
Higher Lipopolysaccharide Binding Protein and Chemerin Concentrations Were Associated with Metabolic Syndrome Features in Pediatric Subjects with Abdominal Obesity during a Lifestyle Intervention

 , and
, and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Lifestyle Intervention
2.2. Anthropometric, Clinical and Biochemical Measurements
2.3. Statistical Analyses
3. Results
3.1. Effect of Lifestyle Intervention
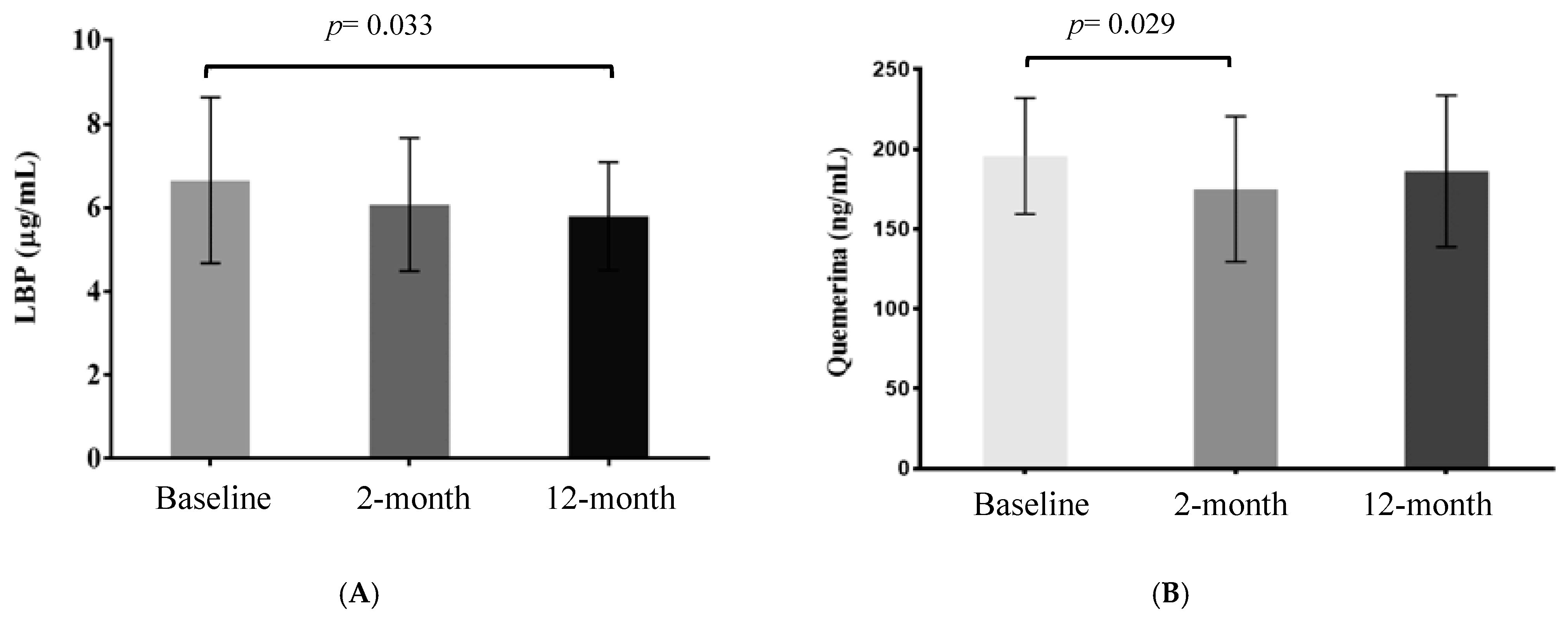
3.2. Effect of Lifestyle Intervention on Quemerin and LBP Plasma Levels
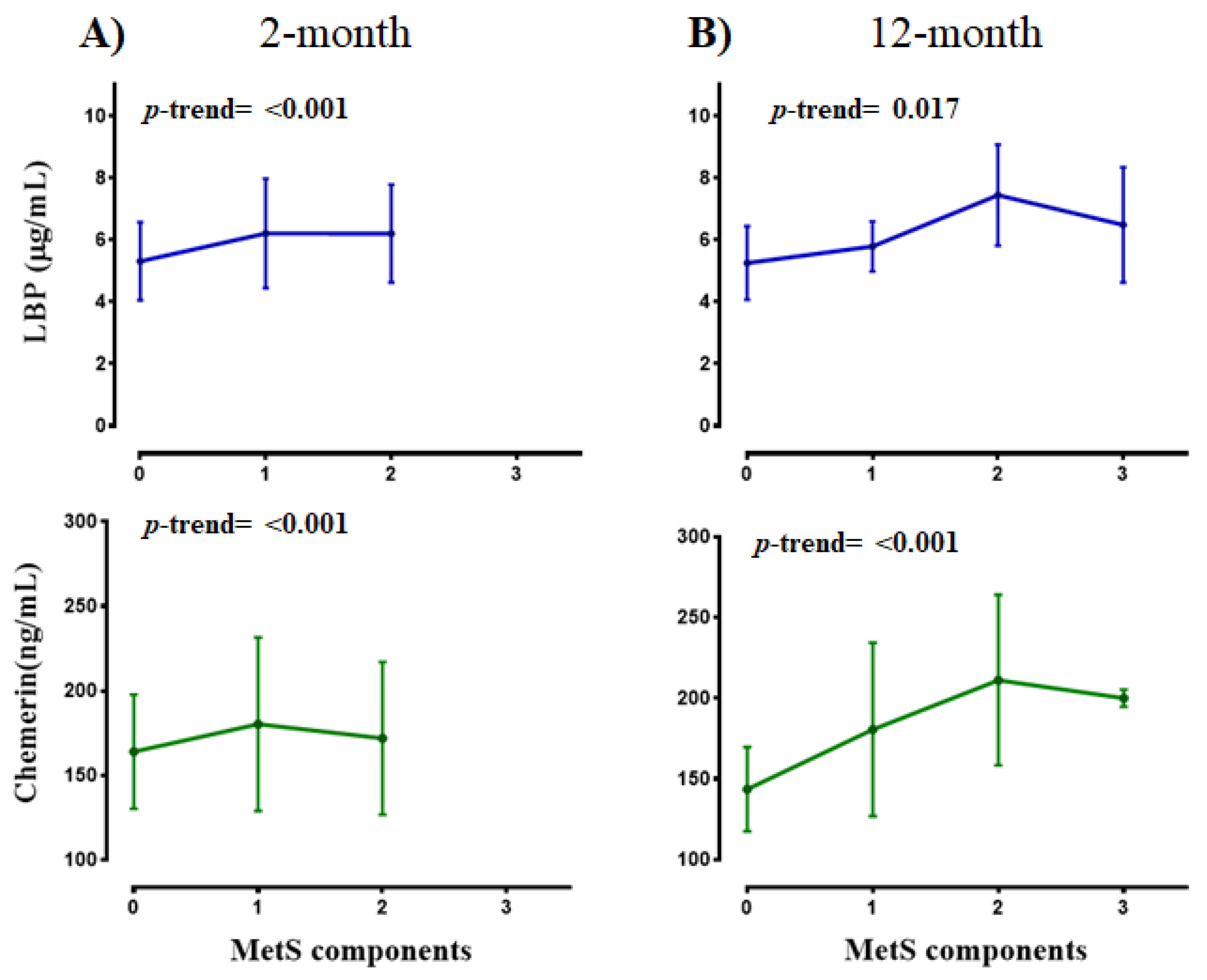
3.3. Associations between Adipokines and Metabolic Syndrome Features
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Obesity and Overweight. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 14 June 2020).
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, X.; Chen, R.; Ouyang, Q.; Lin, X.; Ai, Z.; Zhang, Y.; Yang, X. Novel associations of serum adropin and lipopolysaccharide-binding protein versus lipid profiles in childhood obesity. J. Pediatric Endocrinol. Metab. 2020, 33, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Fontes, V.S.; Neves, F.S.; Cândido, A.P.C. Quemerina E Fatores Relacionados Ao Risco Cardiovascular Em Crianças E Adolescentes: Uma Revisão Sistemática. Rev. Paul. Pediatr. 2018, 36, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuan, R.; Kumser, S.; Kant, R. An update on metabolic syndrome: Metabolik risk markers and adipokines in the development of metabolic syndrome. Diabetes Metab. Syndr. 2019, 13, 2409–2419. [Google Scholar]
- Zubut, A.; Agoston-Coloba, L.; Mocan, T.; Bocsan, I.C.; Mocan, L. Biomarkers in Metabolic Syndrome. In Ultimate Guide to Insulin; (Books on Demand); IntechOpen Limited: London, UK, 2018. [Google Scholar]
- Bozaoglu, K.; Bolton, K.; Mcmillan, J.; Zimmet, P.; Jowett, J.; Collier, G.; Walder, K.; Segal, D. Chemerin Is a Novel Adipokine Associated with Obesity and Metabolic Syndrome. Endocrinology 2007, 148, 4533–5129. [Google Scholar] [CrossRef] [PubMed]
- Bozaoglu, K.; Segal, D.; Shields, K.A.; Cummings, N.; Curran, J.E.; Comuzzie, A.G.; Mahaney, M.C.; Rainwater, D.L.; VandeBerg, J.L.; MacCluer, J.W.; et al. Chemerin is associated with metabolic syndrome phenotypes in a Mexican-American population. J. Clin. Endocrinol. Metab. 2009, 94, 3085–3088. [Google Scholar] [CrossRef]
- Landgraf, K.; Friebe, D.; Ullrich, T.; Kratzsch, J.; Dittrich, K.; Herberth, G.; Adams, V.; Kiess, W.; Erbs, S.; Körner, A. Chemerin as a mediator between obesity and vascular inflammation in children. J. Clin. Endocrinol. Metab. 2012, 97, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Sledzińska, M.; Szlagatys-Sidorkiewicz, A.; Brzezinski, M.; Kaźmierska, K.; Sledziński, T.; Kamińska, B. Serum chemerin in children with excess body weight may be associated with ongoing metabolic complications—A pilot study. Adv. Med. Sci. 2017, 62, 383–386. [Google Scholar] [CrossRef]
- Hamza, R.T.; Elkabbany, Z.A.; Shedid, A.M.; Hamed, A.I.; Ebrahim, A.O. Serum Chemerin in Obese Children and Adolescents Before and After L-Carnitine Therapy: Relation to Nonalcoholic Fatty Liver Disease and Other Features of Metabolic Syndrome. Arch Med Res. 2016, 47, 541–549. [Google Scholar] [CrossRef]
- Daxer, J.; Herttrich, T.; Zhao, Y.Y.; Vogel, M.; Hiemisch, A.; Scheuermann, K.; Körner, A.; Kratzsch, J.; Kiess, W.; Quante, M. Nocturnal levels of chemerin and progranulin in adolescents: Influence of sex, body mass index, glucose metabolism and sleep. J. Pediatric Endocrinol. Metab. 2017, 30, 57–61. [Google Scholar] [CrossRef]
- Maghsoudi, Z.; Kelishadi, R.; Hosseinzadeh-Attar, M.J. Association of chemerin levels with anthropometric indexes and C-reactive protein in obese and non-obese adolescents. ARYA Atheroscler. 2015, 11, 102–108. [Google Scholar] [PubMed]
- Kim, K.E.; Cho, Y.S.; Baek, K.S.; Li, L.; Baek, K.H.; Kim, J.H.; Kim, H.S.; Sheen, Y.H. Lipopolysaccharide-binding protein plasma levels as a biomarker of obesity-related insulin resistance in adolescents. Korean J Pediatrics 2016, 59, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Katsura, T.; Takahara, M.; Miyashita, K.; Katakami, N. Plasma lipopolysaccharide binding protein level statistically mediates between body mass index and chronic microinflammation in Japanese patients with type 1 diabetes. Diabetol. Int. 2020, 11, 293–297. [Google Scholar] [CrossRef]
- Kopp, F.; Kupsch, S.; Schromm, A.B. Lipopolysaccharide-binding protein is bound and internalized by host cells and colocalizes with LPS in the cytoplasm: Implications for a role of LBP in intracellular LPS-signaling. Biochim. Biophys. Acta Mol. Cell Res. 2016, 1863, 660–672. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, L.; Yao, P.; Ma, Y.; Wang, F.; Jin, Q.; Ye, X.; Li, H.; Hu, F.B.; Sun, L.; et al. Lipopolysaccharide binding protein, obesity status and incidence of metabolic syndrome: A prospective study among middle-aged and older Chinese. Diabetologia 2014, 57, 1834–1841. [Google Scholar] [CrossRef] [Green Version]
- Niklowitz, P.; Rothermel, J.; Lass, N.; Barth, A.; Reinehr, T. Link between chemerin, central obesity, and parameters of the Metabolic Syndrome: Findings from a longitudinal study in obese children participating in a lifestyle intervention. Int. J. Obes. 2018, 42, 1743–1752. [Google Scholar] [CrossRef]
- Ojeda-Rodríguez, A.; Morell-Azanza, L.; Zalba, G.; Zazpe, I.; Azcona-SanJulián, M.C.; Marti, A. Associations of telomere length with two dietary quality indices after a lifestyle intervention in children with abdominal obesity: A randomized controlled trial. Pediatric Obes. 2020, 11, e12661. [Google Scholar] [CrossRef]
- Ojeda-Rodríguez, A.; Zazpe, I.; Morell-azanza, L.; Chueca, J. Improved Diet Quality and Nutrient Adequacy in Children and Adolescents with Abdominal Obesity after a Lifestyle Intervention. Nutrients 2018, 10, 1500. [Google Scholar] [CrossRef] [Green Version]
- Morell-Azanza, L.; Ojeda-Rodríguez, A.; Ochotorena-Elicegui, A.; Martín-Calvo, N.; Chueca, M.; Marti, A.; Azcona-San Julian, C. Changes in objectively measured physical activity after a multidisciplinary lifestyle intervention in children with abdominal obesity: A randomized control trial. BMC Pediatr. 2019, 19, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Serra Majem, L.; Aranceta, J.; Ribas, L.; Pérez, C.; García, R. Estudio enKid: Objetivos y Metodología; Crecimiento y desarrollo; Serra, L., Aranceta, J., Eds.; Estudio enKid.: Barcelona, Spain, 2002; Volume 4. [Google Scholar]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de Crecimiento de Bilbao. Curvas y tablas de Crecimiento [Estudio Transversal]; Fundación Faustino Orbegozo: Bilbao, Spain, 2011; pp. 1–35. [Google Scholar]
- Tanner, J.M.; Whitehouse, R.H. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch. Dis. Child. 1976, 51, 170–179. [Google Scholar] [CrossRef] [Green Version]
- Zimmet, P.; Alberti, K.G.; Kaufman, F.; Tajima, N.; Silink, M.; Arslanian, S.; Wong, G.; Bennett, P.; Shaw, J.; Caprio, S. The metabolic syndrome in children and adolescents—An IDF consensus report. Pediatric Diabetes 2007, 8, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Romeo, J.; Martinez-Gomez, D.; Esperanza Diaz, L.; Gómez-Martinez, S.; Marti, A.; Martin-Matillas, M.; Puertollano, M.A.; Veiga, O.L.; Martinez, J.A.; Wärnberg, J.; et al. Changes in cardiometabolic risk factors, appetite-controlling hormones and cytokines after a treatment program in overweight adolescents: Preliminary findings from the EVASYON study. Pediatric Diabetes 2011, 12, 372–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marti, A.; Morell-Azanza, L.; Rendo-Urteaga, T.; García-Calzón, S.; Ojeda-Rodríguez, A.; Martín-Calvo, N.; Moreno-Aliaga, M.J.; Martínez, J.A.; Azcona-San Julián, M.C. Serum and gene expression levels of CT-1, IL-6, and TNF-α after a lifestyle intervention in obese children. Pediatric Diabetes 2018, 19, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Rendo-Urteaga, T.; García-Calzón, S.; Martínez-Ansó, E.; Chueca, M.; Oyarzabal, M.; Azcona-Sanjulián, M.C.; Bustos, M.; Moreno-Aliaga, M.J.; Martínez, J.A.; Marti, A. Decreased cardiotrophin-1 levels are associated with a lower risk of developing the metabolic syndrome in overweight/obese children after a weight loss program. Metabolism 2013, 62, 1429–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinehr, T.; Lass, N.; Toschke, C.; Rothermel, J.; Lanzinger, S.; Holl, R.W. Which amount of BMI-SDS reduction is necessary to improve cardiovascular risk factors in overweight children? J. Clin. Endocrinol. Metab. 2016, 101, 3171–3179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajjo, T.; Almasri, J.; Al Nofal, A.; Farah, W.; Alsawas, M.; Ahmed, A.T.; Mohammed, K.; Kanwar, A.; Asi, N.; Wang, Z. The Association of Weight Loss and Cardiometabolic Outcomes in Obese Children: Systematic Review and Meta-regression. J. Clin. Endocrinol. Metab. 2016, 101, 4764–4768. [Google Scholar] [CrossRef]
- Hvidt, K.N.; Olsen, M.H.; Ibsen, H.; Holm, J.-C. Effect of changes in BMI and waist circumference on ambulatory blood pressure in obese children and adolescents. J. Hypertens. 2014, 32, 1470–1477. [Google Scholar] [CrossRef]
- Kolsgaard, M.L.P.; Joner, G.; Brunborg, C.; Anderssen, S.A.; Tonstad, S.; Andersen, L.F. Reduction in BMI z-score and improvement in cardiometabolic risk factors in obese children and adolescents. The Oslo Adiposity Intervention Study—A hospital/public health nurse combined treatment. BMC Pediatr. 2011, 11, 47. [Google Scholar] [CrossRef] [Green Version]
- Reinehr, T.; Andler, W. Changes in the atherogenic risk factor profile according to degree of weight loss. Arch. Dis. Child. 2004, 89, 419–422. [Google Scholar] [CrossRef] [Green Version]
- Siegrist, M.; Rank, M.; Wolfarth, B.; Langhof, H.; Haller, B.; Koenig, W.; Halle, M. Leptin, adiponectin, and short-term and long-term weight loss after a lifestyle intervention in obese children. Nutrition 2013, 29, 851–857. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Peris, E.; Wang, Y.; Tamae, M.; Khalyfa, A.; Carreras, A.; Gozal, D. Lipopolysaccharide-Binding Protein Plasma Levels in Children: Effects of Obstructive Sleep Apnea and Obesity. J. Clin. Endocrinol. Metab. 2014, 99, 656–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Navarrete, J.M.; Ortega, F.; Serino, M.; Luche, E.; Waget, A.; Pardo, G.; Salvador, J.; Ricart, W.; Frühbeck, G.; Burcelin, R.; et al. Circulating lipopolysaccharide-binding protein [LBP] as a marker of obesity-related insulin resistance. Int. J. Obes. 2012, 36, 1442–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.E.; Heo, J.S.; Han, S.; Kwon, S.K.; Kim, S.Y.; Kim, J.H.; Baek, K.H.; Sheen, Y.H. Blood concentrations of lipopolysaccharide-binding protein, high-sensitivity C-reactive protein, tumor necrosis factor-α and Interleukin-6 in relation to insulin resistance in young adolescents. Clin. Chim. Acta 2018, 486, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Velázquez-López, L.; Santiago-Díaz, G.; Nava-Hernández, J.; Muñoz-Torres, A.V.; Medina-Bravo, P.; Torres-Tamayo, M. Mediterranean-style diet reduces metabolic syndrome components in obese children and adolescents with obesity. BMC Pediatr. 2014, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ba, H.-J.; Xu, L.-L.; Qin, Y.-Z.; Chen, H.-S. Serum Chemerin Levels Correlate with Determinants of Metabolic Syndrome in Obese Children and Adolescents. Clin. Med. Insights Pediatrics 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Fontes, V.S.; Neves, F.S.; Cândido, A.P.C. Chemerin and factors related to cardiovascular risk in children and adolescents: A systematic review. Rev. Paul. Pediatr. 2018, 36, 221–229. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| At Baseline [n = 29] | 2-Month [n = 29] | 12-Month [n = 21] | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p1 | Mean | SD | p2 | |
| Body weight [kg] | 69.24 | 21.72 | 66.14 | 20.81 | <0.001 | 70.99 | 20.14 | <0.001 |
| Sex [F/M] | 15/14 | [52%/48%] | ||||||
| Height [cm] | 150.63 | 14.69 | 151.58 | 14.56 | <0.001 | 155.28 | 14.67 | <0.001 |
| BMI [kg/m2] | 29.67 | 5.21 | 27.96 | 4.98 | <0.001 | 28.73 | 5.37 | <0.001 |
| BMI-SDS | 3.05 | 1.09 | 2.46 | 1.11 | <0.001 | 2.59 | 1.29 | <0.001 |
| WC [cm] | 88.66 | 13.25 | 84.18 | 12.96 | <0.001 | 85.15 | 13.23 | <0.001 |
| WHR | 0.59 | 0.06 | 0.55 | 0.06 | <0.001 | 0.55 | 0.06 | <0.001 |
| HC [cm] | 101.12 | 14.28 | 98.35 | 13.99 | <0.001 | 101.29 | 14.57 | <0.001 |
| Fat mass [%] | 36.64 | 6.87 | 34.06 | 6.67 | <0.001 | 33.91 | 7.68 | 0.002 |
| Fat mass [kg] | 26.29 | 11.85 | 23.34 | 10.55 | <0.001 | 24.91 | 11.38 | <0.001 |
| Lean mass [kg] | 43.02 | 11.82 | 42.83 | 11.97 | 0.514 | 46.11 | 11.61 | <0.001 |
| Body water [kg] | 31.46 | 8.67 | 31.36 | 8.77 | 0.655 | 33.73 | 8.48 | <0.001 |
| SBP [mmHg] | 119.66 | 12.45 | 113.38 | 14.35 | <0.001 | 113.54 | 14.96 | 0.103 |
| DBP [mmHg] | 73.79 | 9.99 | 68.72 | 13.61 | 0.081 | 69.31 | 15.15 | 0.277 |
| Total-C [mg/dL] | 160.81 | 21.94 | 150.4 | 23.75 | 0.007 | 149.77 | 21.48 | 0.009 |
| LDL-C [mg/dL] | 98.24 | 17.69 | 92.27 | 20.36 | 0.045 | 88.60 | 18.55 | 0.007 |
| HDL-C [mg/dL] | 45.79 | 9.55 | 43.83 | 8.01 | 0.074 | 46.81 | 8.85 | 0.106 |
| Triglycerides [mg/dL] | 83.65 | 35.25 | 71.67 | 31.49 | 0.104 | 71.99 | 32.25 | 0.156 |
| Glucose [mg/dL] | 90.31 | 6.86 | 85.21 | 5.85 | <0.001 | 88.34 | 6.39 | <0.001 |
| Insulin [μU/mL] | 14.92 | 7.36 | 11.37 | 5.91 | 0.003 | 12.41 | 5.73 | 0.005 |
| Leptin [ng/mL] | 28.03 | 15.25 | 19.36 | 14.83 | 0.003 | 24.23 | 17.84 | 0.012 |
| Baseline [n = 29] | 2-Months [n = 29] | 12-Months [n = 21] | p | |
|---|---|---|---|---|
| MetS | 7 [24%] | 0 | 4 [19%] | 0.009 |
| MetS components | ||||
| WC ≥ 90th percentile | 29 [100%] | 25 [86%] | 17 [81%] | <0.001 |
| Triglycerides ≥ 150 mg/dL | 2 [7%] | 1 [3%] | 1 [5%] | 0.779 |
| HDL-C ≤ 40 mg/dL | 9 [31%] | 10 [35%] | 5 [24%] | 0.072 |
| Glucose ≥ 100 mg/dL | 5 [17%] | 0 [0%] | 1 [5%] | 0.030 |
| SBP ≥ 130 mmHg | 8 [28%] | 3 [10%] | 3 [14%] | 0.103 |
| DBP ≥ 85 mmHg | 6 [21%] | 2 [7%] | 2 [10%] | 0.135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marti, A.; Martínez, I.; Ojeda-Rodríguez, A.; Azcona-Sanjulian, M.C. Higher Lipopolysaccharide Binding Protein and Chemerin Concentrations Were Associated with Metabolic Syndrome Features in Pediatric Subjects with Abdominal Obesity during a Lifestyle Intervention. Nutrients 2021, 13, 289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020289
Marti A, Martínez I, Ojeda-Rodríguez A, Azcona-Sanjulian MC. Higher Lipopolysaccharide Binding Protein and Chemerin Concentrations Were Associated with Metabolic Syndrome Features in Pediatric Subjects with Abdominal Obesity during a Lifestyle Intervention. Nutrients. 2021; 13(2):289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020289
Chicago/Turabian StyleMarti, Amelia, Isabel Martínez, Ana Ojeda-Rodríguez, and María Cristina Azcona-Sanjulian. 2021. "Higher Lipopolysaccharide Binding Protein and Chemerin Concentrations Were Associated with Metabolic Syndrome Features in Pediatric Subjects with Abdominal Obesity during a Lifestyle Intervention" Nutrients 13, no. 2: 289. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020289