Exploring Attitudes, Subjective Norms and Perceived Behavioural Control in a Genetic-Based and a Population-Based Weight Management Intervention: A One-Year Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
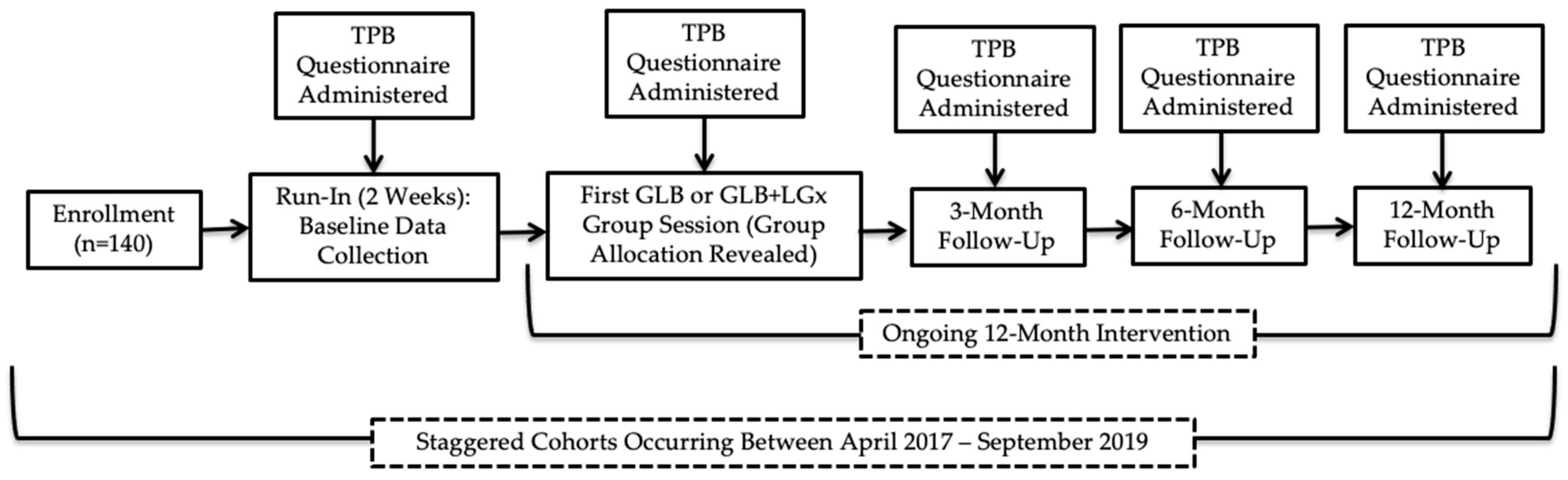
2. Materials and Methods
2.1. Participants and Setting
2.2. Interventions
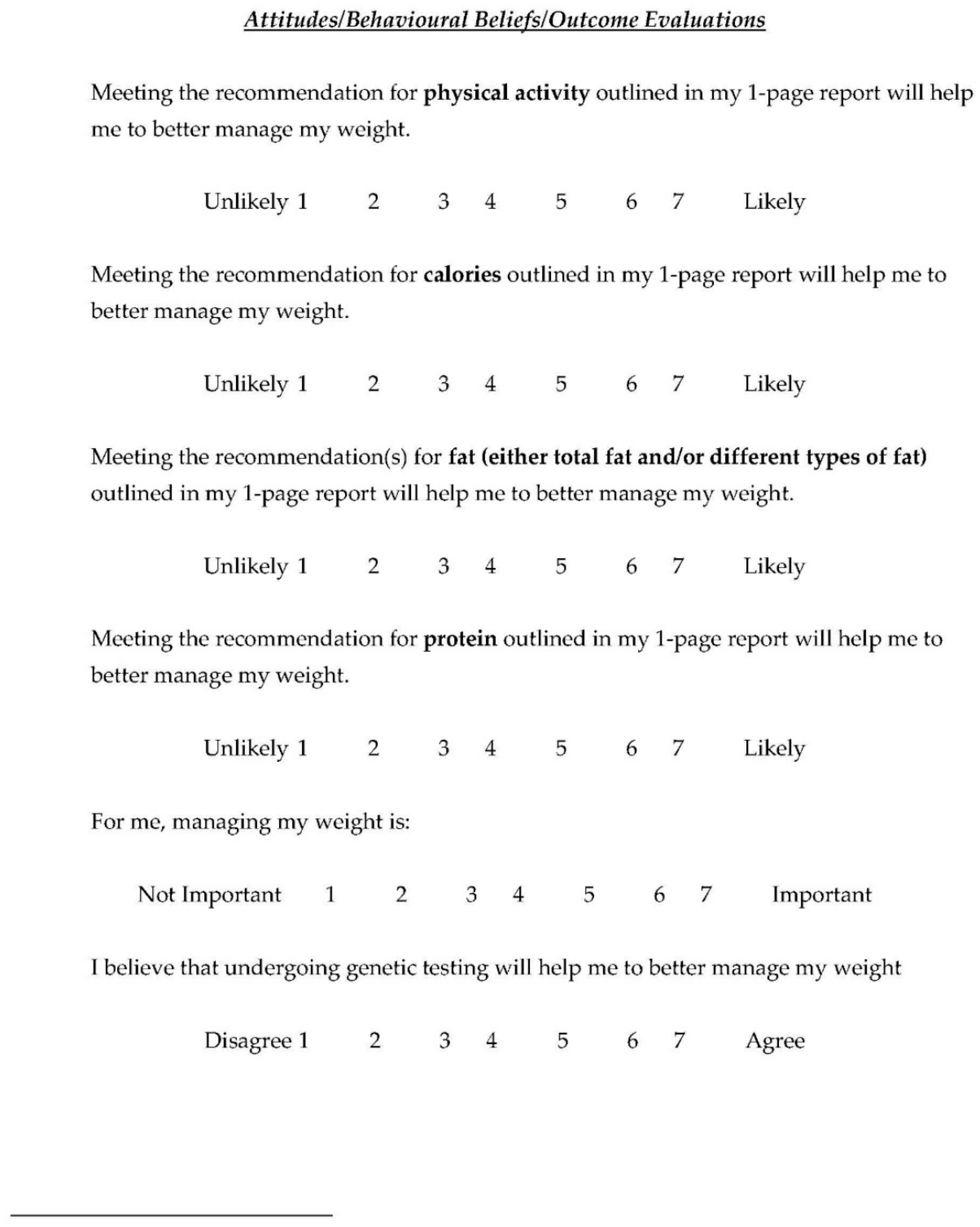
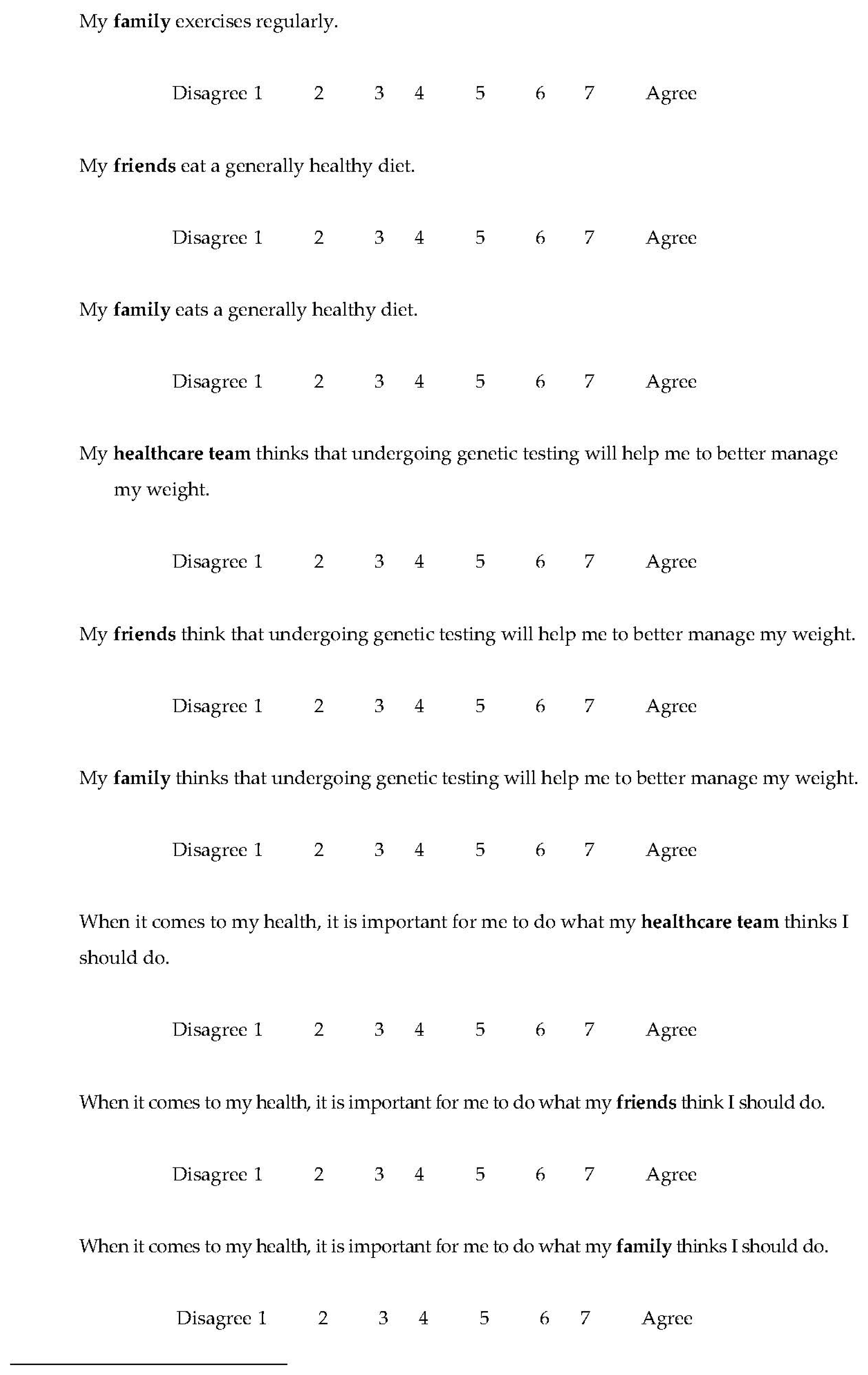
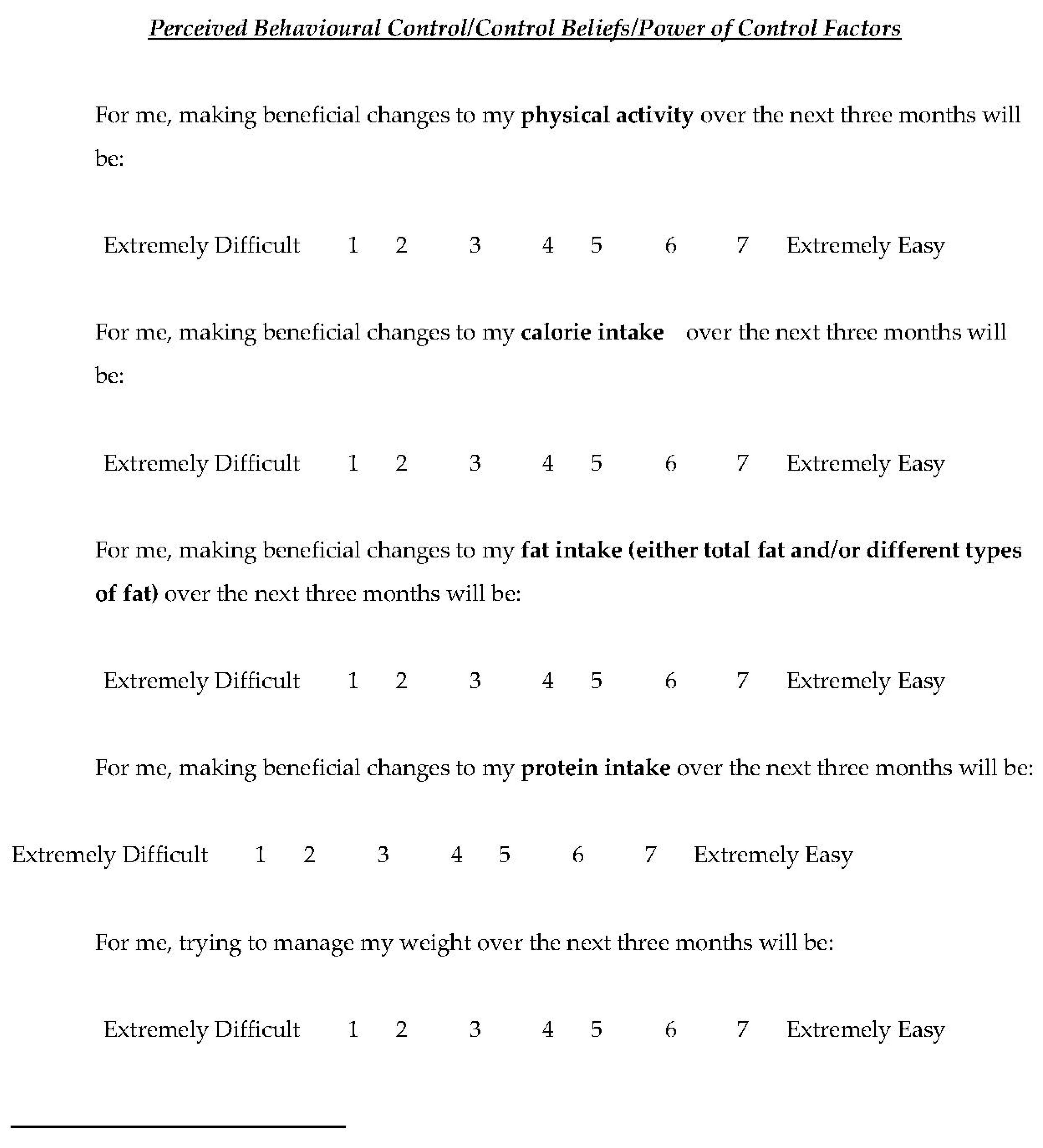
2.3. Outcomes
2.4. Statistical Analyses
3. Results
3.1. Summary of Sample and Baseline Data
3.2. Differences between GLB and GLB+LGx Groups
3.3. Change in Attitudes Within Groups
3.4. Change in Subjective Norms Within Groups
3.5. Change in Perceived Behavioural Control
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Spahn, J.M.; Reeves, R.S.; Keim, K.S.; Laquatra, I.; Kellogg, M.; Jortberg, B.; Clark, N.A. State of the Evidence Regarding Behavior Change Theories and Strategies in Nutrition Counseling to Facilitate Health and Food Behavior Change. J. Am. Diet. Assoc. 2010, 110, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Mak. Process. 1991, 51, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. Icek, Ajzen: Theory of Planned Behavior [Internet]. 2006. Available online: http://people.umass.edu/aizen/tpb.html (accessed on 11 April 2017).
- Mcdermott, M.S.; Oliver, M.; Simnadis, T.; Beck, E.J.; Coltman, T.; Iverson, D.; Caputi, P.; Sharma, R. The Theory of Planned Behaviour and dietary patterns: A systematic review and meta-analysis. Prev. Med. 2015, 81, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEachan, R.R.C.; Conner, M.; Taylor, N.J.; Lawton, R.J. Prospective prediction of health-related behaviours with the Theory of Planned Behaviour: A meta-analysis. Health Psychol. Rev. 2011, 5, 97–144. [Google Scholar] [CrossRef]
- Burgess, E.; Hassmén, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef]
- Stonerock, G.L.; Blumenthal, J.A. Role of Counseling to Promote Adherence in Healthy Lifestyle Medicine: Strategies to Improve Exercise Adherence and Enhance Physical Activity. Prog. Cardiovasc. Dis. 2017, 59, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Hietaranta-Luoma, H.; Tahvonen, R.; Iso-Touru, T.; Puolijoki, H. An Intervention Study of Individual, apoE Genotype-Based Dietary and Physical-Activity Advice: Impact on Health Behavior. Lifestyle Genom. 2014, 7, 161–174. [Google Scholar] [CrossRef]
- Nielsen, D.E.; El-Sohemy, A. Disclosure of genetic information and change in dietary intake: A randomized controlled trial. PLoS ONE 2014, 9, e112665. [Google Scholar] [CrossRef]
- Egglestone, C.; Morris, A.; O’Brien, A. Effect of direct-to-consumer genetic tests on health behaviour and anxiety: A survey of consumers and potential consumers. J. Genet. Couns. 2013, 22, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Horne, J.; Madill, J.; O’Connor, C.; Shelley, J.; Gilliland, J. A Systematic Review of Genetic Testing and Lifestyle Behaviour Change: Are We Using High-Quality Genetic Interventions and Considering Behaviour Change Theory? Lifestyle Genom. 2018, 11, 49–63. [Google Scholar] [CrossRef]
- Horne, J.; Madill, J.; Gilliland, J. Incorporating the ‘Theory of Planned Behavior’ into personalized healthcare behavior change research: A call to action. Pers. Med. 2017, 14, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Kilpeläinen, T.O.; Qi, L.; Brage, S.; Sharp, S.J.; Sonestedt, E.; Demerath, E.; Ahmad, T.; Mora, S.; Kaakinen, M.; Sandholt, C.H.; et al. Physical activity attenuates the influence of FTO variants on obesity risk: A meta-analysis of 218,166 adults and 19,268 children. PLoS Med. 2011, 8, e1001116. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Qi, Q.; Zhang, C.; Smith, S.R.; Hu, F.B.; Sacks, F.M.; Bray, G.A.; QI, L. FTO Genotype and 2-Year Change in Body Composition and Fat Distribution in Response to Weight-Loss Diets The POUNDS LOST Trial. Diabetes 2012, 61, 3005–3011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Madill, J. Change in weight, BMI and body composition in a population-based intervention vs. genetic-based intervention: The NOW Trial. Obesity 2020, 28, 1419–1427. [Google Scholar] [CrossRef]
- Dallal, G. Randomization.com [Internet]. 2017. Available online: www.randomization.com (accessed on 10 August 2018).
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Hannaberg, P.; Madill, J. Study protocol of a pragmatic randomized controlled trial incorporated into the Group Lifestyle BalanceTM program: The nutrigenomics, overweight/obesity and weight management trial (the NOW trial). BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- University of Pittsburgh. DPP Group Lifestyle Balance Curriculum. 2017. Available online: https://www.diabetesprevention.pitt.edu/for-the-public/for-health-providers/group-lifestyle-balance-curriculum/ (accessed on 8 December 2020).
- Health Canada. Dietary Reference Intakes [Internet]. 2010. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/hpfb-dgpsa/pdf/nutrition/dri_tables-eng.pdf (accessed on 4 November 2019).
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Madill, J. Enhanced long-term dietary change and adherence in a nutrigenomics-guided intervention compared to a population-based (GLB/DPP) lifestyle intervention for weight management: Results from the NOW randomized controlled trial. BMJ Nutr. Prev. Health 2020. [Google Scholar] [CrossRef]
- O’Neill, S.C.; Kaufman, E.; DeMarco, T.; Peshkin, B.N.; McKenna, K.; Shelby, R.; Valdimarsdottir, H.B.; Rispoli, J.; Schwartz, M.D. Changes in diet and physical activity following BRCA1/2 testing. J. Psychosoc. Oncol. 2008, 26, 63–80. [Google Scholar] [CrossRef]
- Roke, K.; Walton, K.; Klingel, S.; Harnett, A.; Subedi, S.; Haines, J.; Mutch, D.M. Evaluating Changes in Omega-3 Fatty Acid Intake after Receiving Personal FADS1 Genetic Information: A Randomized Nutrigenetic Intervention. Nutrients 2017, 9, 240. [Google Scholar] [CrossRef] [Green Version]
- Marsaux, C.F.M.; Celis-Morales, C.; Fallaize, R.; Macready, A.L.; Kolossa, S.; Woolhead, C.; O’Donovan, C.B.; Forster, H.; Navas-Carretero, S.; San-Cristobal, R.; et al. Effects of a web-based personalized intervention on physical activity in European adults: A randomized controlled trial. J. Med. Internet Res. 2015, 17, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Chao, S.; Roberts, S.; Marteau, T.; Silliman, R.; Cupples, L.; Green, R. Health Behavior Changes After Genetic Risk Assessment for Alzheimer Disease: The REVEAL Study. Alzheimer Dis. Assoc. Disord. 2008, 100, 130–134. [Google Scholar] [CrossRef] [Green Version]
- Middleton, K.R.; Anton, S.D.; Perri, M.G. Long-Term Adherence to Health Behavior Change. Am. J. Lifestyle Med. 2013, 7, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiMatteo, M.R.; Giordani, P.J.; Lepper, H.S.; Croghan, T.W. Patient adherence and medical treatment outcomes: A meta-analysis. Med. Care 2002, 40, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Cruwys, T.; Bevelander, K.; Hermans, R. Social modeling of eating: A review of when and why social influence affects food intake and choice. Appetite 2015, 86, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Higgs, S. Social norms and their influence on eating behaviours. Appetite 2015, 86, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Schuz, B.; Papadakis, T.; Ferguson, S. Situation-specific social norms as mediators of social influence on snacking. Health Psychol. 2018, 37, 153–159. [Google Scholar] [CrossRef]
- Hermans, R.C.J.; Larsen, J.K.; Lochbuehler, K.; Nederkoorn, C.; Herman, C.P.; Engels, R.C.M.E. The power of social influence over food intake: Examining the effects of attentional bias and impulsivity. Br. J. Nutr. 2013, 109, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Brody, T. Intent-to-Treat Analysis Versus Per Protocol Analysis. In Clinical Trials, 2nd ed.; Elsevier Inc.: Bethesda, MD, USA, 2016. [Google Scholar]
- Gupta, S. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Drewnowski, A.; Spector, S. Poverty and obesity: The role of energy density and energy cost. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef]
- Stamatakis, E. Obesity, eating and physical activity. In Focus on Health London; Bajekal, M., Osbourne, V., Yar, M., Meltzer, M., Eds.; Office for National Statistics/Palgrave Macmillan: Manchester, UK, 2006; pp. 47–61. [Google Scholar]
- Horne, J.; Gilliland, J.; Madill, J.; Shelley, J. A critical examination of legal and ethical considerations for nutrigenetic testing with recommendations for improving regulation in Canada: From science to consumer. J. Law Biosci. 2020, 1–20. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Lifestyle Factor and TPB Component | Run-In (Mean ± SE, 95% CI) | Baseline (Mean ± SE, 95% CI) | 3 Months (Mean ± SE, 95% CI) | 6 Months (Mean ± SE, 95% CI) | 12 Months (Mean ± SE, 95% CI) | Between-Group Analyses |
|---|---|---|---|---|---|---|---|
| GLB | Attitudes towards PA for weight management | 5.79 ± 0.22, 5.82–6.52 | 6.20 ± 0.21, | 6.21 ± 0.18, | 6.33 ± 0.17, | 6.17 ± 0.18, | NS |
| 5.80–6.61 | 5.85–6.57 | 5.98–6.67 | 5.82–6.65 | ||||
| (p = 0.06) | (p = 0.04) | (p < 0.01) | (p = 0.03) | ||||
| GLB+LGx | 5.89 ± 0.20, 5.50–6.28 | 6.51 ± 0.14, | 6.50 ± 0.15, | 6.63 ± 0.11, | 6.55 ± 0.11, | ||
| 6.23–6.80 | 6.20–6.81 | 6.42–6.85 | 6.34–6.76 | ||||
| (p< 0.01) | (p < 0.01) | (p < 0.01) | (p < 0.01) | ||||
| GLB | Attitudes towards kcal for weight management | 6.34 ± 0.15, 6.05–6.64 | 6.44 ± 0.15, | 6.27 ± 0.16, | 6.41 ± 0.14, | 6.36 ± 0.14, | NS |
| 6.15–6.74 | 5.95–6.59 | 6.13–6.70 | 6.09–6.64 | ||||
| (p = 0.475) | (p = 0.627) | (p = 0.583) | (p = 0.860) | ||||
| GLB+LGx | 6.28 ± 0.14, 6.00–6.56 | 6.44 ± 0.12, | 6.55 ± 0.11, | 6.53 ± 0.10, | 6.49 ± 0.09, | ||
| 6.21–6.68 | 6.32–6.77 | 6.34–6.73 | 6.31–6.67 | ||||
| (p = 0.27) | (p = 0.07) | (p = 0.05) | (p = 0.07) | ||||
| GLB | Attitudes towards dietary fat for weight management | 6.11 ± 0.18, 5.76–6.45 | 6.48 ± 0.13, | 6.24 ± 0.15, | 6.36 ± 0.12, | 6.37 ± 0.12, | NS |
| 6.23–6.74 | 5.96–6.54 | 6.13–6.61 | 6.13–6.61 | ||||
| (p= 0.03) | (p = 0.45) | (p = 0.13) | (p = 0.10) | ||||
| GLB+LGx | 6.19 ± 0.15, 5.90–6.49 | 6.42 ± 0.14, | 6.50 ± 0.12, | 6.48 ± 0.12 | 6.39 ± 0.12, | ||
| 6.14–6.69 | 6.25–6.74 | 6.23–6.72 | 6.13–6.62 | ||||
| (p = 0.15) | (p= 0.03) | (p = 0.04) | (p = 0.14) | ||||
| GLB | Attitudes towards protein for weight management | 5.97 ± 0.16, 5.65–6.29 | 6.44 ± 0.14, | 6.13 ± 0.15, | 6.30 ± 0.12, | 6.23 ± 0.13, | NS |
| 6.16–6.71 | 5.84–6.42 | 6.06–6.54 | 5.98–6.49 | ||||
| (p< 0.01) | (p = 0.34) | (p= 0.02) | (p = 0.05) | ||||
| GLB+LGx | 6.25 ± 0.15, 5.96–6.54 | 6.50 ± 0.13, | 6.54 ± 0.11, | 6.58 ± 0.09, | 6.48 ± 0.10, | ||
| 6.25–6.76 | 6.32–6.75 | 6.40–6.77 | 6.28–6.67 | ||||
| (p = 0.12) | (p< 0.05) | (p = 0.01) | (p = 0.07) | ||||
| GLB | Attitudes towards the importance of weight management | 6.67 ± 0.12, 6.43–6.92 | 6.63 ± 0.12, | 6.67 ± 0.10, | 6.61 ± 0.11, | 6.60 ± 0.11, | NS |
| 6.40–6.89 | 6.46–6.87 | 6.39–6.83 | 6.39–6.82 | ||||
| (p = 0.73) | (p = 0.98) | (p = 0.57) | (p = 0.43) | ||||
| GLB+LGx | 6.78 ± 0.11, 6.57–6.96 | 6.90 ± 0.08, | 6.72 ± 0.10, | 6.76 ± 0.08, | 6.68 ± 0.09, | ||
| 6.75–7.05 | 6.52–6.93 | 6.60–6.92 | 6.50–6.89 | ||||
| (p = 0.22) | (p = 0.59) | (p = 0.82) | (p = 0.22) | ||||
| GLB | Attitudes towards the impact of undergoing genetic testing to enhance weight management | 6.31 ± 0.22, 5.88–6.74 | 6.16 ± 0.22, | 6.04 ± 0.21, | 6.16 ± 0.18, | 6.09 ± 0.18, | * p = 0.06 at 3 months (AS) |
| 5.73–6.58 | 5.63–6.44 | 5.81–6.52 | 5.73–6.45 | ||||
| (p = 0.48) | (p = 0.19) * | (p = 0.42) | (p = 0.18) | ||||
| GLB+LGx | 6.35 ± 0.16, 6.04–6.67 | 6.65 ± 0.14, | 6.58 ± 0.13, | 6.58 ± 0.12, | 6.46 ± 0.13, | ||
| 6.39–6.92 | 6.33–6.83 | 6.35–6.82 | 6.21–6.71 | ||||
| (p = 0.07) | (p = 0.14) * | (p = 0.12) | (p = 0.44) |
| Group | Lifestyle Factor and TPB Component | Run-In (Mean ± SE, 95% CI) | Baseline (Mean ± SE, 95% CI) | 3 Months (Mean ± SE, 95% CI) | 6 Months (Mean ± SE, 95% CI) | 12 Months (Mean ± SE, 95% CI) | Between-Group Analyses |
|---|---|---|---|---|---|---|---|
| GLB | Subjective norms: HCT and PA | 5.90 ± 0.25, 5.40–6.40 | 6.11 ± 0.21, | 6.15 ± 0.21, | 6.23 ± 0.20, | 6.08 ± 0.21, | NS |
| 5.70–6.52 | 5.74–6.56 | 5.84–6.61 | 5.66–6.50 | ||||
| (p = 0.36) | (p = 0.27) | (p = 0.12) | (p = 0.36) | ||||
| GLB+LGx | 6.25 ± 0.22, 5.82–6.68 | 6.08 ± 0.24, | 6.41 ± 0.20, | 6.45 ± 0.18, | 6.30 ± 0.20, | ||
| 5.61–6.55 | 6.02–6.81 | 6.09–6.81 | 5.91–6.69 | ||||
| (p = 0.45) | (p = 0.35) | (p = 0.16) | (p = 0.69) | ||||
| GLB | Subjective norms: HCT and nutrition | 6.71 ± 0.17, 5.84–6.50 | 6.25 ± 0.15, | 6.29 ± 0.15, | 6.42 ± 0.13, | 6.28 ± 0.14, | NS |
| 5.95–6.56 | 6.00–6.59 | 6.16–6.68 | 6.00–6.56 | ||||
| (p = 0.619) | (p = 0.419) | (p = 0.061) | (p = 0.372) | ||||
| GLB+LGx | 6.39 ± 0.16, 6.06–6.71 | 6.18 ± 0.19, | 6.55 ± 0.14, | 6.59 ± 0.13, | 6.43 ± 0.16, | ||
| 5.80–6.57 | 6.27–6.83 | 6.32–6.85 | 6.12–6.75 | ||||
| (p = 0.29) | (p = 0.24) | (p = 0.09) | (p = 0.68) | ||||
| GLB | Subjective norms: Friends and PA | 5.36 ± 0.26, 4.85–5.87 | 5.15 ± 0.25, | 5.06 ± 0.24, | 5.35 ± 0.22, | 5.02 ± 0.22, | NS |
| 4.65–5.65 | 4.60–5.53 | 4.83–5.68 | 4.58–5.87 | ||||
| (p = 0.44) | (p = 0.25) | (p = 0.66) | (p = 0.16) | ||||
| GLB+LGx | 5.28 ± 0.25, 4.80–5.77 | 5.15 ± 0.27, | 5.58 ± 0.22, | 5.53 ± 0.21, | 5.37 ± 0.22, | ||
| 4.61–5.70 | 5.15–6.00 | 5.11–5.95 | 4.94–5.80 | ||||
| (p = 0.64) | (p = 0.19) | (p = 0.24) | (p = 0.65) | ||||
| GLB | Subjective norms: Friends and nutrition | 5.43 ± 0.23, 4.96–5.89 | 5.33 ± 0.22, | 5.28 ± 0.21, | 5.38 ± 0.19, | 5.09 ± 0.21, | NS |
| 4.90–5.76 | 4.87–5.70 | 5.00–5.78 | 4.68–5.49 | ||||
| (p = 0.71) | (p = 0.55) | (p = 0.83) | (p = 0.13) | ||||
| GLB+LGx | 5.42 ± 0.23, 4.96–5.88 | 5.07 ± 0.27, | 5.57 ± 0.21, | 5.54 ± 0.20, | 5.48 ± 0.21, | ||
| 4.54–5.60 | 5.15–5.99 | 5.14–5.94 | 5.06–5.89 | ||||
| (p = 0.19) | (p = 0.47) | (p = 0.52) | (p = 0.74) | ||||
| GLB | Subjective norms: Family and PA | 5.86 ± 0.23, 5.40–6.31 | 5.85 ± 0.24, | 5.69 ± 0.22, | 5.85 ± 0.20, | 5.57 ± 0.22, | *p= 0.049 at 12 months |
| 5.39–6.32 | 5.25–6.12 | 5.45–6.25 | 5.13–6.31 | ||||
| (p = 0.99) | (p = 0.41) | (p = 0.98) | (p = 0.11) * | ||||
| GLB+LGx | 5.81 ± 0.22, 5.37–6.24 | 5.57 ± 0.23, | 5.89 ± 0.19, | 6.08 ± 0.16, | 6.01 ± 0.16, | ||
| 5.12–6.03 | 5.51–6.27 | 5.76–6.40 | 5.70–6.33 | ||||
| (p = 0.37) | (p = 0.71) | (p = 0.17) | (p = 0.24) * | ||||
| GLB | Subjective norms: Family and nutrition | 5.79 ± 0.20, 5.39–6.18 | 5.81 ± 0.21, | 5.65 ± 0.20, | 5.80 ± 0.18, | 5.47 ± 0.20, | * p = 0.050 at 12 months(AS) |
| 5.40–6.21 | 5.25–6.05 | 5.45–6.16 | 5.07–5.86 | ||||
| (p = 0.916) | (p = 0.473) | (p = 0.907) | (p = 0.058) * | ||||
| GLB+LGx | 5.93 ± 0.22, 5.50–6.36 | 5.70 ± 0.22, | 6.03 ± 0.18, | 6.05 ± 0.17, | 6.07 ± 0.16, | ||
| 5.25–6.14 | 5.67–6.39 | 5.72–6.39 | 5.75–6.39 | ||||
| (p = 0.344) | (p = 0.631) | (p = 0.523) | (p = 0.387) * | ||||
| GLB | Perception that friends exercise regularly | 3.92 ± 0.32, 3.29–4.56 | 4.33 ± 0.31, | 4.04 ± 0.28, | 4.29 ± 0.27, | 4.15 ± 0.27, | NS |
| 3.73–4.94 | 3.48–4.56 | 3.76–482 | 3.61–4.69 | ||||
| (p = 0.16) | (p = 0.66) | (p = 0.12) | (p = 0.27) | ||||
| GLB+LGx | 3.87 ± 0.28, 3.23–4.42 | 3.99 ± 0.28, | 3.89 ± 0.26, | 4.14 ± 0.24, | 4.10 ± 0.25, | ||
| 3.44–4.54 | 3.38–4.40 | 3.66–4.61 | 3.61–4.59 | ||||
| (p = 0.68) | (p = 0.95) | (p = 0.27) | (p = 0.30) | ||||
| GLB | Perception that family exercises regularly | 3.71 ± 0.35, 3.02–4.41 | 4.02 ± 0.33, | 3.91 ± 0.32, | 4.26 ± 0.31, | 4.07 ± 0.32, | NS |
| 3.36–4.68 | 3.27–4.55 | 3.65–4.87 | 3.43–4.71 | ||||
| (p = 0.28) | (p = 0.45) | (p= 0.02) | (p = 0.08) | ||||
| GLB+LGx | 4.21 ± 0.30, 3.61–4.81 | 4.55 ± 0.30, | 4.60 ± 0.26, | 4.55 ± 0.27, | 4.26 ± 0.26, | ||
| 3.97–5.14 | 4.07–5.12 | 4.01–5.09 | 3.73–4.78 | ||||
| (p = 0.23) | (p = 0.12) | (p = 0.15) | (p = 0.81) | ||||
| GLB | Perception that friends eat a healthy diet | 3.94 ± 0.30, 3.35–4.52 | 4.26 ± 0.28, | 4.21 ± 0.26, | 4.34 ± 0.26, | 4.28 ± 0.26, | NS |
| 3.72–4.81 | 3.70–4.73 | 3.83–4.86 | 3.77–4.80 | ||||
| (p = 0.20) | (p = 0.23) | (p = 0.06) | (p = 0.05) | ||||
| GLB+LGx | 4.43 ± 0.20, 4.03–4.83 | 4.43 ± 0.21, | 4.73 ± 0.20, | 4.83 ± 0.17, | 4.84 ± 0.18, | ||
| 4.02–4.85 | 4.34–5.12 | 4.51–5.16 | 4.49–5.19 | ||||
| (p = 0.99) | (p = 0.17) | (p= 0.03) | (p = 0.03) | ||||
| GLB | Perception that family eats a healthy diet | 4.64 ± 0.30, 4.05–5.23 | 4.66 ± 0.30, | 5.06 ± 0.26, | 5.02 ± 0.26, | 4.84 ± 0.27, | NS |
| 4.07–5.25 | 4.54–5.59 | 4.51–5.54 | 4.31–5.37 | ||||
| (p = 0.93) | (p< 0.05) | (p = 0.05) | (p = 0.22) | ||||
| GLB+LGx | 4.95 ± 0.21, 4.53–5.38 | 5.02 ± 0.22, | 5.23 ± 0.21, | 5.42 ± 0.19, | 5.32 ± 0.19, | ||
| 4.58–5.45 | 4.81–5.64 | 5.04–5.80 | 4.94–5.70 | ||||
| (p = 0.76) | (p = 0.17) | (p< 0.01) | (p = 0.01) | ||||
| GLB | Perception that HCT believes that genetic testing will help with weight management | 5.72 ± 0.23, 5.27–6.17 | 5.63 ± 0.23, | 5.59 ± 0.21, | 5.72 ± 0.19, | 5.67 ± 0.20, | NS |
| 5.18–6.09 | 5.19–6.00 | 5.34–6.09 | 5.27–6.07 | ||||
| (p = 0.72) | (p = 0.55) | (p = 0.98) | (p = 0.81) | ||||
| GLB+LGx | 6.11 ± 0.20, 5.72–6.50 | 5.91 ± 0.22, | 6.36 ± 0.16, | 6.32 ± 0.15, | 6.06 ± 0.20, | ||
| 5.48–6.34 | 6.04–6.67 | 6.02–6.63 | 5.67–6.45 | ||||
| (p = 0.37) | (p = 0.15) | (p = 0.17) | (p = 0.77) | ||||
| GLB | Perception that friends believe that genetic testing will help with weight management | 4.93 ± 0.29, 4.35–5.51 | 4.66 ± 0.29, | 4.38 ± 0.27, | 4.80 ± 2.54, | 4.53 ± 0.26, | *p= 0.024 at 3 months |
| 4.10–5.23 | 3.84–4.92 | 4.30–5.31 | 4.01–5.05 | ||||
| (p = 0.34) | (p= 0.04) * | (p = 0.59) | (p = 0.06) | ||||
| GLB+LGx | 4.92 ± 0.27, 4.39–5.46 | 4.71 ± 0.28, | 5.18 ± 0.24, | 5.24 ± 0.23, | 4.99 ± 0.22, | ||
| 4.15–5.23 | 4.71–5.66 | 4.79–5.68 | 4.55–5.43 | ||||
| (p = 0.46) | (p = 0.28) * | (p = 0.15) | (p = 0.71) | ||||
| GLB | Perception that family believes that genetic testing will help with weight management | 5.16 ± 0.29, 4.59–5.72 | 4.92 ± 0.27, | 4.86 ± 0.25, | 5.13 ± 0.23, | 4.81 ± 0.25, | * p = 0.05 at 12 months (AS) |
| 4.39–5.45 | 4.37–5.35 | 4.68–5.58 | 4.31–5.31 | ||||
| (p = 0.40) | (p = 0.26) | (p = 0.91) | (p = 0.14) * | ||||
| GLB+LGx | 5.16 ± 0.25, 4.65–5.66 | 5.26 ± 0.25, | 5.50 ± 0.22, | 5.67 ± 0.21, | 5.40 ± 0.19, | ||
| 4.76–5.75 | 5.06–5.94 | 5.27–6.08 | 5.03–5.77 | ||||
| (p = 0.72) | (p = 0.16) | (p= 0.02) | (p = 0.19) * | ||||
| GLB | Importance of following HCT’s advice | 6.31 ± 0.16, 5.99–6.62 | 6.08 ± 0.17, | 6.32 ± 0.14, | 6.41 ± 0.12, | 6.38 ± 0.12, | NS |
| 5.74–6.41 | 6.05–6.59 | 6.18–6.65 | 6.15–6.61 | ||||
| (p = 0.20) | (p = 0.95) | (p = 0.41) | (p = 0.53) | ||||
| GLB+LGx | 6.52 ± 0.14, 6.25–6.79 | 6.52 ± 0.13, | 6.55 ± 0.13, | 6.66 ± 0.10, | 6.50 ± 0.14, | ||
| 6.25–6.78 | 6.29–6.81 | 6.45–6.86 | 6.22–6.78 | ||||
| (p = 0.96) | (p = 0.86) | (p = 0.25) | (p = 0.87) | ||||
| GLB | Importance of following friends’ advice | 3.19 ± 0.34, 2.51–3.86 | 3.50 ± 0.34, | 3.43 ± 0.32, | 3.41 ± 0.31, | 3.40 ± 0.30, | NS |
| 2.83–4.17 | 2.80–4.05 | 2.80–4.00 | 2.79–4.00 | ||||
| (p = 0.31) | (p = 0.39) | (p = 0.38) | (p = 0.33) | ||||
| GLB+LGx | 3.49 ± 0.32, 2.85–4.13 | 3.38 ± 0.33, | 3.50 ± 0.30, | 3.62 ± 0.29, | 3.71 ± 0.28, | ||
| 2.72–4.04 | 2.91–4.10 | 3.05–4.20 | 3.15–4.28 | ||||
| (p = 0.74) | (p = 0.97) | (p = 0.63) | (p = 0.35) | ||||
| GLB | Importance of following family’s advice | 4.70 ± 0.37, 3.97–5.44 | 4.94 ± 0.37, | 4.79 ± 0.37, | 4.65 ± 0.35, | 4.65 ± 0.36, | NS |
| 4.21–5.67 | 4.06–5.51 | 3.95–5.36 | 3.95–5.36 | ||||
| (p = 0.42) | (p = 0.76) | (p = 0.80) | (p = 0.78) | ||||
| GLB+LGx | 4.58 ± 0.39, 3.80–5.36 | 4.53 ± 0.37, | 4.67 ± 0.34, | 4.66 ± 0.33, | 4.76 ± 0.32, | ||
| 3.79–5.27 | 4.00–5.35 | 4.01–5.31 | 4.13–5.40 | ||||
| (p = 0.89) | (p = 0.78) | (p = 0.80) | (p = 0.47) |
| Group | Lifestyle Factor and TPB Component | Run-In (Mean ± SE, 95% CI) | Baseline (Mean ± SE, 95% CI) | 3-Months (Mean ± SE, 95% CI) | 6-Month (Mean ± SE, 95% CI) | 12-Months (Mean ± SE, 95% CI) | Between-Group Analyses |
|---|---|---|---|---|---|---|---|
| GLB | Perceived difficulty changing PA | 4.05 ± 0.25, 4.09–5.07 | 4.19 ± 0.26, | 4.79 ± 0.24, | 4.63 ± 0.22, | 4.58 ± 0.25, | NS |
| 3.68–4.70 | 4.32–5.26 | 4.19–5.07 | 4.09–5.07 | ||||
| (p = 0.60) | (p< 0.01) | (p < 0.01) | (p = 0.02) | ||||
| GLB+LGx | 4.43 ± 0.24, 3.96–4.89 | 4.78 ± 0.24, | 5.02 ± 0.22, | 5.01 ± 0.21, | 5.15 ± 0.20, | ||
| 4.30–5.36 | 4.58–5.46 | 4.58–5.43 | 4.75–5.55 | ||||
| (p = 0.15) | (p= 0.01) | (p < 0.01) | (p < 0.01) | ||||
| GLB | Perceived difficulty changing kcal intake | 4.16 ± 0.233 | 4.32 ± 0.22, | 4.81 ± 0.20, | 4.82 ± 0.20, | 4.63 ± 0.21, | NS |
| 3.89–4.76 | 4.42–5.19 | 4.44–5.19 | 4.22–5.03 | ||||
| (p = 0.49) | (p< 0.01) | (p < 0.01) | (p = 0.02) | ||||
| GLB+LGx | 4.32 ± 0.27, 3.78–4.86 | 4.49 ± 0.26, | 4.74 ± 0.24, | 4.73 ± 0.23 | 4.68 ± 0.22, | ||
| 3.96–5.01 | 4.6–5.22 | 4.27–5.18 | 4.24–5.12 | ||||
| (p = 0.53) | (p = 0.07) | (p < 0.05) | (p = 0.03) | ||||
| GLB | Perceived difficulty changing dietary fat intake | 4.35 ± 0.25, 3.86–4.84 | 4.33 ± 0.23, | 4.90 ± 0.20, | 4.89 ± 0.20, | 4.64 ± 0.22, | NS |
| 3.88–4.79 | 4.49–5.30 | 4.49–5.29 | 4.21–5.08 | ||||
| (p = 0.94) | (p= 0.01) | (p = 0.01) | (p = 0.16) | ||||
| GLB+LGx | 4.44 ± 0.27, 3.90–4.97 | 4.20 ± 0.26, | 4.75 ± 0.23, | 4.86 ± 0.23, | 4.75 ± 0.23, | ||
| 3.68–4.72 | 4.30–4.72 | 4.41–5.32 | 4.28–5.21 | ||||
| (p = 0.37) | (p = 0.16) | (p = 0.04) | (p = 0.08) | ||||
| GLB | Perceived difficulty changing protein intake | 4.60 ± 0.24, 4.13–5.07 | 4.78 ± 0.22, | 5.12 ± 0.20, | 5.04 ± 0.20, | 4.96 ± 0.21, | NS |
| 4.34–5.21 | 4.72–5.51 | 4.64–5.43 | 4.55–5.37 | ||||
| (p = 0.45) | (p= 0.02) | (p = 0.04) | (p = 0.07) | ||||
| GLB+LGx | 4.94 ± 0.25, 4.44–5.43 | 4.86 ± 0.22, | 5.14 ± 0.20, | 5.23 ± 0.20, | 5.05 ± 0.21, | ||
| 4.42–5.31 | 7.75–5.53 | 4.84–5.62 | 4.64–5.47 | ||||
| (p = 0.77) | (p = 0.37) | (p = 0.16) | (p = 0.53) | ||||
| GLB | Perceived difficulty managing weight | 3.75 ± 0.24, 3.29–4.22 | 4.04 ± 0,23, | 4.38 ± 0.23, | 4.44 ± 0.22, | 4.39 ± 0.22, | NS |
| 3.59–4.49 | 3.92–4.83 | 3.98–4.89 | 3.95–4.83 | ||||
| (p = 0.157) | (p< 0.01) | (p < 0.01) | (p < 0.01) | ||||
| GLB+LGx | 4.10 ± 0.26, 3.59–4.60 | 4.12 ± 0.24, | 4.71 ± 0.22, | 4.53 ± 0.24, | 4.65 ± 0.22, | ||
| 3.65–4.59 | 4.27–5.14 | 4.06–5.00 | 4.22–5.08 | ||||
| (p = 0.925) | (p< 0.01) | (p = 0.04) | (p < 0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horne, J.R.; Gilliland, J.A.; Vohl, M.-C.; Madill, J. Exploring Attitudes, Subjective Norms and Perceived Behavioural Control in a Genetic-Based and a Population-Based Weight Management Intervention: A One-Year Randomized Controlled Trial. Nutrients 2020, 12, 3768. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123768
Horne JR, Gilliland JA, Vohl M-C, Madill J. Exploring Attitudes, Subjective Norms and Perceived Behavioural Control in a Genetic-Based and a Population-Based Weight Management Intervention: A One-Year Randomized Controlled Trial. Nutrients. 2020; 12(12):3768. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123768
Chicago/Turabian StyleHorne, Justine R., Jason A. Gilliland, Marie-Claude Vohl, and Janet Madill. 2020. "Exploring Attitudes, Subjective Norms and Perceived Behavioural Control in a Genetic-Based and a Population-Based Weight Management Intervention: A One-Year Randomized Controlled Trial" Nutrients 12, no. 12: 3768. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123768