Effect of a Multispecies Probiotic on Intestinal and Skin Colonization by Multidrug-Resistant Gram-Negative Bacteria in Patients in a Long-Term Care Facility: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Design
2.3. Microbiological Methods
2.4. Whole-Genome Sequencing
2.5. DNA Isolation for Microbiome Analysis, 16S rRNA Gene PCR Amplification and Sequencing
3. Results
3.1. Patients’ Characteristics
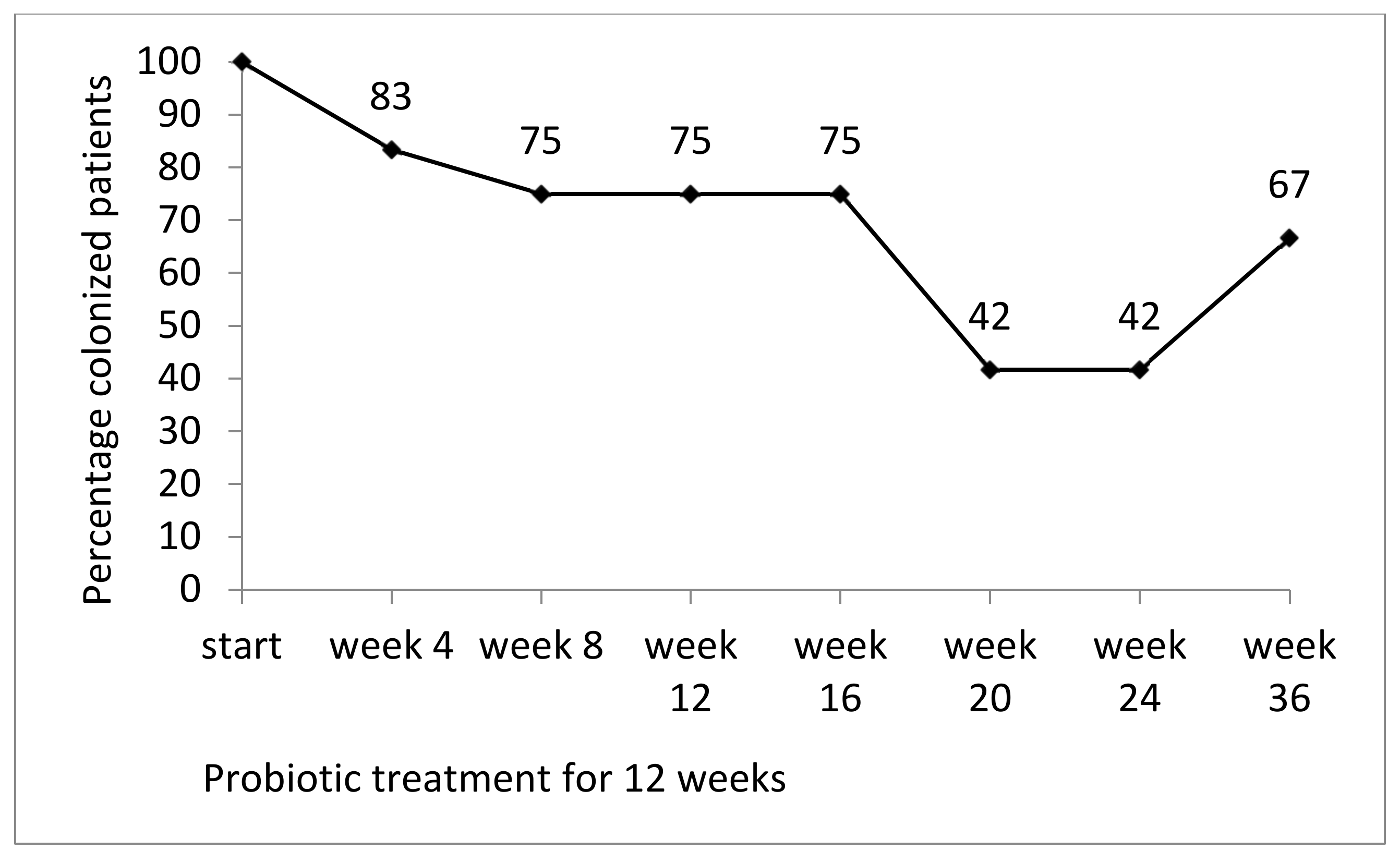
3.2. Prevalence of Colonization by MRGN Bacteria During and after Probiotic Treatment
3.1.1. Stool
3.1.2. Skin
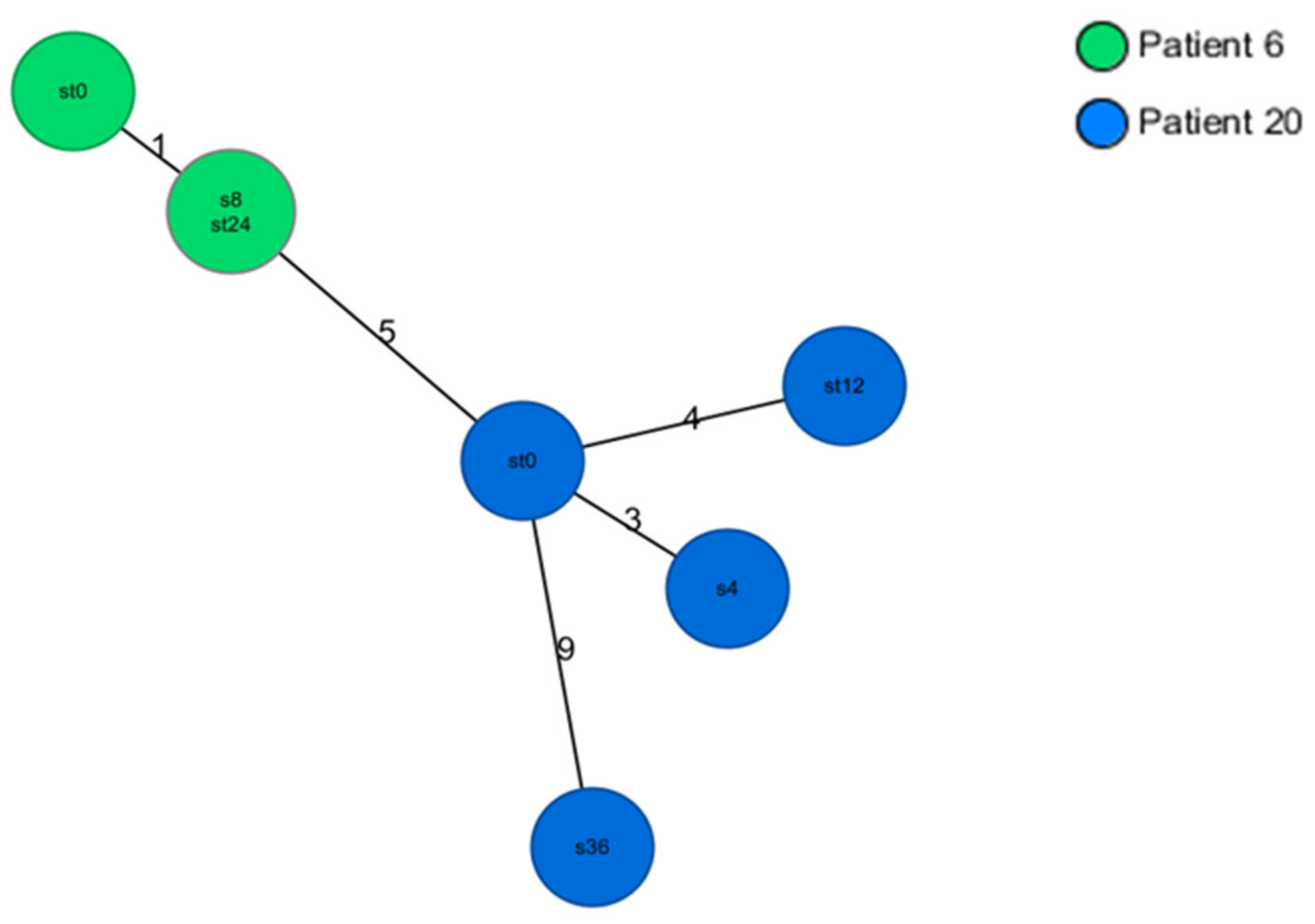
3.3. Genetic Relatedness of E. coli and K. pneumoniae Isolates
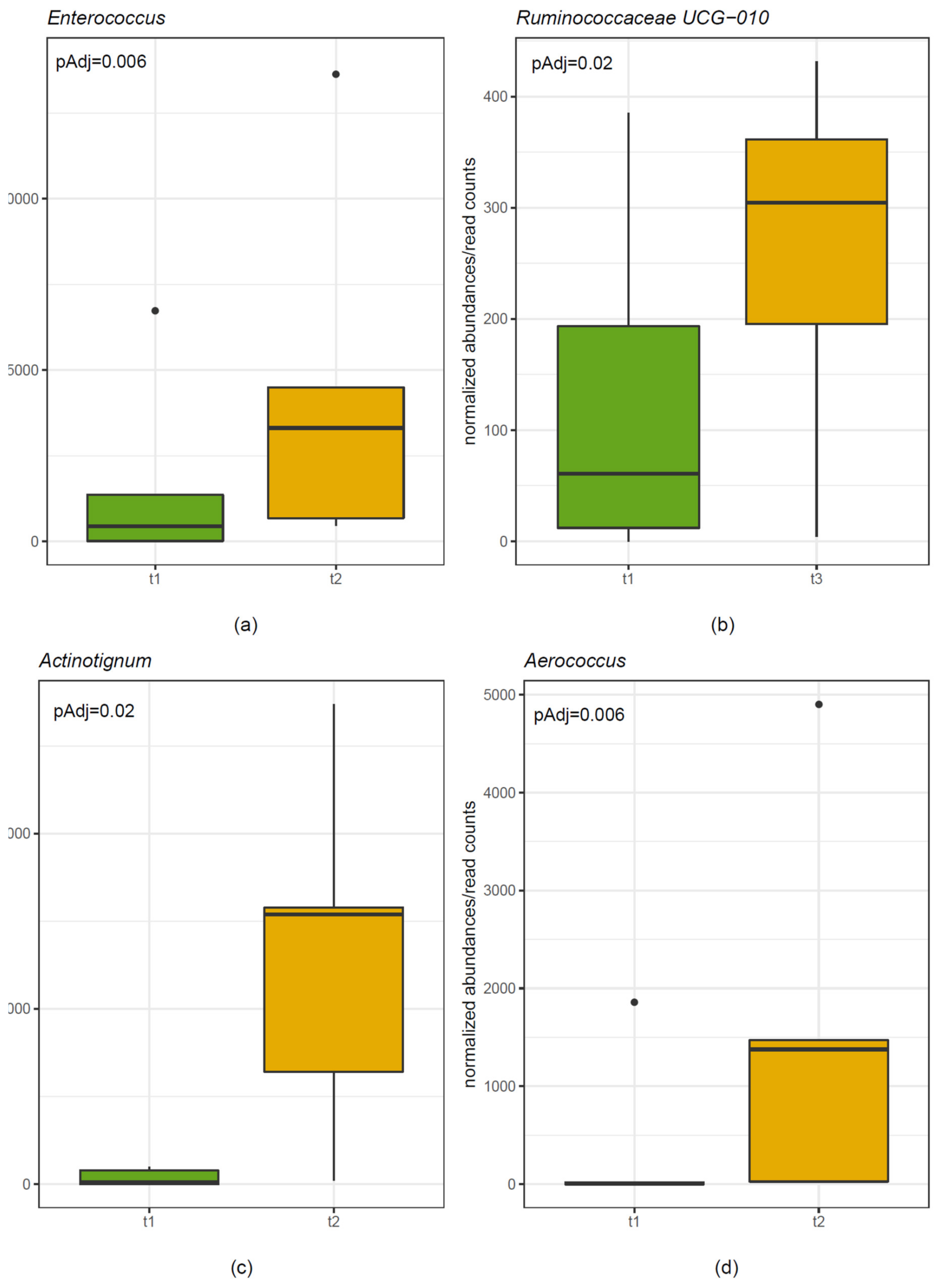
3.4. Microbiome Analysis
3.4.1. Stool
3.4.2. Skin
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A


Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isolate | Amox/clav | Pip | Pip/Taz | CAZ | Cefepim | Mero | Imi | Cipro | Azt | Genta | ESBL |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient 6 | |||||||||||
| K. pneumoniae (week 0, stool) | R | R | S | R | R | S | S | R | R | R | + |
| K. pneumoniae (week 24, stool) | R | R | S | R | R | S | S | R | R | R | + |
| K. pneumoniae (week 8, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient 20 | |||||||||||
| K. pneumoniae (week 0, stool) | R | R | S | R | R | S | S | R | R | R | + |
| K. pneumoniae (week 12, stool) | R | R | S | R | R | S | S | R | R | R | + |
| K. pneumoniae (week 4, skin) | R | R | S | R | R | S | S | R | R | R | + |
| K. pneumoniae (week 36, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient 15 | |||||||||||
| E. coli (week 0, stool) | R | R | S | R | R | S | S | R | R | S | + |
| E. coli (week 36, stool) | R | R | S | R | R | S | S | R | R | S | + |
| E. coli (week 12, skin) | R | R | S | R | R | S | S | R | R | S | + |
| Patient 19 | |||||||||||
| E. coli (week 0, stool) | R | R | S | R | R | S | S | R | R | S | + |
| E. coli (week 8, stool) | R | R | S | R | R | S | S | R | R | S | + |
| E. coli (week 0, skin) | R | R | S | R | R | S | S | R | R | S | + |
| Patient 13 | |||||||||||
| E. coli (week 0, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 36, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 4, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient 16 | |||||||||||
| E. coli (week 0, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 36, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 20, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient 18 | |||||||||||
| E. coli (week 0, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 12, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 8, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient 21 | |||||||||||
| E. coli (week 4, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 16, stool) | R | R | S | R | R | S | S | R | R | R | + |
| E. coli (week 24, skin) | R | R | S | R | R | S | S | R | R | R | + |
| Patient | Start | Week 4 | Week 8 | Week 12 | Week 16 | Week 20 | Week 24 | Week 36 | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Stool | E. coli | - | - | - | - | - | - | - |
| Skin | A. baumannii | - | - | - | - | A. baumannii | A. baumannii | A. baumannii | |
| 2 | Stool | K. oxytoca | - | K. oxytocaAC | K. oxytoca | - | - | - | - |
| Skin | - | - | K. oxytoca | K. oxytoca | - | - | - | A. baumanni | |
| 5 | Stool | E. coli | E. coli/ K. aerog. | E. coli | E. coli | E. coli | - | E. coli | E. coli |
| Skin | E. cloacae | - | - | - | E. coli | E. coli | - | - | |
| 6 | Stool | K. pneumoniae# | K. pneumoniae | K. pneumoniaeC | - | K. pneumoniae | K. pneumoniae | K. pneumoniae# | K. pneumoniae |
| Skin | - | K. pneumoniae | K. pneumoniae# | K. pneumoniae | K. pneumoniae | - | - | - | |
| 12 | Stool | P. aeruginosa | P. aeruginosa | P. aeruginosa | P. aeruginosa | P. aeruginosa | - | - | - |
| Skin | - | - | - | - | - | - | - | - | |
| 13 | Stool | E. coli * | E. coli | - | E. coli | E. coli | - | E. coli | E. coli* |
| Skin | - | E. coli * | E. coli | E. coli | - | E. coli | E. coli | - | |
| 15 | Stool | E. coli§ | - | E. coli | E. coli | E. coli | E. coli | E. coli | E. coli§ |
| Skin | E. coli | - | - | E. coli§ | - | E. coli | - | - | |
| 16 | Stool | E. coli& | E. coli | E. coli | E. coli | E. coli | E. coli | E. coli | E. coli& |
| Skin | K. pneumoniae | - | K. pneumoniae | K. pneumoniae | K. pneumoniae | E.coli&/K. pn. | - | K. pneumoniae | |
| 18 | Stool | E. coli$ | E. coliAC | - | E. coli$ | A. baumannii | - | - | M. morganii |
| Skin | P. aeruginosa | A. baumannii | E. coli$ | - | A. baumannii | A. baumannii | A. baumannii | P. aeruginosa | |
| 19 | Stool | E. coli ° | E. coli | E. coli° | - | - | - | - | M. morganii |
| Skin | E. coli ° | - | - | - | - | - | - | - | |
| 20 | Stool | K. pneumoniae# | K. pneumoniae | K. pneumoniae | K. pneumoniae# | K. pneumoniaeAC | K. pneumoniae | - | - |
| Skin | - | K. pneumoniae# | K. pneumoniae | K. pneumoniae | K. pneumoniae | K. pneumoniae | - | K. pneumoniae# | |
| 21 | Stool | E. coli | E. coli ** | E. coli | E. coli | E. coli ** | E. coli | -AC | K. pneumoniae |
| Skin | E. coli | - | E. coli | - | - | - | E. coli ** | E. coli |
References
- Thorpe, K.E.; Joski, P.; Johnston, K.J. Antibiotic-resistant infection treatment costs have doubled since 2002, now exceeding $2 billion annually. Health Aff. 2018, 37, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Anand, D.; Purwar, S.; Upadhye, K.V.; Gupta, P.; Dhar, D. Association of high mortality with extended-spectrum beta-lactamase (esbl) positive cultures in community acquired infections. J. Crit. Care 2018, 44, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Donskey, C.J. The role of the intestinal tract as a reservoir and source for transmission of nosocomial pathogens. Clin. Infect. Dis. 2004, 39, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruppe, E.; Armand-Lefevre, L.; Estellat, C.; Consigny, P.H.; El Mniai, A.; Boussadia, Y.; Goujon, C.; Ralaimazava, P.; Campa, P.; Girard, P.M.; et al. High rate of acquisition but short duration of carriage of multidrug-resistant enterobacteriaceae after travel to the tropics. Clin. Infect. Dis. 2015, 61, 593–600. [Google Scholar] [CrossRef]
- Isendahl, J.; Giske, C.G.; Hammar, U.; Sparen, P.; Tegmark, W.K.; Ternhag, A.; Naucler, P. Temporal dynamics and risk factors for bloodstream infection with extended-spectrum beta-lactamase-producing bacteria in previously-colonized individuals: National population-based cohort study. Clin. Infect. Dis. 2019, 68, 641–649. [Google Scholar] [CrossRef]
- Ruscher, C.; Pfeifer, Y.; Layer, F.; Schaumann, R.; Levin, K.; Mielke, M. Inguinal skin colonization with multidrug-resistant bacteria among residents of elderly care facilities: Frequency, persistence, molecular analysis and clinical impact. Int. J. Med. Microbiol. 2014, 304, 1123–1134. [Google Scholar] [CrossRef]
- March, A.; Aschbacher, R.; Dhanji, H.; Livermore, D.M.; Bottcher, A.; Sleghel, F.; Maggi, S.; Noale, M.; Larcher, C.; Woodford, N. Colonization of residents and staff of a long-term-care facility and adjacent acute-care hospital geriatric unit by multiresistant bacteria. Clin. Microbiol. Infect. 2010, 16, 934–944. [Google Scholar] [CrossRef]
- Rooney, P.J.; O’Leary, M.C.; Loughrey, A.C.; McCalmont, M.; Smyth, B.; Donaghy, P.; Badri, M.; Woodford, N.; Karisik, E.; Livermore, D.M. Nursing homes as a reservoir of extended-spectrum beta-lactamase (esbl)-producing ciprofloxacin-resistant escherichia coli. J. Antimicrob. Chemother. 2009, 64, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Cochard, H.; Aubier, B.; Quentin, R.; van der Mee-Marquet, N.; Reseau des Hygienistes du, C. Extended-spectrum beta-lactamase-producing enterobacteriaceae in french nursing homes: An association between high carriage rate among residents, environmental contamination, poor conformity with good hygiene practice, and putative resident-to-resident transmission. Infect. Control Hosp. Epidemiol. 2014, 35, 384–389. [Google Scholar]
- Leitner, E.; Zechner, E.; Ullrich, E.; Zarfel, G.; Luxner, J.; Pux, C.; Pichler, G.; Schippinger, W.; Krause, R.; Zollner-Schwetz, I. Low prevalence of colonization with multidrug-resistant gram-negative bacteria in long-term care facilities in graz, austria. Am. J. Infect. Control 2018, 46, 76–80. [Google Scholar] [CrossRef]
- Huttner, B.; Haustein, T.; Uckay, I.; Renzi, G.; Stewardson, A.; Schaerrer, D.; Agostinho, A.; Andremont, A.; Schrenzel, J.; Pittet, D.; et al. Decolonization of intestinal carriage of extended-spectrum beta-lactamase-producing enterobacteriaceae with oral colistin and neomycin: A randomized, double-blind, placebo-controlled trial. J. Antimicrob. Chemother. 2013, 68, 2375–2382. [Google Scholar] [PubMed] [Green Version]
- Saidel-Odes, L.; Polachek, H.; Peled, N.; Riesenberg, K.; Schlaeffer, F.; Trabelsi, Y.; Eskira, S.; Yousef, B.; Smolykov, R.; Codish, S.; et al. A randomized, double-blind, placebo-controlled trial of selective digestive decontamination using oral gentamicin and oral polymyxin e for eradication of carbapenem-resistant klebsiella pneumoniae carriage. Infect. Control Hosp. Epidemiol. 2012, 33, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Tascini, C.; Sbrana, F.; Flammini, S.; Tagliaferri, E.; Arena, F.; Leonildi, A.; Ciullo, I.; Amadori, F.; Di Paolo, A.; Ripoli, A.; et al. Oral gentamicin gut decontamination for prevention of kpc-producing klebsiella pneumoniae infections: Relevance of concomitant systemic antibiotic therapy. Antimicrob. Agents Chemother. 2014, 58, 1972–1976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Mazzaferri, F.; de Smet, A.M.; Bragantini, D.; Eggimann, P.; Huttner, B.D.; Kuijper, E.J.; Lucet, J.C.; Mutters, N.T.; Sanguinetti, M.; et al. Escmid-eucic clinical guidelines on decolonization of multidrug-resistant gram-negative bacteria carriers. Clin. Microbiol. Infect. 2019, 25, 807–817. [Google Scholar] [CrossRef] [Green Version]
- Saidani, N.; Lagier, J.C.; Cassir, N.; Million, M.; Baron, S.; Dubourg, G.; Eldin, C.; Kerbaj, J.; Valles, C.; Raoult, D.; et al. Faecal microbiota transplantation shortens the colonisation period and allows re-entry of patients carrying carbapenamase-producing bacteria into medical care facilities. Int. J. Antimicrob. Agents 2019, 53, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Bilinski, J.; Grzesiowski, P.; Sorensen, N.; Madry, K.; Muszynski, J.; Robak, K.; Wroblewska, M.; Dzieciatkowski, T.; Dulny, G.; Dwilewicz-Trojaczek, J.; et al. Fecal microbiota transplantation in patients with blood disorders inhibits gut colonization with antibiotic-resistant bacteria: Results of a prospective, single-center study. Clin. Infect. Dis. 2017, 65, 364–370. [Google Scholar] [CrossRef]
- Huttner, B.D.; de Lastours, V.; Wassenberg, M.; Maharshak, N.; Mauris, A.; Galperine, T.; Zanichelli, V.; Kapel, N.; Bellanger, A.; Olearo, F.; et al. A 5-day course of oral antibiotics followed by faecal transplantation to eradicate carriage of multidrug-resistant enterobacteriaceae: A randomized clinical trial. Clin. Microbiol. Infect. 2019, 25, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Sanders, M.E. Probiotics: Definition, sources, selection, and uses. Clin. Infect. Dis. 2008, 46 (Suppl. 2), S58–S61. [Google Scholar] [CrossRef] [Green Version]
- Brunel, A.S.; Guery, B. Multidrug resistant (or antimicrobial-resistant) pathogens—Alternatives to new antibiotics? Swiss Med. Wkly 2017, 147, w14553. [Google Scholar]
- Walker, W.A. Mechanisms of action of probiotics. Clin. Infect. Dis. 2008, 46 (Suppl. 2), S87–S91. [Google Scholar] [CrossRef]
- Hachimura, S.; Totsuka, M.; Hosono, A. Immunomodulation by food: Impact on gut immunity and immune cell function. Biosci. Biotechnol. Biochem. 2018, 82, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.J.; Macfarlane, G.T. Nondigestible oligosaccharides enhance bacterial colonization resistance against clostridium difficile in vitro. Appl. Environ. Microbiol. 2003, 69, 1920–1927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koning, C.J.; Jonkers, D.M.; Stobberingh, E.E.; Mulder, L.; Rombouts, F.M.; Stockbrugger, R.W. The effect of a multispecies probiotic on the intestinal microbiota and bowel movements in healthy volunteers taking the antibiotic amoxycillin. Am. J. Gastroenterol. 2008, 103, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Zollner-Schwetz, I.; Zechner, E.; Ullrich, E.; Luxner, J.; Pux, C.; Pichler, G.; Schippinger, W.; Krause, R.; Leitner, E. Colonization of long term care facility patients with mdr-gram-negatives during an acinetobacter baumannii outbreak. Antimicrob. Resist. Infect. Control 2017, 6, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Der KRINKO, E. Hygienemaßnahmen bei infektionen oder besiedlung mit multiresistenten gramnegativen stäbchen. Bundesgesundheitsblatt; Springer: Berlin/Heidelberg, Germany, 2012; pp. 1311–1354. [Google Scholar]
- Stadlbauer, V. Immunosuppression and probiotics: Are they effective and safe? Benef. Microbes. 2015, 6, 823–828. [Google Scholar] [CrossRef]
- Schlager, S.; Lepuschitz, S.; Ruppitsch, W.; Ableitner, O.; Pietzka, A.; Neubauer, S.; Stöger, A.; Lassnig, H.; Mikula, C.; Springer, B.; et al. Petting zoos as sources of shiga toxin-producing escherichia coli (stec) infections. Int. J. Med. Microbiol. 2018, 308, 927–932. [Google Scholar] [CrossRef]
- Lepuschitz, S.; Schill, S.; Stoeger, A.; Pekard-Amenitsch, S.; Huhulescu, S.; Inreiter, N.; Hartl, R.; Kerschner, H.; Sorschag, S.; Springer, B.; et al. Whole genome sequencing reveals resemblance between esbl-producing and carbapenem resistant klebsiella pneumoniae isolates from austrian rivers and clinical isolates from hospitals. Sci. Total Environ. 2019, 662, 227–235. [Google Scholar] [CrossRef]
- Diancourt, L.; Passet, V.; Verhoef, J.; Grimont, P.A.; Brisse, S. Multilocus sequence typing of klebsiella pneumoniae nosocomial isolates. J. Clin. Microbiol. 2005, 43, 4178–4182. [Google Scholar] [CrossRef] [Green Version]
- Klymiuk, I.; Bilgilier, C.; Stadlmann, A.; Thannesberger, J.; Kastner, M.T.; Hogenauer, C.; Puspok, A.; Biowski-Frotz, S.; Schrutka-Kolbl, C.; Thallinger, G.G.; et al. The human gastric microbiome is predicated upon infection with helicobacter pylori. Front. Microbiol. 2017, 8, 2508. [Google Scholar] [CrossRef] [Green Version]
- McKenna, P.; Hoffmann, C.; Minkah, N.; Aye, P.P.; Lackner, A.; Liu, Z.; Lozupone, C.A.; Hamady, M.; Knight, R.; Bushman, F.D. The macaque gut microbiome in health, lentiviral infection, and chronic enterocolitis. PLoS Pathog. 2008, 4, e20. [Google Scholar] [CrossRef] [Green Version]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. Dada2: High-resolution sample inference from illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using qiime 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glockner, F.O. The silva ribosomal rna gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Price, M.N.; Dehal, P.S.; Arkin, A.P. Fasttree 2--approximately maximum-likelihood trees for large alignments. PLoS ONE 2010, 5, e9490. [Google Scholar] [CrossRef] [PubMed]
- Katoh, K.; Standley, D.M. Mafft multiple sequence alignment software version 7: Improvements in performance and usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Reeve, J.; Zhang, L.; Huang, S.; Wang, X.; Chen, J. Gmpr: A robust normalization method for zero-inflated count data with application to microbiome sequencing data. PeerJ 2018, 6, e4600. [Google Scholar] [CrossRef]
- Indra, A.; Schmid, D.; Huhulescu, S.; Simons, E.; Hell, M.; Stickler, K.; Allerberger, F.; Austrian, C.d.S.G. Clostridium difficile ribotypes in austria: A multicenter, hospital-based survey. Wien. Klin. Wochenschr. 2015, 127, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Coman, M.M.; Verdenelli, M.C.; Cecchini, C.; Silvi, S.; Orpianesi, C.; Boyko, N.; Cresci, A. In vitro evaluation of antimicrobial activity of lactobacillus rhamnosus imc 501((r)), lactobacillus paracasei imc 502((r)) and synbio((r)) against pathogens. J. Appl. Microbiol. 2014, 117, 518–527. [Google Scholar] [CrossRef]
- Ljungquist, O.; Kampmann, C.; Resman, F.; Riesbeck, K.; Tham, J. Probiotics for intestinal decolonization of esbl-producing enterobacteriaceae: A randomized, placebo-controlled clinical trial. Clin. Microbiol. Infect. 2020, 26, 456–462. [Google Scholar] [CrossRef]
- O’Neill, C.A.; Monteleone, G.; McLaughlin, J.T.; Paus, R. The gut-skin axis in health and disease: A paradigm with therapeutic implications. Bioessays 2016, 38, 1167–1176. [Google Scholar] [CrossRef]
- Bowe, W.P.; Logan, A.C. Acne vulgaris, probiotics and the gut-brain-skin axis—Back to the future? Gut. Pathog. 2011, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gueniche, A.; Philippe, D.; Bastien, P.; Reuteler, G.; Blum, S.; Castiel-Higounenc, I.; Breton, L.; Benyacoub, J. Randomised double-blind placebo-controlled study of the effect of lactobacillus paracasei ncc 2461 on skin reactivity. Benef. Microbes 2014, 5, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Reygagne, P.; Bastien, P.; Couavoux, M.P.; Philippe, D.; Renouf, M.; Castiel-Higounenc, I.; Gueniche, A. The positive benefit of lactobacillus paracasei ncc2461 st11 in healthy volunteers with moderate to severe dandruff. Benef. Microbes 2017, 8, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Bar-Yoseph, H.; Hussein, K.; Braun, E.; Paul, M. Natural history and decolonization strategies for esbl/carbapenem-resistant enterobacteriaceae carriage: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 71, 2729–2739. [Google Scholar] [CrossRef]
- Wachholz, P.A.; Nunes, V.D.S.; Polachini do Valle, A.; Jacinto, A.F.; Villas-Boas, P.J.F. Effectiveness of probiotics on the occurrence of infections in older people: Systematic review and meta-analysis. Age Ageing 2018, 47, 527–536. [Google Scholar] [CrossRef] [Green Version]




| Characteristics | ACU | Geriatric Wards |
|---|---|---|
| Number of patients | 12 | 9 |
| Age (years, median, range) | 59 (19–80) | 86 (77–100) |
| Gender, n (%) | ||
| Male | 8 (66) | 5 (55) |
| Female | 4 (33) | 4 (45) |
| Comorbidities, n (%) | ||
| Parkinson’s disease | 0 | 2 (22) |
| Coronary heart disease | 0 | 2 (22) |
| Dementia | 0 | 7 (77) |
| Functional status, n (%) | ||
| Bedridden | 12 (100) | 2 (22) |
| Bowel incontinence, n (%) | 12 (100) | 6 (66) |
| Bladder incontinence, n (%) | 12 (100) | 4 (45) |
| Gastrostomy, n (%) | 12 (100) | 1 (11) |
| Antibiotic treatment, n (%) | ||
| During probiotic | 5 (41) | 0 |
| After probiotics | 3 (25) | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zollner-Schwetz, I.; Scarpatetti, M.; Pichler, G.; Pux, C.; Klymiuk, I.; Trajanoski, S.; Krause, R. Effect of a Multispecies Probiotic on Intestinal and Skin Colonization by Multidrug-Resistant Gram-Negative Bacteria in Patients in a Long-Term Care Facility: A Pilot Study. Nutrients 2020, 12, 1586. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061586
Zollner-Schwetz I, Scarpatetti M, Pichler G, Pux C, Klymiuk I, Trajanoski S, Krause R. Effect of a Multispecies Probiotic on Intestinal and Skin Colonization by Multidrug-Resistant Gram-Negative Bacteria in Patients in a Long-Term Care Facility: A Pilot Study. Nutrients. 2020; 12(6):1586. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061586
Chicago/Turabian StyleZollner-Schwetz, Ines, Monika Scarpatetti, Gerald Pichler, Christian Pux, Ingeborg Klymiuk, Slave Trajanoski, and Robert Krause. 2020. "Effect of a Multispecies Probiotic on Intestinal and Skin Colonization by Multidrug-Resistant Gram-Negative Bacteria in Patients in a Long-Term Care Facility: A Pilot Study" Nutrients 12, no. 6: 1586. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061586