Baseline HOMA IR and Circulating FGF21 Levels Predict NAFLD Improvement in Patients Undergoing a Low Carbohydrate Dietary Intervention for Weight Loss: A Prospective Observational Pilot Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Dietary Intervention
2.3. Anthropometric Assessment
2.4. Body Composition Assessment
2.5. Blood and Urine Chemistry
2.6. Data Management and Statistical Methods
2.7. Ethical Aspects
3. Results
3.1. Clinical Features
3.2. Change in Body Mass and Composition
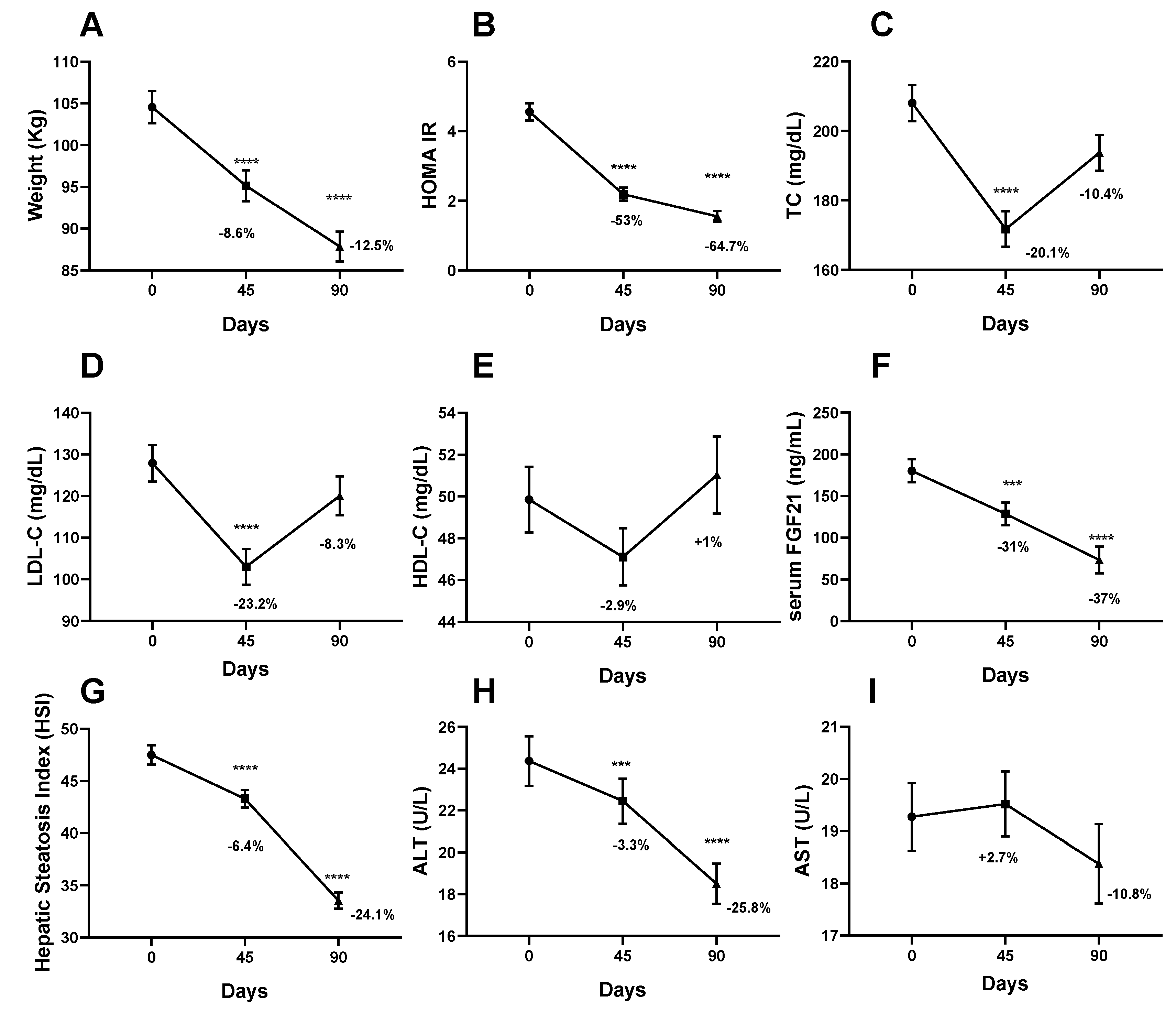
3.3. Change in Biochemical Parameters
3.4. NAFLD Improvement and Its Predictors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Meex, R.C.R.; Watt, M.J. Hepatokines: Linking nonalcoholic fatty liver disease and insulin resistance. Nat. Rev. Endocrinol. 2017, 13, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, G.; Savastano, S.; Colao, A. Hepatic steatosis, low-grade chronic inflammation and hormone/growth factor/adipokine imbalance. World J. Gastroenterol. 2010, 16, 4773–4783. [Google Scholar] [CrossRef] [PubMed]
- Shulman, G.I. Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. N. Engl. J. Med. 2014, 371, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A.; Basta, G. Ectopic fat and cardiovascular disease: What is the link? Nutr. Metab. Cardiovasc. Dis. 2010, 20, 481–490. [Google Scholar] [CrossRef]
- Lee, M.; Choh, A.C.; Demerath, E.W.; Towne, B.; Siervogel, R.M.; Czerwinski, S.A. Associations between trunk, leg and total body adiposity with arterial stiffness. Am. J. Hypertens 2012, 25, 1131–1137. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, A.; Hamilton, D.J.; Deng, T. Epicardial Fat in the Maintenance of Cardiovascular Health. Methodist. Debakey Cardiovasc. J. 2017, 13, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Tchernof, A.; Despres, J.P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef]
- Chen, Z.; Yu, R.; Xiong, Y.; Du, F.; Zhu, S. A vicious circle between insulin resistance and inflammation in nonalcoholic fatty liver disease. Lipids Health Dis. 2017, 16, 203. [Google Scholar] [CrossRef] [Green Version]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- Watanabe, M.; Risi, R.; De Giorgi, F.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Lubrano, C.; Lenzi, A.; Gnessi, L. Obesity treatment within the Italian national healthcare system tertiary care centers: What can we learn? Eat Weight Disord. 2020. [Google Scholar] [CrossRef]
- Mariani, S.; Fiore, D.; Varone, L.; Basciani, S.; Persichetti, A.; Watanabe, M.; Saponara, M.; Spera, G.; Moretti, C.; Gnessi, L. Obstructive sleep apnea and bone mineral density in obese patients. Diabetes Metab. Syndr. Obes. Targets Ther. 2012, 5, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.K.; Dubey, P.; Cistola, D.P.; Reddy, S.Y. Association Between Obesity and Cardiovascular Outcomes: Updated Evidence from Meta-analysis Studies. Curr. Cardiol. Rep. 2020, 22, 25. [Google Scholar] [CrossRef]
- Okamura, T.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: A population-based longitudinal study. Int. J. Obes. (Lond.) 2019, 43, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Palermo, A.; Tuccinardi, D.; Defeudis, G.; Watanabe, M.; D’Onofrio, L.; Lauria, A.P.; Napoli, N.; Pozzilli, P.; Manfrini, S. BMI and BMD: The potential interplay between obesity and bone fragility. Int. J. Environ. Res. Public Health 2016, 13, 544. [Google Scholar] [CrossRef] [Green Version]
- Arboleda, S.; Vargas, M.; Losada, S.; Pinto, A. Review of obesity and periodontitis: An epidemiological view. Br. Dent J. 2019, 227, 235–239. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- Caussy, C.; Chen, J.; Alquiraish, M.H.; Cepin, S.; Nguyen, P.; Hernandez, C.; Yin, M.; Bettencourt, R.; Cachay, E.R.; Jayakumar, S.; et al. Association Between Obesity and Discordance in Fibrosis Stage Determination by Magnetic Resonance vs Transient Elastography in Patients With Nonalcoholic Liver Disease. Clin. Gastroenterol. Hepatol. 2018, 16, 1974–1982.e7. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Stern, C.; Castera, L. Non-invasive diagnosis of hepatic steatosis. Hepatol. Int. 2017, 11, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Gangitano, E.; Francomano, D.; Addessi, E.; Toscano, R.; Costantini, D.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Spera, G.; et al. Mangosteen extract shows a potent insulin sensitizing effect in obese female patients: A prospective randomized controlled pilot study. Nutrients 2018, 10, 586. [Google Scholar] [CrossRef] [Green Version]
- Sumida, Y.; Yoneda, M. Current and future pharmacological therapies for NAFLD/NASH. J. Gastroenterol. 2018, 53, 362–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Colletti, A.; Bellentani, S. Nutraceutical Approach to Non-Alcoholic Fatty Liver Disease (NAFLD): The Available Clinical Evidence. Nutrients 2018, 10, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, M.; Tozzi, R.; Risi, R.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Spera, G.; Lubrano, C.; Gnessi, L. Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease: A comprehensive review of the literature. Obes. Rev. 2020. [Google Scholar] [CrossRef] [Green Version]
- Luukkonen, P.K.; Dufour, S.; Lyu, K.; Zhang, X.M.; Hakkarainen, A.; Lehtimaki, T.E.; Cline, G.W.; Petersen, K.F.; Shulman, G.I.; Yki-Jarvinen, H. Effect of a ketogenic diet on hepatic steatosis and hepatic mitochondrial metabolism in nonalcoholic fatty liver disease. Proc. Natl. Acad. Sci. USA 2020, 117, 7347–7354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprio, M.; Infante, M.; Moriconi, E.; Armani, A.; Fabbri, A.; Mantovani, G.; Mariani, S.; Lubrano, C.; Poggiogalle, E.; Migliaccio, S.; et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: Systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J. Endocrinol. Investig. 2019, 42, 1365–1386. [Google Scholar] [CrossRef]
- Gupta, L.; Khandelwal, D.; Kalra, S.; Gupta, P.; Dutta, D.; Aggarwal, S. Ketogenic diet in endocrine disorders: Current perspectives. J. Postgrad. Med. 2017, 63, 242–251. [Google Scholar] [CrossRef]
- Bruci, A.; Tuccinardi, D.; Tozzi, R.; Balena, A.; Santucci, S.; Frontani, R.; Mariani, S.; Basciani, S.; Spera, G.; Gnessi, L.; et al. Very low-calorie ketogenic diet: A safe and effective tool for weight loss in patients with obesity and mild kidney failure. Nutrients 2020, 12, 333. [Google Scholar] [CrossRef] [Green Version]
- Basciani, S.; Costantini, D.; Contini, S.; Persichetti, A.; Watanabe, M.; Mariani, S.; Lubrano, C.; Spera, G.; Lenzi, A.; Gnessi, L. Safety and efficacy of a multiphase dietetic protocol with meal replacements including a step with very low calorie diet. Endocrine 2015, 48, 863–870. [Google Scholar] [CrossRef]
- Basciani, S.; Camajani, E.; Contini, S.; Persichetti, A.; Risi, R.; Bertoldi, L.; Strigari, L.; Prossomariti, G.; Watanabe, M.; Mariani, S.; et al. Very-Low-Calorie Ketogenic Diets with Whey, Vegetable or Animal Protein in Patients with Obesity: A Randomized Pilot Study. J. Clin. Endocrinol. Metab. 2020. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Pugliese, G.; Salzano, C.; Savastano, S.; Colao, A. The management of very low-calorie ketogenic diet in obesity outpatient clinic: A practical guide. J. Transl. Med. 2019, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Steven, S.; Hollingsworth, K.G.; Al-Mrabeh, A.; Avery, L.; Aribisala, B.; Caslake, M.; Taylor, R. Very Low-Calorie Diet and 6 Months of Weight Stability in Type 2 Diabetes: Pathophysiological Changes in Responders and Nonresponders. Diabetes Care 2016, 39, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mardinoglu, A.; Wu, H.; Bjornson, E.; Zhang, C.; Hakkarainen, A.; Rasanen, S.M.; Lee, S.; Mancina, R.M.; Bergentall, M.; Pietilainen, K.H.; et al. An Integrated Understanding of the Rapid Metabolic Benefits of a Carbohydrate-Restricted Diet on Hepatic Steatosis in Humans. Cell. Metab. 2018, 27, 559–571.e55. [Google Scholar] [CrossRef] [Green Version]
- Lazo, M.; Solga, S.F.; Horska, A.; Bonekamp, S.; Diehl, A.M.; Brancati, F.L.; Wagenknecht, L.E.; Pi-Sunyer, F.X.; Kahn, S.E.; Clark, J.M.; et al. Effect of a 12-month intensive lifestyle intervention on hepatic steatosis in adults with type 2 diabetes. Diabetes Care 2010, 33, 2156–2163. [Google Scholar] [CrossRef] [Green Version]
- Fisher, F.M.; Maratos-Flier, E. Understanding the Physiology of FGF21. Annu. Rev. Physiol. 2016, 78, 223–241. [Google Scholar] [CrossRef] [Green Version]
- Badman, M.K.; Pissios, P.; Kennedy, A.R.; Koukos, G.; Flier, J.S.; Maratos-Flier, E. Hepatic fibroblast growth factor 21 is regulated by PPARalpha and is a key mediator of hepatic lipid metabolism in ketotic states. Cell. Metab. 2007, 5, 426–437. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Singhal, G.; Fisher, F.M.; Beck, T.C.; Morgan, D.A.; Socciarelli, F.; Mather, M.L.; Risi, R.; Bourke, J.; Rahmouni, K.; et al. Liver-derived FGF21 is essential for full adaptation to ketogenic diet but does not regulate glucose homeostasis. Endocrine 2020, 67, 95–108. [Google Scholar] [CrossRef]
- Tucker, B.; McClelland, R.L.; Allison, M.A.; Budoff, M.J.; Wu, B.J.; Barter, P.J.; Rye, K.A.; Ong, K.L. Relationship of fibroblast growth factor 21 levels with inflammation, lipoproteins and non-alcoholic fatty liver disease. Atherosclerosis 2020, 299, 38–44. [Google Scholar] [CrossRef]
- Fisher, F.M.; Chui, P.C.; Antonellis, P.J.; Bina, H.A.; Kharitonenkov, A.; Flier, J.S.; Maratos-Flier, E. Obesity is a fibroblast growth factor 21 (FGF21)-resistant state. Diabetes 2010, 59, 2781–2789. [Google Scholar] [CrossRef] [Green Version]
- Markan, K.R. Defining “FGF21 Resistance” during obesity: Controversy, criteria and unresolved questions. F1000Res 2018, 7, 289. [Google Scholar] [CrossRef] [PubMed]
- Fazeli, P.K.; Lun, M.; Kim, S.M.; Bredella, M.A.; Wright, S.; Zhang, Y.; Lee, H.; Catana, C.; Klibanski, A.; Patwari, P.; et al. FGF21 and the late adaptive response to starvation in humans. J. Clin. Investig. 2015, 125, 4601–4611. [Google Scholar] [CrossRef] [Green Version]
- Crujeiras, A.B.; Gomez-Arbelaez, D.; Zulet, M.A.; Carreira, M.C.; Sajoux, I.; de Luis, D.; Castro, A.I.; Baltar, J.; Baamonde, I.; Sueiro, A.; et al. Plasma FGF21 levels in obese patients undergoing energy-restricted diets or bariatric surgery: A marker of metabolic stress? Int. J. Obes. (Lond.) 2017, 41, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M.; Hall, K.D.; Guo, J.; Ravussin, E.; Mayer, L.S.; Reitman, M.L.; Smith, S.R.; Walsh, B.T.; Leibel, R.L. Glucose and Lipid Homeostasis and Inflammation in Humans Following an Isocaloric Ketogenic Diet. Obesity (Silver Spring) 2019, 27, 971–981. [Google Scholar] [CrossRef]
- Lips, M.A.; de Groot, G.H.; Berends, F.J.; Wiezer, R.; van Wagensveld, B.A.; Swank, D.J.; Luijten, A.; van Dijk, K.W.; Pijl, H.; Jansen, P.L.; et al. Calorie restriction and Roux-en-Y gastric bypass have opposing effects on circulating FGF21 in morbidly obese subjects. Clin. Endocrinol. (Oxf.) 2014, 81, 862–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, B.N.; Singhal, G.; Watanabe, M.; Stevanovic, D.; Lundasen, T.; Fisher, F.M.; Mather, M.L.; Vardeh, H.G.; Douris, N.; Adams, A.C.; et al. Fibroblast growth factor 21 (FGF21) is robustly induced by ethanol and has a protective role in ethanol associated liver injury. Mol. Metab. 2017, 6, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Dushay, J.R.; Toschi, E.; Mitten, E.K.; Fisher, F.M.; Herman, M.A.; Maratos-Flier, E. Fructose ingestion acutely stimulates circulating FGF21 levels in humans. Mol. Metab. 2015, 4, 51–57. [Google Scholar] [CrossRef]
- Schaafsma, G. The protein digestibility-corrected amino acid score. J. Nutr. 2000, 130, 1865S–1867S. [Google Scholar] [CrossRef] [Green Version]
- Dietary Reference Values for Nutrients Summary Report. EFSA 2017, 2017, e15121. [CrossRef]
- Remer, T.; Manz, F. Potential renal acid load of foods and its influence on urine pH. J. Am. Diet Assoc. 1995, 95, 791–797. [Google Scholar] [CrossRef]
- Watanabe, M.; Masieri, S.; Costantini, D.; Tozzi, R.; De Giorgi, F.; Gangitano, E.; Tuccinardi, D.; Poggiogalle, E.; Mariani, S.; Basciani, S.; et al. Overweight and obese patients with nickel allergy have a worse metabolic profile compared to weight matched non-allergic individuals. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzmarzyk, P.T.; Greenway, F.L.; Heymsfield, S.B.; Bouchard, C. Clinical utility and reproducibility of visceral adipose tissue measurements derived from dual-energy X-ray absorptiometry in White and African American adults. Obes. (Silver Spring) 2013, 21, 2221–2224. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Li, X.; Song, P.; Xu, L. Optimal cut-off values for the homeostasis model assessment of insulin resistance (HOMA-IR) and pre-diabetes screening: Developments in research and prospects for the future. Drug Discov. Ther. 2015, 9, 380–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Tuccinardi, D.; Ernesti, I.; Basciani, S.; Mariani, S.; Genco, A.; Manfrini, S.; Lubrano, C.; Gnessi, L. Scientific evidence underlying contraindications to the ketogenic diet: An update. Obes. Rev. 2020. [Google Scholar] [CrossRef]
- Castaldo, G.; Monaco, L.; Castaldo, L.; Galdo, G.; Cereda, E. An observational study of sequential protein-sparing, very low-calorie ketogenic diet (Oloproteic diet) and hypocaloric Mediterranean-like diet for the treatment of obesity. Int. J. Food Sci. Nutr. 2016, 67, 696–706. [Google Scholar] [CrossRef]
- Paoli, A.; Bosco, G.; Camporesi, E.M.; Mangar, D. Ketosis, ketogenic diet and food intake control: A complex relationship. Front. Psychol. 2015, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.K.; O’Neil, P.M.; Pawlow, L. Changes in food cravings during low-calorie and very-low-calorie diets. Obes. (Silver Spring) 2006, 14, 115–121. [Google Scholar] [CrossRef]


{kind=link}
| T0 (Mean ± SD) n = 65 (a) | T45 (Mean ± SD) n = 63 (b) | T90 (Mean ± SD) n = 45 (c) | p | |
|---|---|---|---|---|
| Anthropometrics | ||||
| Weight (Kg) | 104.6 ± 15.3 b,c | 95.1 ± 14.1 a,c | 87.5 ± 12 a,b | <0.0001 |
| BMI (Kg/m2) | 38.3 ± 6.0 b,c | 34.7.8 ± 5.7 a,c | 31.3 ± 4.0 a,b | <0.0001 |
| WC (cm) | 112.8 ± 14 b,c | 105.1 ± 17.3 a,c | 98.9 ± 9.1 a,c | <0.0001 |
| HC (cm) | 123.1 ± 10.5 b,c | 117.3 ± 10.3 a,c | 113 ± 9.8 a,b | <0.0001 |
| Body Fat (g) | 39824 ± 10492 b,c | 34078 ± 10230 a,c | 30064 ± 8923 a,b | <0.0001 |
| Lean Mass (g) | 62680±11608 b,c | 61116 ± 12160 a,c | 57412 ± 10167 a,b | <0.0001 |
| Body Fat (%) | 37.3 ± 7.0 b,c | 34.7 ± 7.7 a,c | 33.3 ± 8.1 a,b | <0.0001 |
| Lean Mass (%) | 59.8 ± 7.8 b,c | 62.9 ± 7.2 a,c | 64.1 ± 7.8 a,b | 0.0003 |
| VAT Mass (g) | 862.8 ± 295.9 b,c | 781.6 ± 267.5 a,c | 689.81 ± 206.9 a,b | <0.0001 |
| Clinical parameters | ||||
| Systolic BP (mmHg) | 131 (20) b,c | 122.3 ± 13.7 a,c | 120 (10) a,c | <0.0001 |
| Diastolic BP (mmHg) | 80 (15) b,c | 70 (16) a | 70 (15) a | <0.0001 |
| Biochemical parameters | ||||
| FGF21 (ng/mL) | 180.1 ± 88.9 b,c | 128.7 ± 87.7 a,c | 73.5 ± 55.5 a,b | <0.0001 |
| HbA1C (%) | 5.6 ± 0.4 b,c | 5.3 (0.4) a | 5.4 ± 0.27 a | <0.0001 |
| Glucose (mg/dL) | 98.8 ± 12.6 b | 92 (18) a | 95.2 ± 8.4 | 0.001 |
| Insulin (µUI/mL) | 16.3 (7.8) b,c | 8.1 (8.1) a,c | 6.4 ± 3 a,c | <0.0001 |
| HOMA-IR (ng/mL) | 4.5 ± 1.8 b,c | 2.2 ± 1.4 a,c | 1.5 ± 0.8 a,b | <0.0001 |
| Creatinine (mg/dL) | 0.8 (1.3) | 0.8 (1) | 0.8 ± 0.2 | ns |
| BUN (mg/dL) | 37.9 ± 8.2 | 39 (65) | 40.3 ± 11.4 | ns |
| AST (U/L) | 19 (7) | 19.5 (5) c | 17 (6) b | 0.008 |
| ALT (U/L) | 22 (13) b,c | 20 (9) a,c | 16 (9) a,b | <0.0001 |
| HSI | 47.5 ± 7.5 b,c | 43.3 ± 6.3 a,c | 33.5 ± 4.6 a,b | <0.0001 |
| TC (mg/dL) | 208-1 ± 42.0 b | 171.8 ± 38.2 a,c | 193.7 ± 32.3 b | <0.0001 |
| LDL-C (mg/dL) | 127.9 ± 35.3 b | 103.0 ± 32.2 a,c | 120.1 ± 29.5 b | <0.0001 |
| HDL-C (mg/dL) | 49.9 ± 12.5 | 48.7 ± 12.8 | 48 (12) | ns |
| TG (mg/dL) | 125.0 (55) b,c | 91 (33) a | 90 ± 27.7 a | <0.0001 |
| CRP (µg/dL) | 3300 (5075) | 2350 (3750) | 3650 (5350) | ns |
| ESR (mm/h) | 26 (19) | 25.5 (21) | 28 (26) | ns |
| Pearson Correlation Coefficient | p | |
|---|---|---|
| Anthropometric parameters | ||
| Age (years) | 0.132 | 0.406 |
| Weight (Kg) | −0.058 | 0.715 |
| BMI (Kg/m2) | −0.032 | 0.842 |
| WC (cm) | 0.077 | 0.626 |
| HC (cm) | −0.139 | 0.379 |
| Total Fat (g) | −0.153 | 0.333 |
| VAT Mass (g) | 0.140 | 0.382 |
| Systolic BP (mmHg) | 0.136 | 0.389 |
| Diastolic BP (mmHg) | 0.397 | 0.009 |
| Biochemical parameters | ||
| HbA1C% | 0.213 | 0.192 |
| Glucose (mg/dL) | 0.123 | 0.445 |
| Insulin (µUI/mL) | 0.400 | 0.012 |
| HOMA-IR (ng/mL) | 0.388 | 0.015 |
| Creatinine (mg/dL) | 0.106 | 0.510 |
| BUN (mg/dL) | −0.089 | 0.586 |
| AST (U/L) | 0.234 | 0.147 |
| ALT (U/L) | 0.346 | 0.025 |
| HSI | −0.083 | 0.603 |
| TC (mg/dL) | −0.075 | 0.635 |
| LDL-C (mg/dL) | −0.113 | 0.475 |
| HDL-C (mg/dL) | −0.077 | 0.634 |
| TG (mg/dL) | 0.054 | 0.741 |
| CRP (µg/dL) | −0.117 | 0.478 |
| ESR (mm/h) | −0.222 | 0.158 |
| A | Independent Variable | Standardized β | SE | Sig. | R | R Change | |||||
| Baseline HOMA-IR | 0.414 | 0.483 | 0.0009 | 0.414 | 0.172 | ||||||
| B | Independent Variable | Standardized β | SE | Sig. | R | R Change | |||||
| Baseline serum FGF21 level | −0.364 | 0.014 | 0.04 | 0.364 | 0.132 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, M.; Risi, R.; Camajani, E.; Contini, S.; Persichetti, A.; Tuccinardi, D.; Ernesti, I.; Mariani, S.; Lubrano, C.; Genco, A.; et al. Baseline HOMA IR and Circulating FGF21 Levels Predict NAFLD Improvement in Patients Undergoing a Low Carbohydrate Dietary Intervention for Weight Loss: A Prospective Observational Pilot Study. Nutrients 2020, 12, 2141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072141
Watanabe M, Risi R, Camajani E, Contini S, Persichetti A, Tuccinardi D, Ernesti I, Mariani S, Lubrano C, Genco A, et al. Baseline HOMA IR and Circulating FGF21 Levels Predict NAFLD Improvement in Patients Undergoing a Low Carbohydrate Dietary Intervention for Weight Loss: A Prospective Observational Pilot Study. Nutrients. 2020; 12(7):2141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072141
Chicago/Turabian StyleWatanabe, Mikiko, Renata Risi, Elisabetta Camajani, Savina Contini, Agnese Persichetti, Dario Tuccinardi, Ilaria Ernesti, Stefania Mariani, Carla Lubrano, Alfredo Genco, and et al. 2020. "Baseline HOMA IR and Circulating FGF21 Levels Predict NAFLD Improvement in Patients Undergoing a Low Carbohydrate Dietary Intervention for Weight Loss: A Prospective Observational Pilot Study" Nutrients 12, no. 7: 2141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072141