Ayurvedic Herbal Preparation Supplementation Does Not Improve Metabolic Health in Impaired Glucose Tolerance Subjects; Observations from a Randomised Placebo Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Subjects
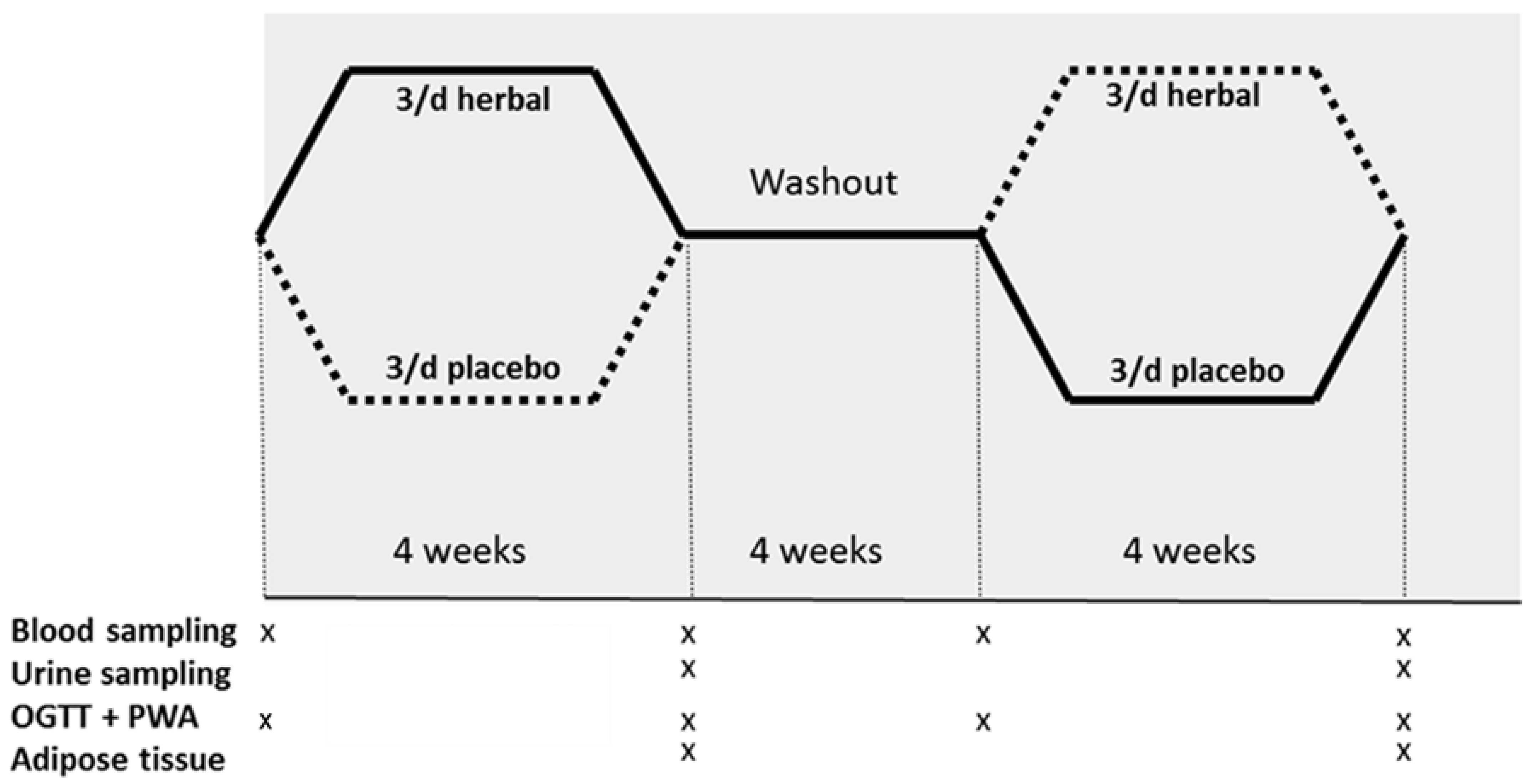
2.3. Study Design
2.4. Herbal and Placebo Supplement
2.5. Metabolic Parameters and Differentiated Leukocyte Count
2.6. Measures of Vascular Function
2.7. Adipose Tissue Collection and RNA Isolation
2.8. Microarray Processing and Analysis
2.9. Urinary Metabolomics
2.10. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Metabolic Parameters and Differentiated Leukocyte Count
3.3. Measures of Vascular Function
3.4. Urine Metabolites
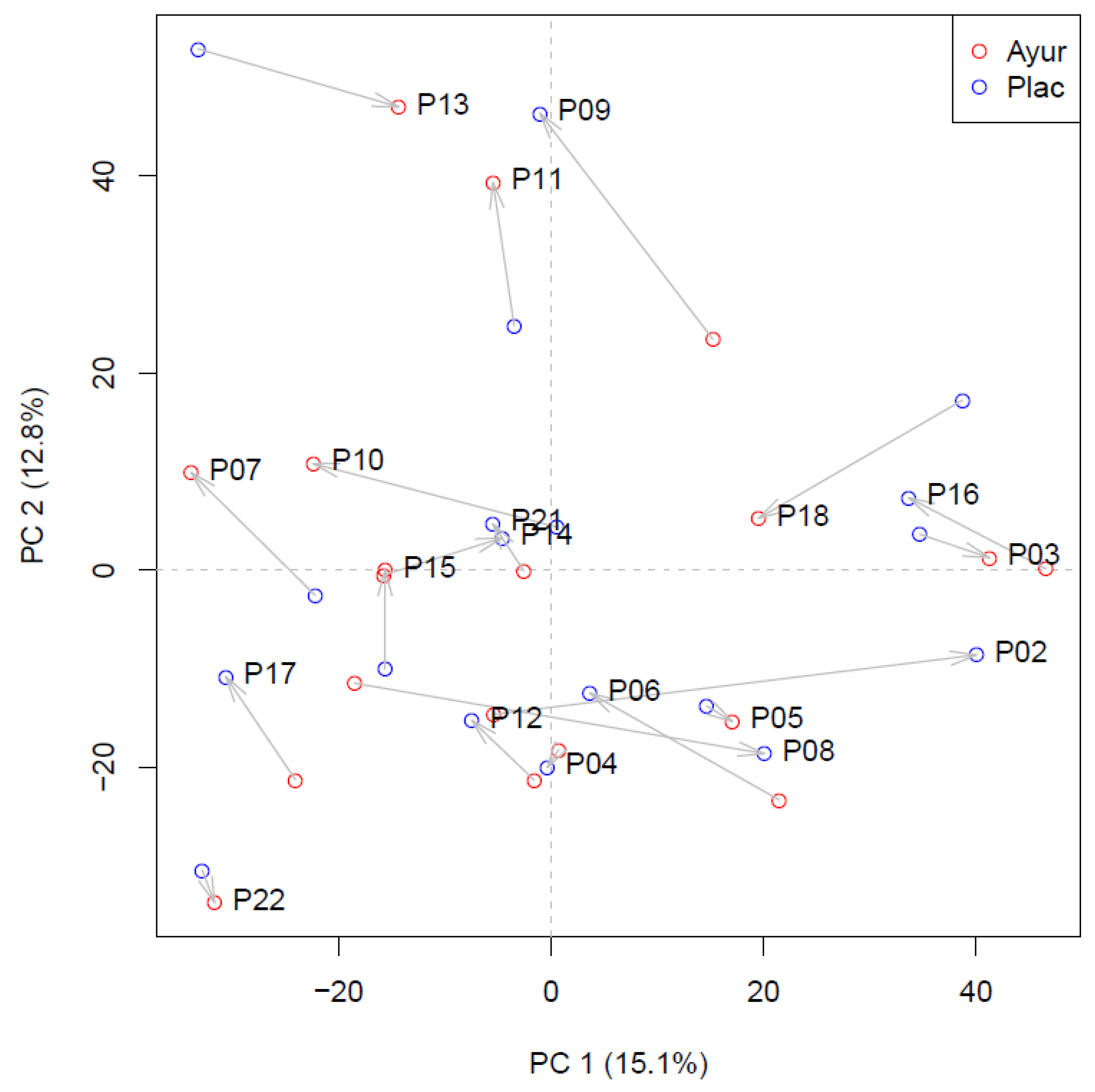
3.5. Whole Genome Adipose Tissue Gene Expression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smyth, S.; Heron, A. Diabetes and obesity: The twin epidemics. Nat. Med. 2006, 12, 75–80. [Google Scholar] [CrossRef]
- Fabricant, D.S.; Farnsworth, N.R. The value of plants used in traditional medicine for drug discovery. Environ. Health Perspect. 2001, 109, 69–75. [Google Scholar] [PubMed]
- Virdi, J.; Sivakami, S.; Shahani, S.; Suthar, A.C.; Banavalikar, M.M.; Biyani, M.K. Antihyperglycemic effects of three extracts from Momordica charantia. J. Ethnopharmacol. 2003, 88, 107–111. [Google Scholar] [CrossRef]
- Gray, A.M.; Flatt, P.R. Insulin-releasing and insulin-like activity of the traditional anti-diabetic plant Coriandrum sativum (coriander). Br. J. Nutr. 1999, 81, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomotake, H.; Shimaoka, I.; Kayashita, J.; Yokoyama, F.; Nakajoh, M.; Kato, N. Stronger Suppression of Plasma Cholesterol and Enhancement of the Fecal Excretion of Steroids by a Buckwheat Protein Product than by a Soy Protein Isolate in Rats Fed on a Cholesterol-free Diet. Biosci. Biotechnol. Biochem. 2001, 65, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Naik, P.R.; Mohammadi, J. Evaluation of hypoglycemic effect of Morus alba in an animal model. Indian J. Pharmacol. 2008, 40, 15–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahramikia, S.; Yazdanparast, R. Effect of hydroalcoholic extracts of Nasturtium officinale leaves on lipid profile in high-fat diet rats. J. Ethnopharmacol. 2008, 115, 116–121. [Google Scholar] [CrossRef]
- Sridharan, K.; Mohan, R.; Ramaratnam, S.; Panneerselvam, D. Ayurvedic treatments for diabetes mellitus. Cochrane Database Syst. Rev. 2011, CD008288. [Google Scholar] [CrossRef] [Green Version]
- Van Duynhoven, J.; van der Hooft, J.J.; van Dorsten, F.A.; Peters, S.; Foltz, M.; Gomez-Roldan, V.; Vervoort, J.; de Vos, R.C.H.; Jacobs, D.M. Rapid and sustained systemic circulation of conjugated gut microbial catabolites after single-dose black tea extract consumption. J. Proteome Res. 2014, 13, 2668–2678. [Google Scholar] [CrossRef]
- Van Der Hooft, J.J.; de Vos, R.C.H.; Mihaleva, V.; Bino, R.J.; Ridder, L.; de Roo, N.; Jacobs, D.M.; van Duynhoven, J.P.M.; Vervoort, J. Structural Elucidation and Quantification of Phenolic Conjugates Present in Human Urine after Tea Intake. Anal. Chem. 2012, 84, 7263–7271. [Google Scholar] [CrossRef]
- Saper, R.; Kales, S.N.; Paquin, J.; Burns, M.J.; Eisenberg, D.M.; Davis, R.B.; Phillips, R.S. Heavy Metal Content of Ayurvedic Herbal Medicine Products. JAMA 2004, 292, 2868. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-S.; Li, Y.-Y.; Weng, L.-J.; Zhou, C.-X.; He, Q.-J.; Lou, Y.-J. A Fraction ofAcorus calamus L. extract devoid of β-asarone Enhances adipocyte differentiation in 3T3-L1 cells. Phytother. Res. 2007, 21, 562–564. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-S.; Zhu, D.-F.; Zhou, C.-X.; Feng, C.-R.; Lou, Y.-J.; Yang, B.; He, Q.-J. Insulin sensitizing activity of ethyl acetate fraction of Acorus calamus L. in vitro and in vivo. J. Ethnopharmacol. 2009, 123, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Yokozawa, T.; Cho, E.J.; Cheigh, H.S.; Choi, J.S.; Chung, H.Y. In Vitro and in vivo antioxidant effects of mustard leaf (Brassica juncea). Phytother. Res. 2003, 17, 465–471. [Google Scholar] [CrossRef]
- Yokozawa, T.; Kim, H.Y.K.; Cho, E.J.; Yamabe, N.; Choi, J.S. Protective Effects of Mustard Leaf (Brassica juncea) against Diabetic Oxidative Stress. J. Nutr. Sci. Vitaminol. 2003, 49, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Roman-Ramos, R.; Almanza-Perez, J.C.; Fortis-Barrera, A.; Angeles-Mejia, S.; Banderas-Dorantes, T.R.; Zamilpa-Alvarez, A.; Diaz-Flores, M.; Jasso, I.; Blancas-Flores, G.; Gomez, J.; et al. Antioxidant and Anti-Inflammatory Effects of a Hypoglycemic Fraction fromCucurbita ficifoliaBouché in Streptozotocin-Induced Diabetes Mice. Am. J. Chin. Med. 2012, 40, 97–110. [Google Scholar] [CrossRef]
- Xia, T.; Wang, Q. Antihyperglycemic effect of Cucurbita ficifolia fruit extract in streptozotocin-induced diabetic rats. Fitoterapia 2006, 77, 530–533. [Google Scholar] [CrossRef]
- Lee, C.-C.; Hsu, W.-H.; Shen, S.-R.; Cheng, Y.-H.; Wu, S.-C. Fagopyrum tataricum(Buckwheat) Improved High-Glucose-Induced Insulin Resistance in Mouse Hepatocytes and Diabetes in Fructose-Rich Diet-Induced Mice. Exp. Diabetes Res. 2012, 2012, 375673. [Google Scholar] [CrossRef] [Green Version]
- Hong, H.; Maeng, W.J. Effects of Malted Barley Extract and Banaba Extract on Blood Glucose Levels in Genetically Diabetic Mice. J. Med. Food 2004, 7, 487–490. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.-M.; Chang, W.-C.; Chang, C.-T.; Hsieh, C.-L.; Tsai, C.E. Effects of young barley leaf extract and antioxidative vitamins on LDL oxidation and free radical scavenging activities in type 2 diabetes. Diabetes Metab. 2002, 28, 107–114. [Google Scholar]
- Hasanein, P.; Shahidi, S. Effects of Hypericum perforatum extract on diabetes-induced learning and memory impairment in rats. Phytother. Res. 2010, 25, 544–549. [Google Scholar] [CrossRef]
- Dorman, H.J.D.; Koşar, M.; Kahlos, K.; Holm, A.Y.; Hiltunen, R. Antioxidant Properties and Composition of Aqueous Extracts from Mentha Species, Hybrids, Varieties, and Cultivars. J. Agric. Food Chem. 2003, 51, 4563–4569. [Google Scholar] [CrossRef] [PubMed]
- Fuangchan, A.; Sonthisombat, P.; Seubnukarn, T.; Chanouan, R.; Chotchaisuwat, P.; Sirigulsatien, V.; Ingkaninan, K.; Plianbangchang, P.; Haines, S.T. Hypoglycemic effect of bitter melon compared with metformin in newly diagnosed type 2 diabetes patients. J. Ethnopharmacol. 2011, 134, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Kameswararao, B.; Kesavulu, M.; Chippada, A.R. Evaluation of antidiabetic effect of Momordica cymbalaria fruit in alloxan-diabetic rats. Fitoterapia 2003, 74, 7–13. [Google Scholar] [CrossRef]
- Hansawasdi, C.; Kawabata, J. α-Glucosidase inhibitory effect of mulberry (Morus alba) leaves on Caco-2. Fitoterapia 2006, 77, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Sudha, P.; Zinjarde, S.S.; Bhargava, S.Y.; Kumar, A.R. Potent α-amylase inhibitory activity of Indian Ayurvedic medicinal plants. BMC Complement. Altern. Med. 2011, 11. [Google Scholar] [CrossRef] [Green Version]
- Yazdanparast, R.; Bahramikia, S.; Ardestani, A. Nasturtium officinale reduces oxidative stress and enhances antioxidant capacity in hypercholesterolaemic rats. Chem.-Biol. Interact. 2008, 172, 176–184. [Google Scholar] [CrossRef]
- Fararh, K.; Atoji, Y.; Shimizu, Y.; Takewaki, T. Isulinotropic properties of Nigella sativa oil in Streptozotocin plus Nicotinamide diabetic hamster. Res. Vet. Sci. 2002, 73, 279–282. [Google Scholar] [CrossRef]
- Liang, C.-H.; Chan, L.-P.; Ding, H.-Y.; So, E.C.; Lin, R.-J.; Wang, H.-M.; Chen, Y.-G.; Chou, T.-H. Free Radical Scavenging Activity of 4-(3,4-Dihydroxybenzoyloxymethyl)phenyl-O-β-d-glucopyranoside from Origanum vulgare and Its Protection against Oxidative Damage. J. Agric. Food Chem. 2012, 60, 7690–7696. [Google Scholar] [CrossRef]
- Jain, S.; Bhatia, G.; Barik, R.; Kumar, P.; Jain, A.; Dixit, V.K. Antidiabetic activity of Paspalum scrobiculatum Linn. in alloxan induced diabetic rats. J. Ethnopharmacol. 2010, 127, 325–328. [Google Scholar] [CrossRef]
- Bakırel, T.; Bakırel, U.; Keleş, O.Ü.; Ülgen, S.G.; Yardibi, H. In vivo assessment of antidiabetic and antioxidant activities of rosemary (Rosmarinus officinalis) in alloxan-diabetic rabbits. J. Ethnopharmacol. 2008, 116, 64–73. [Google Scholar] [CrossRef]
- Eidi, M.; Eidi, A.; Zamanizadeh, H. Effect of Salvia officinalis L. leaves on serum glucose and insulin in healthy and streptozotocin-induced diabetic rats. J. Ethnopharmacol. 2005, 100, 310–313. [Google Scholar] [CrossRef]
- Lima, C.F.; Azevedo, M.F.; Araujo, R.; Fernandes-Ferreira, M.; Pereira-Wilson, C. Metformin-like effect of Salvia officinalis (common sage): Is it useful in diabetes prevention? Br. J. Nutr. 2006, 96, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Gupta, R.; Lal, B. Effect of Trigonella foenum-graecum (fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes mellitus: A double blind placebo controlled study. J. Assoc. Physicians India 2001, 49, 1057–1061. [Google Scholar]
- Kumar, P.; Taha, A.; Kale, R.K.; McLean, P.; Baquer, N.Z. Beneficial effects of Trigonella foenum graecum and sodium orthovanadate on metabolic parameters in experimental diabetes. Cell Biochem. Funct. 2012, 30, 464–473. [Google Scholar] [CrossRef]
- Esser, D.; van Dijk, S.J.; Oosterink, E.; Müller, M.; Afman, L.A. A High-Fat SFA, MUFA, or n3 PUFA Challenge Affects the Vascular Response and Initiates an Activated State of Cellular Adherence in Lean and Obese Middle-Aged Men. J. Nutr. 2013, 143, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.; Kools, H.; de Groot, P.J.; Gavai, A.K.; Basnet, R.K.; Cheng, F.; Wu, J.; Wang, X.; Lommen, A.; Hooiveld, G.J.E.J.; et al. MADMAX—Management and analysis database for multiple ~ Omics experiments. J. Integr. Bioinform. 2011, 8. [Google Scholar] [CrossRef]
- Dai, M.; Wang, P.; Boyd, A.D.; Kostov, G.; Athey, B.; Jones, E.G.; Bunney, W.E.; Myers, R.M.; Speed, T.P.; Akil, H.; et al. Evolving gene/transcript definitions significantly alter the interpretation of GeneChip data. Nucleic Acids Res. 2005, 33, e175. [Google Scholar] [CrossRef] [Green Version]
- Bolstad, B.M.; Irizarry, R.M.; Åstrand, M.; Speed, T.P. A comparison of normalization methods for high density oligonucleotide array data based on variance and bias. Bioinformatics 2003, 19, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Irizarry, R.A.; Bolstad, B.M.; Collin, F.; Cope, L.M.; Hobbs, B.; Speed, T.P. Summaries of Affymetrix GeneChip probe level data. Nucleic Acids Res. 2003, 31, 15e. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Treuren, R.; van Eekelen, H.D.L.M.; Wehrens, R.; de Vos, R.C.H. Metabolite variation in the lettuce gene pool: Towards healthier crop varieties and food. Metabolomics 2018, 14, 146. [Google Scholar] [CrossRef] [Green Version]
- Purves, R.D. Optimum numerical integration methods for estimation of area-under-the-curve (AUC) and area-under-the-moment-curve (AUMC). J. Pharmacokinet. Biopharm. 1992, 20, 211–226. [Google Scholar] [CrossRef]
- Smyth, G.K. Linear Models and Empirical Bayes Methods for Assessing Differential Expression in Microarray Experiments. Stat. Appl. Genet. Mol. Biol. 2004, 3, 1–25. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Hastie, T.; Friedman, J.H.; Tibshirani, R. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2001; Volume XVI, p. 533. [Google Scholar]
- Martens, H.; Næs, T. Multivariate Calibration; Wiley: Chichester, UK; New York, NY, USA, 1989; Volume XVII, p. 419. [Google Scholar]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Lee, Y.H.; Nair, S.; Rousseau, E.; Allison, D.B.; Page, G.P.; Tataranni, P.A.; Bogardus, C.; Permana, P.A. Microarray profiling of isolated abdominal subcutaneous adipocytes from obese vs non-obese Pima Indians: Increased expression of inflammation-related genes. Diabetologia 2005, 48, 1776–1783. [Google Scholar] [CrossRef] [Green Version]
- Henegar, C.; Tordjman, J.; Achard, V.; Lacasa, D.; Cremer, I.; Guerre-Millo, M.; Poitou, C.; Basdevant, A.; Stich, V.; Viguerie, N.; et al. Adipose tissue transcriptomic signature highlights the pathological relevance of extracellular matrix in human obesity. Genome Biol. 2008, 9, R14. [Google Scholar] [CrossRef]
- Vandanmagsar, B.; Youm, Y.-H.; Ravussin, A.; Galgani, J.E.; Stadler, K.; Mynatt, R.L.; Ravussin, E.; Stephens, J.M.; Dixit, V.D. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat. Med. 2011, 17, 179–188. [Google Scholar] [CrossRef]
- Ahuja, K.D.K.; Robertson, I.K.; Ball, M.J. Acute effects of food on postprandial blood pressure and measures of arterial stiffness in healthy humans. Am. J. Clin. Nutr. 2009, 90, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Esser, D.; Mars, M.; Oosterink, E.; Stalmach, A.; Müller, M.; Afman, L.A. Dark chocolate consumption improves leukocyte adhesion factors and vascular function in overweight men. FASEB J. 2013, 28, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, J.R.; Samaras, K.; Hayward, C.S.; Chisholm, D.J.; Campbell, L.V. Beneficial Postprandial Effect of a Small Amount of Alcohol on Diabetes and Cardiovascular Risk Factors: Modification by Insulin Resistance. J. Clin. Endocrinol. Metab. 2005, 90, 661–672. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Name of Herb (Part Used) | Common Name | % (of Total) | Potential Health Effect (Type of Sudy) |
|---|---|---|---|
| Acorus calamus (rhizome) | Sweet flag | 2 | Hypoglycaemic, increased glucose metabolism, decrease in TG, FFA, insulin sensitizer (in vitro, animal) [12,13] |
| Brassica juncea (seed) | Indian mustard | 2 | Hypoglycaemic, antioxidant (animal) [14,15] |
| Coriandrum sativum (seed) | Coriander | 9 | Hypoglycaemic (increased glucose oxidation, increased glyconeogensis), insulin-releasing and insulin-like activity (animal) [4] |
| Cucurbita ficifolia (fruit) | Siam pumpkin | 14 | Hypoglycaemic, increased insulin levels, antioxidant (animal) [16,17] |
| Fagopyrum esculentum (seed) | Buckwheat | 7 | Insulin sensitizing, antioxidant (animal) [18] |
| Hordeum vulgare (grain) | Barley | 7 | Hypoglycaemic (decreased activity of glucose-6-phosphatase), antioxidant (animal/human) [19,20] |
| Hypericum perforatum (leaf) | St John’s wort | 2 | Prevention of deleterious effects of diabetes (animal) [21] |
| Mentha aquatica (whole plant) | Watermint | 2 | Antioxidant (in vitro) [22] |
| Mentha crispa (whole plant) | Wrinkled-leaf mint | 2 | Antioxidant (in vitro) [22] |
| Mentha piperita (whole plant) | Peppermint | 2 | Antioxidant (in vitro) [22] |
| Menyanthes trifoliate (whole plant) | Buckbean | 2 | |
| Momordica charantia (fruit) | Bitter melon | 14 | Inhibition of α-glucosidase, sucrose, maltase, inhibition of porcine pancreatic α-amylase activity and reduced starch hydrolysis (in vitro) [23,24] |
| Morus alba (leaf and fruit) | White mulberry | 2 | Hypoglycaemic, hypolipidemic (animal/human) [25,26] |
| Nasturtium officinale (whole plant) | Watercress | 2 | Antioxidant (animal) [27] |
| Nigella sativa (seed) | Fennel flower | 5 | Hypoglycaemic, increase in serum insulin level (animal) [28] |
| Origanum vulgare (whole plant) | Oregano | 4 | Antioxidant (in vitro) [29] |
| Paspalum scrobiculatum (seed) | Kodo/Kodra millet | 7 | Hypoglycaemic, increase in serum insulin level, hypolipidemic, increased liver glycogen (animal) [30] |
| Rosmarinus officinalis (leaf and twig) | Rosemary | 2 | Hypoglycaemic, increased insulin levels and antioxidant (animal) [31] |
| Salvia officinalis (leaf and twig) | Common sage | 5 | Reduction of fasting plasma glucose (decreased gluconeogenesis, increased insulin sensitivity), increased plasma insulin levels (animal) [32,33] |
| Trigonellafoenum-graecum (seed) | Fenugreek | 9 | Increased peripheral glucose uptake, insulin-releasing, decreased gluconeogenesis/glycogenolysis, insulin sensitizing (animal/human) [34,35] |
| Mean ± SD (n = 19) | |
|---|---|
| Males/females | 12/7 |
| Age (y) | 64.2 ± 4.5 |
| BMI (kg/m2) | 30.9 ± 3.9 |
| Fasting glucose (mmol/L) | 5.3 ± 0.7 |
| Postprandial (2 h) glucose (mmol/L) | 8.9 ± 1.2 |
| Diastolic blood pressure (mmHg) | 74 ± 10 |
| Systolic blood pressure (mmHg) | 130 ± 24 |
| Intervention | p Value | ||||||
|---|---|---|---|---|---|---|---|
| Herbal | Placebo | Main | Interaction | ||||
| Before (W0) | ΔW4 | Before (W0) | ΔW4 | Intervention | Time (4 weeks) | Intervention × Time | |
| Markers of glucose metabolism | |||||||
| Fasting | |||||||
| Glucose (mmol/L) | 6.0 ± 0.8 | 0.0 ± 0.2 | 5.9 ± 0.8 | 0.1 ± 0.3 | 0.410 | 0.221 | 0.393 |
| Insulin (mU/L) | 13.1 ± 7.3 | 1.4 ± 4.0 | 15.6 ± 8.4 | −0.4 ± 3.8 | 0.054 | 0.269 | 0.054 |
| HOMA-IR | 3.4 ± 1.9 | 0.4 ± 1.1 | 4.0 ± 2.2 | 0.1 ± 1.0 | 0.051 | 0.254 | 0.056 |
| HbA1c (mmol/moL) | 40.2 ± 2.6 | 0.4 ± 0.8 | 39.9 ± 3.0 | 0.7 ± 1.1 | 0.559 | <0.001 | 0.590 |
| Response to 75 g OGTT | |||||||
| 2 h glucose (mmol/L) | 7.9 ± 2.3 | 0.4 ± 1.6 | 8.4 ± 2.3 | −0.2 ± 1.0 | 0.052 | 0.370 | 0.057 |
| 2 h insulin (mU/L) | 76.3 ± 40.9 | 10.9 ± 24.6 | 90.2 ± 52.1 | −3.7 ± 26.7 | 0.084 | 0.153 | 0.095 |
| iAUC Δ glucose (AU) | 277 ± 197 | 20 ± 77 | 333 ± 178 | −13 ± 81 | 0.162 | 0.389 | 0.167 |
| iAUC Δ insulin (AU) | 5873 ± 3602 | 569 ± 2141 | 6692 ± 4666 | 84 ± 2018 | 0.595 | 0.236 | 0.484 |
| Markers of vascular health | |||||||
| SBP (mmHg) | 126 ± 17 | 0 ± 8 | 127 ± 18 | 0 ± 9 | 0.811 | 0.996 | 0.807 |
| DBP (mmHg) | 73 ± 10 | 0 ± 4 | 73 ± 8 | 0 ± 4 | 0.970 | 0.576 | 0.980 |
| AIX (%) | 25 ± 6 | 0 ± 3 | 25 ± 6 | 1 ± 4 | 0.354 | 0.595 | 0.444 |
| Total cholesterol (mmol/L) | 5.8 ± 0.9 | −0.1 ± 0.4 | 5.8 ± 1.1 | 0.1 ± 0.5 | 0.255 | 0.678 | 0.255 |
| TG (mmol/L) | 1.6 ± 0.5 | 0.0 ± 0.4 | 1.7 ± 0.7 | 0.0 ± 0.4 | 0.618 | 0.804 | 0.618 |
| Leucocytes 109 (#/l) | 5.6 ± 13 | 0.2 ± 0.9 | 6.4 ± 2.2 | −0.4 ± 1.2 | 0.099 | 0.154 | 0.141 |
| Before | (W0) | After | (W4) | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Change in overall response | ||||||||||
| I | ΔT30 | ΔT60 | ΔT90 | ΔT120 | ΔT30 | ΔT60 | ΔT90 | ΔT120 | between interventions | |
| Glucose | Herbal | 2.6 ± 1.3 | 3.6 ± 2.1 | 2.6 ± 2.9 | 1.9 ± 2.2 | 2.9 ± 1.3 | 3.8 ± 2.7 | 3.0 ± 2.6 | 2.7 ± 2.3 | 0.49 |
| (mmol/L) | Placebo | 3.0 ± 1.5 | 3.7 ± 2.2 | 3.1 ± 2.3 | 2.5 ± 1.9 | 3.1 ± 1.4 | 3.3 ± 2.3 | 2.9 ± 2.9 | 2.0 ± 2.3 | |
| Insulin | Herbal | 34 ± 32 | 72 ± 64 | 61 ± 34 | 63 ± 37 | 39 ± 36 | 76 ± 62 | 73 ± 56 | 82 ± 48 | 0.44 |
| (mU/L) | Placebo | 43 ± 46 | 71 ± 54 | 77 ± 52 | 75 ± 49 | 51 ± 42 | 68 ± 40 | 71 ± 44 | 70 ± 41 | |
| SBP | Herbal | - | 1 ± 10 | - | −3 ± 12 | - | −2 ± 5 | - | −3 ± 8 | 0.40 |
| (mmHg) | Placebo | - | 0 ± 9 | - | −5 ± 9 | - | 0 ± 13 | - | 1 ± 16 | |
| DBP | Herbal | - | −2 ± 6 | - | −3 ± 5 | - | −3 ± 4 | - | −4 ± 3 | 0.78 |
| (mmHg) | Placebo | - | −2 ± 5 | - | −4 ± 4 | - | −3 ± 4 | - | −3 ± 5 | |
| AIX | Herbal | - | −5 ± 4 | - | −5 ± 4 | - | −5 ± 3 | - | −5 ± 4 | 0.79 |
| (%) | Placebo | - | −5 ± 4 | - | −5 ± 4 | - | −5 ± 5 | - | −5 ± 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esser, D.; Matualatupauw, J.; de Vos, R.C.H.; Wehrens, R.; van der Stappen, J.; van der Meer, I.; Afman, L.A. Ayurvedic Herbal Preparation Supplementation Does Not Improve Metabolic Health in Impaired Glucose Tolerance Subjects; Observations from a Randomised Placebo Controlled Trial. Nutrients 2021, 13, 260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010260
Esser D, Matualatupauw J, de Vos RCH, Wehrens R, van der Stappen J, van der Meer I, Afman LA. Ayurvedic Herbal Preparation Supplementation Does Not Improve Metabolic Health in Impaired Glucose Tolerance Subjects; Observations from a Randomised Placebo Controlled Trial. Nutrients. 2021; 13(1):260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010260
Chicago/Turabian StyleEsser, Diederik, Juri Matualatupauw, Ric C. H. de Vos, Ron Wehrens, Jos van der Stappen, Ingrid van der Meer, and Lydia A. Afman. 2021. "Ayurvedic Herbal Preparation Supplementation Does Not Improve Metabolic Health in Impaired Glucose Tolerance Subjects; Observations from a Randomised Placebo Controlled Trial" Nutrients 13, no. 1: 260. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13010260