The Effects of an Infant Formula Enriched with Milk Fat Globule Membrane, Long-Chain Polyunsaturated Fatty Acids and Synbiotics on Child Behavior up to 2.5 Years Old: The COGNIS Study

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
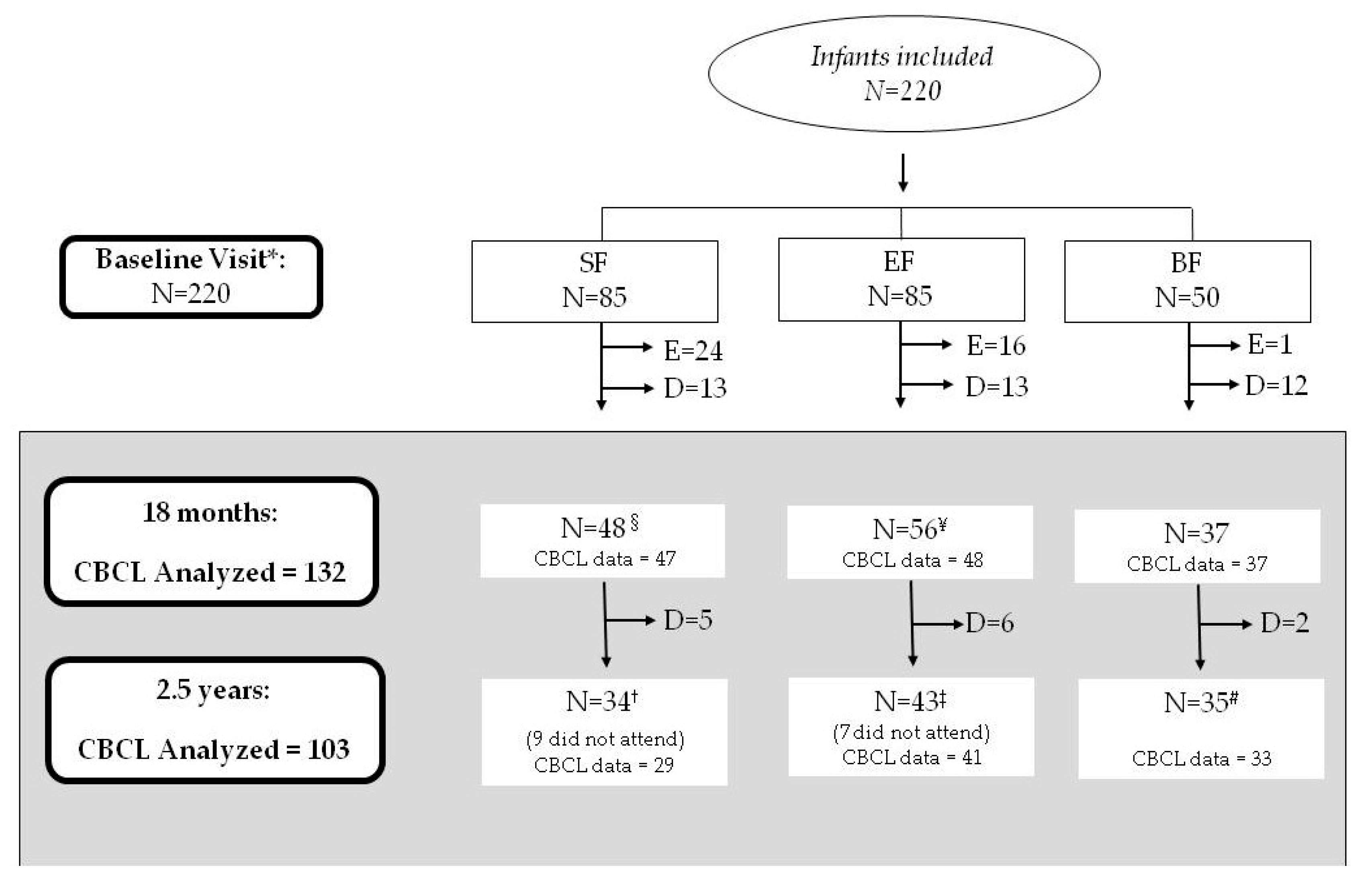
2.1. Study Design and Subjects
2.2. Ethics, Consent, and Permissions
2.3. CBCL Test (Child Behavior Checklist)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the COGNIS Study Participants up to 2.5 Years Old
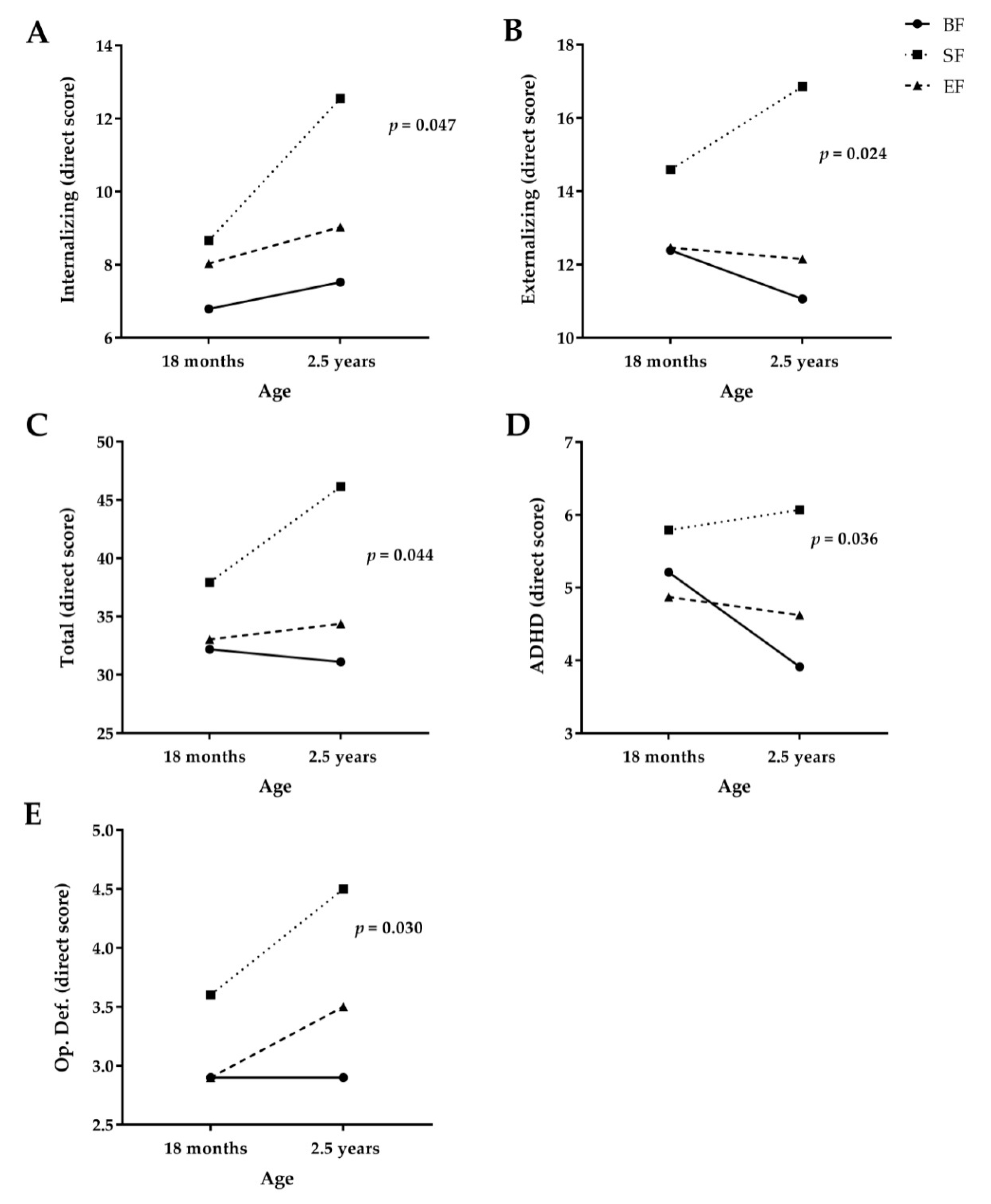
3.2. Effects of Type of Early Nutrition on Behavior Development in COGNIS Infants at 18 Months and 2.5 Years Old
3.3. Effects of Potential Confounders on Behavioral Development in COGNIS Infants at 18 Months and 2.5 Years
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Statement
References
- Rees, S.; Inder, T. Fetal and neonatal origins of altered brain development. Early Hum. Dev. 2005, 81, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Lien, E.; Agostoni, C.; Böhles, H.; Campoy, C.; Cetin, I.; Decsi, T.; Dudenhausen, J.W.; Dupont, C.; Forsyth, S.; et al. The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: Review of current knowledge and consensus recommendations. J. Perinat. Med. 2008, 36, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anjos, T.; Altmäe, S.; Emmett, P.; Tiemeier, H.; Closa-Monasterolo, R.; Luque, V.; Wiseman, S.; Pérez-García, M.; Lattka, E.; Demmelmair, H.; et al. Nutrition and neurodevelopment in children: Focus on NUTRIMENTHE project. Eur. J. Nutr. 2013, 52, 1825–1842. [Google Scholar] [CrossRef] [PubMed]
- John, C.C.; Black, M.M.; Nelson, C.A. Neurodevelopment: The Impact of Nutrition and Inflammation During Early to Middle Childhood in Low-Resource Settings. Pediatrics 2017, 139, S59–S71. [Google Scholar] [CrossRef] [Green Version]
- Furman, L. Breastfeeding: What Do We Know, and Where Do We Go From Here? Pediatrics 2017, 139, e20170150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Quinn, P.; O’Callaghan, M.; Williams, G.; Najman, J.; Andersen, M.; Bor, W. The effect of breastfeeding on child development at 5 years: A cohort study. J. Paediatr. Child Health 2001, 37, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, B.-N.; Kim, J.-W.; Shin, M.-S.; Yoo, H.J.; Cho, S.-C. Protective effect of breastfeeding with regard to children’s behavioral and cognitive problems. Nutr. J. 2014, 13, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Leung, P.; Yang, A. Breastfeeding and Active Bonding Protects against Children’s Internalizing Behavior Problems. Nutrients 2013, 6, 76–89. [Google Scholar] [CrossRef] [Green Version]
- Oddy, W.H.; Kendall, G.E.; Li, J.; Jacoby, P.; Robinson, M.; de Klerk, N.H.; Silburn, S.R.; Zubrick, S.R.; Landau, L.I.; Stanley, F.J. The long-term effects of breastfeeding on child and adolescent mental health: A pregnancy cohort study followed for 14 years. J. Pediatr. 2010, 156, 568–574. [Google Scholar] [CrossRef]
- Belfort, M.B.; Rifas-Shiman, S.L.; Kleinman, K.P.; Bellinger, D.C.; Harris, M.H.; Taveras, E.M.; Gillman, M.W.; Oken, E. Infant Breastfeeding Duration and Mid-Childhood Executive Function, Behavior, and Social-Emotional Development. J. Dev. Behav. Pediatr. 2016, 37, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of infant feeding: Key features of breast milk and infant formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to docosahexaenoic acid (DHA), eicosapentaenoic acid (EPA) and brain, eye and nerve development (ID 501, 513, 540), maintenance of normal brain function (ID 497, 501, 510, 513, 519, 521, 534, 540, 688, 1323, 1360, 4294), maintenance of normal vision (ID 508, 510, 513, 519, 529, 540, 688, 2905, 4294), maintenance of normal cardiac function (ID 510, 688, 1360), “maternal health; pregnancy and nursing” (ID 514), “to fulfil increased omega-3 fatty acids need during pregnancy” (ID 539), “skin and digestive tract epithelial cells maintenance” (ID 525), enhancement of mood (ID 536), “membranes cell structure” (ID 4295), “anti-inflammatory action” (ID 4688) and maintenance of normal blood LDL-cholesterol concentrations (ID 4719) pursuant to Article 13(1) of Regulation (EC) No 1924/2006). EFSA J. 2016, 9, 2078. [Google Scholar] [CrossRef]
- Birch, E.E.; Carlson, S.E.; Hoffman, D.R.; Fitzgerald-Gustafson, K.M.; Fu, V.L.N.; Drover, J.R.; Castañeda, Y.S.; Minns, L.; Wheaton, D.K.H.; Mundy, D.; et al. The DIAMOND (DHA Intake And Measurement Of Neural Development) Study: A double-masked, randomized controlled clinical trial of the maturation of infant visual acuity as a function of the dietary level of docosahexaenoic acid. Am. J. Clin. Nutr. 2010, 91, 848–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birch, E.E.; Garfield, S.; Castañeda, Y.; Hughbanks-Wheaton, D.; Uauy, R.; Hoffman, D. Visual acuity and cognitive outcomes at 4 years of age in a double-blind, randomized trial of long-chain polyunsaturated fatty acid-supplemented infant formula. Early Hum. Dev. 2007, 83, 279–284. [Google Scholar] [CrossRef]
- Morale, S.E.; Hoffman, D.R.; Castañeda, Y.S.; Wheaton, D.H.; Burns, R.A.; Birch, E.E. Duration of long-chain polyunsaturated fatty acids availability in the diet and visual acuity. Early Hum. Dev. 2005, 81, 197–203. [Google Scholar] [CrossRef]
- Rosenfeld, E.; Beyerlein, A.; Hadders-Algra, M.; Kennedy, K.; Singhal, A.; Fewtrell, M.; Lucas, A.; Koletzko, B.; von Kries, R. IPD meta-analysis shows no effect of LC-PUFA supplementation on infant growth at 18 months. Acta Paediatr. 2009, 98, 91–97. [Google Scholar] [CrossRef]
- Spitsberg, V.L. Invited review: Bovine milk fat globule membrane as a potential nutraceutical. J. Dairy Sci. 2005, 88, 2289–2294. [Google Scholar] [CrossRef]
- Dewettinck, K.; Rombaut, R.; Thienpont, N.; Le, T.T.; Messens, K.; Van Camp, J. Nutritional and technological aspects of milk fat globule membrane material. Int. Dairy J. 2008, 18, 436–457. [Google Scholar] [CrossRef]
- Jensen, R.G.; Ferris, A.M.; Lammi-Keefe, C.J. The Composition of Milk Fat1. J. Dairy Sci. 1991, 74, 3228–3243. [Google Scholar] [CrossRef]
- Singh, H. The milk fat globule membrane—A biophysical system for food applications. Curr. Opin. Colloid Interface Sci. 2006, 11, 154–163. [Google Scholar] [CrossRef]
- Timby, N.; Domellöf, E.; Hernell, O.; Lönnerdal, B.; Domellöf, M. Neurodevelopment, nutrition, and growth until 12 mo of age in infants fed a low-energy, low-protein formula supplemented with bovine milk fat globule membranes: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 860–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veereman-Wauters, G.; Staelens, S.; Rombaut, R.; Dewettinck, K.; Deboutte, D.; Brummer, R.-J.; Boone, M.; Le Ruyet, P. Milk fat globule membrane (INPULSE) enriched formula milk decreases febrile episodes and may improve behavioral regulation in young children. Nutrition 2012, 28, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Le Doare, K.; Holder, B.; Bassett, A.; Pannaraj, P.S. Mother’s Milk: A purposeful contribution to the development of the infant microbiota and immunity. Front. Immunol. 2018, 9, 361. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, A.; Jehmlich, N.; Haange, S.; Campoy, C.; Grasslands, A.; Drive, T.; Bag, P.; North, P. Gut microbial functional maturation and succession during human early life. Environ. Microbiol. 2018, 20, 2160–2177. [Google Scholar]
- Tognini, P. Gut Microbiota: A Potential Regulator of Neurodevelopment. Front. Cell. Neurosci. 2017, 11, 1–8. [Google Scholar] [CrossRef]
- Carlson, A.L.; Xia, K.; Azcarate-Peril, M.A.; Goldman, B.D.; Ahn, M.; Styner, M.A.; Thompson, A.L.; Geng, X.; Gilmore, J.H.; Knickmeyer, R.C. Infant Gut Microbiome Associated With Cognitive Development. Biol. Psychiatry 2018, 83, 148–159. [Google Scholar] [CrossRef]
- Nieto-Ruiz, A.; García-Santos, J.A.; Bermúdez, M.G.; Herrmann, F.; Diéguez, E.; Sepúlveda-Valbuena, N.; García, S.; Miranda, M.T.; De-Castellar, R.; Rodríguez-Palmero, M.; et al. Cortical Visual Evoked Potentials and Growth in Infants Fed with Bioactive Compounds-Enriched Infant Formula: Results from COGNIS Randomized Clinical Trial. Nutrients 2019, 11, 2456. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo, I.S.; Chisaguano-Tonato, M.; Puentes, A.D.L.G.; Nieto-Ruiz, A.; Herrmann, F.; Dieguez, E.; Castellote, A.; López-Sabater, M.C.; Rodríguez-Palmero, M.; Campoy, C. The Effect of an Infant Formula Supplemented with AA and DHA on Fatty Acid Levels of Infants with Different FADS Genotypes: The COGNIS Study. Nutrients 2019, 11, 602. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; Baker, S.; Cleghorn, G.; Fagundes, N.; Sarath, G.; Hernell, O.; Hock, Q.S.; Jirapinyo, P.; Lonnerdal, B.; Pencharz, P.; et al. Global standard for the composition of infant formula: Recomendations of an ESPGHAN coordinated international expert group. JPGN 2005, 41, 584–599. [Google Scholar] [CrossRef] [Green Version]
- Association, W.M. World medical association declaration of helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Volkmar, F.R. Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA Preschool Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2000; Volume 30. [Google Scholar]
- Rescorla, L.A. Assessment of young children using the Achenbach System of Empirically Based Assessment (ASEBA). Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.A.; Luna, J.D. Bioestadística +: Para Las Ciencias De La Salud; Capitel Editores: Madrid, Spain, 2004. [Google Scholar]
- Keunen, K.; van Elburg, R.M.; van Bel, F.; Benders, M.J.N.L. Impact of nutrition on brain development and its neuroprotective implications following preterm birth. Pediatr. Res. 2015, 77, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaelsen, K.F.; Lauritzen, L.; Mortensen, E.L. Effects of breast-feeding on cognitive function. Adv. Exp. Med. Biol. 2009, 639, 199–215. [Google Scholar]
- Horta, B.L.; Loret De Mola, C.; Victora, C.G. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. Int. J. Paediatr. 2015, 104, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; Fombonne, E.; Igumnov, S.; Vanilovich, I.; Matush, L.; Mironova, E.; Bogdanovich, N.; Tremblay, R.E.; Chalmers, B.; Zhang, X.; et al. Effects of prolonged and exclusive breastfeeding on child behavior and maternal adjustment: Evidence from a large, randomized trial. Pediatrics 2008, 121, e435–e440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wigg, N.R.; Tong, S.; McMichael, A.J.; Baghurst, P.A.; Vimpani, G.; Roberts, R. Does breastfeeding at six months predict cognitive development? Aust. N. Z. J. Public Health 1998, 22, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Mazzocchi, A.; Leone, L.; Ciappolino, V.; Delvecchio, G.; Altamura, C.A.; Brambilla, P. The first model of keeping energy balance and optimal psycho affective development: Breastfed infants. J. Affect. Disord. 2017, 224, 10–15. [Google Scholar] [CrossRef]
- Lönnerdal, B. Infant formula and infant nutrition: Bioactive proteins of human milk and implications for composition of infant formulas. Am. J. Clin. Nutr. 2014, 99, 712S–717S. [Google Scholar] [CrossRef] [Green Version]
- Sauer, P.J.J. Can we define an infant’s need from the composition of human milk? Am. J. Clin. Nutr. 2013, 98, 521S–528S. [Google Scholar]
- Qawasmi, A.; Landeros-Weisenberger, A.; Leckman, J.F.; Bloch, M.H. Meta-analysis of long-chain polyunsaturated fatty acid supplementation of formula and infant cognition. Pediatrics 2012, 129, 1141–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pecoraro, L.; Agostoni, C.; Pepaj, O.; Pietrobelli, A. Behind human milk and breastfeeding: Not only food. Int. J. Food Sci. Nutr. 2017, 69, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Green, P.; John Mann, J.; Rapoport, S.I.; Sublette, M.E. Pathways of polyunsaturated fatty acid utilization: Implications for brain function in neuropsychiatric health and disease. Brain Res. 2015, 1597, 220–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the essential composition of infant and follow-on formulae. EFSA J. 2014, 12, 3760. [Google Scholar] [CrossRef] [Green Version]
- Pärtty, A.; Kalliomäki, M.; Wacklin, P.; Salminen, S.; Isolauri, E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: A randomized trial. Pediatr. Res. 2015, 77, 823–828. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.A.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutr. Neurosci. 2018, 21, 676–681. [Google Scholar] [CrossRef]
- Sonego, M.; Llácer, A.; Galán, I.; Simón, F. The influence of parental education on child mental health in Spain. Qual. Life Res. 2013, 22, 203–211. [Google Scholar] [CrossRef]
- Kwok, M.K.; Leung, G.M.; Schooling, C.M. Breast feeding and early adolescent behaviour, self-esteem and depression: Hong Kong’s “Children of 1997” birth cohort. Arch. Dis. Child. 2013, 98, 887–894. [Google Scholar] [CrossRef]
- Liu, J.; Chen, X.; Lewis, G. Childhood internalizing behaviour: Analysis and implications. J. Psychiatr. Ment. Health Nurs. 2011, 18, 884–894. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, N.; Cumberland, A.; Spinrad, T.L.; Fabes, R.A.; Shepard, S.A.; Reiser, M.; Murphy, B.C.; Losoya, S.H.; Guthrie, I.K. The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Dev. 2001, 72, 1112–1134. [Google Scholar] [CrossRef]
- Gustavson, K.; Ystrom, E.; Stoltenberg, C.; Susser, E.; Surén, P.; Magnus, P.; Knudsen, G.P.; Smith, G.D.; Langley, K.; Rutter, M.; et al. Smoking in Pregnancy and Child ADHD. Pediatrics 2017, 139, e20162509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malanchini, M.; Smith-Woolley, E.; Ayorech, Z.; Rimfeld, K.; Krapohl, E.; Vuoksimaa, E.; Korhonen, T.; Bartels, M.; van Beijsterveldt, T.C.E.M.; Rose, R.J.; et al. Aggressive behaviour in childhood and adolescence: The role of smoking during pregnancy, evidence from four twin cohorts in the EU-ACTION consortium. Psychol. Med. 2019, 49, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Grossi, E.; Migliore, L.; Muratori, F. Pregnancy risk factors related to autism: An Italian case-control study in mothers of children with autism spectrum disorders (ASD), their siblings and of typically developing children. J. Dev. Orig. Health Dis. 2018, 9, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.H.; van den Heuvel, M.I.; Lahti, M.; Braeken, M.; de Rooij, S.R.; Entringer, S.; Hoyer, D.; Roseboom, T.; Räikkönen, K.; King, S.; et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2017, 117, 26–64. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parents Characteristics | 18 Months | 2.5 Years Old | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SF (n = 47) | EF (n = 48) | BF (n =37) | p1 | SF (n = 29) | EF (n = 41) | BF (n = 33) | p1 | ||
| Maternal age (years) | 32 (27–35) | 32 (27.5–36) | 34 (30–38) | 0.12 | 33(29.5–3) | 32 (29–36) | 34(31–38.5) | 0.27 | |
| Maternal pBMI, (kg/m2) | 24.3 ± 3.9 | 24.8 ± 4.4 | 24.5 ± 3.2 | 0.86 | 24.2 ± 3.5 | 24.3 ± 4.3 | 24.9 ± 3.2 | 0.71 | |
| Maternal educational level | Primary | 9(19.1%) a,b | 13 (27.1%) b | 1 (2.7%) a | < 0.001 | 4 (13.8%) | 6 (14.6%) | 1 (3.0%) | 0.001 |
| Secondary | 14 (29.9%) a | 8 (16.7%) a,b | 2 (5.4%) b | 11 (37.9%) a | 10 (24.4%) a,b | 2 (6.1%) b | |||
| VT | 9 (19.1%) | 15 (31.2%) | 9 (24.3%) | 4 (13.8%) | 15 (36.6%) | 8 (24.2%) | |||
| University | 15 (31.9%) a | 12 (25.0%) a | 25 (67.6%) b | 10 (34.5%) a | 10 (24.4%) a | 22 (66.7%) b | |||
| Maternal IQ (points) | 104.7 ± 14.4 a,b | 101.1 ± 14.2a | 109.4 ± 13.5 b | 0.030 | 105.4 ± 15.5 | 102.4 ± 12.9 | 109.5 ± 14.1 | 0.10 | |
| Smoking during pregnancy | No | 31 (73.8%) a | 37 (84.1%) a,b | 34 (94.4%) b | 0.049 | 21 (77.8%) | 33 (82.5%) | 31 (93.9%) | 0.16 |
| Yes | 11 (26.2%) a | 7 (15.9%) a,b | 2 (5.6%) b | 6 (22.2%) | 7 (17.5%) | 2 (6.1%) | |||
| GWG (kg) | 6.5 (4–10) | 5 (3–9) | 6.3 (4.5–9) | 0.80 | 5 (3–8) | 5 (3–8.7) | 6 (4.2–8.7) | 0.42 | |
| Type of delivery | Vaginal | 34 (72.3%) | 33 (68.8%) | 27 (73.0%) | 0.89 | 23 (79.3%) | 27 (65.9%) | 25 (75.8%) | 0.46 |
| Caesarean | 13 (27.7%) | 15 (31.2%) | 10 (27.0%) | 6 (20.7%) | 14 (34.1%) | 8 (24.2%) | |||
| Postpartum Depression | No | 38 (80.9%) | 39 (81.2%) | 31 (83.8%) | 0.93 | 22 (75.9%) | 34 (82.9%) | 28 (84.8%) | 0.63 |
| Yes | 9 (19.1%) | 9 (18.8%) | 6 (16.2%) | 7 (24.1%) | 7 (17.1%) | 5 (15.2%) | |||
| Paternal educational level | Primary | 16 (34.8%) a,b | 23 (48.9%) b | 6 (16.2%) a | 0.013 | 10 (34.5%) | 16 (39.0%) | 6 (18.2%) | 0.45 |
| Secondary | 13 (28.3%) | 6 (12.8%) | 5 (13.5%) | 6 (20.7%) | 8 (19.5%) | 5 (15.2%) | |||
| VT | 7 (15.2%) | 8 (17.0%) | 11 (29.8%) | 6 (20.7%) | 9 (22.0%) | 10 (30.3%) | |||
| University | 10 (21.7%) | 10 (21.3%) | 15 (40.5%) | 7 (24.1%) | 8 (19.5%) | 12 (36.4%) | |||
| Paternal IQ (points) | 105.9 ± 13.8 | 106.2 ± 15.2 | 107.2 ± 13.3 | 0.93 | 107.8 ± 14.1 | 104.8 ± 15.1 | 106.9 ± 12.9 | 0.70 | |
| Socioeconomic status | Low | N/A | N/A | N/A | 6 (21.4%) a,b | 13 (31.7%) b | 1 (3.0%) a | <0.001 | |
| Mid–Low | N/A | N/A | N/A | 14 (50.0%) | 21 (51.2%) | 11 (33.3%) | |||
| Mid–High | N/A | N/A | N/A | 7(25.0%) a,b | 7 (17.1%) b | 14 (42.4%) a | |||
| High | N/A | N/A | N/A | 1 (3.6%) a,b | 0 (0.0%) b | 7 (21.3%) a | |||
| Place of residence | Urban | 23 (48.9%) a | 14 (29.2%) a,b | 9 (24.3%) b | 0.037 | 18 (62.1%) a | 13 (33.3%) a,b | 9 (27.3%) b | 0.012 |
| Rural | 24 (51.1%) a | 34 (70.8%) a,b | 28 (75.7%) b | 11 (37.9%) a | 26 (66.7%) a,b | 24 (72.7%) b | |||
| Siblings | 0 | 21 (44.7%) | 25 (52.1%) | 20 (54.1%) | 0.65 | 9 (31.0%) | 16 (39.0%) | 12 (36.4%) | 0.79 |
| ≥1 | 26 (55.3%) | 23 (47.9%) | 17 (45.9%) | 20 (69.0%) | 25 (61.0%) | 21 (63.6%) | |||
| Gestational age (weeks) | 40 (39–41) | 40 (39–40) | 40 (39–41) | 0.50 | 40 (39–41) | 40 (37.5–40.5) | 40 (38.5–41) | 0.67 | |
| Newborn characteristics | |||||||||
| Newborn weight (g) | 3350.1 ± 413.7 | 3241.5 ± 434.4 | 3395.7 ± 381.1 | 0.20 | 3344.8 ± 462.6 | 3297.3 ± 569.0 | 3374.2 ± 392.6 | 0.74 | |
| Newborn length (cm) | 51 (49.5–52) | 50.5 (49–52) | 51 (50–52) | 0.52 | 51 (49.2–52.9) | 51 (49–52) | 51 (50–52) | 0.70 | |
| Newborn HC (cm) | 34.5 (34–36) | 34 (34–35) | 35 (33.8–35) | 0.15 | 35 (34–35.7) | 34 (33.5–35) | 35 (33.6–35.7) | 0.25 | |
| Newborn Gender | Boy | 27 (57.4%) | 29 (60.4%) | 15 (40.5%) | 0.16 | 18 (62.1%) | 25 (61.0%) | 13 (39.4%) | 0.06 |
| Girl | 20 (42.6%) | 19 (39.6%) | 22 (59.5%) | 11 (37.9%) | 16 (39.0%) | 20 (60.6%) | |||
| Breastfeeding lactation (days) | 10 (0–21) a | 11.5 (0.5–25) a | 420 (270–540) b | <0.001 | 15 (5–43.5) a | 14 (2.5–29.5) a | 390 (270–765) b | <0.001 | |
| CBCL Scales | 18 Months | 2.5 Years Old | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SF (n = 47) | EF (n = 48) | BF (n = 37) | Fisher’s Exact Test | p1 | SF (n = 29) | EF (n = 41) | BF (n = 33) | Fisher’s Exact Test | p1 | ||
| Internalizing Problems | Normal | 41 (87.2%) | 41 (85.4%) | 33 (89.2%) | 2.606 | 0.65 | 17 (58.7%) | 33 (80.5%) | 28 (84.9%) | 9.516 | 0.042 |
| Borderline | 5 (10.6%) | 3 (6.3%) | 3 (8.1%) | 7 (24.1%) a | 6 (14.6%) a,b | 1 (3.0%) b | |||||
| Pathology | 1 (2.1%) | 4 (8.3%) | 1 (2.7%) | 5 (17.2%) | 2 (4.9%) | 4 (12.1%) | |||||
| Externalizing Problems | Normal | 39 (83.0%) | 41 (85.4%) | 32 (86.5%) | 4.220 | 0.37 | 22 (75.9%) | 36 (87.8%) | 29 (87.9%) | 6.470 | 0.15 |
| Borderline | 5 (10.6%) | 3 (6.3%) | 5 (13.5%) | 1 (3.4%) | 3 (7.3%) | 3 (9.1%) | |||||
| Pathology | 3 (6.4%) | 4 (8.3%) | 0 (0.0%) | 6 (20.7%) | 2 (4.9%) | 1 (3.0%) | |||||
| Total Problems | Normal | 40 (85.1%) | 39 (81.3%) | 31 (83.8%) | 1.659 | 0.83 | 19 (65.5%) | 33 (80.5%) | 28 (84.8%) | 6.970 | 0.13 |
| Borderline | 5 (10.6%) | 4 (8.3%) | 4 (10.8%) | 3 (10.3%) | 6 (14.6%) | 2 (6.1%) | |||||
| Pathology | 2 (4.3%) | 5 (10.4%) | 2 (5.4%) | 7 (24.2%) | 2 (4.9%) | 3 (9.1%) | |||||
| Affective Problems | Normal | 45 (95.7%) | 42 (87.5%) | 35 (94.6%) | 4.386 | 0.35 | 25 (86.2%) | 40 (97.6%) | 28 (84.8%) | 8.491 | 0.026 |
| Borderline | 2 (4.3%) | 2 (4.2%) | 1 (2.7%) | 0 (0.0%) | 1 (2.4%) | 3 (9.1%) | |||||
| Pathology | 0 (0.0%) | 4 (8.3%) | 1 (2.7%) | 4 (13.8%) a | 0 (0.0%) b | 2 (6.1%) a,b | |||||
| Anxiety Problems | Normal | 46 (97.9%) | 46 (95.8%) | 35 (94.6%) | 1.948 | 0.94 | 24 (82.8%) | 36 (87.8%) | 29 (87.9%) | 1.700 | 0.92 |
| Borderline | 1 (2.1%) | 1 (2.1%) | 1 (2.7%) | 1 (3.4%) | 1 (2.4%) | 0 (0.0%) | |||||
| Pathology | 0 (0.0%) | 1 (2.1%) | 1 (2.7%) | 4 (13.8%) | 4 (9.8%) | 4 (12.1%) | |||||
| Perv. Develop. Problems | Normal | 44 (93.6%) | 43 (89.6%) | 33 (89.2%) | 2.027 | 0.78 | 23 (79.3%) | 34 (82.9%) | 32 (97.0%) | 5.207 | 0.25 |
| Borderline | 1 (2.1%) | 3 (6.3%) | 1 (2.7%) | 4 (13.7%) | 4 (9.8%) | 1 (3.0%) | |||||
| Pathology | 2 (4.3%) | 2 (4.2%) | 3 (8.1%) | 2 (6.9%) | 3 (7.3%) | 0 (0.0%) | |||||
| ADHD | Normal | 44 (93.6%) | 46 (95.8%) | 35 (94.6%) | 1.100 | 0.97 | 26 (89.7%) | 39 (95.2%) | 33 (100%) | 3.589 | 0.46 |
| Borderline | 2 (4.3%) | 1 (2.1%) | 1 (2.7%) | 1 (3.4%) | 1 (2.4%) | 0 (0.0%) | |||||
| Pathology | 1 (2.1%) | 1 (2.1%) | 1 (2.7%) | 2 (6.9%) | 1 (2.4%) | 0 (0.0%) | |||||
| Op. Def. Problems | Normal | 45 (95.7%) | 46 (95.8%) | 37 (100%) | 3.118 | 0.78 | 28 (96.5%) | 37 (90.3%) | 32 (97.0%) | 2.397 | 0.85 |
| Borderline | 2 (4.3%) | 1 (2.1%) | 0 (0.0%) | 0 (0.0%) | 1 (2.4%) | 0 (0.0%) | |||||
| Pathology | 0 (0.0%) | 1 (2.1%) | 0 (0.0%) | 1 (3.5%) | 3 (7.3%) | 1 (3.0%) | |||||
| CBCL Scales | 18 Months | 2.5 Years | F(df) | p1 | p2 | p3 | ηp2 | |
|---|---|---|---|---|---|---|---|---|
| Internalizing Problems | SF | 8.7 ± 4.6 | 12.6 ± 9.9 a | 3.041(2,98) | 0.011 | 0.16 | 0.047 | 0.058 |
| EF | 8.0 ± 6.7 | 9.0 ± 6.0 a,b | ||||||
| BF | 6.8 ± 5.5 | 7.5 ± 6.0 b | ||||||
| Externalizing Problems | SF | 14.6 ± 6.2 | 16.9 ± 7.9 a | 3.885(2,98) | 0.77 | 0.13 | 0.024 | 0.073 |
| EF | 12.5 ± 6.9 | 12.2 ± 6.8 b | ||||||
| BF | 12.4 ± 6.6 | 11.1 ± 7.7 b | ||||||
| Total Problems | SF | 37.9 ± 13.9 | 46.1 ± 26.3 a | 3.222(2,98) | 0.15 | 0.16 | 0.044 | 0.062 |
| EF | 33.0 ± 21.3 | 34.4 ± 17.5 a,b | ||||||
| BF | 32.2 ± 16.9 | 31.1 ± 19.6 b | ||||||
| Affective Problems | SF | 2.6 ± 1.5 | 3.4 ± 2.6 | 0.403(2,98) | 0.14 | 0.07 | 0.67 | 0.008 |
| EF | 2.8 ± 2.9 | 2.4 ± 1.6 | ||||||
| BF | 2.2 ± 1.8 | 2.9 ± 2.2 | ||||||
| Anxiety Problems | SF | 3.6 ± 1.7 | 4.7 ± 3.0 | 0.500(2,98) | 0.005 | 0.34 | 0.61 | 0.010 |
| EF | 3.3 ± 2.2 | 4.2 ± 3.0 | ||||||
| BF | 3.5 ± 2.2 | 3.7 ± 3.0 | ||||||
| Perv. Develop. Problems | SF | 3.5 ± 2.5 | 4.4 ± 3.7 | 1.710(2,98) | 0.25 | 0.42 | 0.19 | 0.034 |
| EF | 3.3 ± 3.5 | 3.8 ± 3.0 | ||||||
| BF | 3.0 ± 2.6 | 2.8 ± 2.1 | ||||||
| ADHD | SF | 5.8 ± 2.5 | 6.1 ± 2.6 a | 3.442(2,98) | 0.11 | 0.06 | 0.036 | 0.066 |
| EF | 4.9 ± 2.3 | 4.6 ± 2.7 a,b | ||||||
| BF | 5.2 ± 2.6 | 3.9 ± 2.7 b | ||||||
| Op. Def. Problems | SF | 3.6 ± 2.1 | 4.5 ± 2.0 a | 3.630(2,98) | 0.034 | 0.39 | 0.030 | 0.069 |
| EF | 2.9 ± 1.8 | 3.5 ± 2.5 a,b | ||||||
| BF | 2.9 ± 1.9 | 2.9 ± 2.3 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieto-Ruiz, A.; Diéguez, E.; Sepúlveda-Valbuena, N.; Herrmann, F.; Cerdó, T.; López-Torrecillas, F.; De-Castellar, R.; Jiménez, J.; Pérez-García, M.; Miranda, M.T.; et al. The Effects of an Infant Formula Enriched with Milk Fat Globule Membrane, Long-Chain Polyunsaturated Fatty Acids and Synbiotics on Child Behavior up to 2.5 Years Old: The COGNIS Study. Nutrients 2020, 12, 3825. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123825
Nieto-Ruiz A, Diéguez E, Sepúlveda-Valbuena N, Herrmann F, Cerdó T, López-Torrecillas F, De-Castellar R, Jiménez J, Pérez-García M, Miranda MT, et al. The Effects of an Infant Formula Enriched with Milk Fat Globule Membrane, Long-Chain Polyunsaturated Fatty Acids and Synbiotics on Child Behavior up to 2.5 Years Old: The COGNIS Study. Nutrients. 2020; 12(12):3825. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123825
Chicago/Turabian StyleNieto-Ruiz, Ana, Estefanía Diéguez, Natalia Sepúlveda-Valbuena, Florian Herrmann, Tomás Cerdó, Francisca López-Torrecillas, Roser De-Castellar, Jesús Jiménez, Miguel Pérez-García, María T. Miranda, and et al. 2020. "The Effects of an Infant Formula Enriched with Milk Fat Globule Membrane, Long-Chain Polyunsaturated Fatty Acids and Synbiotics on Child Behavior up to 2.5 Years Old: The COGNIS Study" Nutrients 12, no. 12: 3825. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123825