Effectiveness of Protein Supplementation Combined with Resistance Training on Muscle Strength and Physical Performance in Elderly: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources and Search
2.3. Eligibility Criteria and Study Selection
2.4. Data Collection Process
2.5. Outcomes
2.6. Risk of Bias of Individual Studies
2.7. Statistical Analyses
3. Results
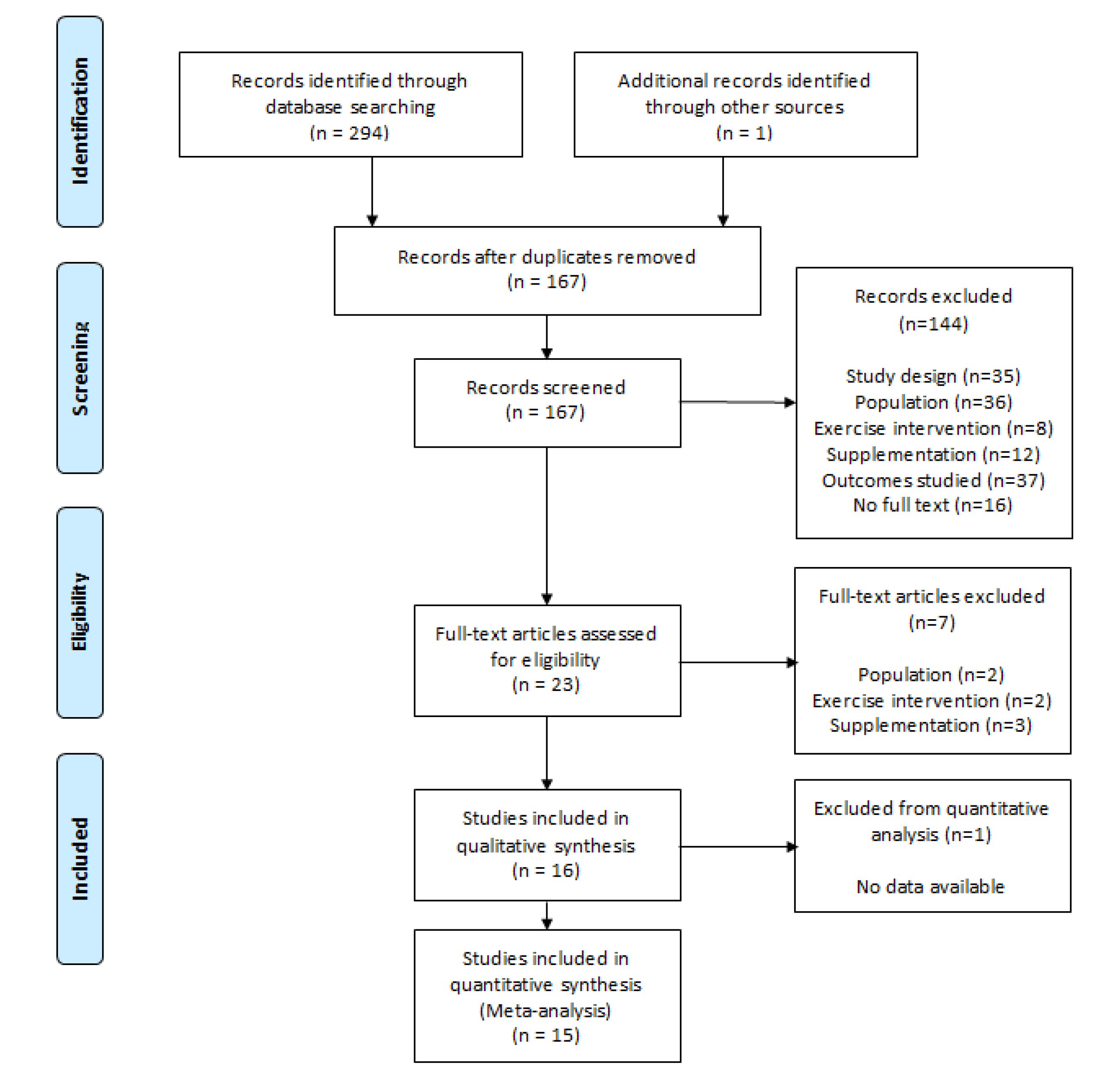
3.1. Search Strategy
3.2. Study Selection
3.3. Study Characteristics
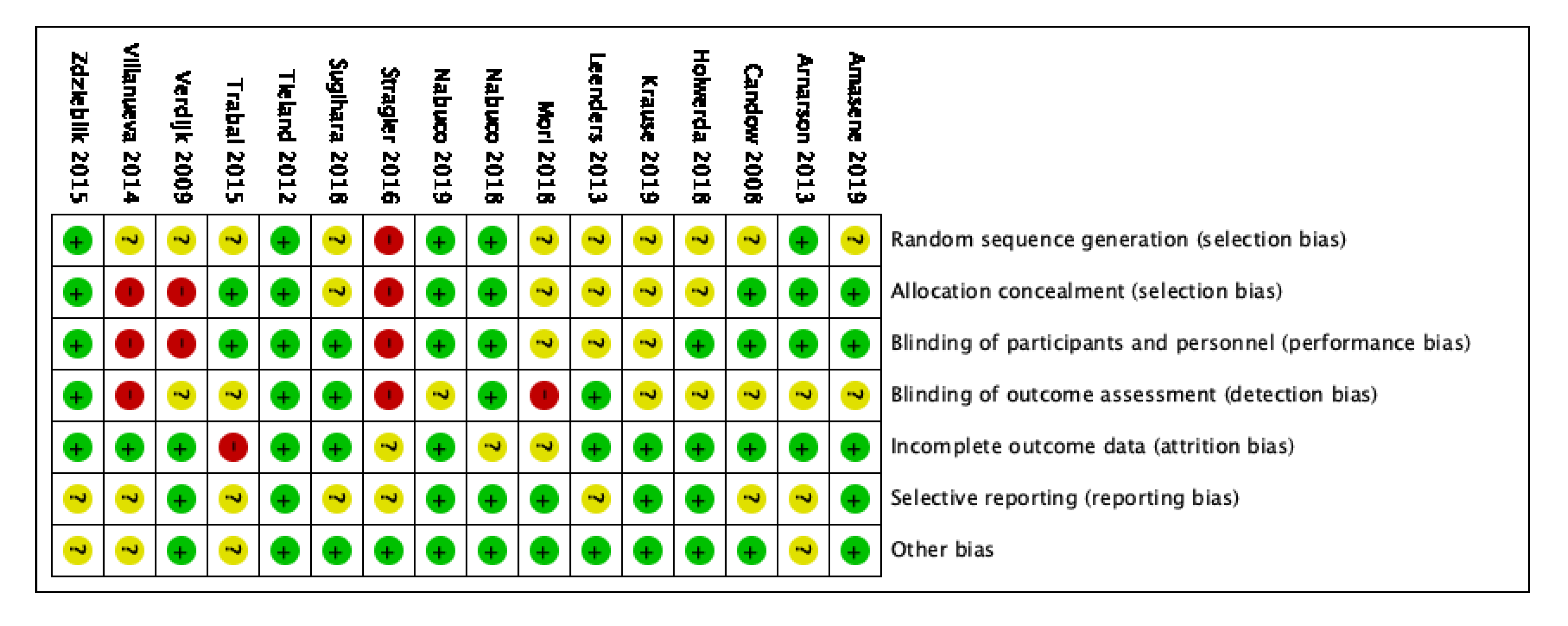
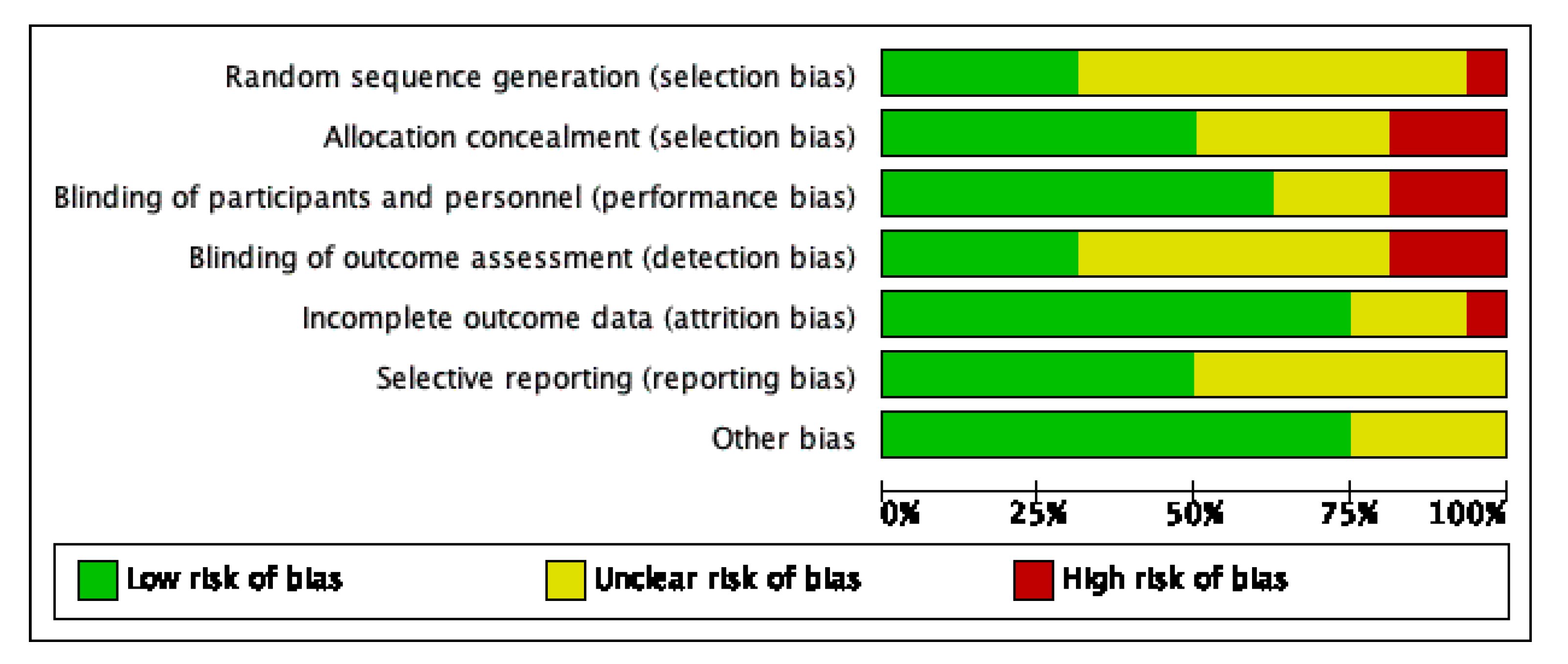
3.4. Risk of Bias Assessment
3.5. Outcomes
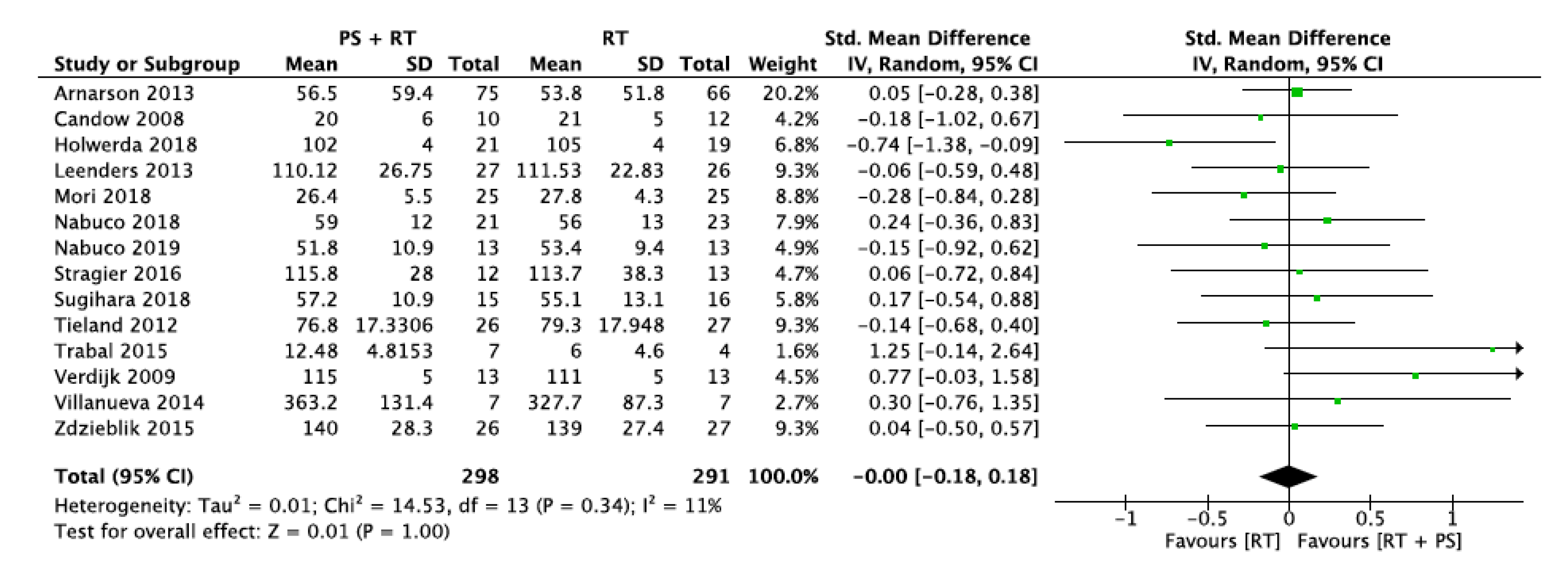
3.5.1. Lower-Limb Strength (LLS)
3.5.2. Upper-Limb Strength (ULS)
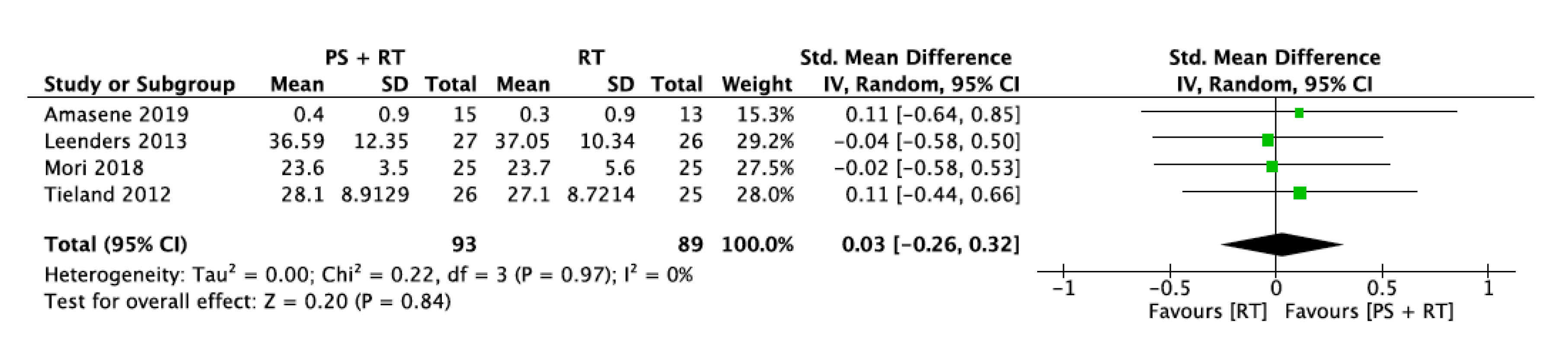
3.5.3. Handgrip Strength (HS)
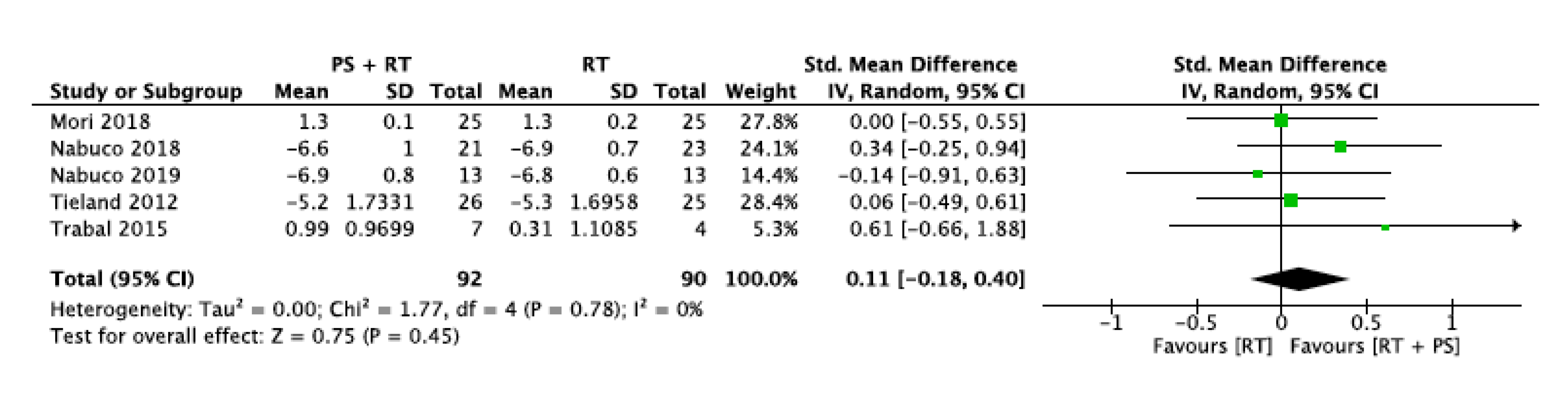
3.5.4. Gait Speed (GS)
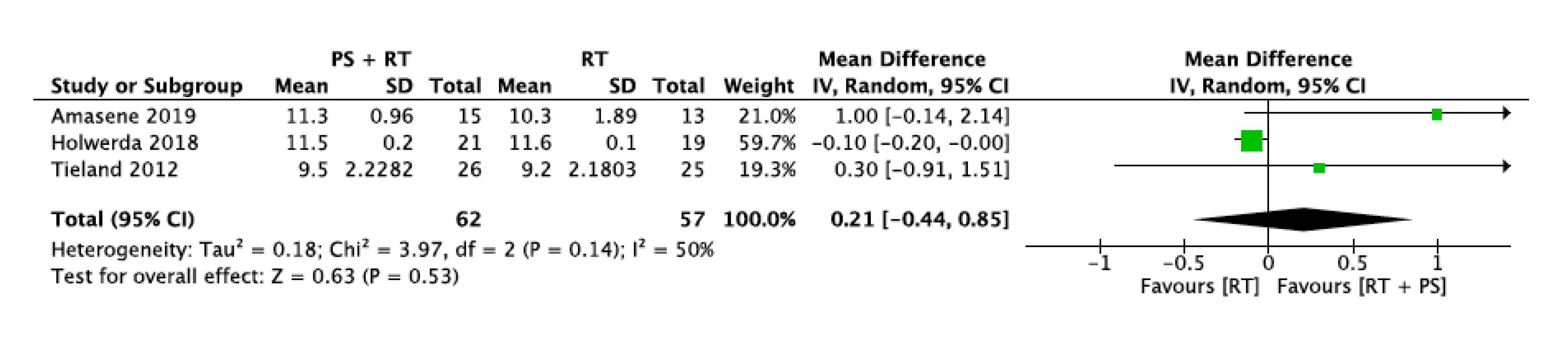
3.5.5. Short Physical Performance Battery (SPPB)
3.5.6. Five-Chair-Rise Test (5CRT)
4. Discussion
4.1. Muscle Strength
4.2. Physical Performance
4.3. Protein Supplementation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- García-Hermoso, A.; Ramirez-Vélez, R.; Sáez De Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Valenzuela, P.L.; Lucia, A.; Izquierdo, M. Safety and Effectiveness of Long-Term Exercise Interventions in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1095–1106. [Google Scholar] [CrossRef] [PubMed]
- Beltrán-Sánchez, H.; Jiménez, M.P.; Subramanian, S.V. Assessing morbidity compression in two cohorts from the health and retirement study. J. Epidemiol. Community Health 2016, 70, 1011–1016. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Keadle, S.K.; McKinnon, R.; Graubard, B.I.; Troiano, R.P. Prevalence and trends in physical activity among older adults in the United States: A comparison across three national surveys. Prev. Med. (Baltim.) 2016, 89, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Visser, M.; Simonsick, E.M.; Colbert, L.H.; Brach, J.; Rubin, S.M.; Kritchevsky, S.B.; Newman, A.B.; Harris, T.B. Type and intensity of activity and risk of mobility limitation: The mediating role of muscle parameters. J. Am. Geriatr. Soc. 2005, 53, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, L.; Cyrino, E.S.; Antunes, M.; Santos, D.A.; Sardinha, L.B. Sarcopenia and physical independence in older adults: The independent and synergic role of muscle mass and muscle function. J. Cachexia Sarcopenia Muscle 2017, 8, 245–250. [Google Scholar] [CrossRef]
- Gani, F.; Buettner, S.; Margonis, G.A.; Sasaki, K.; Wagner, D.; Kim, Y.; Hundt, J.; Kamel, I.R.; Pawlik, T.M. Sarcopenia predicts costs among patients undergoing major abdominal operations. Surgery (United States) 2016, 160, 1162–1171. [Google Scholar] [CrossRef]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail olderpersons aged 80 years and older: Results from iLSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.; Manini, T. Sarcopenia ≠ Dynapenia | The Journals of Gerontology: Series A | Oxford Academic. J. Gerontol. 2008, 63, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Morales, J.S.; Pareja-Galeano, H.; Izquierdo, M.; Emanuele, E.; de la Villa, P.; Lucia, A. Physical strategies to prevent disuse-induced functional decline in the elderly. Ageing Res. Rev. 2018, 47, 80–88. [Google Scholar] [CrossRef]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Collamati, A.; D’Angelo, E.; Pahor, M.; Bernabei, R.; et al. Sarcopenia: An overview. Aging Clin. Exp. Res. 2017, 29, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Tessier, A.J.; Chevalier, S. An update on protein, leucine, omega-3 fatty acids, and vitamin d in the prevention and treatment of sarcopenia and functional decline. Nutrients 2018, 10, 1099. [Google Scholar] [CrossRef] [Green Version]
- Martone, A.M.; Marzetti, E.; Calvani, R.; Picca, A.; Tosato, M.; Santoro, L.; Di Giorgio, A.; Nesci, A.; Sisto, A.; Santoliquido, A.; et al. Exercise and Protein Intake: A Synergistic Approach against Sarcopenia. BioMed Res. Int. 2017, 2017, 2672435. [Google Scholar] [CrossRef]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [Green Version]
- Shad, B.J.; Thompson, J.L.; Breen, L. Does the muscle protein synthetic response to exercise and amino acid-based nutrition diminish with advancing age? a systematic review. Am. J. Physiol.-Endocrinol. Metab. 2016, 311, E803–E817. [Google Scholar] [CrossRef] [Green Version]
- Paddon-Jones, D.; Short, K.R.; Campbell, W.W.; Volpi, E.; Wolfe, R.R. Role of dietary protein in the sarcopenia of aging. Am. J. Clin. Nutr. 2008, 87, 1562–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Chichester, UK, 2019; ISBN 9781119536628. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Trabal, J.; Forga, M.; Leyes, P.; Torres, F.; Rubio, J.; Prieto, E.; Farran-Codina, A. Effects of free leucine supplementation and resistance training on muscle strength and functional status in older adults: A randomized controlled trial. Clin. Interv. Aging 2015, 10, 713–723. [Google Scholar] [CrossRef] [Green Version]
- Arnarson, A.; Gudny Geirsdottir, O.; Ramel, A.; Briem, K.; Jonsson, P.V.; Thorsdottir, I. Effects of whey proteins and carbohydrates on the efficacy of resistance training in elderly people: Double blind, randomised controlled trial. Eur. J. Clin. Nutr. 2013, 67, 821–826. [Google Scholar] [CrossRef]
- Amasene, M.; Besga, A.; Echeverria, I.; Urquiza, M.; Ruiz, J.R.; Rodriguez-Larrad, A.; Aldamiz, M.; Anaut, P.; Irazusta, J.; Labayen, I. Effects of Leucine-enriched whey protein supplementation on physical function in post-hospitalized older adults participating in 12-weeks of resistance training program: A randomized controlled trial. Nutrients 2019, 11, 2337. [Google Scholar] [CrossRef] [Green Version]
- Candow, D.G.; Little, J.P.; Chilibeck, P.D.; Abeysekara, S.; Zello, G.A.; Kazachkov, M.; Cornish, S.M.; Yu, P.H. Low-dose creatine combined with protein during resistance training in older men. Med. Sci. Sports Exerc. 2008, 40, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, A.M.; Overkamp, M.; Paulussen, K.J.M.; Smeets, J.S.J.; Van Kranenburg, J.; Backx, E.M.P.; Gijsen, A.P.; Goessens, J.P.B.; Verdijk, L.B.; Van Loon, L.J.C. Protein Supplementation after Exercise and before Sleep Does Not Further Augment Muscle Mass and Strength Gains during Resistance Exercise Training in Active Older Men. J. Nutr. 2018, 148, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Crognale, D.; Cogan, K.; Contarelli, S.; Egan, B.; Newsholme, P.; De Vito, G. The effects of a combined bodyweight-based and elastic bands resistance training, with or without protein supplementation, on muscle mass, signaling and heat shock response in healthy older people. Exp. Gerontol. 2019, 115, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Verdijk, L.B.; Van Der Hoeven, L.; Van Kranenburg, J.; Nilwik, R.; Wodzig, W.K.W.H.; Senden, J.M.G.; Keizer, H.A.; Van Loon, L.J.C. Protein supplementation during resistance-type exercise training in the elderly. Med. Sci. Sports Exerc. 2013, 45, 542–552. [Google Scholar] [CrossRef]
- Mori, H.; Tokuda, Y. Effect of whey protein supplementation after resistance exercise on the muscle mass and physical function of healthy older women: A randomized controlled trial. Geriatr. Gerontol. Int. 2018, 18, 1398–1404. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.G.; Tomeleri, C.M.; Sugihara Junior, P.; Fernandes, R.R.; Cavalcante, E.F.; Antunes, M.; Ribeiro, A.S.; Teixeira, D.C.; Silva, A.M.; Sardinha, L.B.; et al. Effects of whey protein supplementation pre- or post-resistance training on muscle mass, muscular strength, and functional capacity in pre-conditioned olderwomen: A randomized clinical trial. Nutrients 2018, 10, 563. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.G.; Tomeleri, C.M.; Fernandes, R.R.; Sugihara Junior, P.; Cavalcante, E.F.; Cunha, P.M.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; et al. Effect of whey protein supplementation combined with resistance training on body composition, muscular strength, functional capacity, and plasma-metabolism biomarkers in older women with sarcopenic obesity: A randomized, double-blind, placebo-controlled t. Clin. Nutr. ESPEN 2019, 32, 88–95. [Google Scholar] [CrossRef]
- Stragier, S.; Baudry, S.; Poortmans, J.; Duchateau, J.; Carpentier, A. Leucine-enriched protein supplementation does not influence neuromuscular adaptations in response to a 6-month strength training programme in older adults. Exp. Gerontol. 2016, 82, 58–66. [Google Scholar] [CrossRef]
- Sugihara Junior, P.; Ribeiro, A.S.; Nabuco, H.C.G.; Fernandes, R.R.; Tomeleri, C.M.; Cunha, P.M.; Venturini, D.; Barbosa, D.S.; Schoenfeld, B.J.; Cyrino, E.S. Effects of Whey Protein Supplementation Associated With Resistance Training on Muscular Strength, Hypertrophy, and Muscle Quality in Preconditioned Older Women. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 528–535. [Google Scholar] [CrossRef]
- Tieland, M.; Dirks, M.L.; van der Zwaluw, N.; Verdijk, L.B.; van de Rest, O.; de Groot, L.C.P.G.M.; van Loon, L.J.C. Protein Supplementation Increases Muscle Mass Gain During Prolonged Resistance-Type Exercise Training in Frail Elderly People: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef]
- Verdijk, L.B.; Jonkers, R.A.M.; Gleeson, B.G.; Beelen, M.; Meijer, K.; Savelberg, H.H.C.M.; Wodzig, K.W.H.W.; Dendale, P.; Van Loon, L.J.C. Protein supplementation before and after exercise does not further augment skeletal muscle hypertrophy after resistance training in elderly men. Am. J. Clin. Nutr. 2009, 89, 608–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villanueva, M.G.; He, J.; Schroeder, E.T. Periodized resistance training with and without supplementation improve body composition and performance in older men. Eur. J. Appl. Physiol. 2014, 114, 891–905. [Google Scholar] [CrossRef] [PubMed]
- Zdzieblik, D.; Oesser, S.; Baumstark, M.W.; Gollhofer, A.; König, D. Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: A randomised controlled trial. Br. J. Nutr. 2015, 114, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzuela, P.L.; Mata, F.; Morales, J.S.; Castillo-García, A.; Lucia, A. Does beef protein supplementation improve body composition and exercise performance? A systematic review and meta-analysis of randomized controlled trials. Nutrients 2019, 11, 1429. [Google Scholar] [CrossRef] [Green Version]
- Hou, L.; Lei, Y.; Li, X.; Huo, C.; Jia, X.; Yang, J.; Xu, R.; Wang, X.-M. Effect of Protein Supplementation Combined With Resistance Training on Muscle Mass, Strength and Function in the Elderly: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2019, 23, 451–458. [Google Scholar] [CrossRef]
- Ten Haaf, D.S.M.; Nuijten, M.A.H.; Maessen, M.F.H.; Horstman, A.M.H.; Eijsvogels, T.M.H.; Hopman, M.T.E. Effects of protein supplementation on lean body mass, muscle strength, and physical performance in nonfrail community-dwelling older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2018, 108, 1043–1059. [Google Scholar] [CrossRef] [Green Version]
- Hsu, K.J.; Liao, C.D.; Tsai, M.W.; Chen, C.N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [Green Version]
- Finger, D.; Goltz, F.R.; Umpierre, D.; Meyer, E.; Rosa, L.H.T.; Schneider, C.D. Effects of Protein Supplementation in Older Adults Undergoing Resistance Training: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 245–255. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [Green Version]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Castro, L.H.A.; de Araújo, F.H.S.; Olimpio, M.Y.M.; Primo, R.B.D.B.; Pereira, T.T.; Lopes, L.A.F.; Trindade, E.B.S.D.M.; Fernandes, R.; Oesterreich, S.A. Comparative meta-analysis of the effect of concentrated, hydrolyzed, and isolated whey protein supplementation on body composition of physical activity practitioners. Nutrients 2019, 11, 2047. [Google Scholar] [CrossRef] [Green Version]
- Davies, R.W.; Carson, B.P.; Jakeman, P.M. The effect of whey protein supplementation on the temporal recovery of muscle function following resistance training: A systematic review and meta-analysis. Nutrients 2018, 10, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Ling, C.H.Y.; Taekema, D.; De Craen, A.J.M.; Gussekloo, J.; Westendorp, R.G.J.; Maier, A.B. Handgrip strength and mortality in the oldest old population: The Leiden 85-plus study. Cmaj 2010, 182, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyère, O.; Beaudart, C.; Reginster, J.Y.; Buckinx, F.; Schoene, D.; Hirani, V.; Cooper, C.; Kanis, J.A.; Rizzoli, R.; McCloskey, E.; et al. Assessment of muscle mass, muscle strength and physical performance in clinical practice: An international survey. Eur. Geriatr. Med. 2016, 7, 243–246. [Google Scholar] [CrossRef]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpato, S.; Cavalieri, M.; Sioulis, F.; Guerra, G.; Maraldi, C.; Zuliani, G.; Fellin, R.; Guralnik, J.M. Predictive value of the Short Physical Performance Battery following hospitalization in older patients. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2011, 66A, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Peel, N.M.; Kuys, S.S.; Klein, K. Gait speed as a measure in geriatric assessment in clinical settings: A systematic review. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 68, 39–46. [Google Scholar] [CrossRef]
- Ostir, G.V.; Berges, I.M.; Ottenbacher, K.J.; Fisher, S.R.; Barr, E.; Hebel, J.R.; Guralnik, J.M. Gait Speed and Dismobility in Older Adults. Arch. Phys. Med. Rehabil. 2015, 96, 1641–1645. [Google Scholar] [CrossRef]
- Van Kan, G.A.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) task force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertière, M.C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Kritchevsky, S.B.; Newman, A.B.; Simonsick, E.M.; Harris, T.B.; Penninx, B.W.; Brach, J.S.; Tylavsky, F.A.; Satterfield, S.; Bauer, D.C.; et al. Added Value of Physical Performance Measures in Predicting Adverse Health-Related Events: Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2009, 57, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Shikany, J.M.; Thomson, C.A. The Role of Dietary Protein Intake in the Prevention of Sarcopenia of Aging. Nutr. Clin. Pract. 2013, 28, 684–690. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Intervention | Control | Outcomes |
|---|---|---|---|
| Aged | Resistance training | Protein supplementation | Physical fitness |
| Old people | Strength training | Supplemental protein | Functionality |
| Elderly | Performance | ||
| Aging | Fitness | ||
| Older people | Strength | ||
| Older adults | Resistance | ||
| Old adults | Endurance | ||
| Frail | Balance | ||
| Senior | Stability | ||
| Geriatric | Agility | ||
| Mobility | |||
| Gait | |||
| Speed | |||
| Locomotion | |||
| Fall | |||
| Falling | |||
| Handgrip | |||
| SPPB | |||
| Tandem | |||
| TUG | |||
| Timed up and go | |||
| Quality of life | |||
| Min-mental | |||
| Cognition |
| PubMed Search Strategy |
|---|
| (aged OR “old people” OR “older people” OR “older adults” OR “old adults” OR elderly OR senior OR geriatric OR frail) AND (resistance training OR strength training) AND (“protein supplementation” OR “supplemental protein”) AND (physical fitness OR functionality OR performance OR strength OR resistance OR endurance OR balance OR stability OR agility OR mobility OR gait OR speed OR locomotion OR fall OR handgrip OR SPPB OR tandem OR TUG OR “timed up and go” OR “quality of life”) AND ((randomized controlled trial [pt] OR controlled clinical trial [pt] OR randomized [TiAb]) OR placebo [TiAb] OR clinical trials as topic [mesh: noexp] OR randomly [TiAb]) OR trial [Ti]) NOT (animals [mh] NOT humans [mh])) |
| Study | Population | RT Intervention | PS Intervention | CG | Outcomes | Main Results | ||
|---|---|---|---|---|---|---|---|---|
| N (EG/CG) | Gender (M/F) | Duration × Frequency | Type | Amount (g/d or g/s) | ||||
| Amasene, 2019 [31] | 28 (15/13) | 14/14 | 12 w × 2 s/w | Whey (+Leucine enriched) | 20 g (+3 g)/s | RT + plS | PP | ND PP |
| Arnarson, 2013 [30] | 141 (76/66) | NR | 12 w × 3 s/w | Whey | 20 g/s | RT + plS | ST, PP | ND LLS ND PP |
| Candow, 2008 [32] | 22 (10/12) | 20/0 | 10 w × 3 s/w | Whey (+Creatin) | Protein: 0.3 g∙kg−1 Creatin: 0.1 g∙kg−1 | RT + plS | ST | ↑ULS ND LLS |
| Holwerda, 2018 [33] | 40 (21/19) | 40/0 | 12 w × 3 s/w | Whey (+Leucine enriched) | 21 g/d | RT + plS | ST, PP | ND LLS ND SPPB |
| Krause, 2019 [34] | 21 (11/10) | 12/9 | 12 w × 3 s/w | Whey | 0.165 g∙kg−1 | RT + plS | PP | ND PP |
| Leenders, 2013 [35] | 53 (27/26) | 29/24 | 24 w × 3 s/w | Whey (+Casein) | 3 g + 12 g/d | RT + plS | ST, PP | ND LLS ND 5CRT ND HS |
| Mori, 2018 [36] | 50 (25/25) | 0/50 | 24 w × 2 s/w | Whey | 25 g/s | RT | ST, PP | ND LLS ND HS ND GS |
| Nabuco, 2018 [37] | 44 (21/23) | 0/44 | 12 w × 3 s/w | Whey | 35 g/s | RT + plS | ST, PP | ↑ST ↑PP |
| Nabuco, 2019 [38] | 26 (13/13) | 0/26 | 12 w × 3 s/w | Whey | 35 g/s | RT + plS | ST, PP | ND ST ND PP |
| Stragier S, 2016 [39] | 25 (12/13) | 11/14 | 24 w × 2 s/w | Leucine | 27.6 g/d | RT + plS | ST | ND LLS |
| Sugihara, 2018 [40] | 31 (15/16) | 0/31 | 12 w × 3 s/w | Whey | 35 g/s | RT + plS | ST | ↑ST |
| Tieland, 2012 [41] | 53 (26/27) | NR | 24 w × 2 s/w | Whey | 15 g/d | RT + plS | ST, PP | ND LLS ND HS ND SPPB ND GS 5CRT |
| Trabal, 2015 [29] | 11 (7/4) | NR | 12 w × 4 s/w | Leucine | 10 g/d | RT + plS | ST, PP | ↑LLS ↑TUG ND 5CRT |
| Verdijk, 2009 [42] | 26 (13/13) | 26/0 | 12 w × 3 s/w | Casein | 20 g/s | RT + plS | ST | ND LLS |
| Villanueva, 2014 [43] | 14 (7/7) | 14/0 | 12 w × 3 s/w | Whey (+Creatin) | 35 g/d | RT | ST, PP | ND ULS ND LLS ND PP |
| Zdzieblik D, 2015 [44] | 53 (26/27) | 53/0 | 12 w × 3 s/w | Collagen peptides | 15 g/d | RT + plS | ST | ↑LLS |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amasene, 2019 [31] | X | X | X | X | X | X | X | X | 8 | |||
| Arnarson, 2013 [30] | X | X | X | X | X | X | X | X | X | 9 | ||
| Candow, 2008 [32] | X | X | X | X | X | X | X | X | X | 9 | ||
| Holwerda, 2018 [33] | X | X | X | X | X | X | X | X | X | 9 | ||
| Krause, 2019 [34] | X | X | X | X | X | X | X | X | X | 9 | ||
| Leenders, 2013 [35] | X | X | X | X | X | X | X | X | X | 9 | ||
| Mori, 2018 [36] | X | X | X | X | X | X | X | X | 8 | |||
| Nabuco, 2018 [37] | X | X | X | X | X | X | X | X | X | X | 10 | |
| Nabuco, 2019 [38] | X | X | X | X | X | X | X | X | X | 9 | ||
| Stragier S, 2016 [39] | X | X | X | X | X | 5 | ||||||
| Sugihara, 2018 [40] | X | X | X | X | X | X | X | X | X | X | 10 | |
| Tieland, 2012 [41] | X | X | X | X | X | X | X | X | X | X | 10 | |
| Trabal, 2015 [29] | X | X | X | X | X | X | X | X | 8 | |||
| Verdijk, 2009 [42] | X | X | X | X | X | X | X | X | 8 | |||
| Villanueva, 2014 [43] | X | X | X | X | X | X | X | 7 | ||||
| Zdzieblik D, 2015 [44] | X | X | X | X | X | X | X | X | X | 9 | ||
| Average | 8.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labata-Lezaun, N.; Llurda-Almuzara, L.; López-de-Celis, C.; Rodríguez-Sanz, J.; González-Rueda, V.; Hidalgo-García, C.; Muniz-Pardos, B.; Pérez-Bellmunt, A. Effectiveness of Protein Supplementation Combined with Resistance Training on Muscle Strength and Physical Performance in Elderly: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2607. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092607
Labata-Lezaun N, Llurda-Almuzara L, López-de-Celis C, Rodríguez-Sanz J, González-Rueda V, Hidalgo-García C, Muniz-Pardos B, Pérez-Bellmunt A. Effectiveness of Protein Supplementation Combined with Resistance Training on Muscle Strength and Physical Performance in Elderly: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(9):2607. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092607
Chicago/Turabian StyleLabata-Lezaun, Noé, Luis Llurda-Almuzara, Carlos López-de-Celis, Jacobo Rodríguez-Sanz, Vanessa González-Rueda, César Hidalgo-García, Borja Muniz-Pardos, and Albert Pérez-Bellmunt. 2020. "Effectiveness of Protein Supplementation Combined with Resistance Training on Muscle Strength and Physical Performance in Elderly: A Systematic Review and Meta-Analysis" Nutrients 12, no. 9: 2607. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092607