A Double-Blind, Randomized Placebo-Controlled Trial of Probiotic Lactobacillus casei Shirota in Stable Cirrhotic Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
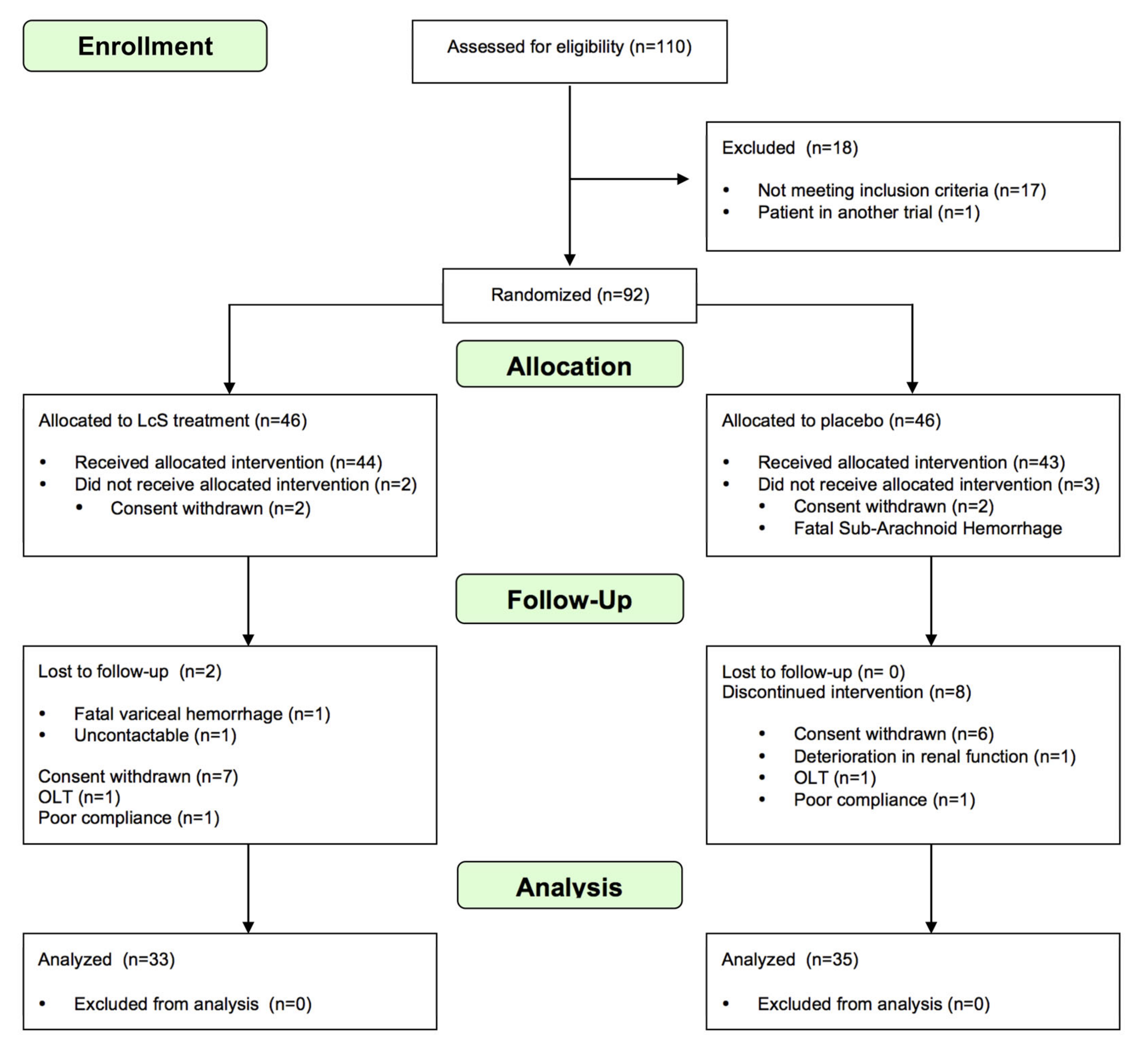
2.1. Patient Selection, Randomization and Study Outline
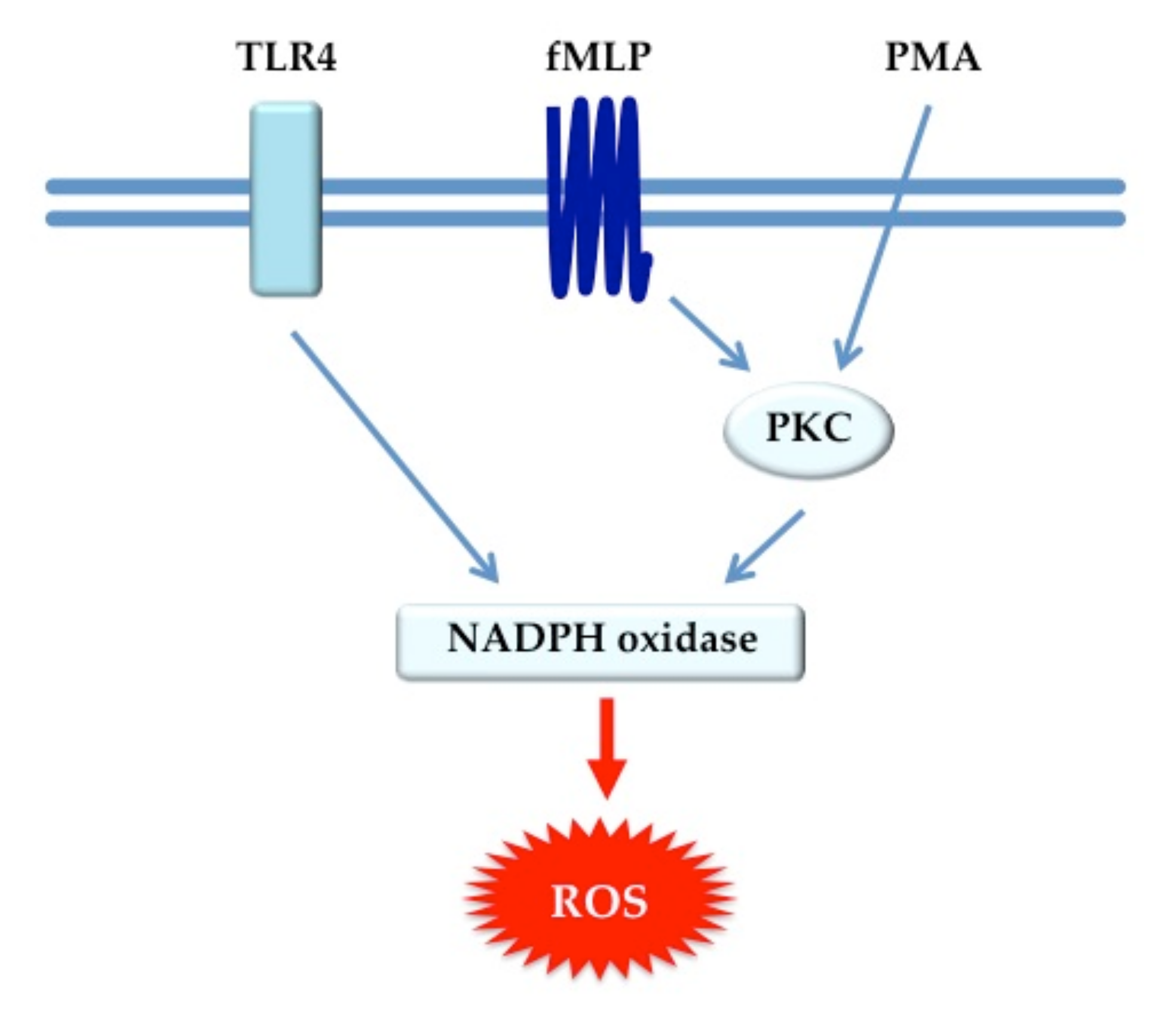
2.2. Neutrophil Function Tests
2.3. Lactulose/Rhamnose Assay
2.4. Markers of Bacterial Translocation
2.5. Plasma Cytokine Measurement
2.6. Urinary Metabolic Profiling Using 1H NMR Spectroscopy
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Neutrophil Function
3.3. Infective Episodes and Decompensation Rates
3.4. Intestinal Permeability, Markers of Bacterial Translocation and Urinary Metabolic Profiling
3.5. Plasma Cytokine Concentrations
3.6. Quality of Life Assessment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Claria, J.; Arroyo, V.; Moreau, R. The Acute-on-Chronic Liver Failure Syndrome, or When the Innate Immune System Goes Astray. J. Immunol. 2016, 197, 3755–3761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437. [Google Scholar] [CrossRef]
- Mookerjee, R.P.; Stadlbauer, V.; Lidder, S.; Wright, G.A.; Hodges, S.J.; Davies, N.A.; Jalan, R. Neutrophil dysfunction in alcoholic hepatitis superimposed on cirrhosis is reversible and predicts the outcome. Hepatology 2007, 46, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Navasa, M.; Planas, R.; Montoliu, S.; Monfort, D.; Soriano, G.; Vila, C.; Pardo, A.; Quintero, E.; Vargas, V.; et al. Primary Prophylaxis of Spontaneous Bacterial Peritonitis Delays Hepatorenal Syndrome and Improves Survival in Cirrhosis. Gastroenterology 2007, 133, 818–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiest, R.; Garcia-Tsao, G. Bacterial translocation (BT) in cirrhosis. Hepatology 2005, 41, 422–433. [Google Scholar] [CrossRef]
- Riordan, S.M.; Williams, R. The intestinal flora and bacterial infection in cirrhosis. J. Hepatol. 2006, 45, 744–757. [Google Scholar] [CrossRef]
- Liu, Q.; Duan, Z.P.; Ha, D.K.; Bengmark, S.; Kurtovic, J.; Riordan, S.M. Synbiotic modulation of gut flora: Effect on minimal hepatic encephalopathy in patients with cirrhosis. Hepatology 2004, 39, 1441–1449. [Google Scholar] [CrossRef]
- Dbouk, N.; McGuire, B.M. Hepatic encephalopathy: A review of its pathophysiology and treatment. Curr Treat. Options Gastroenterol. 2006, 9, 464–474. [Google Scholar] [CrossRef]
- Lirussi, F.; Mastropasqua, E.; Orando, S.; Orlando, R. Probiotics for non-alcoholic fatty liver disease and/or steatohepatitis. Cochrane Database Syst. Rev. 2007, 1, CD005165. [Google Scholar] [CrossRef]
- Saab, S.; Suraweera, D.; Au, J.; Saab, E.G.; Alper, T.S.; Tong, M.J. Probiotics are helpful in hepatic encephalopathy: A meta-analysis of randomized trials. Liver Int. 2016, 36, 986–993. [Google Scholar] [CrossRef]
- Rayes, N.; Seehofer, D.; Hansen, S.; Boucsein, K.; Müller, A.R.; Serke, S.; Bengmark, S.; Neuhaus, P. Early enteral supply of lactobacillus and fiber versus selective bowel decontamination: A controlled trial in liver transplant recipients. Transplantation 2002, 74, 123–128. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, A.L.; Rajkumar, C.; Cooke, J.; Bulpitt, C.J. Probiotics in prevention of antibiotic associated diarrhoea: Meta-analysis. BMJ 2002, 324, 1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cremonini, F.; Di Caro, S.; Nista, E.C.; Bartolozzi, F.; Capelli, G.; Gasbarrini, G.; Gasbarrini, A. Meta-analysis: The effect of probiotic administration on antibiotic-associated diarrhoea. Aliment. Pharmacol. Ther. 2002, 16, 1461–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarland, L.V. Meta-analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am. J. Gastroenterol. 2006, 101, 812–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadlbauer, V.; Mookerjee, R.P.; Hodges, S.; Wright, G.A.; Davies, N.A.; Jalan, R. Effect of probiotic treatment on deranged neutrophil function and cytokine responses in patients with compensated alcoholic cirrhosis. J. Hepatol. 2008, 48, 945–951. [Google Scholar] [CrossRef]
- Zapater, P.; Francés, R.; González-Navajas, J.; De La Hoz, M.A.; Moreu, R.; Pascual, S.; Monfort, D.; Montoliu, S.; Vila, C.; Escudero, A.; et al. Serum and ascitic fluid bacterial DNA: A new independent prognostic factor in noninfected patients with cirrhosis. Hepatology 2008, 48, 1924–1931. [Google Scholar] [CrossRef]
- Beckonert, O.; Keun, H.C.; Ebbels, T.M.D.; Bundy, J.G.; Holmes, E.; Lindon, J.C.; Nicholson, J.K. Metabolic profiling, metabolomic and metabonomic procedures for NMR spectroscopy of urine, plasma, serum and tissue extracts. Nat. Protoc. 2007, 2, 2692–2703. [Google Scholar] [CrossRef]
- Cox, I.J.; E Aliev, A.; Crossey, M.M.; Dawood, M.; Al-Mahtab, M.; Akbar, S.M.; Rahman, S.; Riva, A.; Williams, R.; Taylor-Robinson, S.D. Urinary nuclear magnetic resonance spectroscopy of a Bangladeshi cohort with hepatitis-B hepatocellular carcinoma: A biomarker corroboration study. World J. Gastroenterol. 2016, 22, 4191–4200. [Google Scholar] [CrossRef] [Green Version]
- Bouatra, S.; Aziat, F.; Mandal, R.; Guo, A.C.; Wilson, M.R.; Knox, C.; Bjorndahl, T.C.; Krishnamurthy, R.; Saleem, F.; Liu, P.; et al. The Human Urine Metabolome. PLoS ONE 2013, 8, e73076. [Google Scholar] [CrossRef] [Green Version]
- Åberg, K.M. Variance Reduction in Analytical Chemistry: New Numerical Methods in Chemometrics and Molecular simulation. Ph.D. Thesis, Stockholm University, Stockholm, Sweden, 2004. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Fergusson, D. CONSORT 2010 changes and testing blindness in RCTs. Lancet 2010, 375, 1144–1146. [Google Scholar] [CrossRef]
- Macnaughtan, J.; Jalan, R. Clinical and pathophysiological consequences of alterations in the microbiome in cirrhosis. Am. J. Gastroenterol. 2015, 110, 1399–1410. [Google Scholar] [CrossRef] [PubMed]
- Szuster-Ciesielska, A.; Daniluk, J.; Kandefer-Szerszen, M. Alcohol-related cirrhosis with pancreatitis. The role of oxidative stress in the progression of the disease. Arch. Immunol. Ex. 2001, 49, 139–146. [Google Scholar]
- Qin, N.; Yang, F.; Li, A.; Prifti, E.; Chen, Y.; Shao, L.; Guo, J.; Le Chatelier, E.; Yao, J.; Wu, L.; et al. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014, 513, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Panasiuk, A.; Wysocka, J.; Maciorkowska, E.; Panasiuk, B.; Prokopowicz, D.; Zak, J.; Radomski, K. Phagocytic and oxidative burst activity of neutrophils in the end stage of liver cirrhosis. World J. Gastroenterol. 2005, 11, 7661–7665. [Google Scholar] [CrossRef]
- Kim, J.K.; Chon, C.Y.; Kim, J.H.; Kim, Y.J.; Cho, J.H.; Bang, S.; Ahn, S.H.; Han, K.-H.; Moon, Y.M. Changes in Serum and Ascitic Monocyte Chemotactic Protein-1 (MCP-1) and IL-10 Levels in Cirrhotic Patients with Spontaneous Bacterial Peritonitis. J. Interf. Cytokine Res. 2007, 27, 227–230. [Google Scholar] [CrossRef]
- Gäbele, E.; Mühlbauer, M.; Paulo, H.; Johann, M.; Meltzer, C.; Leidl, F.; Wodarz, N.; Wiest, R.; Schölmerich, J.; Hellerbrand, C. Analysis of monocyte chemotactic protein-1 gene polymorphism in patients with spontaneous bacterial peritonitis. World J. Gastroenterol. 2009, 15, 5558–5562. [Google Scholar] [CrossRef]
- Clària, J.; Stauber, R.E.; Coenraad, M.J.; Moreau, R.; Jalan, R.; Pavesi, M.; Amorós, À.; Titos, E.; Alcaraz-Quiles, J.; Oettl, K.; et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology 2016, 64, 1249–1264. [Google Scholar]
- Giles, D.A.; Moreno-Fernandez, M.E.; Divanovic, S. IL-17 Axis Driven Inflammation in Non-Alcoholic Fatty Liver Disease Progression. Curr. Drug Targets. 2015, 16, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- Gomes, A.L.; Teijeiro, A.; Burén, S.; Tummala, K.S.; Yilmaz, M.; Waisman, A.; Theurillat, J.-P.; Perna, C.; Djouder, N. Metabolic Inflammation-Associated IL-17A Causes Non-alcoholic Steatohepatitis and Hepatocellular Carcinoma. Cancer Cell 2016, 30, 161–175. [Google Scholar] [CrossRef]
- Ivanov, I.I.; Atarashi, K.; Manel, N.; Brodie, E.L.; Shima, T.; Karaoz, U.; Wei, D.; Goldfarb, K.C.; Santee, C.A.; Lynch, S.V.; et al. Induction of Intestinal Th17 Cells by Segmented Filamentous Bacteria. Cell 2009, 139, 485–498. [Google Scholar] [CrossRef] [Green Version]
- Meng, F.; Wang, K.; Aoyama, T.; Grivennikov, S.I.; Paik, Y.; Scholten, D.; Cong, M.; Iwaisako, K.; Liu, X.; Zhang, M.; et al. Interleukin-17 signaling in inflammatory, Kupffer cells, and hepatic stellate cells exacerbates liver fibrosis in mice. Gastroenterology 2012, 143, 765–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrášek, J.; Bala, S.; Csak, T.; Lippai, R.; Kodys, K.; Menashy, V.; Barrieau, M.; Min, S.-Y.; Kurt-Jones, E.A.; Szabo, G. IL-1 receptor antagonist ameliorates inflammasome-dependent alcoholic steatohepatitis in mice. J. Clin. Investig. 2012, 122, 3476–3489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Sadi, R.; Guo, S.; Ye, D.; Dokladny, K.; Alhmoud, T.; Ereifej, L.; Said, H.M.; Ma, T.Y. Mechanism of IL-1beta modulation of intestinal epithelial barrier involves p38 kinase and activating transcription factor-2 activation. J. Immunol. 2013, 190, 6596–6606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giofre, M.R.; Meduri, G.; Pallio, S.; Calandra, S.; Magnano, A.; Niceforo, D.; Cinquegrani, M.; di Leo, V.; Mazzon, E.; Sturniolo, G.C.; et al. Gastric permeability to sucrose is increased in portal hypertensive gastropathy. Eur. J. Gastroenterol. Hepatol. 2000, 12, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, V.; Leber, B.; Lemesch, S.; Trajanoski, S.; Bashir, M.; Horvath, A.; Tawdrous, M.; Stojakovic, T.; Fauler, G.; Fickert, P.; et al. Lactobacillus casei Shirota Supplementation Does Not Restore Gut Microbiota Composition and Gut Barrier in Metabolic Syndrome: A Randomized Pilot Study. PLoS ONE 2015, 10, e0141399. [Google Scholar] [CrossRef] [Green Version]
- Wagnerberger, S.; Spruss, A.; Kanuri, G.; Stahl, C.; Schröder, M.; Vetter, W.; Bischoff, S.; Bergheim, I. Lactobacillus casei Shirota protects from fructose-induced liver steatosis: A mouse model. J. Nutr. Biochem. 2013, 24, 531–538. [Google Scholar] [CrossRef]
- Horvath, A.; Leber, B.; Schmerboeck, B.; Tawdrous, M.; Zettel, G.; Hartl, A.; Madl, T.; Stryeck, S.; Fuchs, D.; Lemesch, S.; et al. Randomised clinical trial: The effects of a multispecies probiotic vs. placebo on innate immune function, bacterial translocation and gut permeability in patients with cirrhosis. Aliment. Pharmacol. Ther. 2016, 44, 926–935. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Rana, B.; Agrawal, S.; Garg, A.; Chopra, M.; Thumburu, K.K.; Khattri, A.; Malhotra, S.; Duseja, A.; Chawla, Y.K. Probiotic VSL#3 Reduces Liver Disease Severity and Hospitalization in Patients With Cirrhosis: A Randomized, Controlled Trial. Gastroenterology 2014, 147, 1327–1337. [Google Scholar]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; Puri, P.; Sterling, R.K.; Luketic, V.; Stravitz, R.T.; Siddiqui, M.S.; Fuchs, M.; et al. Randomised clinical trial: Lactobacillus GG modulates gut microbiome, metabolome and endotoxemia in patients with cirrhosis. Aliment. Pharmacol. Ther. 2014, 39, 1113–1125. [Google Scholar] [CrossRef]
- Tritto, G.; Bechlis, Z.; Stadlbauer, V.; Davies, N.; Francés, R.; Shah, N.; Mookerjee, R.; Such, J.; Jalan, R.; Stadlbauer, V. Evidence of neutrophil functional defect despite inflammation in stable cirrhosis. J. Hepatol. 2011, 55, 574–581. [Google Scholar] [CrossRef]
- O’Toole, P.W.; Jeffery, I.B. Gut Microbiota and Aging. Science 2015, 350, 1214–1215. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Placebo | LcS | p Value | |
|---|---|---|---|---|
| n | 87 | 43 | 44 | |
| Age (Mean ± SD) | 57.15 ± 8.83 | 58.16 ± 9.18 | 56.16 ± 8.47 | 0.29 |
| Male (n (%)) | 62 (71.26%) | 30 (69.77%) | 32 (72.73%) | 0.76 |
| Etiology of Cirrhosis (n (%)) | ||||
| Alcohol | 45 (51.72%) | 24 (55.81%) | 21 (47.73%) | 0.45 |
| Hepatitis B | 6 (6.90%) | 2 (4.65%) | 4 (9.09%) | 0.41 |
| Hepatitis C | 18 (20.69%) | 12 (27.91%) | 6 (13.64%) | 0.10 |
| NASH | 11 (12.64%) | 3 (6.98%) | 8 (18.18%) | 0.12 |
| Other | 7 (8.05%) | 2 (4.65%) | 5 (11.36%) | 0.25 |
| MELD (Mean ± SD) | 9.02 ± 2.80 | 8.88 ± 2.38 | 9.15 ± 3.17 | 0.66 |
| Child Pugh Class (n (%)) | ||||
| A | 72 (85.71%) | 37 (88.10%) | 35 (83.33%) | 0.56 |
| B | 11 (13.10%) | 5 (11.90%) | 6 (14.29%) | |
| C | 1 (1.19%) | 0 | 1 (2.38%) | |
| History of decompensation event (n (%)) | ||||
| Hepatic encephalopathy | 8 (9.30%) | 5 (11.63%) | 3 (6.98%) | 0.46 |
| Ascites | 33 (37.93%) | 19 (44.19%) | 14 (31.82%) | 0.23 |
| Jaundice | 19 (22.09%) | 10 (23.26%) | 9 (20.93%) | 0.79 |
| Variceal Hemorrhage | 39 (44.83%) | 18 (41.86%) | 21 (47.73%) | 0.58 |
| A | Time Point | Placebo (GMFI) (Median (IQR)) | LcS (GMFI) (Median (IQR)) | p-Value | |
| Constitutive ROS | Day 0 | 35.90 (25.50–51.10) | 35.80 (26.65–48.70) | 0.75 | |
| Month 1 | 36.35 (25.75–64.15) | 33.70 (27.00–47.60) | 0.85 | ||
| Month 6 | 39.20 (26.80–71.00) | 36.70 (29.20–57.00) | 0.87 | ||
| E.coli-induced ROS | Day 0 | 760.00 (498.00–1031.00) | 778.50 (496.50–1177.00) | 0.83 | |
| Month 1 | 744.50 (505.50–1073.50) | 706.00 (526.00–1010.00) | 0.97 | ||
| Month 6 | 604.00 (363.00–965.00) | 719.00 (540.00–1049.00) | 0.26 | ||
| fMLP-induced ROS | Day 0 | 76.40 (58.90–98.60) | 92.05 (59.75–127.50) | 0.22 | |
| Month 1 | 76.35 (51.30–133.50) | 88.10 (49.10–129.00) | 0.64 | ||
| Month 6 | 85.80 (52.00–140.00) | 86.85 (64.80–147.00) | 0.68 | ||
| PMA-induced ROS | Day 0 | 1344.00 (1022.00–1857.00) | 1574.00 (1175.00–2540.00) | 0.19 | |
| Month 1 | 1504.00 (1112.00–2401.00) | 1490.00 (1219.00–2660.00) | 0.19 | ||
| Month 6 | 1207.00 (1014.00–1837.00) | 1493.00 (1228.50–2049.50) | 0.07 | ||
| B | Time Point | Placebo (GMFI) (Median (IQR)) | LcS (GMFI) (Median (IQR)) | p-Value | |
| Constitutive ROS | Day 0 | 45.10 (35.20–74.50) | 44.10 (31.60–81.50) | 0.91 | |
| Month 1 | 50.80 (30.30–83.70) | 42.80 (30.90–101.35) | 0.89 | ||
| Month 6 | 56.20 (35.30–72.40) | 39.30 (29.20–84.20) | 0.69 | ||
| E. coli-induced ROS | Day 0 | 567.00 (316.00–1023.00) | 766.00 (513.00–1093.00) | 0.16 | |
| Month 1 | 553.00 (332.00–754.00) | 669.00 (507.50–1066.50) | 0.29 | ||
| Month 6 | 506.00 (287.00–687.00) | 731.00 (516.00–1067.00) | 0.06 | ||
| fMLP-induced ROS | Day 0 | 85.50 (65.05–131.50) | 123.00 (92.00–146.00) | 0.23 | |
| Month 1 | 86.20 (57.40–149.00) | 100.80 (73.50–174.50) | 0.56 | ||
| Month 6 | 99.10 (73.00–180.00) | 95.30 (65.90–149.00) | 0.73 | ||
| PMA-induced ROS | Day 0 | 1149.00 (833.50–1654.50) | 1460.00 (1179.00–1937.00) | 0.07 | |
| Month 1 | 1170.00 (925.00–2101.00) | 1390.00 (1150.00–2043.50) | 0.25 | ||
| Month 6 | 1168.00 (1014.00–1266.00) | 1403.00 (1214.00–1821.00) | 0.02 | ||
| C | Time Point | Placebo (GMFI) (Median (IQR)) | LcS (GMFI) (Median (IQR)) | p-Value | |
| Phagocytosis | Day 0 | 1556.00 (1070.00–1903.00) | 1737.00 (1246.50–2124.50) | 0.32 | |
| Month 1 | 1562.00 (1042.50–1863.50) | 1782.00 (1405.00–2302.00) | 0.25 | ||
| Month 6 | 1433.00 (866.00–1985.00) | 1626.50 (1062.00–1898.00) | 0.62 |
| A | Placebo (%) | LcS (%) | |||||
| Day 0 | Month 1 | Month 6 | Day 0 | Month 1 | Month 6 | ||
| Spontaneous Bacterial Peritonitis | 0 | 0 | 0 | 0 | 0 | 0 | |
| Lower Respiratory Tract Infection | 2.33 | 2.44 | 0 | 0 | 0 | 0 | |
| Urinary Tract Infection | 0 | 0 | 0 | 2.27 | 0 | 0 | |
| Gastroenteritis | 2.33 | 0 | 0 | 0 | 0 | 0 | |
| Occult sepsis | 0 | 0 | 0 | 0 | 0 | 0 | |
| Other | 6.98 | 2.44 | 5.72 | 0 | 0 | 3.23 | |
| B | Placebo (%) | LcS (%) | |||||
| Day 0 | Month 1 | Month 6 | Day 0 | Month 1 | Month 6 | ||
| Ascites | 2.33 | 4.86 | 5.71 | 6.82 | 5.13 | 6.45 | |
| Variceal Hemorrhage | 0 | 0 | 0 | 0 | 1.27 | 1.52 | |
| Jaundice | 2.33 | 0 | 0 | 4.55 | 2.56 | 0 | |
| Hepatic Encephalopathy | 0 | 0 | 0 | 2.27 | 0 | 0 | |
| Hepatorenal Syndrome | 0 | 0 | 0 | 2.27 | 0 | 0 | |
| Assay | Time Point | Placebo (n, Median (IQR)) | LcS (n, Median (IQR)) | p-Value |
|---|---|---|---|---|
| Lactulose:Rhamnose Ratio | Day 0 | 31, 0.03 (0.02–0.05) | 30, 0.03 (0.02–0.04) | 0.54 |
| Month 1 | 24, 0.03 (0.02–0.04) | 21, 0.03 (0.02–0.04) | 0.99 | |
| Month 6 | 22, 0.03 (0.03–0.03) | 18, 0.03 (0.02–0.05) | 0.76 | |
| Endotoxin (EU/mL) | Day 0 | 28, 0.04 (0.01–0.06) | 28, 0.04 (0.01–0.05) | 0.87 |
| Month 1 | 32, 0.06 (0.02–0.14) | 28, 0.05 (0.01–0.10) | 0.27 | |
| Month 6 | 23, 0.09 (0.01–0.17) | 21, 0.04 (0.01–0.10) | 0.5 | |
| Placebo (n, %) | LcS (n, %) | |||
| Bacterial DNA Positivity | Day 0 | 4 (10.00) | 3 (8.11) | 1 |
| Month 1 | 5 (12.82) | 3 (7.89) | 0.71 | |
| Month 6 | 4 (12.90) | 4 (13.33) | 1 |
| A | Cytokine | Placebo (pg/mL) (Median (IQR)) | LcS (pg/mL) (Median (IQR)) | p-Value | |
| IL-1β | Day 0 | 0.31 (0.26–0.51) | 0.41 (0.20–0.67) | 0.65 | |
| Month 1 | 0.31 (0.22–0.51) | 0.26 (0.12–0.63) | 0.65 | ||
| Month 6 | 0.34 (0.26–0.89 | 0.39 (0.09–0.73) | 0.2 | ||
| IL-2 | Day 0 | 1.14 (1.07–1.17) | 1.14 (1.07–1.17) | 0.8 | |
| Month 1 | 1.14 (1.07–1.17) | 1.17 (1.07–1.17) | 0.87 | ||
| Month 6 | 1.14 (1.07–1.36) | 1.14 (1.07–1.17) | 0.86 | ||
| IL-4 | Day 0 | 0.25 (0.14–0.33) | 0.28 (0.19–0.31) | 0.89 | |
| Month 1 | 0.28 (0.19–0.31) | 0.25 (0.19–0.31) | 0.68 | ||
| Month 6 | 0.25 (0.14–0.59) | 0.25 (0.16–0.30) | 0.94 | ||
| IL-6 | Day 0 | 2.31 (1.19–4.53) | 2.31 (1.35–3.57) | 0.54 | |
| Month 1 | 2.31 (1.89–4.41) | 2.28 (1.55–3.41) | 0.46 | ||
| Month 6 | 2.46 (1.47–4.67) | 2.31 (0.97–2.58) | 0.12 | ||
| IL-8 | Day 0 | 4.77 (3.22–8.50) | 4.96 (3.33–7.20) | 0.86 | |
| Month 1 | 4.72 (2.68–7.48) | 3.63 (2.02–6.95) | 0.27 | ||
| Month 6 | 4.40 (3.11–7.58) | 3.54 (2.55–6.39) | 0.11 | ||
| IL-10 | Day 0 | 1.71 (0.81–2.22) | 1.72 (0.60–2.44) | 0.72 | |
| Month 1 | 2.15 (0.89–3.24) | 2.15 (0.56–4.80) | 0.85 | ||
| Month 6 | 2.00 (0.89–3.84) | 2.15 (0.94–3.26) | 0.75 | ||
| IL12_p70 | Day 0 | 2.19 (1.11–4.74) | 1.77 (1.23–4.10) | 0.73 | |
| Month 1 | 2.68 (1.46–5.00) | 1.94 (1.00–5.14) | 0.25 | ||
| Month 6 | 2.52 (1.47–5.80) | 2.17 (0.88–2.96) | 0.06 | ||
| IL-17A | Day 0 | 4.33 (1.63–8.75) | 3.83 (1.99–5.99) | 0.31 | |
| Month 1 | 4.90 (1.99–11.01) | 4.33 (1.99–6.99) | 0.81 | ||
| Month 6 | 4.14 (1.74–15.78) | 2.29 (1.87–6.36) | 0.21 | ||
| IFN-γ | Day 0 | 21.87 (12.32 407.11) | 25.94 (19.33–79.97) | 0.98 | |
| Month 1 | 21.87 (11.52–54.25) | 52.20 (21.87–407.11) | 0.11 | ||
| Month 6 | 21.87 (15.18–92.89) | 21.87 (15.82-107.54) | 0.85 | ||
| MCP-1 | Day 0 | 11.09 (5.18–18.42) | 12.22 (6.19–18.42) | 0.36 | |
| Month 1 | 11.18 (5.18–21.76) | 7.60 (6.19–24.12) | 0.96 | ||
| Month 6 | 13.70 (7.60–22.50) | 8.11 (4.58–13.75) | 0.02 | ||
| MIP-1b | Day 0 | 21.76 (17.57–32.49) | 26.25 (18.98–33.41) | 0.44 | |
| Month 1 | 27.47 (18.64–40.21) | 23.59 (15.27–29.98) | 0.08 | ||
| Month 6 | 29.69 (22.84–36.26) | 22.63 (17.16–32.66) | 0.19 | ||
| TNF-α | Day 0 | 3.98 (1.59–8.98) | 4.35 (1.59–7.66) | 0.79 | |
| Month 1 | 4.35 (2.11–9.66) | 3.57 (1.18–13.10) | 0.35 | ||
| Month 6 | 4.35 (2.91–9.93) | 4.35 (1.18–12.92) | 0.77 | ||
| B | Cytokine | Placebo (pg/mL) (Median (IQR)) | LcS (pg/mL) (Median (IQR)) | p-Value | |
| IL-1β | Day 0 | 0.29 (0.24–0.49) | 0.26 (0.17–0.57) | 0.47 | |
| Month 1 | 0.26 (0.16–0.34) | 0.22 (0.12–0.63) | 0.88 | ||
| Month 6 | 0.41 (0.31–0.89) | 0.14 (0.07–0.70) | 0.04 | ||
| IL-2 | Day 0 | 1.14 (1.07–1.17) | 1.17 (1.07–1.17) | 0.22 | |
| Month 1 | 1.15 (1.14–1.38) | 1.17 (1.14–1.17) | 0.96 | ||
| Month 6 | 1.14 (1.07–1.50) | 1.15 (1.07–1.17) | 0.70 | ||
| IL-4 | Day 0 | 0.25 (0.14–0.30) | 0.19 (0.12–0.28) | 0.27 | |
| Month 1 | 0.25 (0.15–0.28) | 0.25 (0.25–0.42) | 0.34 | ||
| Month 6 | 0.28 (0.14–0.60) | 0.25 (0.14–0.28) | 0.57 | ||
| IL-6 | Day 0 | 2.31 (0.97–5.89) | 2.31 (1.43–3.73) | 0.73 | |
| Month 1 | 2.31 (2.15–6.38) | 2.31 (1.62–3.41) | 0.29 | ||
| Month 6 | 2.84 (1.90–8.39) | 2.34 (1.20–2.78) | 0.17 | ||
| IL-8 | Day 0 | 4.72 (2.63–9.21) | 5.80 (3.44–9.22) | 0.57 | |
| Month 1 | 4.62 (2.47–8.18) | 4.59 (2.79–8.77) | 0.90 | ||
| Month 6 | 4.96 (3.84–7.58) | 4.03 (2.67–6.85) | 0.45 | ||
| IL-10 | Day 0 | 1.85 (0.99–2.22) | 1.60 (0.60–2.22) | 0.55 | |
| Month 1 | 1.86 (0.58–3.18) | 2.15 (0.56–4.80) | 0.84 | ||
| Month 6 | 2.22 (1.72–4.01) | 2.15 (0.94–4.29) | 0.89 | ||
| IL12_p70 | Day 0 | 2.51 (1.00–5.08) | 1.70 (1.23–3.34) | 0.72 | |
| Month 1 | 3.15 (1.24–10.37) | 2.21 (1.23–4.40) | 0.27 | ||
| Month 6 | 3.34 (2.15–13.47) | 2.29 (1.23–4.36) | 0.12 | ||
| IL-17A | Day 0 | 3.42 (1.63–8.84) | 3.96 (1.18–5.99) | 0.67 | |
| Month 1 | 4.25 (1.99–16.93) | 4.98 (1.99–6.99) | 1.00 | ||
| Month 6 | 1.99 (1.74–18.27) | 3.60 (1.81–7.66) | 0.87 | ||
| IFN-γ | Day 0 | 20.60 (7.38–40.99) | 21.87 (11.52–407.11) | 0.58 | |
| Month 1 | 21.87 (11.09–407.11) | 65.40 (21.87–407.11) | 0.37 | ||
| Month 6 | 21.87 (19.33–50.27) | 28.17 (14.67–273.81) | 0.58 | ||
| MCP-1 | Day 0 | 9.48 (4.35–15.71) | 10.11 (6.19–15.83) | 0.66 | |
| Month 1 | 11.51 (4.96–20.92) | 6.28 (6.19–25.31) | 0.63 | ||
| Month 6 | 16.70 (9.11–24.19) | 6.19 (4.58–13.36) | 0.04 | ||
| MIP-1b | Day 0 | 21.58 (18.16–34.70) | 26.25 (20.76–31.89) | 0.51 | |
| Month 1 | 27.88 (19.01–40.50) | 25.42 (17.62–31.27) | 0.37 | ||
| Month 6 | 24.75 (20.33–33.59) | 28.71 (19.35–35.35) | 0.47 | ||
| TNF-α | Day 0 | 3.45 (1.18–6.66) | 2.91 (1.59–6.74) | 0.84 | |
| Month 1 | 3.30 (1.59–4.91) | 4.35 (2.12–13.10) | 0.60 | ||
| Month 6 | 4.35 (3.06–9.66) | 4.35 (1.18–17.42) | 0.91 | ||
| C | Cytokine | Placebo (pg/mL) (Median (IQR)) | LcS (pg/mL) (Median (IQR)) | p-Value | |
| IL-1β | Day 0 | 0.34 (0.26–0.52) | 0.58 (0.46–0.94) | 0.16 | |
| Month 1 | 0.36 (0.31–0.78) | 0.33 (0.14–0.62) | 0.49 | ||
| Month 6 | 0.31 (0.17–0.52) | 0.53 (0.26–0.73) | 0.54 | ||
| IL-2 | Day 0 | 1.17 (1.14–1.17) | 1.14 (1.10–1.17) | 0.27 | |
| Month 1 | 1.14 (1.07–1.17) | 1.14 (1.07–1.17) | 0.90 | ||
| Month 6 | 1.17 (1.07–1.17) | 1.14 (1.10–1.15) | 0.42 | ||
| IL-4 | Day 0 | 0.28 (0.14–0.36) | 0.30 (0.28–0.52) | 0.20 | |
| Month 1 | 0.28 (0.24–0.36) | 0.25 (0.12–0.30) | 0.16 | ||
| Month 6 | 0.22 (0.14–0.28) | 0.28 (0.21–0.34) | 0.49 | ||
| IL-6 | Day 0 | 2.31 (1.62–3.33) | 1.70 (1.27–3.45) | 0.48 | |
| Month 1 | 2.14 (1.83–3.09) | 2.14 (0.71–3.04) | 0.93 | ||
| Month 6 | 2.31 (1.20–3.97) | 1.82 (0.82–2.45) | 0.36 | ||
| IL-8 | Day 0 | 4.77 (3.63–6.24) | 3.85 (2.26–4.63) | 0.17 | |
| Month 1 | 4.83 (2.68–6.82) | 2.82 (1.57–4.77) | 0.06 | ||
| Month 6 | 3.92 (3.00–6.02) | 2.96 (1.88–4.21) | 0.15 | ||
| IL-10 | Day 0 | 1.69 (0.72–2.22) | 2.07 (0.72–2.49) | 0.93 | |
| Month 1 | 2.22 (1.15–3.24) | 2.15 (0.98–4.22) | 0.83 | ||
| Month 6 | 1.15 (0.87–3.54) | 2.07 (0.73–2.70) | 0.98 | ||
| IL12_p70 | Day 0 | 1.94 (1.23–2.68) | 2.81 (0.63–4.49) | 1.00 | |
| Month 1 | 2.68 (1.46–4.49) | 1.68 (0.66–5.53) | 0.68 | ||
| Month 6 | 1.70 (1.47–4.74) | 1.65 (0.59–2.62) | 0.34 | ||
| IL-17A | Day 0 | 5.80 (1.99–8.75) | 3.18 (1.99–6.00) | 0.28 | |
| Month 1 | 5.25 (1.99–9.12) | 3.78 (1.99–7.09) | 0.82 | ||
| Month 6 | 6.91 (2.25–9.83) | 1.99 (1.87–2.64) | 0.02 | ||
| IFN-γ | Day 0 | 66.07 (21.87–407.11) | 27.54 (21.87–59.62) | 0.36 | |
| Month 1 | 21.87 (11.52–47.15) | 22.41 (20.27–407.11) | 0.27 | ||
| Month 6 | 49.69 (12.32–407.11) | 21.87 (15.82–41.06) | 0.50 | ||
| MCP-1 | Day 0 | 13.14 (6.19–18.42) | 15.83 (10.29–25.70) | 0.39 | |
| Month 1 | 11.18 (5.90–21.76) | 7.60 (4.29–13.93) | 0.59 | ||
| Month 6 | 12.77 (7.60–17.57) | 9.61 (4.50–14.50) | 0.31 | ||
| MIP-1b | Day 0 | 21.92 (17.57–28.10) | 24.14 (18.16–33.47) | 0.79 | |
| Month 1 | 27.47 (17.38–40.21) | 21.82 (14.19–24.41) | 0.06 | ||
| Month 6 | 33.84 (29.85–36.82) | 18.35 (16.28–22.63) | 0.04 | ||
| TNF-α | Day 0 | 3.98 (2.25–11.72) | 4.63 (4.30–13.65) | 0.38 | |
| Month 1 | 6.57 (3.52–10.38) | 2.68 (0.96–12.58) | 0.14 | ||
| Month 6 | 4.35 (2.91–9.93) | 4.17 (1.65–10.40) | 0.71 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macnaughtan, J.; Figorilli, F.; García-López, E.; Lu, H.; Jones, H.; Sawhney, R.; Suzuki, K.; Fairclough, S.; Marsden, J.; Moratalla, A.; et al. A Double-Blind, Randomized Placebo-Controlled Trial of Probiotic Lactobacillus casei Shirota in Stable Cirrhotic Patients. Nutrients 2020, 12, 1651. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061651
Macnaughtan J, Figorilli F, García-López E, Lu H, Jones H, Sawhney R, Suzuki K, Fairclough S, Marsden J, Moratalla A, et al. A Double-Blind, Randomized Placebo-Controlled Trial of Probiotic Lactobacillus casei Shirota in Stable Cirrhotic Patients. Nutrients. 2020; 12(6):1651. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061651
Chicago/Turabian StyleMacnaughtan, Jane, Francesco Figorilli, Elisabet García-López, Haw Lu, Helen Jones, Rohit Sawhney, Kaori Suzuki, Sarah Fairclough, Joanne Marsden, Alba Moratalla, and et al. 2020. "A Double-Blind, Randomized Placebo-Controlled Trial of Probiotic Lactobacillus casei Shirota in Stable Cirrhotic Patients" Nutrients 12, no. 6: 1651. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061651