Associations of Serum Retinol and α-Tocopherol Levels with Uric Acid Concentrations: Analysis of a Population-Based, Nationally Representative Sample


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection and Measurement
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of Study Participants
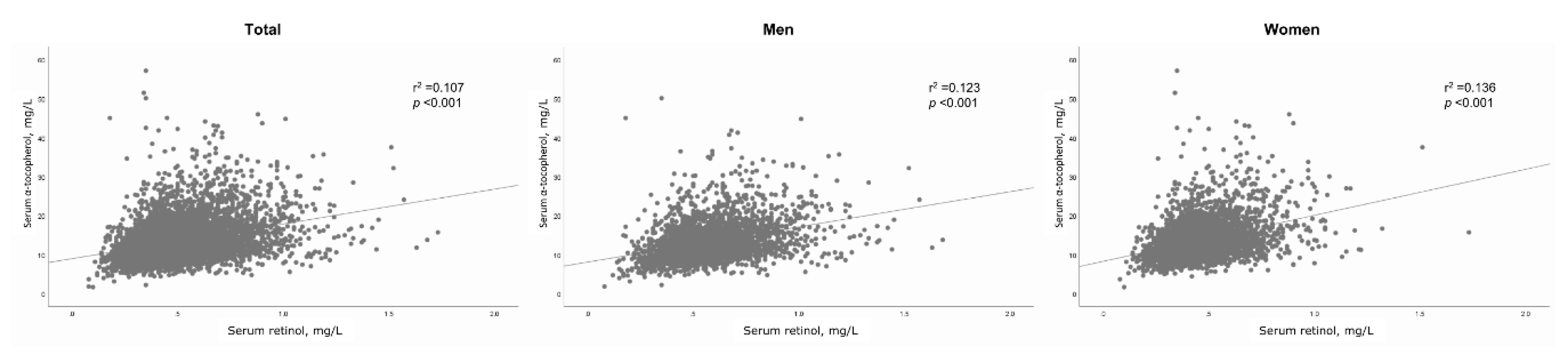
3.2. Correlation between Serum Retinol and α-Tocopherol
3.3. Association of Serum Retinol and α-Tocopherol Concentration with Uric Acid Levels
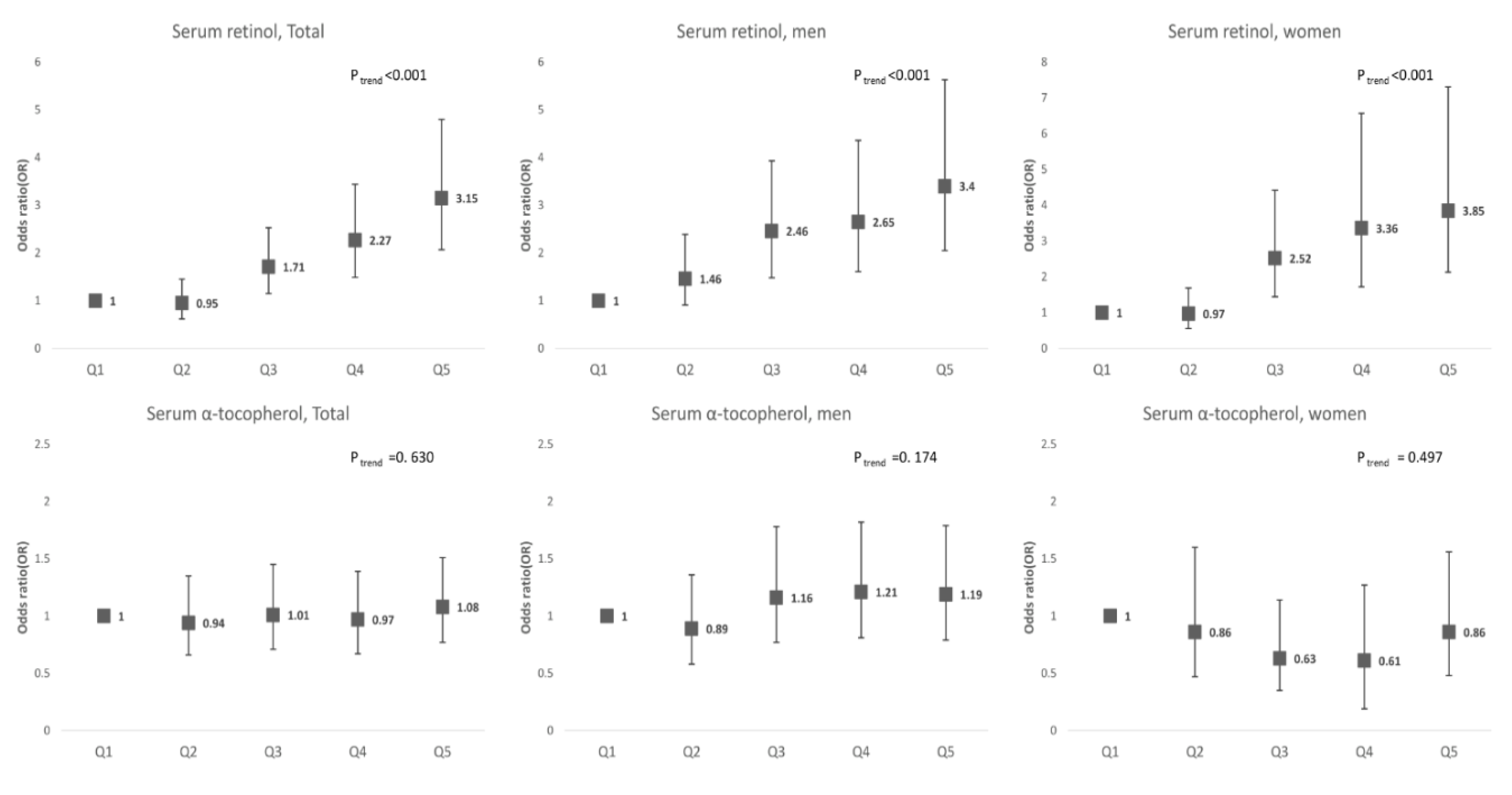
3.4. Association between Serum Retinol and α-Tocopherol Levels and Hyperuricemia
3.5. Interactive Effects of Dietary Supplements and Serum Retinol and α-Tocopherol on Hyperuricemia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kuo, C.-F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649. [Google Scholar] [CrossRef]
- Dehghan, A.; Van Hoek, M.; Sijbrands, E.J.; Hofman, A.; Witteman, J.C. High serum uric acid as a novel risk factor for type 2 diabetes. Diabetes Care 2008, 31, 361–362. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Kang, D.-H.; Feig, D.; Kivlighn, S.; Kanellis, J.; Watanabe, S.; Tuttle, K.R.; Rodriguez-Iturbe, B.; Herrera-Acosta, J.; Mazzali, M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 2003, 41, 1183–1190. [Google Scholar] [CrossRef] [Green Version]
- Onat, A.; Uyarel, H.; Hergenc, G.; Karabulut, A.; Albayrak, S.; Sarı, I.; Yazıcı, M.; Keleş, I. Serum uric acid is a determinant of metabolic syndrome in a population-based study. Am. J. Hypertens. 2006, 19, 1055–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madero, M.; Sarnak, M.J.; Wang, X.; Greene, T.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Menon, V. Uric acid and long-term outcomes in CKD. Am. J. Kidney Dis. 2009, 53, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afsar, B.; Elsurer, R.; Ozdemir, F.N.; Sezer, S. Uric acid and nocturnal nondipping in hypertensive patients with normal renal function. J. Nephrol. 2008, 21, 406–411. [Google Scholar]
- Maloberti, A.; Giannattasio, C.; Bombelli, M.; Desideri, G.; Cicero, A.; Muiesan, M.; Rosei, E.; Salvetti, M.; Ungar, A.; Rivasi, G. Hyperuricemia and risk of cardiovascular outcomes: The experience of the URRAH (Uric Acid Right for Heart Health) project. High Blood Press. Cardiovasc. Prev. 2020, 21, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Curhan, G. Beer, liquor, and wine consumption and serum uric acid level: The Third National Health and Nutrition Examination Survey. Arthritis Rheum 2004, 51, 1023–1029. [Google Scholar] [CrossRef]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.; Curhan, G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N. Engl. J. Med. 2004, 350, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Ichida, K.; Matsuo, H.; Takada, T.; Nakayama, A.; Murakami, K.; Shimizu, T.; Yamanashi, Y.; Kasuga, H.; Nakashima, H.; Nakamura, T. Decreased extra-renal urate excretion is a common cause of hyperuricemia. Nat. Commun. 2012, 3, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, M.B.; Thakkar, S.; Hix, J.K.; Bhandarkar, N.D.; Wong, A.; Schreiber, M.J. Pathophysiology, clinical consequences, and treatment of tumor lysis syndrome. Am. J. Med. 2004, 116, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef]
- Trifiro, G.; Morabito, P.; Cavagna, L.; Ferrajolo, C.; Pecchioli, S.; Simonetti, M.; Bianchini, E.; Medea, G.; Cricelli, C.; Caputi, A.P.; et al. Epidemiology of gout and hyperuricaemia in Italy during the years 2005–2009: A nationwide population-based study. Ann. Rheum. Dis. 2013, 72, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kang, J.; Kim, G.-T. Prevalence of hyperuricemia and its associated factors in the general Korean population: An analysis of a population-based nationally representative sample. Clin. Rheumatol. 2018, 37, 2529–2538. [Google Scholar] [CrossRef] [PubMed]
- Shils, M.E.; Shike, M. Modern Nutrition in Health and Disease; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch. Ophthalmol. 2001, 119, 1417–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huiming, Y.; Chaomin, W.; Meng, M. Vitamin A for treating measles in children. Cochrane Database Syst. Rev. 2005, 4, CD001479. [Google Scholar]
- Kang, M.; Kim, D.; Baek, Y.; Moon, S.; Jung, H.; Song, Y.; Paik, H. Dietary supplement use and its effect on nutrient intake in Korean adult population in the Korea National Health and Nutrition Examination Survey IV (2007–2009) data. Eur. J. Clin. Nutr. 2014, 68, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Penniston, K.L.; Tanumihardjo, S.A. The acute and chronic toxic effects of vitamin A. Am. J. Clin. Nutr. 2006, 83, 191–201. [Google Scholar] [CrossRef]
- Solak, B.; Erdem, T.; Solak, Y. Isotretinoin use for acne vulgaris is associated with increased serum uric acid levels. J. Dermatol. Treat. 2017, 28, 82–85. [Google Scholar] [CrossRef]
- Vanhooteghem, O.; André, J.; Pochet, J.; Demaubeuge, J.; Song, M. Occurrence of gouty tophi following acitretin therapy. Clin. Exp. Derm. 1998, 23, 274–276. [Google Scholar] [CrossRef]
- Choi, W.J.; Ford, E.S.; Curhan, G.; Rankin, J.I.; Choi, H.K. Independent association of serum retinol and β-carotene levels with hyperuricemia: A national population study. Arthritis Care Res. (Hoboken) 2012, 64, 389–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.S.; Choi, H.K. Associations between concentrations of uric acid with concentrations of vitamin A and beta-carotene among adults in the United States. Nutr. Res. 2013, 33, 995–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beydoun, M.A.; Canas, J.A.; Beydoun, H.A.; Chen, X.; Shroff, M.R.; Zonderman, A.B. Serum antioxidant concentrations and metabolic syndrome are associated among US adolescents in recent national surveys. J. Nutr. 2012, 142, 1693–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinonen, O.P.; Albanes, D.; Virtamo, J.; Taylor, P.R.; Huttunen, J.K.; Hartman, A.M.; Haapakoski, J.; Malila, N.; Rautalahti, M.; Ripatti, S.; et al. Prostate cancer and supplementation with alpha-tocopherol and beta-carotene: Incidence and mortality in a controlled trial. J. Natl. Cancer Inst. 1998, 90, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. Jama 2007, 297, 842–857. [Google Scholar] [CrossRef]
- Sesso, H.D.; Buring, J.E.; Christen, W.G.; Kurth, T.; Belanger, C.; MacFadyen, J.; Bubes, V.; Manson, J.E.; Glynn, R.J.; Gaziano, J.M. Vitamins E and C in the prevention of cardiovascular disease in men: The Physicians’ Health Study II randomized controlled trial. Jama 2008, 300, 2123–2133. [Google Scholar] [CrossRef] [Green Version]
- Seifi, B.; Kadkhodaee, M.; Zahmatkesh, M. Effect of vitamin E therapy on serum uric acid in DOCA-salt-treated rats. Acta Physiol. Hung. 2011, 98, 214–220. [Google Scholar] [CrossRef]
- Kuroda, M.; Asaka, S.; Tofuku, Y.; Takeda, R. Serum antioxidant activity in uremic patients. Nephron 1985, 41, 293–298. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, T.; Bull, F. Development of the world health organization global physical activity questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Feskanich, D.; Singh, V.; Willett, W.C.; Colditz, G.A. Vitamin A intake and hip fractures among postmenopausal women. Jama 2002, 287, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Michaëlsson, K.; Lithell, H.; Vessby, B.; Melhus, H. Serum retinol levels and the risk of fracture. N. Engl. J. Med. 2003, 348, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Lee, J.S.; Shin, A.; Kang, M.H.; Shin, D.S.; Chung, H.R.; Kim, W.K. Sociodemographic and lifestyle factors are associated with the use of dietary supplements in a Korean population. J. Epidemiol. 2010, 20, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Fulgoni, V.L., 3rd; Keast, D.R.; Bailey, R.L.; Dwyer, J. Foods, fortificants, and supplements: Where do Americans get their nutrients? J. Nutr. 2011, 141, 1847–1854. [Google Scholar] [CrossRef]
- Hak, A.E.; Choi, H.K. Menopause, postmenopausal hormone use and serum uric acid levels in US women–the Third National Health and Nutrition Examination Survey. Arthritis Res. 2008, 10, R116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taibi, G.; Nicotra, C.M. Xanthine oxidase catalyzes the oxidation of retinol. J. Enzym. Inhib. Med. Chem. 2007, 22, 471–476. [Google Scholar] [CrossRef]
- Mawson, A. Hypervitaminosis A toxicity and gout. Lancet (Lond. Engl.) 1984, 1, 1181. [Google Scholar] [CrossRef]
- Tungtrongchitr, R.; Changbumrung, S.; Tungtrongchitr, A.; Schelp, F.P. The relationships between anthropometric measurements, serum vitamin A and E concentrations and lipid profiles in overweight and obese subjects. Asia Pac. J. Clin. Nutr. 2003, 12, 73–79. [Google Scholar]
- Kim, J.-W.; Kwak, S.G.; Lee, H.; Kim, S.-K.; Choe, J.-Y.; Park, S.-H. Prevalence and incidence of gout in Korea: Data from the national health claims database 2007–2015. Rheumatol. Int. 2017, 37, 1499–1506. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A. Vitamin A: Biomarkers of nutrition for development. Am. J. Clin. Nutr. 2011, 94, 658S–665S. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total | Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Hyperuricemia (N = 665) | No Hyperuricemia (N = 5358) | p-Value | Hyperuricemia (N = 472) | No Hyperuricemia (N = 2250) | p-Value | Hyperuricemia (N = 193) | No Hyperuricemia (N = 3108) | p-Value | |
| Age, mean (SE) | 42.4(0.7) | 45.9(0.3) | <0.001 | 40.2 (0.7) | 45.8 (0.4) | <0.001 | 49.7 (1.6) | 46.0 (0.3) | 0.022 |
| Area of residence, % (SE) | 0.619 | 0.838 | 0.318 | ||||||
| Urban | 85.6 (2.0) | 86.3 (1.4) | 86.3 (2.2) | 86.6 (1.5) | 83.2 (3.4) | 86.1 (1.5) | |||
| Rural | 14.4 (2.0) | 13.7 (1.4) | 13.7 (2.2) | 13.4 (1.5) | 16.8 (3.4) | 13.9 (1.5) | |||
| Education, % (SE) | 0.061 | 0.028 | 0.040 | ||||||
| Elementary school | 8.5 (1.1) | 12.4 (0.5) | 4.4 (0.8) | 9.1 (0.6) | 22.7 (3.3) | 15.5 (0.7) | |||
| Middle school | 8.3 (1.1) | 8.3 (0.4) | 7.5 (1.3) | 7.5 (0.6) | 11.0 (2.2) | 9.0 (0.5) | |||
| High school | 38.7 (2.4) | 35.5 (0.8) | 39.8 (2.8) | 36.9 (1.2) | 34.9 (4.0) | 34.3 (1.0) | |||
| University or above | 44.5 (2.5) | 43.7 (1.0) | 48.2. (2.9) | 46.6 (1.3) | 31.5 (4.4) | 41.2 (1.1) | |||
| Smoking status * | 0.001 | 0.413 | 0.016 | ||||||
| Non-smokers | 44.4 (2.3) | 60.5 (0.7) | 32.3 (2.6) | 29.4 (1.1) | 86.4 (2.7) | 89.0 (0.7) | |||
| Past smokers | 23.8 (1.9) | 18.5 (0.6) | 29.8 (2.3) | 33.1 (1.1) | 2.9 (1.1) | 5.1 (0.5) | |||
| Current smokers | 31.8 (2.1) | 21.0 (0.7) | 37.9 (2.6) | 37.5 (1.3) | 10.7 (2.6) | 5.8 (0.5) | |||
| Alcohol consumption, % (SE) † | 0.001 | 0.090 | 0.171 | ||||||
| None | 34.1 (2.1) | 45.7 (0.8) | 25.2 (2.3) | 31.0 (1.1) | 64.9 (3.9) | 59.2 (1.1) | |||
| <1/week | 33.6 (2.3) | 32.7 (0.8) | 36.6 (2.8) | 35.1 (1.2) | 23.2 (3.8) | 30.6 (1.0) | |||
| ≥1/week | 32.3 (2.2) | 21.6 (0.7) | 38.2 (2.6) | 34.0 (1.2) | 11.9 (2.5) | 10.2 (0.7) | |||
| Physical activity, % (SE) ‡ | 0.368 | 0.897 | 0.657 | ||||||
| No | 49.4 (2.3) | 51.5 (0.9) | 48.3 (2.7) | 47.9 (1.2) | 53.0 (4.2) | 54.8 (1.1) | |||
| Yes | 50.6 (2.3) | 48.5 (0.9) | 51.7 (2.7) | 52.1 (1.2) | 47.0 (4.2) | 45.2 (1.1) | |||
| Body mass index, % (SE) | 26.2 (0.2) | 23.6 (0.1) | <0.001 | 26.1 (0.2) | 24.2 (0.1) | <0.001 | 26.3 (0.4) | 23.1 (0.1) | <0.001 |
| Systolic blood pressure, mmHg | 121.6 (0.7) | 116.4 (0.3) | <0.001 | 122.1 (0.7) | 119.1 (0.4) | <0.001 | 120.1 (2.0) | 114.0 (0.3) | 0.002 |
| Diastolic blood pressure, mmHg | 79.9 (0.5) | 75.6 (0.2) | <0.001 | 81.2 (0.5) | 78.0 (0.3) | <0.001 | 75.3 (0.9) | 73.4 (0.2) | 0.037 |
| GFR, mL/min/1.73m2 | 94.1 (0.9) | 99.6 (0.3) | <0.001 | 95.4 (0.9) | 96.8 (0.4) | 0.161 | 89.7 (2.0) | 102.1 (0.3) | <0.001 |
| hs-CRP, mg/L | |||||||||
| Median (IQR) | 0.8 (0.5,1.6) | 0.5 (0.3,0.98) | <0.001 | 0.78 (0.48,1.53) | 0.55 (0.35,1.04) | <0.001 | 0.93 (0.6,1.78) | 0.46 (0.3,0.89) | <0.001 |
| Uric acid, mg/dL | 7.64 (0.04) | 4.86 (0.02) | <0.001 | 7.89 (0.04) | 5.50 (0.02) | <0.001 | 6.74 (0.05) | 4.27 (0.02) | <0.001 |
| Serum retinol, mg/L | 0.61 (0.01) | 0.51 (0.01) | <0.001 | 0.63 (0.01) | 0.57 (0.01) | <0.001 | 0.54 (0.02) | 0.46 (0.01) | <0.001 |
| Serum α-tocopherol, mg/L | 14.1 (0.3) | 13.3 (0.1) | 0.006 | 14.0 (0.3) | 13.1 (0.1) | 0.008 | 14.3 (0.4) | 13.5 (0.1) | 0.074 |
| Q1 | Q2 | Q3 | Q4 | Q5 | ptrend * | |
|---|---|---|---|---|---|---|
| Total | ||||||
| Retinol | ||||||
| Model 1 * | 4.83 (4.76,4.91) | 5.03 (4.95,5.11) | 5.15 (5.07,5.22) | 5.33 (5.25,5.41) | 5.56 (5.47,5.65) | <0.001 |
| Model 2 † | 4.93 (4.87,5.00) | 5.06 (4.99,5.13) | 5.16 (5.09,5.23) | 5.30 (5.23,5.38) | 5.47 (5.38,5.55) | <0.001 |
| Model 3 ‡ | 4.90 (4.81,4.99) | 5.04 (4.96,5.13) | 5.17 (5.08,5.26) | 5.31 (5.23,5.40) | 5.49 (5.39,5.59) | <0.001 |
| Model 4 § | 4.89 (4.80,4.99) | 5.04 (4.95,5.13) | 5.17 (5.08,5.26) | 5.31 (5.23,5.40) | 5.49 (5.39,5.59) | <0.001 |
| α-tocopherol | ||||||
| Model 1 * | 5.04 (4.96,5.11) | 5.1 (5.02,5.17) | 5.17 (5.09.5.25) | 5.30 (5.21,5.38) | 5.31 (5.23,5.39) | <0.001 |
| Model 2 † | 5.10 (5.02,5.17) | 5.13 (5.07,5.20) | 5.18 (5.11,5.25) | 5.26 (5.18,5.34) | 5.26 (5.18,5.33) | <0.001 |
| Model 3 ‡ | 5.13 (5.04,5.22) | 5.17 (5.08,5.25) | 5.21 (5.12,5.30) | 5.28 (5.19,5.38) | 5.26 (5.17,5.36) | 0.002 |
| Model 4 § | 5.19 (5.10,5.28) | 5.17 (5.09,5.25) | 5.19 (5.10,5.28) | 5.23 (5.13,5.32) | 5.14 (5.05,5.24) | 0.849 |
| Men | ||||||
| Retinol | ||||||
| Model 1 * | 5.61 (5.50,5.73) | 5.79 (5.67,5.91) | 6.01 (5.89,6.13) | 6.09 (5.96,6.22) | 6.27 (6.14,6.40) | <0.001 |
| Model 2 † | 5.70 (5.59,5.80) | 5.83 (5.71,.594) | 6.02 (5.91,6.12) | 6.03 (5.90,6.15) | 6.19 (6.06,6.32) | <0.001 |
| Model 3 ‡ | 5.67 (5.54,5.80) | 5.85 (5.71,5.99) | 6.05 (5.92,6.19) | 6.08 (5.94,6.23) | 6.24 (6.09,6.39) | <0.001 |
| Model 4 § | 5.67 (5.53,5.80) | 5.85 (5.71,5.99) | 6.05 (5.92,6.19) | 6.08 (5.94,6.23) | 6.24 (6.09,6.40) | <0.001 |
| α-tocopherol | ||||||
| Model 1 * | 5.78 (5.66,5.90) | 5.84 (5.73,5.96) | 5.98 (5.86,6.10) | 6.09 (5.95,6.22) | 6.05 (5.91,6.18) | <0.001 |
| Model 2 † | 5.86 (5.75,5.98) | 5.87 (5.77,5.98) | 5.97 (5.86,6.08) | 6.03 (5.90,6.17) | 5.99 (5.86,6.11) | 0.034 |
| Model 3 ‡ | 5.90 (5.76,6.04) | 5.91 (5.78,6.03) | 5.99 (5.86,6.12) | 6.06 (5.90,6.21) | 6.00 (5.85,6.15) | 0.097 |
| Model 4 § | 6.00 (5.86,6.15) | 5.93 (5.81,6.06) | 6.00 (5.87,6.13) | 6.02 (5.87,6.17) | 5.90 (5.75,6.06) | 0.549 |
| Women | ||||||
| Retinol | ||||||
| Model 1 * | 4.25 (4.19,4.30) | 4.38 (4.30,4.45) | 4.59 (4.49,4.70) | 4.74 (4.60,4.87) | 4.96 (4.77,5.14) | <0.001 |
| Model 2 † | 4.28 (4.23,4.33) | 4.37 (4.30,4.45) | 4.56 (4.46,4.66) | 4.68 (4.55,4.80) | 4.83 (4.67,4.99) | <0.001 |
| Model 3 ‡ | 4.35 (4.24,4.45) | 4.44 (4.34,3.54) | 4.63 (4.51,4.76) | 4.75 (4.61,4.88) | 4.89 (4.72,5.06) | <0.001 |
| Model 4 § | 4.35 (4.25,4.45) | 4.45 (4.34,4.55) | 4.63 (4.51,4.76) | 4.75 (4.61,4.88) | 4.89 (4.72,5.07) | <0.001 |
| α-tocopherol | ||||||
| Model 1 * | 4.30 (4.21,4.39) | 4.36 (4.27,4.44) | 4.38 (4.30,4.47) | 4.48 (4.39,4.57) | 4.56 (4.47,4.65) | <0.001 |
| Model 2 † | 4.33 (4.25,4.41) | 4.36 (4.28,4.45) | 4.41 (4.33,4.49) | 4.46 (4.37,4.54) | 4.51 (4.43,4.60) | 0.001 |
| Model 3 ‡ | 4.45 (4.33,4.56) | 4.50 (4.39,4.61) | 4.53 (4.41,4.64) | 4.57 (4.46,4.68) | 4.61 (4.49,4.72) | 0.006 |
| Model 4 § | 4.46 (4.35,4.57) | 4.48 (4.37,4.59) | 4.48 (4.36,4.60) | 4.49 (4.38,4.60) | 4.47 (4.34,4.59) | 0.996 |
| Q1 | Q2 | Q3 | Q4 | Q5 | ptrend * | pinteraction† | |
|---|---|---|---|---|---|---|---|
| Total | |||||||
| Retinol | |||||||
| Dietary supplements | Reference | 0.72 (0.37,1.39) | 1.17 (0.59,2.33) | 1.91 (0.97,3.73) | 2.24 (1.13,4.45) | <0.001 | 0.617 |
| No dietary supplements | Reference | 1.13 (0.66,1.96) | 2.13 (1.26,3.61) | 2.48 (1.42,4.31) | 3.89 (2.25,6.74) | <0.001 | |
| α-tocopherol | |||||||
| Dietary supplements | Reference | 1.02 (0.55,1.90) | 1.01 (0.55,1.86) | 0.71 (0.38,1.32) | 1.29 (0.72,2.30) | 0.622 | 0.295 |
| No dietary supplements | Reference | 0.90 (0.58,1.40) | 1.04 (0.67,1.61) | 1.18 (0.76,1.85) | 1.00 (0.65,1.53) | 0.565 | |
| Men | |||||||
| Retinol | |||||||
| Dietary supplements | Reference | 1.02 (0.38,2.70) | 2.34 (0.91,6.00) | 1.68 (0.65,4.43) | 2.31 (0.90,5.95) | 0.033 | 0.604 |
| No dietary supplements | Reference | 1.67 (0.96,2.92) | 2.37 (1.37,4.10) | 3.16 (1.78,5.62) | 3.93 (2.16,7.14) | <0.001 | |
| α-tocopherol | |||||||
| Dietary supplements | Reference | 0.67 (0.30,1.51) | 0.98 (0.44,2.18) | 0.98 (0.47,2.08) | 1.31 (0.62,2.77) | 0.247 | 0.764 |
| No dietary supplements | Reference | 0.96 (0.57,1.61) | 1.24 (0.73,2.10) | 1.33 (0.78,2.26) | 1.09 (0.65,1.82) | 0.373 | |
| Women | |||||||
| Retinol | |||||||
| Dietary supplements | Reference | 0.37 (0.15,0.96) | 1.26 (0.53,3.00) | 4.36 (1.87,10.15) | 5.61 (2.06,15.32) | <0.001 | 0.012 |
| No dietary supplements | Reference | 1.46 (0.71,2.98) | 3.77 (1.78,7.97) | 2.19 (0.79,6.09) | 3.45 (1.53,7.75) | 0.001 | |
| α-tocopherol | |||||||
| Dietary supplements | Reference | 0.85 (0.30,2.40) | 0.61 (0.22,1.70) | 0.28 (0.08,1.01) | 0.66 (0.22,1.97) | 0.255 | 0.618 |
| No dietary supplements | Reference | 0.79 (0.37,1.68) | 0.64 (0.30,1.38) | 0.82 (0.35,1.92) | 0.90 (0.43,1.88) | 0.837 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Choi, J.H.; Kang, J.; Kim, G.-T.; Lee, S.-G. Associations of Serum Retinol and α-Tocopherol Levels with Uric Acid Concentrations: Analysis of a Population-Based, Nationally Representative Sample. Nutrients 2020, 12, 1797. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061797
Kim Y, Choi JH, Kang J, Kim G-T, Lee S-G. Associations of Serum Retinol and α-Tocopherol Levels with Uric Acid Concentrations: Analysis of a Population-Based, Nationally Representative Sample. Nutrients. 2020; 12(6):1797. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061797
Chicago/Turabian StyleKim, Yunkyung, Jung Hee Choi, Jihun Kang, Geun-Tae Kim, and Seung-Geun Lee. 2020. "Associations of Serum Retinol and α-Tocopherol Levels with Uric Acid Concentrations: Analysis of a Population-Based, Nationally Representative Sample" Nutrients 12, no. 6: 1797. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061797