
Feeding Your Himalayan Expedition: Nutritional Signatures and Body Composition Adaptations of Trekkers and Porters

 ,
,  , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
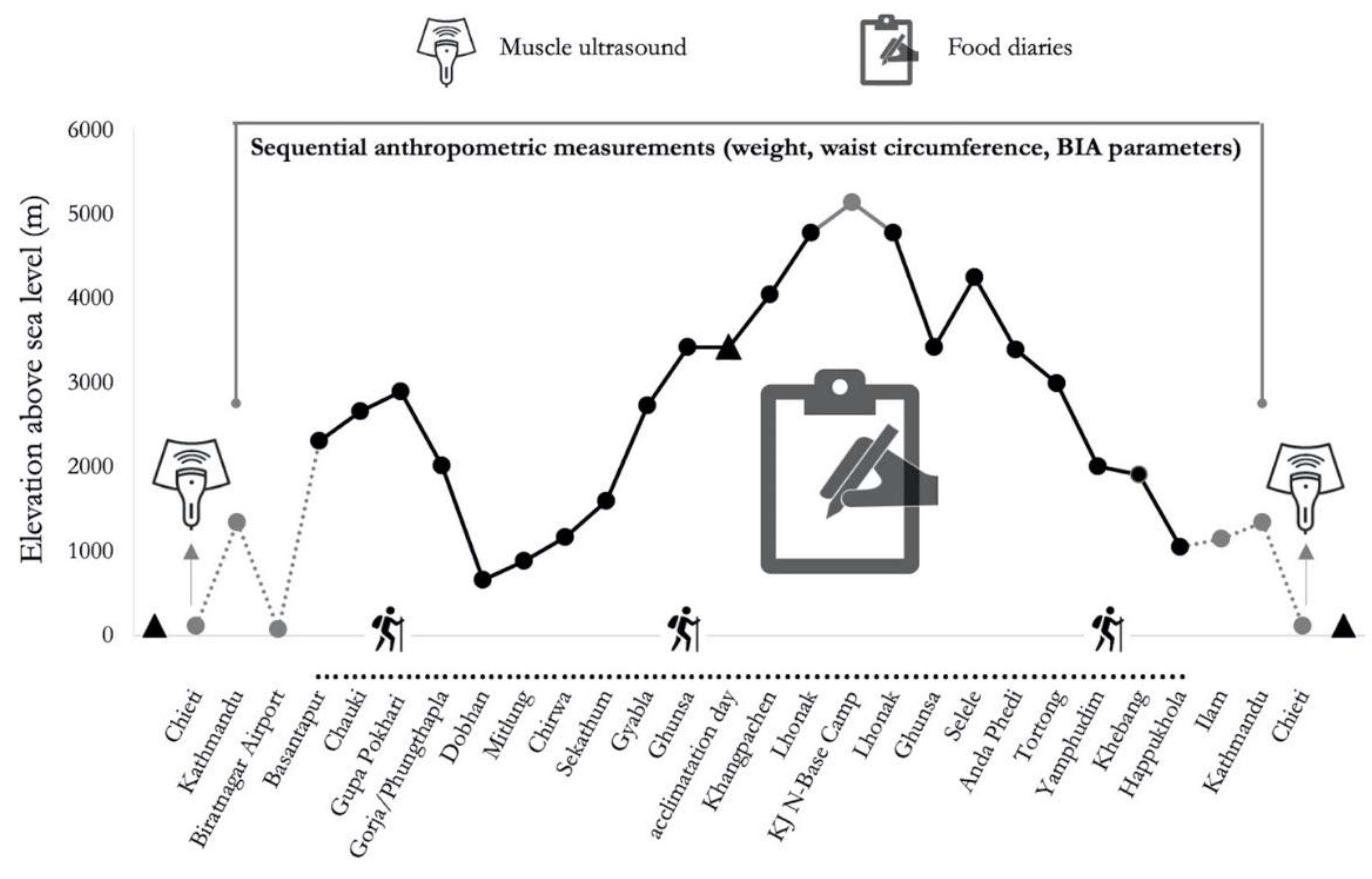
2.1. Study Design and Participants
2.2. Dietary Assessment
2.3. Bioimpedance Analysis
2.4. Muscle Ultrasound
2.5. Statistics
3. Results
3.1. Dietary Analysis
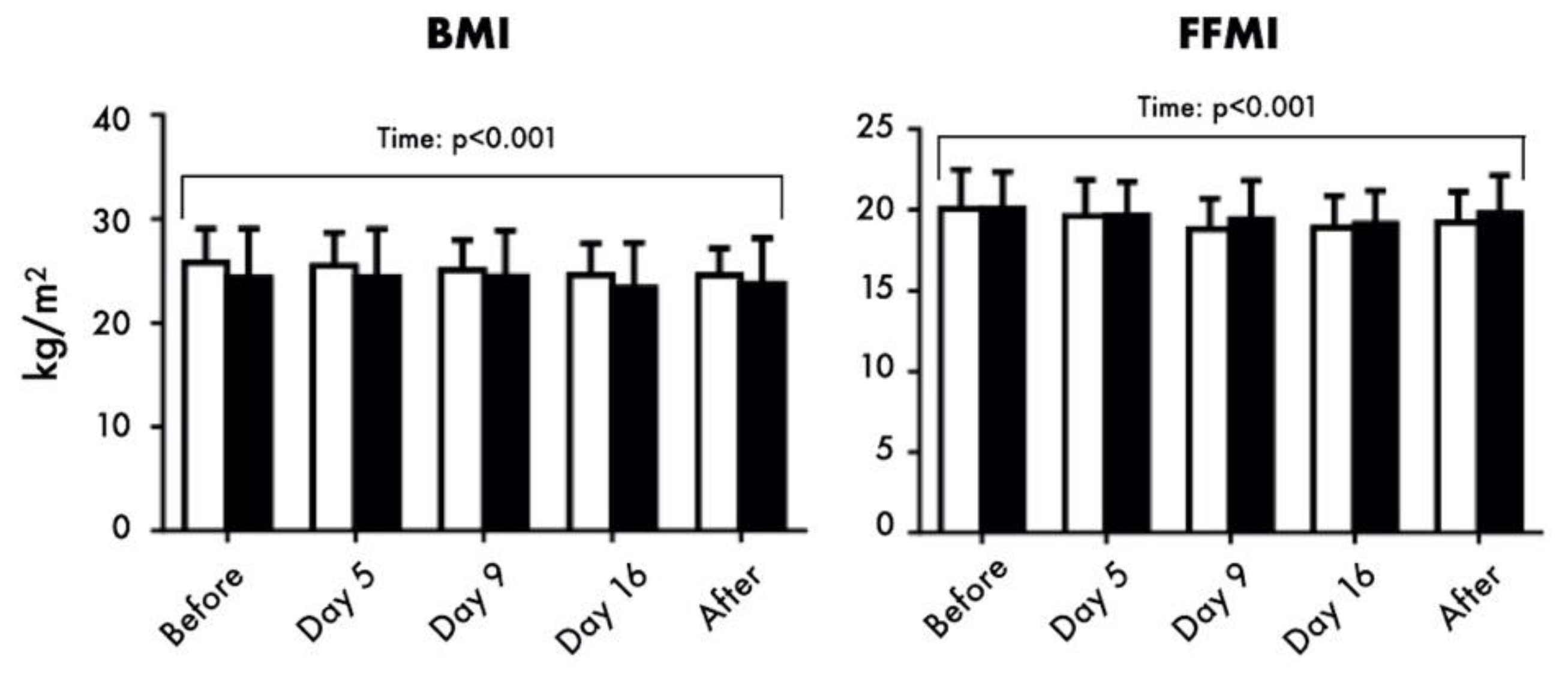
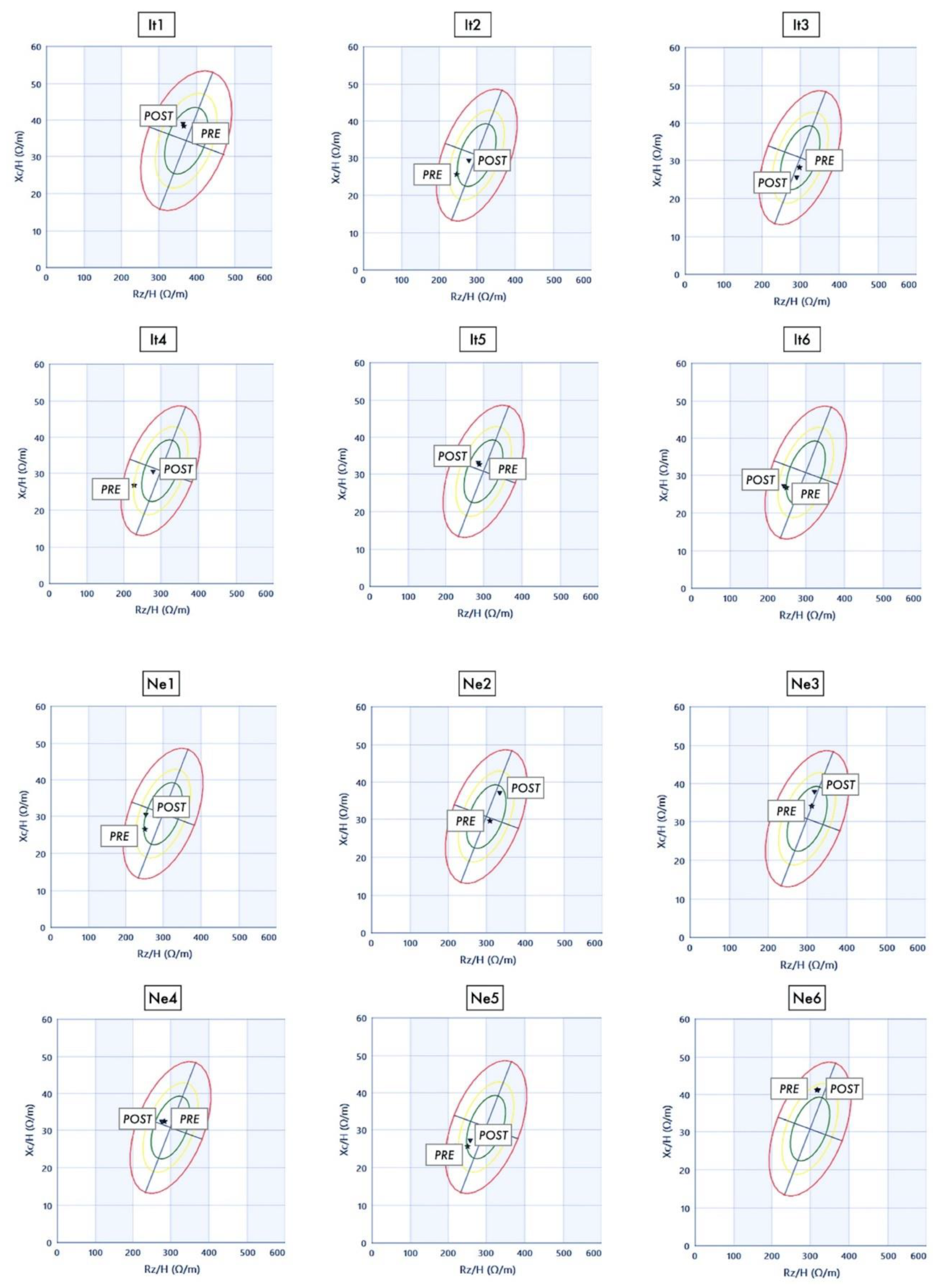
3.2. Anthropometrics and BIA
3.3. Muscle Ultrosound
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pasiakos, S.M. Nutritional Requirements for Sustaining Health and Performance During Exposure to Extreme Environments. Annu. Rev. Nutr. 2020. [Google Scholar] [CrossRef]
- Young, A.J.; Reeves, J.T. Human Adaptation to High Terrestrial Altitude. In Medical Aspects of Harsh Environments; Pandoff, K.B., Burr, R.E., Eds.; Walter Reed Army Medical Center Borden Institute: Washington, DC, USA, 2002; Volume 2, pp. 644–688. [Google Scholar]
- Schommer, K.; Bärtsch, P. Basic Medical Advice for Travelers to High Altitudes. Dtsch. Ärztebl. Int. 2011, 108. [Google Scholar] [CrossRef]
- Julian, C.G.; Moore, L.G. Human Genetic Adaptation to High Altitude: Evidence from the Andes. Genes 2019, 10, 150. [Google Scholar] [CrossRef] [Green Version]
- Horscroft, J.A.; Kotwica, A.O.; Laner, V.; West, J.A.; Hennis, P.J.; Levett, D.Z.H.; Howard, D.J.; Fernandez, B.O.; Burgess, S.L.; Ament, Z.; et al. Metabolic Basis to Sherpa Altitude Adaptation. Proc. Natl. Acad. Sci. USA 2017, 114, 6382–6387. [Google Scholar] [CrossRef] [Green Version]
- Magliulo, L.; Bondi, D.; Pietrangelo, T.; Fulle, S.; Piccinelli, R.; Jandova, T.; Blasio, G.D.; Taraborrelli, M.; Verratti, V. Serum Ferritin and Vitamin D Evaluation in Response to High Altitude Comparing Italians Trekkers vs Nepalese Porters. Eur. J. Sport Sci. 2020, 1–21. [Google Scholar] [CrossRef]
- Dawadi, S.; Basnyat, B.; Adhikari, S. A Review of Medical Problems in Himalayan Porters. High Alt. Med. Biol. 2020, 21, 109–113. [Google Scholar] [CrossRef]
- Stellingwerff, T.; Peeling, P.; Lewis, G.L.A.; Hall, R.; Koivisto, A.E.; Heikura, I.A.; Burke, L.M. Nutrition and Altitude: Strategies to Enhance Adaptation, Improve Performance and Maintain Health: A Narrative Review. Sports Med. 2019, 49, 169–184. [Google Scholar] [CrossRef] [Green Version]
- Michalczyk, M.; Czuba, M.; Zydek, G.; Zając, A.; Langfort, J. Dietary Recommendations for Cyclists during Altitude Training. Nutrients 2016, 8, 377. [Google Scholar] [CrossRef] [Green Version]
- Gaia, W.S. Nutritional Strategies for the Preservation of Fat Free Mass at High Altitude. Nutrients 2014, 6, 665–681. [Google Scholar] [CrossRef] [Green Version]
- Tam, E.; Bruseghini, P.; Calabria, E.; Sacco, D.L.; Doria, C.; Grassi, B.; Pietrangelo, T.; Pogliaghi, S.; Reggiani, C.; Salvadego, D.; et al. Gokyo Khumbu/Ama Dablam Trek 2012: Effects of Physical Training and High-Altitude Exposure on Oxidative Metabolism, Muscle Composition, and Metabolic Cost of Walking in Women. Eur. J. Appl. Physiol. 2016, 116, 129–144. [Google Scholar] [CrossRef]
- Doria, C.; Toniolo, L.; Verratti, V.; Cancellara, P.; Pietrangelo, T.; Marconi, V.; Paoli, A.; Pogliaghi, S.; Fanò, G.; Reggiani, C.; et al. Improved VO2 Uptake Kinetics and Shift in Muscle Fiber Type in High-Altitude Trekkers. J. Appl. Physiol. Bethesda Md 1985 2011, 111, 1597–1605. [Google Scholar] [CrossRef]
- Kayser, B. Nutrition and High Altitude Exposure. Int. J. Sports Med. 1992, 13 (Suppl. 1), S129–S132. [Google Scholar] [CrossRef] [PubMed]
- Kayser, B. Nutrition and Energetics of Exercise at Altitude. Sports Med. 1994, 17, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Hamad, N.; Travis, S.P.L. Weight Loss at High Altitude: Pathophysiology and Practical Implications. Eur. J. Gastroenterol. Hepatol. 2006, 18, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Bosco, G.; Paoli, A.; Rizzato, A.; Marcolin, G.; Guagnano, M.T.; Doria, C.; Bhandari, S.; Pietrangelo, T.; Verratti, V. Body Composition and Endocrine Adaptations to High-Altitude Trekking in the Himalayas. Adv. Exp. Med. Biol. 2019. [Google Scholar] [CrossRef]
- Verratti, V.; Bondi, D.; Shakir, A.; Pietrangelo, T.; Piccinelli, R.; Altieri, V.M.; Migliorelli, D.; Tafuri, A. Uroflowmetry and Altitude Hypoxia: A Report from Healthy Italian Trekkers and Nepali Porters During Himalayan Expedition. Adv. Exp. Med. Biol. 2020. [Google Scholar] [CrossRef]
- Olier, C.J.; Irurtia, A.; Jemni, M.; Marginet, C.M.; García, F.R.; Rodríguez, F.A. Bioelectrical Impedance Vector Analysis (BIVA) in Sport and Exercise: Systematic Review and Future Perspectives. PLoS ONE 2018, 13, e0197957. [Google Scholar] [CrossRef]
- Campa, F.; Matias, C.; Gatterer, H.; Toselli, S.; Koury, J.C.; Andreoli, A.; Melchiorri, G.; Sardinha, L.B.; Silva, A.M. Classic Bioelectrical Impedance Vector Reference Values for Assessing Body Composition in Male and Female Athletes. Int. J. Environ. Res. Public. Health 2019, 16, 5066. [Google Scholar] [CrossRef] [Green Version]
- Lori, S.; Lolli, F.; Molesti, E.; Bastianelli, M.; Gabbanini, S.; Saia, V.; Trapani, S.; Marinoni, M. Muscle-Ultrasound Evaluation in Healthy Pediatric Subjects: Age-Related Normative Data: Pediatric Muscular Ultrasound. Muscle Nerve 2018, 58, 245–250. [Google Scholar] [CrossRef]
- Nijholt, W.; Scafoglieri, A.; Wittenaar, J.H.; Hobbelen, J.S.M.; Schans, C.P. The Reliability and Validity of Ultrasound to Quantify Muscles in Older Adults: A Systematic Review. J. Cachexia Sarcopenia Muscle 2017, 8, 702–712. [Google Scholar] [CrossRef]
- Turrini, A.; Addezio, L.; Dhurandhar, E.; Ferrari, M.; Donne, C.; Mistura, L.; Piccinelli, R.; Scalvedi, M.L.; Sette, S. Editorial: Emerging Topics in Dietary Assessment. Front. Nutr. 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Guidance on the EU Menu Methodology. EFSA J. 2014, 12. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191. [Google Scholar] [CrossRef] [Green Version]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Ryan, S.A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN Exercise & Sports Nutrition Review Update: Research & Recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 1–57. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]
- Carlsohn, A. Recent Nutritional Guidelines for Endurance Athletes. Ger. J. Sports Med. 2016, 2016, 7–12. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Diaz, V.N.; Talluri, A.; Nescolarde, L. Classification of Hydration in Clinical Conditions: Indirect and Direct Approaches Using Bioimpedance. Nutrients 2019, 11, 809. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, S.A.; Lucas, F.M.; Teruel, J.L. Fundamentos Eléctricos de La Bioimpedancia. Nefrología 2012, 32, 133–135. [Google Scholar] [CrossRef]
- Rankin, G.; Stokes, M. Reliability of Assessment Tools in Rehabilitation: An Illustration of Appropriate Statistical Analyses. Clin. Rehabil. 1998, 12, 187–199. [Google Scholar] [CrossRef]
- Ticinesi, A.; Narici, M.V.; Lauretani, F.; Nouvenne, A.; Colizzi, E.; Mantovani, M.; Corsonello, A.; Landi, F.; Meschi, T.; Maggio, M. Assessing Sarcopenia with Vastus Lateralis Muscle Ultrasound: An Operative Protocol. Aging Clin. Exp. Res. 2018, 30, 1437–1443. [Google Scholar] [CrossRef]
- Stokes, M.; Hides, J.; Elliott, J.; Kiesel, K.; Hodges, P. Rehabilitative Ultrasound Imaging of the Posterior Paraspinal Muscles. J. Orthop. Sports Phys. Ther. 2007, 37, 581–595. [Google Scholar] [CrossRef] [PubMed]
- Stokes, M.; Rankin, G.; Newham, D.J. Ultrasound Imaging of Lumbar Multifidus Muscle: Normal Reference Ranges for Measurements and Practical Guidance on the Technique. Man. Ther. 2005, 10, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SINU The Italian Society of Human Nutrition (SINU) Tables. Available online: https://sinu.it/tabelle-larn-2014 (accessed on 10 August 2020).
- Westerterp, K.R.; Kayser, B.; Brouns, F.; Herry, J.P.; Saris, W.H. Energy Expenditure Climbing Mt. Everest. J. Appl. Physiol. Bethesda Md 1985 1992, 73, 1815–1819. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R.; Kayser, B.; Wouters, L.; Trong, J.L.; Richalet, J.P. Energy Balance at High Altitude of 6542 m. J. Appl. Physiol. Bethesda Md 1985 1994, 77, 862–866. [Google Scholar] [CrossRef]
- Westerterp, K.R.; Meijer, E.P.; Rubbens, M.; Robach, P.; Richalet, J.P. Operation Everest III: Energy and Water Balance. Pflug. Arch. 2000, 439, 483–488. [Google Scholar] [CrossRef]
- Reynolds, R.D.; Lickteig, J.A.; Howard, M.P.; Deuster, P.A. Intakes of High Fat and High Carbohydrate Foods by Humans Increased with Exposure to Increasing Altitude during an Expedition to Mt. Everest. J. Nutr. 1998, 128, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, R.D.; Lickteig, J.A.; Deuster, P.A.; Howard, M.P.; Conway, J.M.; Pietersma, A.; Stoppelaar, J.; Deurenberg, P. Energy Metabolism Increases and Regional Body Fat Decreases While Regional Muscle Mass Is Spared in Humans Climbing Mt. Everest. J. Nutr. 1999, 129, 1307–1314. [Google Scholar] [CrossRef] [Green Version]
- Verratti, V.; Falone, S.; Doria, C.; Pietrangelo, T.; Giulio, C. Kilimanjaro Abruzzo Expedition: Effects of High-Altitude Trekking on Anthropometric, Cardiovascular and Blood Biochemical Parameters. Sport Sci. Health 2015, 11, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Woods, A.L.; Sharma, A.P.; Lewis, G.L.A.; Saunders, P.U.; Rice, A.J.; Thompson, K.G. Four Weeks of Classical Altitude Training Increases Resting Metabolic Rate in Highly Trained Middle-Distance Runners. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 83–90. [Google Scholar] [CrossRef]
- Macdonald, J.H.; Oliver, S.J.; Hillyer, K.; Sanders, S.; Smith, Z.; Williams, C.; Yates, D.; Ginnever, H.; Scanlon, E.; Roberts, E.; et al. Body Composition at High Altitude: A Randomized Placebo-Controlled Trial of Dietary Carbohydrate Supplementation. Am. J. Clin. Nutr. 2009, 90, 1193–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butterfield, G.E.; Gates, J.; Fleming, S.; Brooks, G.A.; Sutton, J.R.; Reeves, J.T. Increased Energy Intake Minimizes Weight Loss in Men at High Altitude. J. Appl. Physiol. Bethesda Md 1985 1992, 72, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Kayser, B.; Narici, M.; Milesi, S.; Grassi, B.; Cerretelli, P. Body Composition and Maximum Alactic Anaerobic Performance During a One Month Stay at High Altitude. Int. J. Sports Med. 1993, 14, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Lima, H.M.; Moreira, D.C.; Ingraham, R.G.A.; Billoud, G.M.; Mattos, G.T.C.; Campos, É.G. Preparation for Oxidative Stress under Hypoxia and Metabolic Depression: Revisiting the Proposal Two Decades Later. Free Radic. Biol. Med. 2015, 89, 1122–1143. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Cao, R.; Zhang, X.Y.; Guan, Y. Aquaporins in the Kidney: Physiology and Pathophysiology. Am. J. Physiol. Ren. Physiol. 2020, 318, F193–F203. [Google Scholar] [CrossRef]
- Hoogewijs, D.; Vogler, M.; Zwenger, E.; Krull, S.; Zieseniss, A. Oxygen-Dependent Regulation of Aquaporin-3 Expression. Hypoxia Auckl. NZ 2016, 4, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Wakayama, Y.; Jimi, T.; Inoue, M.; Kojima, H.; Shibuya, S.; Murahashi, M.; Hara, H.; Oniki, H. Expression of Aquaporin 3 and Its Localization in Normal Skeletal Myofibres. Histochem. J. 2002, 34, 331–337. [Google Scholar] [CrossRef]
- Askew, E.W. Food for High-Altitude Expeditions: Pugh Got It Right in 1954—A Commentary on the Report by L.G.C.E. Pugh: “Himalayan Rations with Special Reference to the 1953 Expedition to Mount Everest”. Wilderness Environ. Med. 2004, 15, 121–124. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Breakfast | Lunch | Dinner | Snacks | |||||
|---|---|---|---|---|---|---|---|---|
| Ita | Nep | Ita | Nep | Ita | Nep | Ita | Nep | |
| Energy Intake | 25% | 12% | 31% | 41% | 34% | 43% | 10% | 4% |
| Water | 11% | 14% | 25% | 30% | 27% | 30% | 37% | 26% |
| Protein | 28% | 8% | 26% | 44% | 35% | 47% | 11% | 1% |
| Fat | 18% | 20% | 34% | 39% | 36% | 41% | 12% | 0% |
| Carbohydrates | 31% | 11% | 30% | 41% | 31% | 43% | 8% | 5% |
| Italian Group (n = 5) | Nepalese Group (n = 6) | ||||||
|---|---|---|---|---|---|---|---|
| Food Categories | Food Sub-Categories | n Consumers Only | Mean TOTAL Group | SD * | n Consumers Only | Mean TOTAL Group | SD * |
| Cereals, cereal products and substitutes | 5 | 408.5 | 239.6 | 6 | 897.9 | 42.0 | |
| Bread | 5 | 165.0 | 94.1 | 0 | 0.0 | 0.0 | |
| Pasta and pasta substitutes | 5 | 65.5 | 18.2 | 6 | 55.0 | 12.2 | |
| Rice | 3 | 100.0 | 145.8 | 6 | 838.5 | 41.5 | |
| Wheat and wheat flour | 5 | 53.2 | 28.6 | 1 | 4.4 | 0.0 | |
| Breakfast cereals | 2 | 6.7 | 0.0 | 0 | 0.0 | 0.0 | |
| Biscuits | 2 | 17.1 | 0.0 | 0 | 0.0 | 0.0 | |
| Sweets and sweet snacks without creams, jams and without chocolate toppings | 1 | 1.1 | 0.0 | 0 | 0.0 | 0.0 | |
| Pulses, fresh and processed | 5 | 28.1 | 40.8 | 6 | 212.9 | 31.4 | |
| Pulses, fresh and preserved | 5 | 13.2 | 9.0 | 0 | 0.0 | 0.0 | |
| Pulses, dried | 1 | 14.9 | 0.0 | 6 | 212.9 | 31.4 | |
| Vegetables, fresh and processed | 5 | 247.6 | 85.7 | 6 | 185.7 | 21.8 | |
| Leafy vegetables, fresh | 5 | 91.7 | 40.6 | 0 | 0.0 | 0.0 | |
| Tomatoes, fresh | 3 | 13.3 | 25.9 | 6 | 123.1 | 18.2 | |
| Tomatoes, processed | 5 | 20.0 | 0.0 | 0 | 0.0 | 0.0 | |
| Other fruiting vegetables, fresh | 5 | 40.0 | 10.5 | 0 | 0.0 | 0.0 | |
| Roots and onions, fresh | 5 | 28.0 | 13.1 | 6 | 43.9 | 0.9 | |
| Other vegetables, fresh | 5 | 52.0 | 31.6 | 6 | 18.7 | 2.8 | |
| Other vegetables, preserved | 1 | 1.9 | 0.0 | 0 | 0.0 | 0.0 | |
| Spices and herbs | 5 | 0.8 | 0.3 | 1 | 0.02 | 0.0 | |
| Potatoes, tubers and their products | 5 | 174.7 | 39.1 | 6 | 395.8 | 64.5 | |
| Potatoes, potatoes-based products, excluding french fries | 5 | 174.7 | 39.1 | 6 | 395.8 | 64.5 | |
| Fruit, fresh and processed | 5 | 117.3 | 29.1 | 4 | 16.7 | 0.0 | |
| Exoticf ruit, fresh | 5 | 81.7 | 22.4 | 4 | 16.7 | 0.0 | |
| Other fruit, fresh | 4 | 20.0 | 0.0 | 0 | 0.0 | 0.0 | |
| Nuts, seeds, olives and their products, dried fruit | 5 | 15.7 | 6.8 | 0 | 0.0 | 0.0 | |
| Meat, meat products and substitutes | 5 | 86.9 | 16.6 | 0 | 0.0 | 0.0 | |
| Beef and veal, not preserved, excl. offal | 5 | 30.9 | 15.1 | 0 | 0.0 | 0.0 | |
| Pork, not preserved, excl. offal | 5 | 15.6 | 6.1 | 0 | 0.0 | 0.0 | |
| Poultry and game, not preserved, excl. offal | 5 | 26.7 | 3.7 | 0 | 0.0 | 0.0 | |
| Other meats, not preserved, excl. offal | 2 | 4.2 | 5.9 | 0 | 0.0 | 0.0 | |
| Ham, salami, sausages and other preserved meats, excl. offal | 3 | 9.6 | 4.6 | 0 | 0.0 | 0.0 | |
| Milk, milk products and substitutes | 5 | 251.4 | 133.8 | 1 | 5.6 | 0.0 | |
| Milk, milk-based beverages | 5 | 240.7 | 127.4 | 1 | 5.6 | 0.0 | |
| Cheese and substitutes | 3 | 10.7 | 9.2 | 0 | 0.0 | 0.0 | |
| Eggs | 5 | 108.9 | 49.4 | 1 | 11.8 | 0.0 | |
| Eggs | 5 | 108.9 | 49.4 | 1 | 11.8 | 0.0 | |
| Oils and fats | 5 | 71.9 | 19.7 | 6 | 65.1 | 5.4 | |
| Olive oil | 5 | 17.6 | 7.3 | 6 | 33.5 | 3.9 | |
| Other vegetable oils | 5 | 53.1 | 15.5 | 6 | 30.5 | 4.9 | |
| Butter and creams | 3 | 1.3 | 0.6 | 1 | 1.1 | 0.0 | |
| Sweet products and substitutes | 5 | 38.7 | 18.1 | 6 | 25.1 | 5.3 | |
| Chocolate and substitutes | 1 | 1.3 | 0.0 | 0 | 0.0 | 0.0 | |
| Candies, jam and other sweet products incl. sugar-free | 3 | 4.7 | 5.1 | 0 | 0.0 | 0.0 | |
| Sugar, fructose, honey and other nutritious sweeteners | 5 | 32.6 | 17.9 | 6 | 25.1 | 5.3 | |
| Water and other non-alcoholic beverages | 5 | 2083.8 | 312.8 | 6 | 2093.3 | 276.8 | |
| Tap water as such, in beverages or recipes | 5 | 1429.7 | 322.0 | 6 | 1673.3 | 390.1 | |
| Coffee, tea, herbal tea and substitutes | 5 | 653.7 | 166.9 | 6 | 420.0 | 144.3 | |
| Fruit and vegetable juices | 1 | 0.4 | 0.0 | 0 | 0.0 | 0.0 | |
| Alcoholic beverages and substitutes | 3 | 66.0 | 0.0 | 0 | 0.0 | 0.0 | |
| Beer, cider and substitutes | 3 | 66.0 | 0.0 | 0 | 0.0 | 0.0 | |
| Meal substitutes | 1 | 1.8 | 0.0 | 0 | 0.0 | 0.0 | |
| Meal substitutes | 1 | 1.8 | 0.0 | 0 | 0.0 | 0.0 | |
| Miscellaneous | 5 | 3.7 | 3.1 | 1 | 0.2 | 0.0 | |
| Non-fat sauces or condiments (ketchup, vinegar, etc.) | 5 | 2.9 | 2.6 | 0 | 0.0 | 0.0 | |
| Nuts for broth or other various products | 4 | 0.8 | 0.5 | 1 | 0.2 | 0.0 | |
| Food supplements | 3 | 2.7 | 2.9 | 0 | 0.0 | 0.0 | |
| Food supplements | 3 | 2.7 | 2.9 | 0 | 0.0 | 0.0 | |
| Total amount of foods and beverages | 3692 | 3910 | |||||
| Total amount of solid foods | 1302 | 1811 | |||||
| Total amount of liquid foods ** | 2391 | 2099 | |||||
| Nepalese (n = 6) | Italians (n = 5) | Tr GL 1,2,3 | It RDA 4 | |||
|---|---|---|---|---|---|---|
| Mean | SD * | Mean | SD * | |||
| Energy Intake_EI (MJ) | 12 | 3 | 12 | 1 | ||
| Energy Intake_EI (kcal) | 2793 | 810 | 2755 | 188 | 2000–7000 | |
| Water (g/day) | 3099 | 462 | 3240 | 310 | 4000–5000 2 | 2500 AI |
| Protein (g/day) | 90 | 30 | 84 | 7 | 63 PRI | |
| Protein (g/kg/day) | 1.2 | 0.4 | 1.3 | 0.3 | 1.2→2.0 1,2 | 0.9 PRI |
| Fat (g/day) | 118 | 27 | 74 | 6 | ||
| SFA (g/day) | 25 | 6 | 11 | 2 | ||
| MUFA(g/day) | 46 | 11 | 37 | 3 | ||
| PUFA (g/day) | 39 | 9 | 23 | 3 | ||
| Cholesterol (mg/day) | 510 | 190 | 47 | 116 | <300 SDT | |
| Available carbohydrate (g/day) | 362 | 127 | 466 | 33 | ||
| Available carbohydrate (g/kg bw/day) | 5 | 2 | 7 | 2 | 8 1–12 2 | |
| Simple carbohydrate (g) | 90 | 15 | 45 | 6 | ||
| Starch (g/day) | 248 | 116 | 383 | 28 | ||
| Dietary fibre (g/day) | 23 | 9 | 43 | 6 | >25 SDT | |
| Dietary fibre (g/1000 Kcal/d) | 8.1 | 0.9 | 15.6 | 1.3 | 12.6–16.7 RI | |
| Alcohol (g/day) | 2 | 2 | 0.0 | 0.0 | ||
| % Total energy from | ||||||
| Protein (%EI) | 13 | 4 | 12 | 1 | ||
| Fat (%EI) | 38 | 9 | 24 | 5 | up to 50 1 | ≤30 RI |
| SFA (%EI) | 8 | 2 | 4 | 1 | pRDA ° | <10 SDT |
| PUFA (%EI) | 12 | 3 | 7 | 1 | pRDA ° | 5–10 RI |
| Available carbohydrate (%EI) | 49 | 17 | 63 | 5 | 45–60 RI | |
| Simple carbohydrate (%EI) | 13 | 4 | 6 | 1 | <15 SDT | |
| Minerals | ||||||
| Potassium (mg/day) | 3815 | 993 | 5479 | 700 | pRDA ° | 3900 AI |
| Phosphorus (mg/day) | 1446.4 | 449.6 | 1453.0 | 129.6 | pRDA ° | 700 PRI |
| Calcium (mg/day) | 789 | 219 | 468 | 57 | pRDA ° | 1000 PRI |
| Magnesium (mg/day) | 408 | 72 | 462 | 48 | pRDA ° | 240 PRI |
| Iron (mg/day) | 14 | 5 | 24 | 3 | Up to 70% of requirement | 10 PRI |
| Zinc (mg/day) | 14 | 4 | 17 | 2 | pRDA ° | 12 PRI |
| Vitamins | ||||||
| Thiamine (mg/day) | 1.3 | 0.4 | 1.8 | 0.2 | pRDA ° | 1.2 PRI |
| Riboflavin (mg/day) | 1.9 | 0.4 | 1.0 | 0.1 | pRDA ° | 1.6 PRI |
| Niacin (mg/day) | 21 | 4 | 21 | 3 | pRDA ° | 18 PRI |
| Vitamin C (mg/day) | 121 | 22 | 114 | 16 | pRDA ° | 105 PRI |
| Vitamin B6 (mg/day) | 3 | 1 | 5 | 1 | pRDA ° | 1.3 PRI |
| Vitamin A (REs µg/day) § | 855 | 228 | 284 | 81 | pRDA ° | 700 PRI |
| Vitamin K (µg /day) | 831 | 344 | 52 | 6 | pRDA ° | 140 AI |
| Vitamin E (mg/day) | 43 | 11 | 30 | 4 | pRDA ° | 13 AI |
| Vitamin D (µg/day) | 3.1 | 1.2 | 0.2 | 0.5 | pRDA ° | 15 AI |
| Vitamin B12 (µg/day) | 3.7 | 1.0 | 0.2 | 0.4 | pRDA ° | 2.4 PRI |
| Before | Day 5 | Day9 | Day 16 | After | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ita | Nep | Ita | Nep | Ita | Nep | Ita | Nep | Ita | Nep | |
| WtHR | 0.53 | 0.51 | 0.52 | 0.50 | 0.51 | 0.49 | 0.50 | 0.50 | 0.50 | 0.50 |
| Rz/h (Ω) | 482.80 | 476.00 | 497.30 | 508.30 | 530.00 | 515.50 | 520.20 | 511.20 | 501.70 | 486.80 |
| Xc/h (Ω) | 51.67 | 52.50 | 52.50 | 63.83 | 57.67 | 60.17 | 57.00 | 61.67 | 53.50 | 57.33 |
| PhA (degree) | 6.13 | 6.28 | 6.03 | 7.13 | 6.25 | 6.63 | 6.27 | 6.88 | 6.08 | 6.70 |
| Before | After | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | 95% Confidence Interval | |
| CSA, VL (cm2) * | 16.78 | 4.05 | 15.57 | 3.41 | −0.27 to −2.15 |
| MT, VL (cm) | 2.17 | 0.38 | 2.13 | 0.35 | 0.10 to −0.18 |
| FL, VL (cm) | 7.40 | 0.61 | 7.50 | 0.57 | 0.35 to −0.15 |
| PA, VL (°) | 15.51 | 0.87 | 14.95 | 1.50 | 0.59 to −1.71 |
| CSA, r-LM (cm2) | 13.13 | 1.90 | 12.49 | 1.43 | 0.61 to −2.15 |
| CSA, l-LM (cm2) | 13.15 | 1.96 | 12.38 | 1.54 | 0.56 to −1.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bondi, D.; Aloisi, A.M.; Pietrangelo, T.; Piccinelli, R.; Le Donne, C.; Jandova, T.; Pieretti, S.; Taraborrelli, M.; Santangelo, C.; Lattanzi, B.; et al. Feeding Your Himalayan Expedition: Nutritional Signatures and Body Composition Adaptations of Trekkers and Porters. Nutrients 2021, 13, 460. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020460
Bondi D, Aloisi AM, Pietrangelo T, Piccinelli R, Le Donne C, Jandova T, Pieretti S, Taraborrelli M, Santangelo C, Lattanzi B, et al. Feeding Your Himalayan Expedition: Nutritional Signatures and Body Composition Adaptations of Trekkers and Porters. Nutrients. 2021; 13(2):460. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020460
Chicago/Turabian StyleBondi, Danilo, Anna Maria Aloisi, Tiziana Pietrangelo, Raffaela Piccinelli, Cinzia Le Donne, Tereza Jandova, Stefano Pieretti, Mattia Taraborrelli, Carmen Santangelo, Bruna Lattanzi, and et al. 2021. "Feeding Your Himalayan Expedition: Nutritional Signatures and Body Composition Adaptations of Trekkers and Porters" Nutrients 13, no. 2: 460. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020460