Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Setting
2.3. Sample Size and Sampling
2.4. Data Collection
2.4.1. Dietary Intakes
2.4.2. Maternal Anthropometry
2.4.3. Red Blood Cell Indices
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Dietary Diversity
3.2. Socio-Demographic, Health and Anthropometry Characteristic
3.3. Habitual Dietary Patterns
3.4. Predictors for Meeting the Minimum Dietary Diversity Indicator
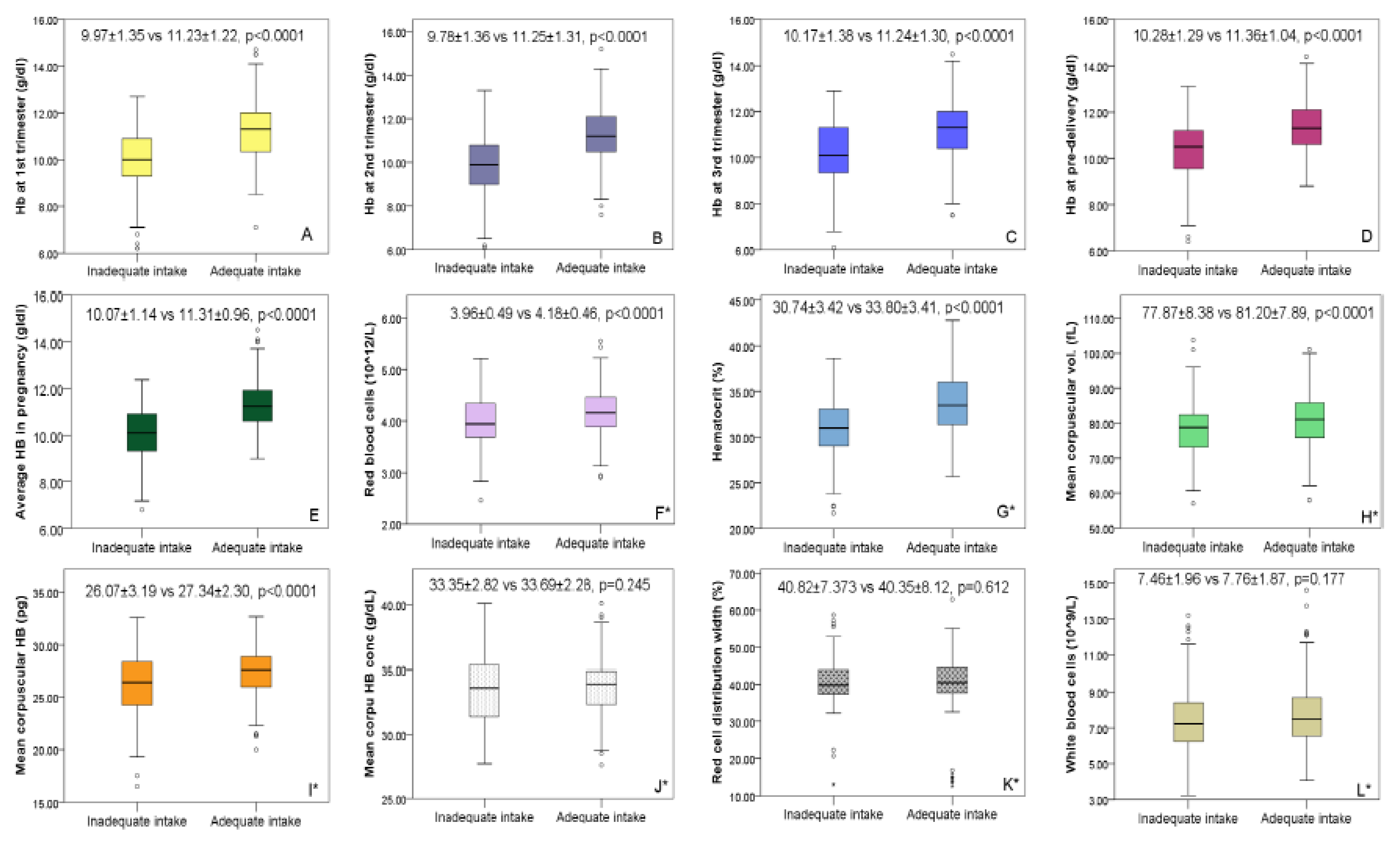
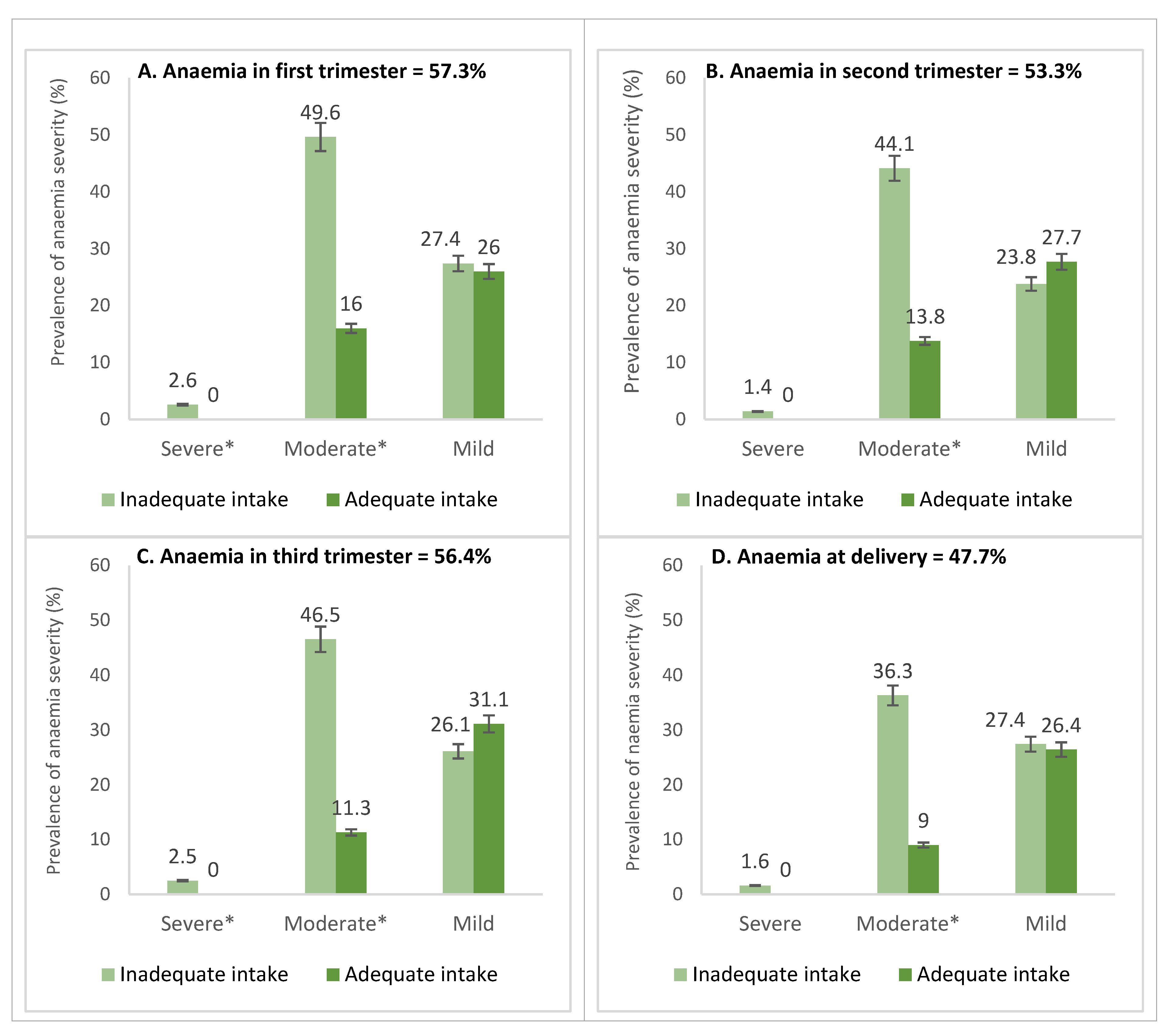
3.5. Anemia Levels by Hemoglobin, Red Blood Cell Morphology and Mean Red Blood Cell Indices
3.6. Risk Factors for Anemia in Pregnancy
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. The Global Prevalence of Anaemia in 2011; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Rahman, M.M.; Abe, S.K.; Rahman, M.S.; Kanda, M.; Narita, S.; Bilano, V.; Ota, E.; Gilmour, S.; Shibuya, K. Maternal anemia and risk of adverse birth and health outcomes in low-and middle-income countries: Systematic review and meta-analysis, 2. Am. J. Clin. Nutr. 2016, 103, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Scholl, T.O. Maternal iron status: Relation to fetal growth, length of gestation, and iron endowment of the neonate. Nutr. Rev. 2011, 69, S23–S29. [Google Scholar] [CrossRef] [Green Version]
- Menon, K.C.; Ferguson, E.L.; Thomson, C.D.; Gray, A.R.; Zodpey, S.; Saraf, A.; Das, P.K.; Skeaff, S.A. Effects of anemia at different stages of gestation on infant outcomes. Nutrition 2016, 32, 61–65. [Google Scholar] [CrossRef]
- Bora, R.; Sable, C.; Wolfson, J.; Boro, K.; Rao, R. Prevalence of anemia in pregnant women and its effect on neonatal outcomes in Northeast India. J. Matern. Fetal Neonatal Med. 2014, 27, 887–891. [Google Scholar] [CrossRef]
- Drukker, L.; Hants, Y.; Farkash, R.; Ruchlemer, R.; Samueloff, A.; Grisaru-Granovsky, S. Iron deficiency anemia at admission for labor and delivery is associated with an increased risk for Cesarean section and adverse maternal and neonatal outcomes. Transfusion 2015, 55, 2799–2806. [Google Scholar] [CrossRef]
- Ghana Statistical Service. Ghana Demographic and Health Survey 2008; Accra: Ghana Health Service Accra, Ghana and ICF Macro: Calverton, MD, USA, 2008.
- Ghana Statistical Service. Ghana Demographic and Health Survey 2014 Key Indicators; Accra: Ghana Health Service Accra, Ghana and The DHS Program, ICF International: Rockville, MD, USA, 2015.
- Ruel, M.T.; Alderman, H.; Maternal Group CNS. Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? Lancet 2013, 382, 536–551. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.E.; Talegawkar, S.A.; Merialdi, M.; Caulfield, L.E. Dietary intakes of women during pregnancy in low- and middle-income countries. Public Health Nutr. 2012, 16, 1340–1353. [Google Scholar] [CrossRef] [PubMed]
- Zerfu, T.A.; Umeta, M.; Baye, K. Dietary diversity during pregnancy is associated with reduced risk of maternal anemia, preterm delivery, and low birth weight in a prospective cohort study in rural Ethiopia. Am. J. Clin. Nutr. 2016, 103, 1482–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadesse, S.E.; Seid, O.; G/Mariam, Y.; Fekadu, A.; Wasihun, Y.; Endris, K.; Bitew, A. Determinants of anemia among pregnant mothers attending antenatal care in Dessie town health facilities, northern central Ethiopia, unmatched case -control study. PLoS ONE 2017, 12, e0173173. [Google Scholar] [CrossRef] [PubMed]
- de-Graft Aikins, A. Food Beliefs and Practices During Pregnancy in Ghana: Implications for Maternal Health Interventions. Health Care Women Intern. 2014, 35, 954–972. [Google Scholar] [CrossRef] [PubMed]
- Martin-Prével, Y.; Allemand, P.; Wiesmann, D.; Arimond, M.; Ballard, T.; Deitchler, M.; Dop, M.-C.; Kennedy, G.; Lee, W.T.; Moursi, M. Moving forward on Choosing a Standard Operational Indicator of Women’s Dietary Diversity; FAO: Rome, Italy, 2015. [Google Scholar]
- Chakona, G.; Shackleton, C. Minimum Dietary Diversity Scores for Women Indicate Micronutrient Adequacy and Food Insecurity Status in South African Towns. Nutrients 2017, 9, 812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO. Introducing the Minimum Dietary Diversity–Women (MDD-W). Global Dietary Diversity Indicator for Women; Food and Agriculture Organization and the Food and Nutrition Technical Assistance III (FANTA): Washington, DC, USA, 2014. [Google Scholar]
- Abubakari, A.; Jahn, A. Maternal Dietary Patterns and Practices and Birth Weight in Northern Ghana. PLoS ONE 2016, 11, e0162285. [Google Scholar] [CrossRef]
- WHO. Global Nutrition Targets 2025: Anaemia Policy Brief; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Ghana Statistical Service. 2010 Population and Housing Census: Regional Analytical Report, Volta Region; Ghana Statistical Service: Accra, Ghana, 2013; pp. 11–53.
- WHO. Global Database on Body Mass Index: BMI Classification; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham, F.G. Pregnancy and laboratory studies: A reference table for clinicians. Obstet. Gynecol. 2009, 114, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Cheng, T.S.; Loy, S.L.; Cheung, Y.B.; Godfrey, K.M.; Gluckman, P.D.; Kwek, K.; Saw, S.M.; Chong, Y.-S.; Lee, Y.S.; Yap, F. Demographic characteristics, health behaviors before and during pregnancy, and pregnancy and birth outcomes in mothers with different pregnancy planning status. Prev. Sci. 2016, 17, 960–969. [Google Scholar] [CrossRef] [Green Version]
- Lebso, M.; Anato, A.; Loha, E. Prevalence of anemia and associated factors among pregnant women in Southern Ethiopia: A community based cross-sectional study. PLoS ONE 2017, 12, e0188783. [Google Scholar] [CrossRef]
- Branca, F.; Mahy, L.; Mustafa, T.S. The lack of progress in reducing anaemia among women: The inconvenient truth. Bull. World Health Organ. 2014, 92, 231. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, Z.; Ananth, C.V. Prevalence and risk factors for anaemia in pregnant women: A population-based prospective cohort study in China. Paediatr. Perinat. Epidemiol. 2009, 23, 282–291. [Google Scholar] [CrossRef]
- Melku, M.; Addis, Z.; Alem, M.; Enawgaw, B. Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: An institutional based cross-sectional study. Anemia 2014, 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Liu, S.; Rao, Y.; Shi, Z.; Wang, L.; Sharma, M.; Zhao, Y. Prevalence and Sociodemographic and Lifestyle Determinants of Anemia during Pregnancy: A Cross-Sectional Study of Pregnant Women in China. Int. J. Environ. Res. Public Health 2016, 13, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agbozo, F.; Colecraft, E.; Ellahi, B. Impact of type of child growth intervention program on caregivers’ child feeding knowledge and practices: A comparative study in Ga West Municipality, Ghana. Food Sci. Nutr. 2016, 4, 562–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agbozo, F.; Atitto, P.; Jahn, A.; Abubakari, A. Nutrient composition and dietary diversity of on-site lunch meals, and anthropometry of beneficiary children in private and public primary schools in Ghana. Nutr. Health 2018, 24, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Agbozo, F.; Amardi-Mfoafo, J.; Dwase, H.; Ellahi, B. Nutrition knowledge, dietary patterns and anthropometric indices of older persons in four peri-urban communities in Ga West municipality, Ghana. Afr. Health Sci. 2018, 18, 743–755. [Google Scholar] [CrossRef] [Green Version]
- WHO. Nutritional Anaemias: Tools for Effective Prevention and Control; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Nair, M.; Choudhury, M.K.; Choudhury, S.S.; Kakoty, S.D.; Sarma, U.C.; Webster, P.; Knight, M. Association between maternal anaemia and pregnancy outcomes: A cohort study in Assam, India. BMJ Glob. Health 2016, 1, e000026. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Sub-Groups | Overall % | Micronutrient Dense Diet | Micronutrient Poor Diet | χ2 |
|---|---|---|---|---|---|
| Maternal age | <20 years 20–29 years 30–39 years ≥40 years | 8.4 54.0 32.9 4.7 | 8.8 52.7 33.3 5.2 | 7.9 56.0 32.1 4.0 | 0.753 |
| Parity | No child 1–2 children ≥3 children | 29.2 51.4 19.4 | 27.7 50.4 21.9 | 31.8 53.0 15.2 | 0.070 |
| Marital status | Married | 73.0 | 76.3 | 68.5 | 0.054 |
| Place of residence | Rural | 32.8 | 30.8 | 35.7 | 0.335 |
| Employment status | Employed | 77.7 | 79.3 | 74.0 | 0.145 |
| Educational level | None/primary Secondary Tertiary | 13.8 70.9 15.3 | 11.6 74.0 14.5 | 17.0 66.7 16.4 | 0.212 |
| Level of care | Primary a Secondary a Tertiary | 15.4 69.4 15.2 | 9.1 78.6 12.3 | 24.4 56.4 19.2 | <0.0001 |
| Pregnancy intention | Unplanned | 37.1 | 32.2 | 43.8 | 0.012 |
| HIV status | Positive | 2.1 | 2.2 | 1.9 | 0.553 |
| Hepatitis B status | Positive | 4.2 | 6.3 | 1.1 | 0.047 |
| VDRL status | Positive | 3.4 | 2.8 | 4.2 | 0.342 |
| Malaria infection | Positive b | 10.3 | 7.2 | 14.5 | 0.081 |
| Worm infestation | Positive | 4.0 | 0.0 | 10.3 | 0.021 |
| Sickling status | Positive | 14.0 | 13.4 | 14.9 | 0.437 |
| Blood group | A a B AB O a | 19.7 24.6 4.8 50.9 | 16.2 24.9 3.5 55.5 | 24.7 24.1 6.6 44.6 | 0.051 |
| Rhesus status | Negative | 6.6 | 5.7 | 7.8 | 0.263 |
| BMI c | Underweight Overweight Obese | 9.6 23.9 9.4 | 9.7 24.1 6.2 | 9.5 23.7 3.2 | 0.786 |
| MUAC c | <24 cm | 8.2 | 6.4 | 10.8 | 0.130 |
| Counselled on diet | Yes | 51.7 | 52.3 | 50.8 | 0.446 |
| Counselled on IFA | Yes | 28.8 | 25.7 | 33.1 | 0.105 |
| Takes daily IFA | Yes | 96.8 | 97.0 | 96.6 | 0.566 |
| Food taboos | Yes | 17.7 | 16.1 | 20.4 | 0.169 |
| Variable (Reference) | Sub-Groups | Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|---|
| UOR | 95% CI | p-Value | AOR | 95% CI | p-Value | ||
| Age (years) (<20 years) | 20–29 | 0.83 | 0.41–1.68 | 0.622 | 0.43 | 0.09–2.04 | 0.293 |
| 30–39 | 0.99 | 0.48–2.04 | 0.996 | 0.57 | 0.10–3.11 | 0.518 | |
| ≥40 | 2.12 | 0.64–6.96 | 0.214 | 0.62 | 0.05–6.76 | 0.701 | |
| Parity (≥3 children) | 1–2 children | 1.61 | 0.92–2.83 | 0.098 | 1.93 | 0.50–2.36 | 0.821 |
| No child | 0.83 | 0.54–1.25 | 0.382 | 1.95 | 0.71–5.33 | 0.192 | |
| Marital status (Cobabitating) | Married | 1.61 | 0.95–2.72 | 0.076 | 2.46 | 0.94–6.40 | 0.065 |
| Single | 1.5 | 0.73–3.07 | 0.269 | 1.96 | 0.51–7.47 | 0.322 | |
| Women’s employment (Unemployed) | Informal sector | 1.93 | 1.16–3.21 | 0.011 | 1.49 | 0.54-4.14 | 0.436 |
| Formal sector | 1.31 | 0.67–2.56 | 0.427 | 0.59 | 0.09–3.82 | 0.586 | |
| Student | 1.62 | 0.59–4.41 | 0.344 | 0.55 | 0.08–3.48 | 0.532 | |
| Partner’s employment (Unemployed) | Informal sector | 0.86 | 0.28–2.65 | 0.803 | 0.24 | 0.03–1.55 | 0.136 |
| Formal sector | 0.91 | 0.28–2.90 | 0.884 | 0.54 | 0.06–4.36 | 0.569 | |
| Student | 0.39 | 0.08–1.93 | 0.253 | 0.06 | 0.00–1.51 | 0.088 | |
| Women’s education (Up to primary) | JHS | 1.23 | 0.70–2.17 | 0.465 | 1.07 | 0.40–2.84 | 0.877 |
| SHS | 1.08 | 0.56–2.07 | 0.804 | 2.13 | 0.64–7.00 | 0.212 | |
| Tertiary | 1.02 | 0.51–2.03 | 0.944 | 3.74 | 0.49–28.60 | 0.203 | |
| Partner’s education (Up to primary) | JHS | 1.80 | 0.84–3.85 | 0.125 | 1.26 | 0.37–4.21 | 0.707 |
| SHS | 1.85 | 0.86–4.01 | 0.114 | 2.13 | 0.60–7.53 | 0.238 | |
| Tertiary | 1.52 | 0.70–3.28 | 0.286 | 0.69 | 0.13-3.55 | 0.663 | |
| Level of care (Primary) | Secondary | 7.32 | 4.10–13.09 | 0.000 | 5.12 | 2.12–12.37 | 0.000 |
| Tertiary | 0.72 | 0.30–1.68 | 0.448 | 0.80 | 0.20–3.09 | 0.747 | |
| Body mass index (Normal) | Underweight | 1.65 | 0.80–3.37 | 0.171 | 2.76 | 0.77–9.83 | 0.097 |
| Overweight | 0.76 | 0.48–1.21 | 0.259 | 0.71 | 0.32–1.56 | 0.415 | |
| Obese | 0.97 | 0.49–1.89 | 0.930 | 0.72 | 0.22–2.31 | 0.585 | |
| Diet counselling | Yes | 1.42 | 0.89–2.28 | 0.137 | 1.63 | 0.85–3.11 | 0.136 |
| IFA counselling | Yes | 0.71 | 0.42–1.18 | 0.194 | 1.00 | 0.47–2.11 | 0.990 |
| Pregnancy planned | Yes | 1.77 | 1.19–2.61 | 0.004 | 2.31 | 1.07–4.92 | 0.031 |
| Food taboos | Yes | 1.31 | 0.80–2.14 | 0.267 | 1.09 | 0.49–2.44 | 0.821 |
| Sickling | Positive | 3.41 | 0.73–15.77 | 0.116 | 1.20 | 0.11–13.12 | 0.880 |
| History of NCDs (None) | Hypertension | 0.97 | 0.57–1.65 | 0.915 | 0.41 | 0.16–1.08 | 0.073 |
| Diabetes | 0.58 | 0.21–1.54 | 0.278 | 0.32 | 0.04–2.53 | 0.285 | |
| Both | 1.44 | 0.49–4.24 | 0.506 | 0.95 | 0.19–4.57 | 0.953 | |
| RBC Index | Reference Rangea | Interpretation of RBC Morphology | Overall ± SD | Overall % | Micronutrient Dense | Micronutrient Poor | p-Value |
|---|---|---|---|---|---|---|---|
| Hb (g/dL) b | <7.0 | Severe | 10.80 ± 1.20 | 0.2 | 0 | 0.6 | <0.0001 |
| 7.0–9.9 | Moderate c | 23.1 | 6.2 | 47.1 | |||
| 10.0–10.9 | Mild | 31.1 | 32.5 | 29.1 | |||
| ≥11.0 | Non-anemic c | 45.5 | 61.3 | 23.3 | |||
| Hct (%) | <30 | Low c | 33.72 ± 18.20 | 22.3 | 15.7 | 39.3 | <0.0001 |
| 30–39 | Normal c | 74.7 | 80.6 | 59.5 | |||
| >39 | High | 3.0 | 3.7 | 1.2 | |||
| RBC count (×1012/L) | <2.81 | Low | 6.75 ± 29.88 | 0.3 | 0.5 | 0 | 0.788 |
| 2.81–4.49 | Normal | 81.1 | 80.6 | 82.4 | |||
| >4.49 | Polycythemia | 18.6 | 19.0 | 17.6 | |||
| MCV (fl) | <85.8 | Microcytic c | 83.45 ± 46.46 | 79.4 | 73.6 | 94.1 | 0.007 |
| 85.8–99.4 | Normal c | 18.9 | 24.1 | 5.9 | |||
| >99.4 | Macrocytic | 1.7 | 2.3 | 0 | |||
| MCH (pg/cell) | <33 | Low | 27.76 ± 15.34 | 88.4 | 86.6 | 92.9 | 0.089 |
| 30–33 | Normal | 11.6 | 13.4 | 7.1 | |||
| MCHC (g/dL) | <32.4 | Hypochromic c | 33.90 ± 13.26 | 29.3 | 24.9 | 35.8 | 0.021 |
| 32.4–35.2 | Normal c | 47.7 | 54.2 | 38.2 | |||
| >35.2 | Hyperchromic | 23.0 | 20.9 | 26.0 | |||
| RDW (%) | <12.3 | Low | 41.75 ± 19.71 | 0 | 0 | 0 | 0.365 |
| 12.3–14.7 | Normal | 2.3 | 2.8 | 1.2 | |||
| >14.7 | High | 97.7 | 97.2 | 98.8 |
| Maternal Risk Factors (Reference in Square Brackets) | Adjusted Odds Ratio (95% Confidence Interval) for Anemia | ||||
|---|---|---|---|---|---|
| Overall | 1st Trimester | 2nd Trimester | 3rd Trimester | Pre-Delivery c | |
| Maternal age a | 0.90 (0.84–0.96) * | 0.92 (0.86–0.98) * | 0.99 (0.95–1.05) | 0.94 (0.89–0.99) * | 1.01 (0.94–1.09) |
| BMI/MUAC a,b | 0.87 (0.82–0.94) * | 0.91 (0.85–0.98) * | 0.97 (0.86–1.09) | 0.99 (0.97–1.02) | 0.96 (0.84–1.10) |
| Housewife (self/formal job) | 0.31 (0.12–0.80) * | 0.67 (0.27–1.69) | 0.57 (0.16–2.05) | 0.64 (0.24–1.72) | 0.61 (0.23–1.64) |
| Primary education (tertiary) Secondary education (tertiary) | 1.45 (0.44–4.86) 1.00 (0.38–2.63) | 2.31 (0.65–8.19) 1.13 (0.40–3.18) | 0.08 (0.01–0.76) * 0.03 (0.00–0.28) * | 1.40 (0.36–5.47) 0.76 (0.27–2.09) | 0.08 (0.01–1.25) 0.21 (0.02–2.64) |
| Poor diet intake (adequate diet) | 2.73 (1.35–5.50) * | 2.53 (1.28–4.99) * | 2.99 (1.12–8.02) * | 4.18 (1.97–8.87) * | 1.63 (0.65–4.08) * |
| No dietary advice (counselled) | 1.14 (0.63–2.09) | 2.07 (1.07–3.98) * | 1.98 (0.78–4.99) | 1.48 (0.77–2.81) | 3.52 (1.11–11.15) * |
| No IFA advice (counselled) | 1.23 (0.63–2.39) | 0.84 (0.42–1.67) | 1.74 (0.24–12.77) | 2.40 (1.13–5.09) * | 1.27 (0.44–3.67) |
| Non-routine IFA use (daily IFA) | 1.08 (0.10–11.54) | 2.08 (0.42–10.17) | 2.24 (0.25–19.89) | 7.05 (1.06–46.81) * | 3.42 (0.31–37.37) |
| Positive sickle cell (negative) | 1.30 (0.53–3.19) | 1.26 (0.53–3.03) | 1.14 (0.39–3.37) | 2.55 (1.07–6.08) * | 1.33 (0.44–4.06) |
| Positive malaria (negative) | 1.64 (0.52–5.17) | 5.32 (1.35–20.90) * | 3.42 (1.11–10.54) * | 3.06 (0.84–11.18) | 2.05 (0.47–8.97) |
| No. antenatal care visits a | 0.85 (0.75–0.96) * | - | 0.77 (0.63–0.95) * | 0.80 (0.76–0.96) * | 0.76 (0.62–0.94) * |
| No. of IPT in pregnancy a | 1.06 (0.74–1.50) | - | 1.02 (0.64–1.60) | 0.95 (0.65–1.39) | 1.01 (0.67– 1.52) |
| Preeclampsia (No) | 0.94 (0.45–1.93) | - | 0.86 (0.31–2.40) | 2.71 (1.23–5.99) * | 3.38 (1.17–9.76) * |
| Gestational diabetes (negative) | 0.93 (0.41–2.10) | - | 0.76 (0.32–1.79) | 1.03 (0.32–3.38) | 2.13 (0.54–8.35) |
| Model summary | n = 250; Prob > chi2 = 0.0000; R2 = 0.2205; Log likelihood = −122.113 | n = 291; Prob > chi2 = 0.0000; R2 = 0.2112; Log likelihood = −161.213 | n = 244; Prob > chi2 = 0.0000; R2 = 0.1963; Log likelihood = −112.009 | n = 248; Prob > chi2 = 0.0000; R2 = 0.1898; Log likelihood = −129.755 | n = 245; Prob > chi2 = 0.0022; R2 = 0.1858; Log likelihood = −90.505 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbozo, F.; Abubakari, A.; Der, J.; Jahn, A. Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery. Nutrients 2020, 12, 777. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030777
Agbozo F, Abubakari A, Der J, Jahn A. Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery. Nutrients. 2020; 12(3):777. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030777
Chicago/Turabian StyleAgbozo, Faith, Abdulai Abubakari, Joyce Der, and Albrecht Jahn. 2020. "Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery" Nutrients 12, no. 3: 777. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030777