Effects of Pistachio Consumption in a Behavioral Weight Loss Intervention on Weight Change, Cardiometabolic Factors, and Dietary Intake

Abstract
:1. Introduction
2. Materials and Methods
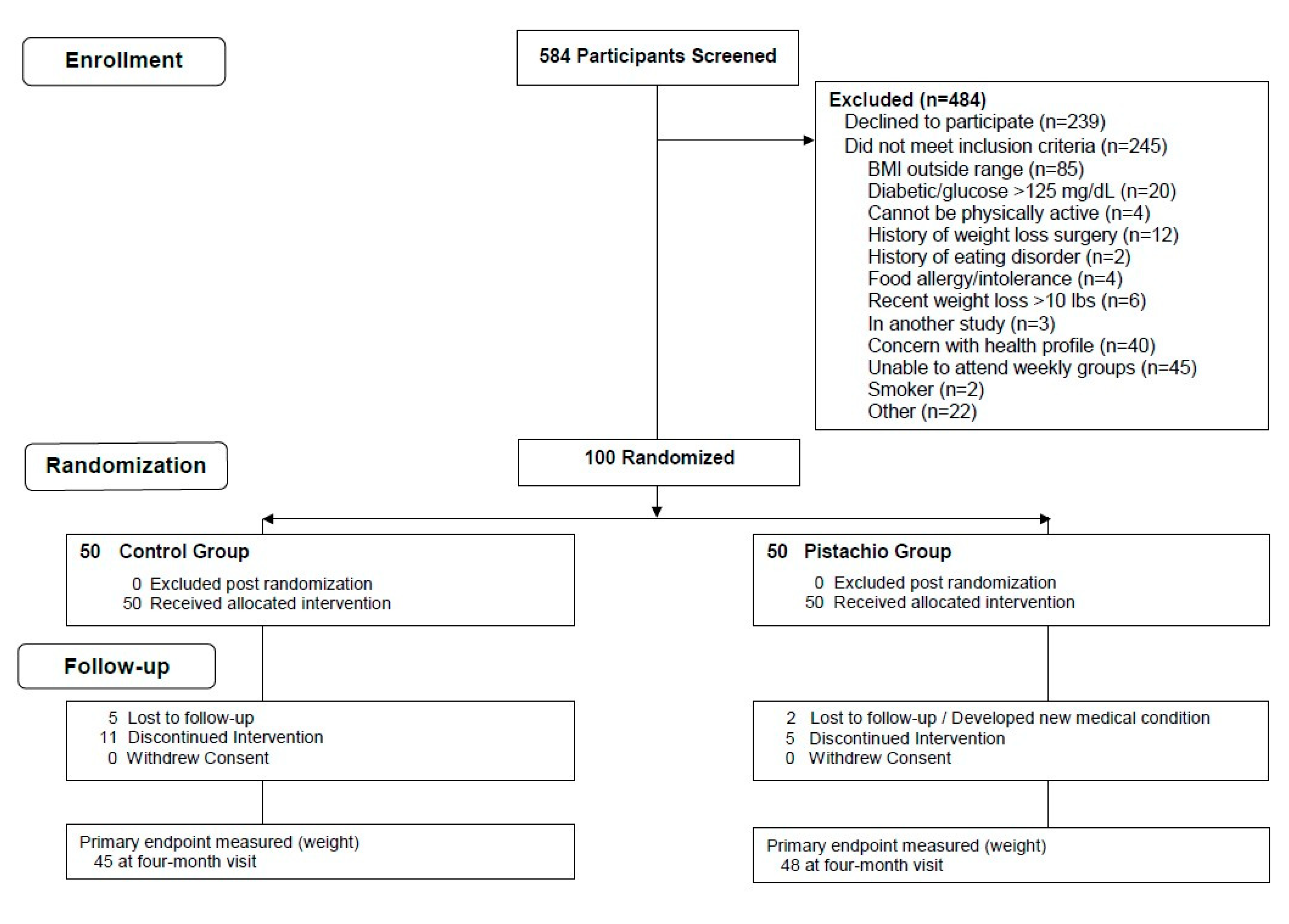
2.1. Subjects
2.2. Intervention
2.3. Measurements
2.3.1. Clinical and Anthropometric Measures
2.3.2. Dietary Assessment
2.3.3. Laboratory Measurements
2.3.4. Other Measurements and Questionnaires
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines For Americans 2015–2020, 8th ed.; U.S. Government Printing Office: Washington, DC, USA, 2015–2020.
- Bes-Rastrollo, M.; Wedick, N.M.; Martinez-Gonzalez, M.A.; Li, T.Y.; Sampson, L.; Hu, F.B. Prospective study of nut consumption, long-term weight change, and obesity risk in women. Am. J. Clin. Nutr. 2009, 89, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, X.; Yuan, S.; Jin, Y.; Lu, J. Nut consumption and risk of metabolic syndrome and overweight/obesity: A meta-analysis of prospective cohort studies and randomized trials. Nutr. Metab. 2018, 15, 46. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Keogh, J.; Clifton, P.M. Nuts and cardio-metabolic disease: A review of meta-analyses. Nutrients 2018, 10, 1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Gobbo, L.C.; Falk, M.C.; Feldman, R.; Lewis, K.; Mozaffarian, D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: Systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am. J. Clin. Nutr. 2015, 102, 1347–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreher, M.L. Pistachio nuts: Composition and potential health benefits. Nutr. Rev. 2012, 70, 234–240. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture, A.R.S. USDA National Nutrient Database for Standard Reference; USDA: Washington, DC, USA, 2016.
- Li, Z.; Song, R.; Nguyen, C.; Zerlin, A.; Karp, H.; Naowamondhol, K.; Thames, G.; Gao, K.; Li, L.; Tseng, C.H.; et al. Pistachio nuts reduce triglycerides and body weight by comparison to refined carbohydrate snack in obese subjects on a 12-week weight loss program. J. Am. Coll. Nutr. 2010, 29, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, Z.; Liu, Y.; Lv, X.; Yang, W. Effects of pistachios on body weight in Chinese subjects with metabolic syndrome. Nutr. J. 2012, 11, 20. [Google Scholar] [CrossRef] [Green Version]
- Gulati, S.; Misra, A.; Pandey, R.M.; Bhatt, S.P.; Saluja, S. Effects of pistachio nuts on body composition, metabolic, inflammatory and oxidative stress parameters in Asian Indians with metabolic syndrome: A 24-wk, randomized control trial. Nutrition 2014, 30, 192–197. [Google Scholar] [CrossRef]
- Burns-Whitmore, B.B.A.; Towne, A.H.; Roy, S.; Hall, L.M. Pistachio consumption at 20% of energy does not significantly change body composition, blood pressure or blood lipids but improves diet quality in freeliving, healthy college-aged women. Food Nutr. J. 2017, 2, 130. [Google Scholar] [CrossRef]
- Carughi, A.; Bellisle, F.; Dougkas, A.; Giboreau, A.; Feeney, M.J.; Higgs, J. A randomized controlled pilot study to assess effects of a daily pistachio (pistacia vera) afternoon snack on next-meal energy intake, satiety, and anthropometry in french women. Nutrients 2019, 11, 767. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.-Y.; Dhillon, J.; Mattes, R. A review of the effects of nuts on appetite, food intake, metabolism, and body weight. Am. J. Clin. Nutr. 2014, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coe, S. Nuts in the diet and bodyweight: What’s the relationship? Nutr. Bull. 2020, 45, 25–34. [Google Scholar] [CrossRef]
- Novotny, J.A.; Gebauer, S.K.; Baer, D.J. Discrepancy between the Atwater factor predicted and empirically measured energy values of almonds in human diets. Am. J. Clin. Nutr. 2012, 96, 296–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baer, D.J.; Gebauer, S.K.; Novotny, J.A. Measured energy value of pistachios in the human diet. Br. J. Nutr. 2012, 107, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Baer, D.J.; Gebauer, S.K.; Novotny, J.A. Walnuts consumed by healthy adults provide less available energy than predicted by the Atwater factors. J. Nutr. 2016, 146, 9–13. [Google Scholar] [CrossRef]
- Casas-Agustench, P.; Lopez-Uriarte, P.; Bullo, M.; Ros, E.; Gomez-Flores, A.; Salas-Salvado, J. Acute effects of three high-fat meals with different fat saturations on energy expenditure, substrate oxidation and satiety. Clin. Nutr. 2009, 28, 39–45. [Google Scholar] [CrossRef]
- Kranz, S.; Hill, A.M.; Fleming, J.A.; Hartman, T.J.; West, S.G.; Kris-Etherton, P.M. Nutrient displacement associated with walnut supplementation in men. J. Hum. Nutr. Diet. 2014, 27 (Suppl. 2), 247–254. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L., 3rd; Nicklas, T.A. Tree nut consumption improves nutrient intake and diet quality in US adults: An analysis of National Health and Nutrition Examination Survey (NHANES) 1999–2004. Asia Pac. J. Clin. Nutr. 2010, 19, 142–150. [Google Scholar]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., 3rd. Tree nut consumption is associated with better nutrient adequacy and diet quality in adults: National Health and Nutrition Examination Survey 2005–2010. Nutrients 2015, 7, 595–607. [Google Scholar] [CrossRef] [Green Version]
- Expert Panel: Report: Guidelines (2013) for managing overweight and obesity in adults. Obesity 2014, 22, i–xvi. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/oby.20818 (accessed on 30 June 2020). [CrossRef]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Energy, Ntrition, and Human Performance, 6th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Schakel, S.F. Maintaining a nutrient database in a changing marketplace: Keeping pace with changing food products—A research perspective. J. Food Compos. Anal. 2001, 14, 315–322. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Targher, G.; Alberiche, M.; Bonadonna, R.C.; Saggiani, F.; Zenere, M.B.; Monauni, T.; Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: Studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 2000, 23, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, C.L.; Natarajan, L.; Pu, M.; Thomson, C.A.; Flatt, S.W.; Caan, B.J.; Gold, E.B.; Al-Delaimy, W.K.; Newman, V.A.; Hajek, R.A.; et al. Longitudinal biological exposure to carotenoids is associated with breast cancer-free survival in the Women’s Healthy Eating and Living Study. Cancer Epidemiol. Prev. Biomark. 2009, 18, 486–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. The use of the Godin-Shephard Leisure-Time Physical Activity Questionnaire in oncology research: A systematic review. BMC Med. Res. Methodol. 2015, 15, 60. [Google Scholar] [CrossRef] [Green Version]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Hays, N.P.; Roberts, S.B. Aspects of eating behaviors “disinhibition” and “restraint” are related to weight gain and BMI in women. Obesity 2008, 16, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Westenhoefer, J.; Stunkard, A.J.; Pudel, V. Validation of the flexible and rigid control dimensions of dietary restraint. Int. J. Eat. Disord. 1999, 26, 53–64. [Google Scholar] [CrossRef]
- Bond, M.J.; McDowell, A.J.; Wilkinson, J.Y. The measurement of dietary restraint, disinhibition and hunger: An examination of the factor structure of the Three Factor Eating Questionnaire (TFEQ). Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2001, 25, 900–906. [Google Scholar] [CrossRef] [Green Version]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abazarfard, Z.; Salehi, M.; Keshavarzi, S. The effect of almonds on anthropometric measurements and lipid profile in overweight and obese females in a weight reduction program: A randomized controlled clinical trial. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2014, 19, 457–464. [Google Scholar]
- Foster, G.D.; Shantz, K.L.; Vander Veur, S.S.; Oliver, T.L.; Lent, M.R.; Virus, A.; Szapary, P.O.; Rader, D.J.; Zemel, B.S.; Gilden-Tsai, A. A randomized trial of the effects of an almond-enriched, hypocaloric diet in the treatment of obesity. Am. J. Clin. Nutr. 2012, 96, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauder, K.A.; McCrea, C.E.; Ulbrecht, J.S.; Kris-Etherton, P.M.; West, S.G. Pistachio nut consumption modifies systemic hemodynamics, increases heart rate variability, and reduces ambulatory blood pressure in well-controlled type 2 diabetes: A randomized trial. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kay, C.D.; Gebauer, S.K.; West, S.G.; Kris-Etherton, P.M. Pistachios increase serum antioxidants and lower serum oxidized-LDL in hypercholesterolemic adults. J. Nutr. 2010, 140, 1093–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Alonso, P.; Salas-Salvado, J.; Baldrich-Mora, M.; Juanola-Falgarona, M.; Bullo, M. Beneficial effect of pistachio consumption on glucose metabolism, insulin resistance, inflammation, and related metabolic risk markers: A randomized clinical trial. Diabetes Care 2014, 37, 3098–3105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njike, V.Y.; Yarandi, N.; Petraro, P.; Ayettey, R.G.; Treu, J.A.; Katz, D.L. Inclusion of walnut in the diets of adults at risk for type 2 diabetes and their dietary pattern changes: A randomized, controlled, cross-over trial. BMJ Open Diabetes Res. Care 2016, 4, e000293. [Google Scholar] [CrossRef] [Green Version]
- Neale, E.P.; Tapsell, L.C.; Martin, A.; Batterham, M.J.; Wibisono, C.; Probst, Y.C. Impact of providing walnut samples in a lifestyle intervention for weight loss: A secondary analysis of the HealthTrack trial. Food Nutr. Res. 2017, 61, 1344522. [Google Scholar] [CrossRef] [Green Version]
- Bitok, E.; Jaceldo-Siegl, K.; Rajaram, S.; Serra-Mir, M.; Roth, I.; Feitas-Simoes, T.; Ros, E.; Sabate, J. Favourable nutrient intake and displacement with long-term walnut supplementation among elderly: Results of a randomised trial. Br. J. Nutr. 2017, 118, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Jaceldo-Siegl, K.; Sabate, J.; Rajaram, S.; Fraser, G.E. Long-term almond supplementation without advice on food replacement induces favourable nutrient modifications to the habitual diets of free-living individuals. Br. J. Nutr. 2004, 92, 533–540. [Google Scholar] [CrossRef] [Green Version]
- Pearson, K.R.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Brown, R.C. Energy compensation and nutrient displacement following regular consumption of hazelnuts and other energy-dense snack foods in non-obese individuals. Eur. J. Nutr. 2017, 56, 1255–1267. [Google Scholar] [CrossRef] [PubMed]
- Lafreniere, J.; Couillard, C.; Lamarche, B.; Laramee, C.; Vohl, M.C.; Lemieux, S. Associations between self-reported vegetable and fruit intake assessed with a new web-based 24-h dietary recall and serum carotenoids in free-living adults: A relative validation study. J. Nutr. Sci. 2019, 8, e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Control Group n = 50 | Pistachio Group n = 50 |
|---|---|---|
| Sex 2 | ||
| Female | 32 (64) | 30 (60) |
| Male | 18 (36) | 20 (40) |
| Age (years) 3 | 56.2 (1.5) | 55.0 (1.6) |
| Education (years) 3 | 16.4 (0.3) | 16.4 (0.3) |
| Race/ethnicity (%) | ||
| Non-Hispanic white | 66 | 80 |
| Hispanic/Latino | 6 | 8 |
| African American | 8 | 4 |
| Asian-American | 4 | 4 |
| Mixed/other | 16 | 4 |
| Variable | Baseline | 4 Months | ||
|---|---|---|---|---|
| Control Group n = 50 | Pistachio Group n = 50 | Control Group n = 47 | Pistachio Group n = 49 | |
| Body weight (kg) | 93.8 (2.2) 1 | 94.7 (2.3) | 88.9 (2.1) | 90.0 (2.2) |
| Body mass index (kg/m2) 2 | 32.8 (0.5) | 32.8 (0.6) | 31.1 (0.5) | 31.2 (0.6) |
| Weight change (kg) | −4.8 (0.5) | −4.7 (0.7) | ||
| % Weight change | −5.1 (0.5) | −4.9 (0.6) | ||
| Waist circumference (cm) 2 | 108.6 (1.6) | 108.4 (1.4) | 102.7 (1.6) | 103.4 (1.6) |
| Variable | Baseline | 4 Months | ||
|---|---|---|---|---|
| Control Group n = 50 | Pistachio Group n = 50 | Control Group n = 45 | Pistachio Group n = 48 | |
| Systolic blood pressure (mm Hg) | 124 (2) 1 | 130 (2) | 121 (2) | 121 (2) 2 |
| Diastolic blood pressure (mm Hg) | 81 (1) | 83 (1) | 77 (2) | 78 (1) 2 |
| Moderate/strenuous physical activity (minutes/week) | 190 (30) | 172 (22) | 373 (62) 2 | 306 (29) 3 |
| Step test (heart rate/30 s) | 54 (1) | 55 (1) | 49 (1) 2 | 50 (1) 2 |
| Variable | Baseline | 4 Months | ||
|---|---|---|---|---|
| Control Group n = 50 | Pistachio Group n = 50 | Control Group n = 44 | Pistachio Group n = 47 | |
| Cholesterol (mg/dL) | 206 (5) 1 | 204 (6) | 194 (5) | 194 (6) |
| Triglycerides (mg/dL) | 123 (8) | 135 (12) | 108 (6) | 123 (8) |
| HDL Cholesterol (mg/dL) | 60 (2) | 58 (2) | 60 (2) | 58 (2) |
| LDL Cholesterol (mg/dL) | 121 (4) | 119 (5) | 112 (4) | 111 (5) |
| Insulin (umol/mL) | 14 (1) | 14 (1) | 13 (1) | 13 (1) |
| Glucose (mg/dL) | 98 (1) | 99 (1) | 99 (1) | 99 (1) |
| Homeostasis model assessment-insulin resistance | 3.4 (0.2) | 3.4 (0.3) | 3.3 (0.3) | 3.1 (0.2) |
| Alpha-Carotene (umol/L) | 0.22 (0.04) 2 | 0.12 (0.01) 2 | 0.60 (0.31) | 0.24 (0.04) 3 |
| Beta-Carotene (umol/L) | 0.72 (0.13) 2 | 0.42 (0.04) 2 | 0.92 (0.12) 2 | 0.63 (0.08) 2,3 |
| B-Cryptoxanthin (umol/L) | 0.25 (0.03) | 0.22 (0.03) | 0.25 (0.04) | 0.22 (0.04) |
| Lutein/Zeaxanthin (umol/L) | 0.60 (0.05) | 0.54 (0.05) | 0.78 (0.07) 2,3 | 0.86 (0.10) 2,3 |
| Lycopene (umol/L) | 0.75 (0.06) | 0.73 (0.06) | 0.71 (0.06) | 0.70 (0.06) |
| Variable | Baseline | 2 Months | 4 months | |||
|---|---|---|---|---|---|---|
| Control n = 50 | Pistachio n = 50 | Control n = 41 | Pistachio n = 46 | Control n = 43 | Pistachio n = 44 | |
| Energy (kcal/day) | 1933 (79) 1 | 1843 (81) | 1617 (106) 2 | 1649 (70) | 1464 (62) 3 | 1488 (60) 3 |
| % Energy from carbohydrate | 42.5 (0.9) | 40.7 (1.2) | 42.3 (1.2) | 39.5 (1.3) | 43.9 (1.3) | 41.7 (1.3) |
| % Energy from protein | 18.5 (0.6) | 18.5 (0.8) | 21.2 (1.0) 2 | 19.0 (0.7) | 20.2 (0.7) | 19.7 (0.8) |
| % Energy from fat | 35.7 (0.8) | 37.7 (1.2) | 33.9 (0.8) 5 | 38.7 (1.3) 5 | 33.7 (1.0) 4 | 36.6 (0.9) 4 |
| Carbohydrate (g/day) | 210.1 (10.5) | 193 (10.1) | 177.4 (11.6) 2 | 169.5 (9.5) | 168.8 (9.1) 2 | 159.1 (7.8) 2 |
| Protein (g/day) | 89.9 (4.8) | 82.7 (4.0) | 85.8 (7.8) | 78.5 (3.8) | 74.4 (4.0) 2 | 74.4 (3.8) |
| Fat (g/day) | 78.1 (3.3) | 79.8 (4.6) | 62.2 (4.5) 2 | 73.1 (3.8) | 56.3 (2.7) 3 | 62.7 (3.1) 2 |
| Dietary Fiber (g/day) | 20.9 (1.2) | 18.6 (0.9) | 22.6 (1.8) | 23.5 (1.4) 2 | 22.4 (1.6) | 21.5 (1.3) |
| Fruit (avg servings/day) | 1.4 (0.2) | 1.3 (0.2) | 2.3 (0.3) 2 | 1.7 (0.2) | 1.8 (0.2) | 1.6 (0.2) |
| Vegetables (avg servings/day) | 3.9 (0.4) | 3.4 (0.3) | 4.4 (0.4) | 4.1 (0.4) | 4.4 (0.4) | 4.0 (0.4) |
| Grains (avg servings/day) | 6.1 (0.3) | 5.4 (0.4) | 4.3 (0.4) 3 | 4.1 (0.4) 2 | 4.3 (0.3) 3 | 4.3 (0.3) 2 |
| Dairy/nondairy alternatives (avg servings/day) | 1.5 (0.1) | 1.5 (0.1) | 1.4 (0.2) | 1.2 (0.1) 2 | 1.4 (0.2) | 1.2 (0.2) |
| Meat, fish, poultry, eggs, nuts, seeds (avg servings/day) | 7.3 (0.6) | 6.8 (0.4) | 6.4 (0.6) 4 | 8.0 (0.5) 4 | 5.6 (0.5) 2,4 | 7.1 (0.5) 4 |
| Sweets (avg servings/day) | 0.9 (0.2) | 0.9 (0.2) | 0.9 (0.2) | 1.2 (0.5) | 1.0 (0.1) 4 | 0.5 (0.1) 2,4 |
| Miscellaneous foods (avg servings/day) | 1.5 (0.3) | 1.4 (0.2) | 1.6 (0.4) | 1.4 (0.2) | 1.2 (0.2) | 1.5 (0.2) |
| Butter, margarine, oil, salad dressing (added fats) (avg servings/day) | 4.2 (0.4) | 4.3 (0.3) | 3.4 (0.4) | 3.2 (0.4) 2 | 3.2 (0.3) | 2.9 (0.3) 2 |
| Total HEI-2015 Score 6 | 63.5 (1.9) | 60.9 (1.8) | 69.1 (1.6) 2 | 72.5 (1.8) 3 | 69.0 (2.0) 2 | 70.3 (1.9) 3 |
| HEI Component 1: Total vegetables | 3.7 (0.2) | 3.7 (0.2) | 4.4 (0.2) 2 | 4.0 (0.2) | 4.4 (0.2) 2 | 4.1 (0.2) |
| HEI Component 2: Greens and beans | 3.6 (0.3) | 3.1 (0.3) | 4.2 (0.2) 2 | 4.0 (0.3) 2 | 4.3 (0.2) 2,4 | 3.4 (0.3) 4 |
| HEI Component 3: Total fruit | 2.1 (0.2) | 2.0 (0.3) | 3.4 (0.2) 3 | 2.8 (0.3) 2 | 3.2 (0.3) 2 | 2.9 (0.3) 2 |
| HEI Component 4: Whole fruit | 3.0 (0.3) | 2.5 (0.3) | 3.9 (0.3) 2 | 3.5 (0.3) 2 | 3.8 (0.3) | 3.5 (0.3) 2 |
| HEI Component 5: Whole grains | 5.5 (0.5) | 4.5 (0.5) | 5.3 (0.6) | 4.9 (0.6) | 5.6 (0.5) | 6.3 (0.5) 2 |
| HEI Component 6: Dairy | 5.3 (0.4) | 5.3 (0.4) | 5.4 (0.5) | 4.8 (0.4) | 5.9 (0.5) | 5.0 (0.4) |
| HEI Component 7: Total protein foods | 4.8 (0.1) | 4.9 (0.1) | 4.9 (0.1) | 5.0 (0.0) | 4.8 (0.1) | 4.8 (0.1) |
| HEI Component 8: Seafood and plant protein | 3.6 (0.3) | 3.9 (0.2) | 3.6 (0.3) 5 | 5.0 (0.0) 3,5 | 3.9 (0.3) | 4.5 (0.2) 2 |
| HEI Component 9: Fatty acid ratio | 5.8 (0.5) | 5.6 (0.5) | 4.7 (0.5) 5 | 8.2 (0.4) 3,5 | 5.0 (0.5) 4 | 6.9 (0.5) 4 |
| HEI Component 10: Sodium | 4.8 (0.4) | 4.8 (0.4) | 5.5 (0.5) | 5.7 (0.5) | 4.6 (0.5) | 5.5 (0.5) |
| HEI Component 11: Refined grains | 6.8 (0.4) | 6.7 (0.5) | 8.5 (0.4) 2 | 8.2 (0.4) 2 | 7.9 (0.4) 2 | 7.3 (0.5) |
| HEI Component 12: Added sugars: | 8.5 (0.3) | 8.4 (0.3) | 9.1 (0.3) | 9.3 (0.2) 2 | 9.3 (0.2) 2 | 9.2 (0.2) 2 |
| HEI Component 13: Saturated fats | 6.1 (0.4) | 5.4 (0.5) | 7.4 (0.5) 2 | 7.3 (0.4) 2 | 7.3 (0.4) 2 | 7.4 (0.4) 2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rock, C.L.; Zunshine, E.; Nguyen, H.T.; Perez, A.O.; Zoumas, C.; Pakiz, B.; White, M.M. Effects of Pistachio Consumption in a Behavioral Weight Loss Intervention on Weight Change, Cardiometabolic Factors, and Dietary Intake. Nutrients 2020, 12, 2155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072155
Rock CL, Zunshine E, Nguyen HT, Perez AO, Zoumas C, Pakiz B, White MM. Effects of Pistachio Consumption in a Behavioral Weight Loss Intervention on Weight Change, Cardiometabolic Factors, and Dietary Intake. Nutrients. 2020; 12(7):2155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072155
Chicago/Turabian StyleRock, Cheryl L., Elizabeth Zunshine, Huong Thien Nguyen, Annemarie O. Perez, Christine Zoumas, Bilge Pakiz, and Martha M. White. 2020. "Effects of Pistachio Consumption in a Behavioral Weight Loss Intervention on Weight Change, Cardiometabolic Factors, and Dietary Intake" Nutrients 12, no. 7: 2155. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072155