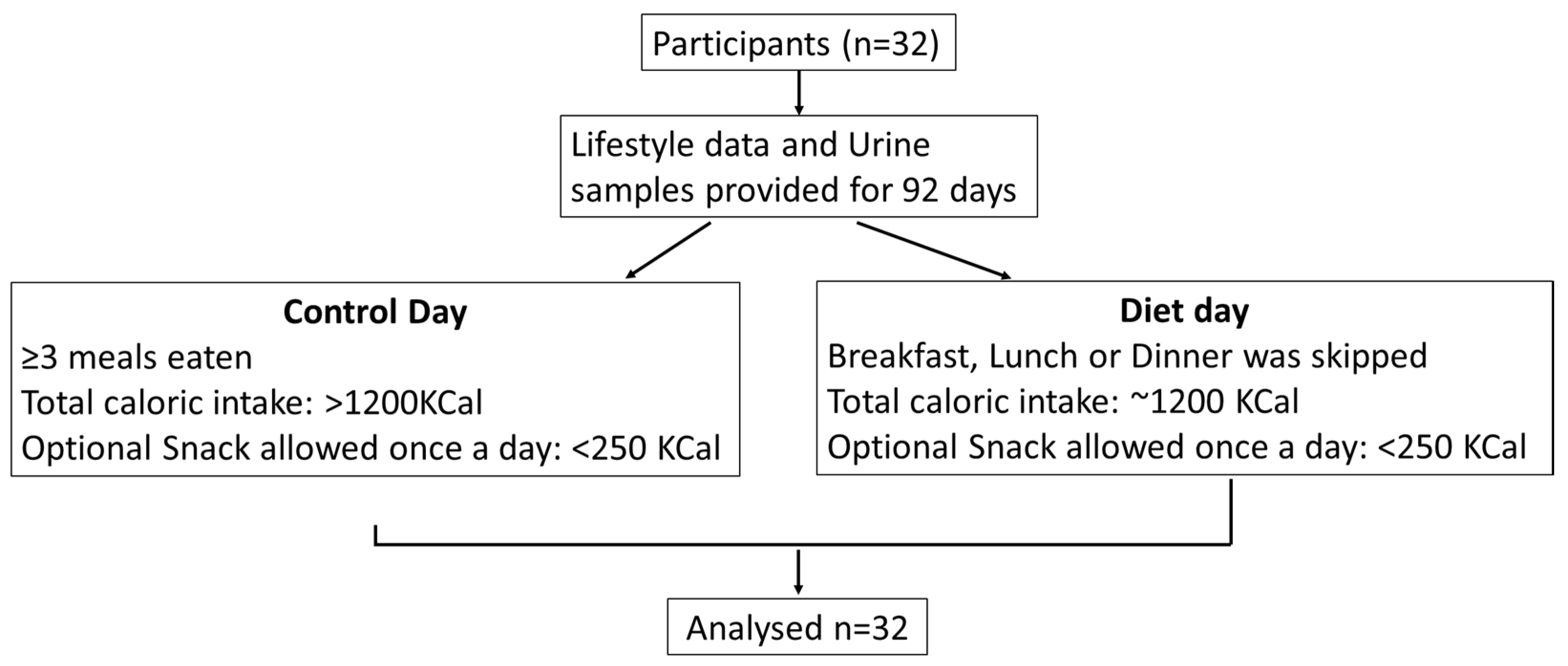
2.1. Study Design
2.2. Measurement of Angiotensin Converting Enzyme
2.3. Measurement of Insulin and Lactate
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
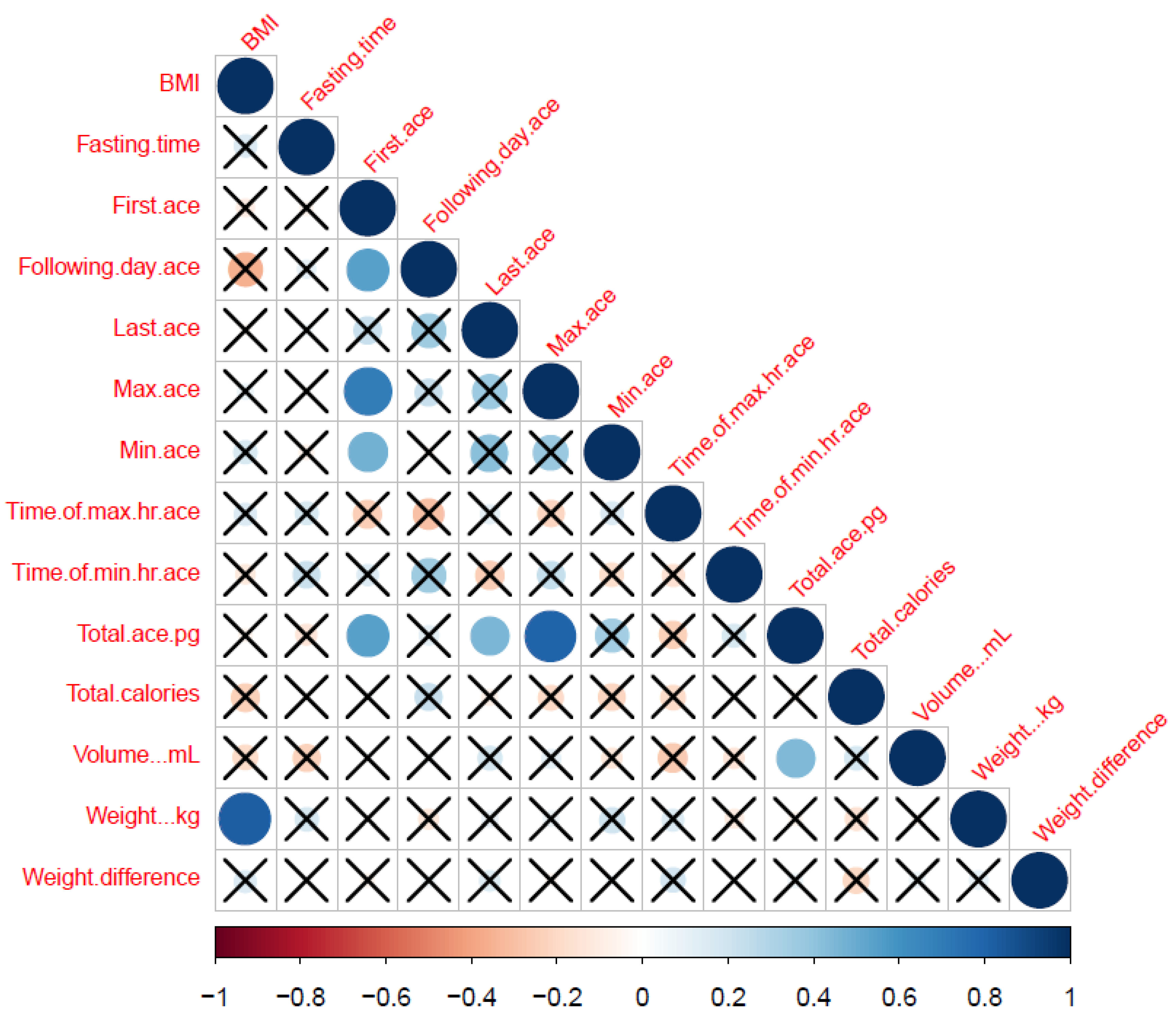
3.2. ACE Levels Correlate with Life-Style Data
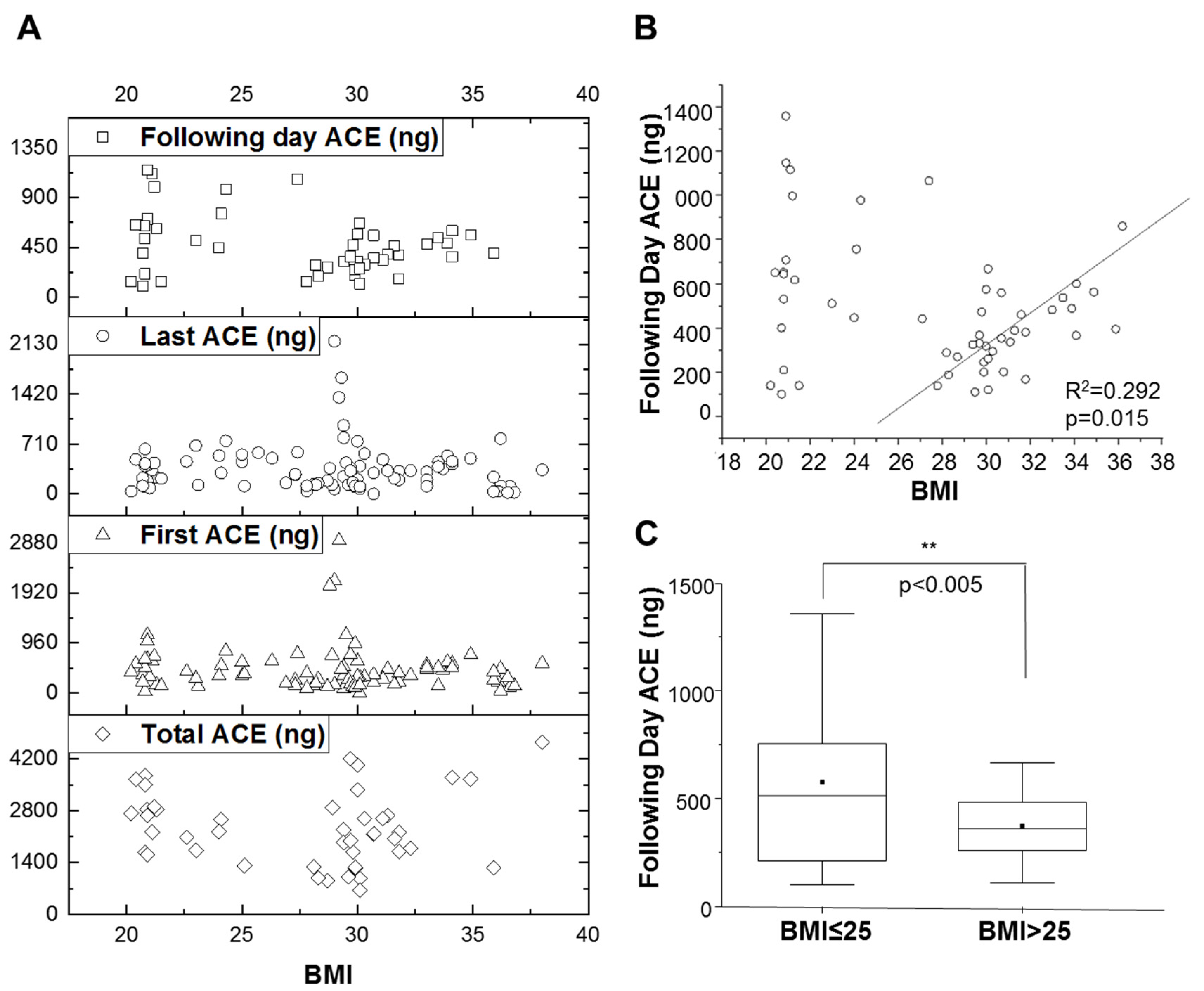
3.3. Effects of BMI on ACE Levels
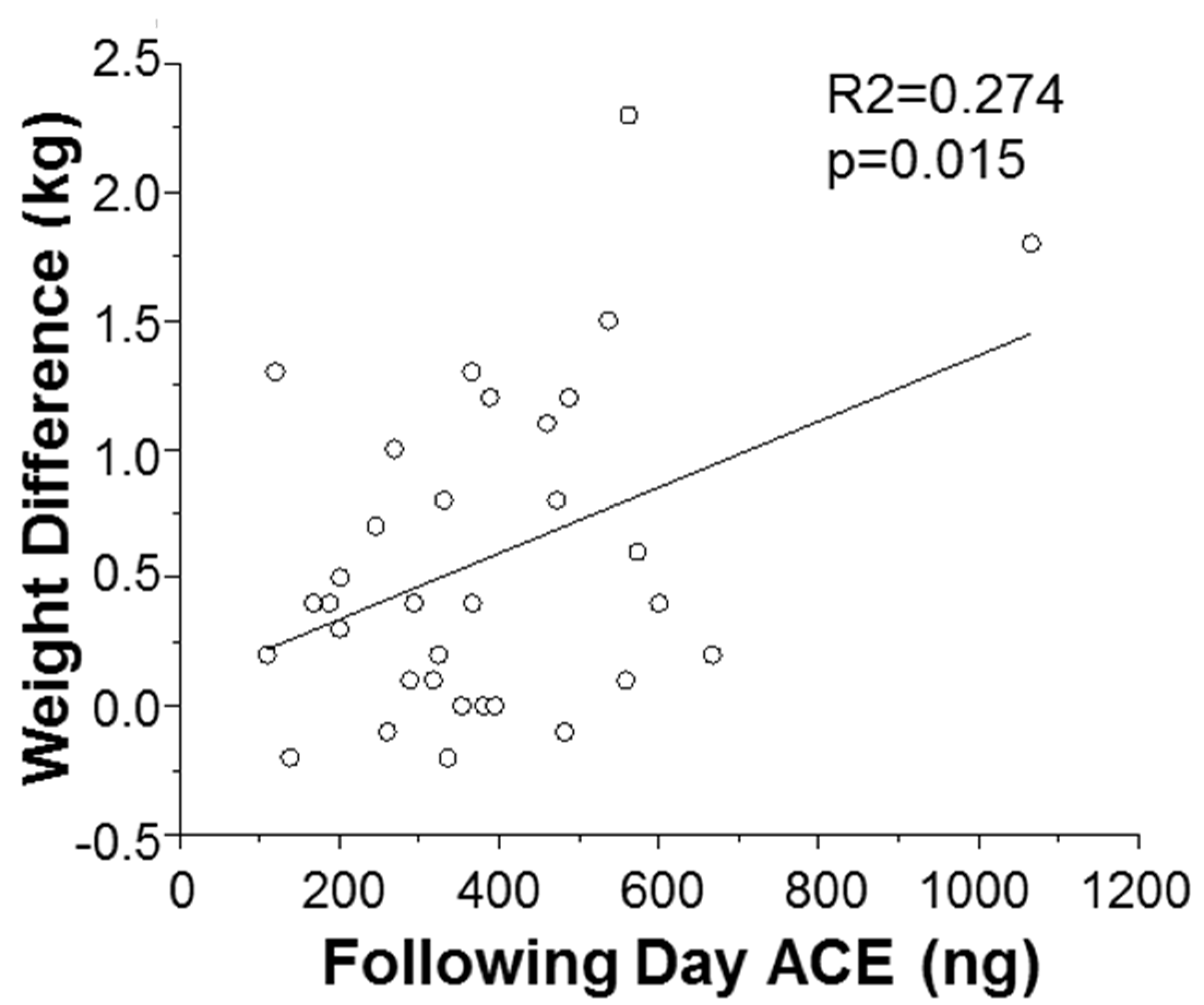
3.4. Dependence of Weight Loss on ACE Level
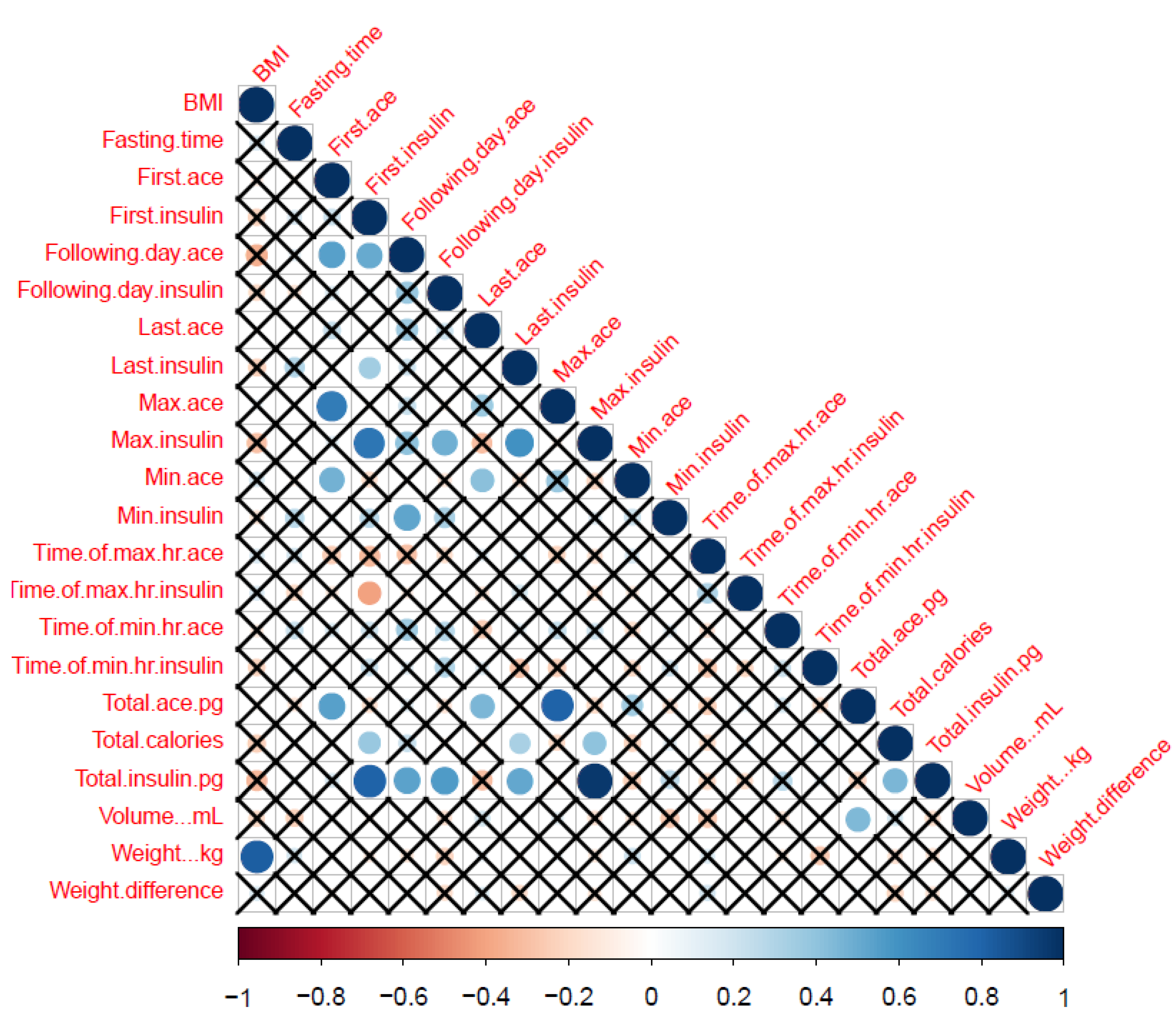
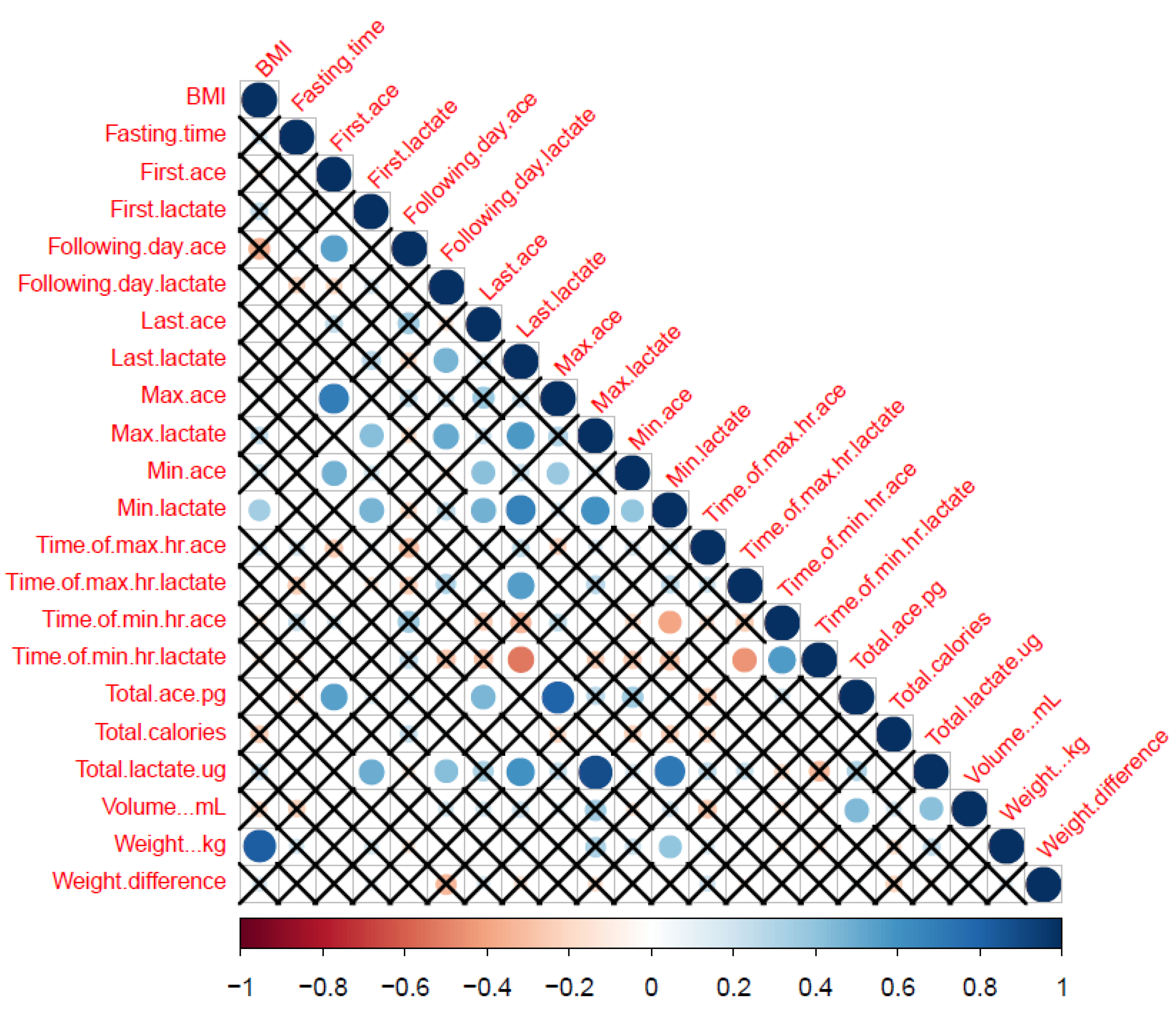
3.5. Correlation among ACE, Insulin and Lactate
4. Discussion
5. Conclusion
Author Contributions
Funding
Conflicts of Interest
References
- González-Muniesa, P.; Mártinez-González, M.-A.; Hu, F.B.; Després, J.-P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Primers 2017, 3, 17034. [Google Scholar] [CrossRef]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 19 November 2019).
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.W.; Shin, S.A.; Yun, Y.H.; Yoo, T.; Huh, B.Y. Cut-off Point of BMI and Obesity-Related Comorbidities and Mortality in Middle-Aged Koreans. Obes. Res. 2004, 12, 2031–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Spinos, T.; Spinou, Μ.; Brinia, Μ.-E.; Mitsopoulou, D.; Katsilambros, N. Defining the Optimal Dietary Approach for Safe, Effective and Sustainable Weight Loss in Overweight and Obese Adults. Healthcare 2018, 6, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.; Tate, D. Tweets, Apps, and Pods: Results of the 6-month Mobile Pounds Off Digitally (Mobile POD) randomized weight-loss intervention among adults. J. Med. Int. Res. 2011, 13, e120. [Google Scholar] [CrossRef]
- Franco, R.Z.; Fallaize, R.; Lovegrove, J.A.; Hwang, F. Popular Nutrition-Related Mobile Apps: A Feature Assessment. JMIR MHealth UHealth 2016, 4, e85. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in Diet and Lifestyle and Long-Term Weight Gain in Women and Men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [Green Version]
- Tejpal, S.; Sanghera, N.; Manoharan, V.; Planas-Iglesias, J.; Myler, K.; Klein-Seetharaman, J. Towards personalised molecular feedback for weight loss. BMC Obes. 2019, 6, 20. [Google Scholar] [CrossRef]
- Liu, B.; Young, H.; Crowe, F.L.; Benson, V.S.; Spencer, E.A.; Key, T.J.; Appleby, P.N.; Beral, V. Development and evaluation of the Oxford WebQ, a low-cost, web-based method for assessment of previous 24 h dietary intakes in large-scale prospective studies. Public Health Nutr. 2011, 14, 1998–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Johns, E.; Atallah, L.; Pettitt, C.; Lo, B.; Frost, G.; Yang, G.Z. An Intelligent Food-Intake Monitoring System Using Wearable Sensors. In Proceedings of the 2012 Ninth International Conference on Wearable and Implantable Body Sensor Networks, London, UK, 9–12 May 2012; pp. 154–160. [Google Scholar]
- Vereecken, C.A.; Covents, M.; Matthys, C.; Maes, L. Young adolescents’ nutrition assessment on computer (YANA-C). Eur. J. Clin. Nutr. 2005, 59, 658–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [Green Version]
- Scisco, J.L.; Muth, E.R.; Dong, Y.; Hoover, A.W. Slowing Bite-Rate Reduces Energy Intake: An Application of the Bite Counter Device. J. Am. Diet. Assoc. 2011, 111, 1231–1235. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Silva, M.N.; Mata, J.; Palmeira, A.L.; Markland, D. Motivation, self-determination, and long-term weight control. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Elobeid, M.A.; Padilla, M.A.; McVie, T.; Thomas, O.; Brock, D.W.; Musser, B.; Lu, K.; Coffey, C.S.; Desmond, R.A.; St-Onge, M.-P.; et al. Missing Data in Randomized Clinical Trials for Weight Loss: Scope of the Problem, State of the Field, and Performance of Statistical Methods. PLoS ONE 2009, 4, e6624. [Google Scholar] [CrossRef]
- Elliott, P.; Posma, J.M.; Chan, Q.; Garcia-Perez, I.; Wijeyesekera, A.; Bictash, M.; Ebbels, T.M.D.; Ueshima, H.; Zhao, L.C.; van Horn, L.; et al. Urinary metabolic signatures of human adiposity. Sci. Transl. Med. 2015, 7, 285ra62. [Google Scholar] [CrossRef] [Green Version]
- Molitor, J.; Brown, I.J.; Chan, Q.; Papathomas, M.; Liverani, S.; Molitor, N.; Richardson, S.; Van Horn, L.; Daviglus, M.L.; Dyer, A.; et al. Blood Pressure Differences Associated With Optimal Macronutrient Intake Trial for Heart Health (OMNIHEART)-Like Diet Compared With a Typical American Diet. Hypertension 2014, 64, 1198–1204. [Google Scholar] [CrossRef] [Green Version]
- Du, F.; Virtue, A.; Wang, H.; Yang, X.-F. Metabolomic analyses for atherosclerosis, diabetes, and obesity. Biomark. Res. 2013, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Holst, C.; Andersen, M.R.; Astrup, A.; Bouwman, F.G.; van Otterdijk, S.; Wkwh, W.; van Baak, M.A.; Larsen, T.M.; Jebb, S.A.; et al. Blood Profile of Proteins and Steroid Hormones Predicts Weight Change after Weight Loss with Interactions of Dietary Protein Level and Glycemic Index. PLoS ONE 2011, 6, e16773. [Google Scholar]
- Brewster, U.C.; Perazella, M.A. The renin-angiotensin-aldosterone system and the kidney: Effects on kidney disease. Am. J. Med. 2004, 116, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.-H.; Wang, M.; Huang, Y.-M.; Wang, Y.-H.; Chen, Y.-L.; Geng, L.-J.; Zhang, X.-X.; Zhao, H.-L. ACE Gene I/D Polymorphism and Obesity in 1,574 Patients with Type 2 Diabetes Mellitus. Dis. Markers 2016, 2016, 7420540. [Google Scholar] [CrossRef]
- Tejpal, S.; Bastie, C.; Seetharaman, J.K. Lemon Juice: A potential source of Angiotensin Converting Enzyme antagonism for weight loss and insulin resistance. Proc. Nutr. Soc. 2018, 77, E213. [Google Scholar] [CrossRef]
- Patel Vaibhav, B.; Parajuli, N.; Oudit Gavin, Y. Role of angiotensin-converting enzyme 2 (ACE2) in diabetic cardiovascular complications. Clin. Sci. 2014, 126, 471. [Google Scholar] [CrossRef]
- Tejpal, S.; Sanghera, N.; Manoharan, V.; Planas-Iglesias, J.; Klein-Seetharaman, J. A marker for personalised feedback on dieting: Angiotensin Converting Enzyme. Proc. Nutr. Soc. 2019, 78, E44. [Google Scholar] [CrossRef] [Green Version]
- Goossens, G.H.; Blaak, E.E.; Van Baak, M.A. Possible involvement of the adipose tissue renin-angiotensin system in the pathophysiology of obesity and obesity-related disorders. Obes. Rev. 2003, 4, 43–55. [Google Scholar] [CrossRef]
- Barton, M.; Carmona, R.; Morawietz, H.; d’Uscio Livius, V.; Goettsch, W.; Hillen, H.; Haudenschild Christian, C.; Krieger Jose, E.; Münter, K.; Lattmann, T.; et al. Obesity Is Associated With Tissue-Specific Activation of Renal Angiotensin-Converting Enzyme In Vivo. Hypertension 2000, 35, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Gunnarsdóttir, I.; Sigurgeirsdóttir, G.K.; Thórsdóttir, I. Predictors of Dropping Out in a Weight Loss Intervention Trial. Ann. Nutr. Metab. 2010, 56, 212–216. [Google Scholar] [CrossRef]
- Moroshko, I.; Brennan, L.; O’Brien, P. Predictors of dropout in weight loss interventions: A systematic review of the literature. Obes. Rev. 2011, 12, 912–934. [Google Scholar] [CrossRef]
- Colombo, O.; Ferretti, V.V.; Ferraris, C.; Trentani, C.; Vinai, P.; Villani, S.; Tagliabue, A. Is drop-out from obesity treatment a predictable and preventable event? Nutr. J. 2014, 13, 13. [Google Scholar] [CrossRef] [PubMed]
- Ortner Hadžiabdić, M.; Mucalo, I.; Hrabač, P.; Matić, T.; Rahelić, D.; Božikov, V. Factors predictive of drop-out and weight loss success in weight management of obese patients. J. Hum. Nutr. Diet. 2015, 28, 24–32. [Google Scholar] [CrossRef]
- Neve, M.J.; Collins, C.E.; Morgan, P.J. Dropout, Nonusage Attrition, and Pretreatment Predictors of Nonusage Attrition in a Commercial Web-Based Weight Loss Program. J. Med. Int. Res. 2010, 12, e69. [Google Scholar] [CrossRef] [PubMed]
- Sanghera, N.; Anderson, A.; Nuar, N.; Xie, C.; Mitchell, D.; Klein-Seetharaman, J. Insulin biosensor development: A case study. Int. J. ParallelEmergent Distrib. Syst. 2017, 32, 119–138. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Goyal, R.; Julka, S. Impact of breakfast skipping on the health status of the population. Indian J. Endocrinol. Metab. 2014, 18, 683–687. [Google Scholar]
- Rong, S.; Snetselaar, L.G.; Xu, G.; Sun, Y.; Liu, B.; Wallace, R.B.; Bao, W. Association of Skipping Breakfast With Cardiovascular and All-Cause Mortality. J. Am. Coll. Cardiol. 2019, 73, 2025–2032. [Google Scholar] [CrossRef]
- Purslow, L.R.; Sandhu, M.S.; Forouhi, N.; Young, E.H.; Luben, R.N.; Welch, A.A.; Khaw, K.-T.; Bingham, S.A.; Wareham, N.J. Energy Intake at Breakfast and Weight Change: Prospective Study of 6764 Middle-aged Men and Women. Am. J. Epidemiol. 2007, 167, 188–192. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; Ard, J.; Baskin Monica, L.; Chiuve Stephanie, E.; Johnson Heather, M.; Kris-Etherton, P.; Varady, K. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef]
- Mekary, R.A.; Giovannucci, E.; Cahill, L.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in older women: Breakfast consumption and eating frequency. Am. J. Clin. Nutr. 2013, 98, 436–443. [Google Scholar] [CrossRef]
- Rigat, B.; Hubert, C.; Alhenc-Gelas, F.; Cambien, F.; Corvol, P.; Soubrier, F. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J. Clin. Investig. 1990, 86, 1343–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rankinen, T.; Zuberi, A.; Chagnon, Y.C.; Weisnagel, S.J.; Argyropoulos, G.; Walts, B.; Pérusse, L.; Bouchard, C. The Human Obesity Gene Map: The 2005 Update. Obesity 2006, 14, 529–644. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, C.; Sjöholm, K.; Ottosson, M.; Sjöström, L.; Carlsson, B.M.S.; Carlsson, L. Human Adipose Tissue Expresses Angiotensinogen and Enzymes Required for Its Conversion to Angiotensin II 1. J. Clin. Endocrinol. Metab. 1998, 83, 3925–3929. [Google Scholar] [PubMed] [Green Version]
- Jones, B.H.; Standridge, M.K.; Moustaid, N. Angiotensin II Increases Lipogenesis in 3T3-L1 and Human Adipose Cells*. Endocrinology 1997, 138, 1512–1519. [Google Scholar] [CrossRef]
- Riera-Fortuny, C.; Real, J.T.; Chaves, F.J.; Morales-Suárez-Varela, M.; Martínez-Triguero, M.L.; Morillas-Ariño, C.; Hernández-Mijares, A. The relation between obesity, abdominal fat deposit and the angiotensin-converting enzyme gene I/D polymorphism and its association with coronary heart disease. Int. J. Obes. 2005, 29, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Engeli, S.; Gorzelniak, K.; Kreutz, R.; Runkel, N.; Distler, A.; Sharma, A.M. Co-expression of renin-angiotensin system genes in human adipose tissue. J. Hypertens. 1999, 17, 555–560. [Google Scholar] [CrossRef]
- Darimont, C.; Vassaux, G.; Ailhaud, G.; Negrel, R. Differentiation of preadipose cells: Paracrine role of prostacyclin upon stimulation of adipose cells by angiotensin-II. Endocrinology 1994, 135, 2030–2036. [Google Scholar] [CrossRef]
- Bakris, G.L.; Toto, R.D.; McCullough, P.A.; Rocha, R.; Purkayastha, D.; Davis, P. Effects of different ACE inhibitor combinations on albuminuria: Results of the GUARD study. Kidney Int. 2008, 73, 1303–1309. [Google Scholar] [CrossRef] [Green Version]
- Chapter 5. Treatment with antihypertensive drugs. Hypertens. Res. 2014, 37, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Cook, A.; Pryer, J.; Shetty, P. The problem of accuracy in dietary surveys. Analysis of the over 65 UK National Diet and Nutrition Survey. J. Epidemiol. Community Health 2000, 54, 611. [Google Scholar] [CrossRef]
- Banna, J.C.; Fialkowski, M.K.; Townsend, M.S. Misreporting of dietary intake affects estimated nutrient intakes in low-income Spanish-speaking women. J. Acad. Nutr. Diet. 2015, 115, 1124–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description |
|---|---|
| Extracted from Biomarker Profile | |
| Volume of urine in 24 hour (mL) | Total volume of urine produced over a 24-hour period |
| First ACE value on diet day | Obtained from urine sample just before the first meal of the day |
| Last ACE value on diet day | Obtained from the last urine sample of the diet day |
| Total ACE value of 24 hour | Summation of ACE values obtained from all the urine samples provided over a 24-hour period |
| Following day ACE | Obtained from the first urine sample at the end of the 24-hour period on the following day |
| Minimum ACE value in 24-hour | The smallest amount of ACE amongst all the urine samples provided over a 24-hour period |
| Maximum ACE value in 24-hour | The largest amount of ACE amongst all the urine samples provided over a 24-hour period |
| Time of maximum ACE in 24-hour | Time stamp of the urine sample entry in the DHP that corresponds to the maximum ACE value |
| Time of minimum ACE in 24-hour | Time stamp of the urine sample entry in the DHP that corresponds to the minimum ACE value |
| Variable from Digital Health Platform (DHP) entries | |
| Fasting time | Obtained by subtracting the time of the second meal from the first meal of the day |
| Total calories | Obtained from summation of the caloric information of the food entries on DHP over a 24-hour period |
| Weight | Entered by the participant (measured every day in the morning) |
| Weight difference | Weight before breakfast minus weight following morning at the same time |
| BMI | Either entered by the participant or calculated based on the weight and height entry of the participant |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tejpal, S.; Sanghera, N.; Manoharan, V.; Planas-Iglesias, J.; Bastie, C.C.; Klein-Seetharaman, J. Angiotensin Converting Enzyme (ACE): A Marker for Personalized Feedback on Dieting. Nutrients 2020, 12, 660. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030660
Tejpal S, Sanghera N, Manoharan V, Planas-Iglesias J, Bastie CC, Klein-Seetharaman J. Angiotensin Converting Enzyme (ACE): A Marker for Personalized Feedback on Dieting. Nutrients. 2020; 12(3):660. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030660
Chicago/Turabian StyleTejpal, Shilpa, Narinder Sanghera, Vijayalaxmi Manoharan, Joan Planas-Iglesias, Claire C Bastie, and Judith Klein-Seetharaman. 2020. "Angiotensin Converting Enzyme (ACE): A Marker for Personalized Feedback on Dieting" Nutrients 12, no. 3: 660. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030660