
Longitudinal Study Depicting Differences in Complementary Feeding and Anthropometric Parameters in Late Preterm Infants up to 2 Years of Age

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Subjects and Methods
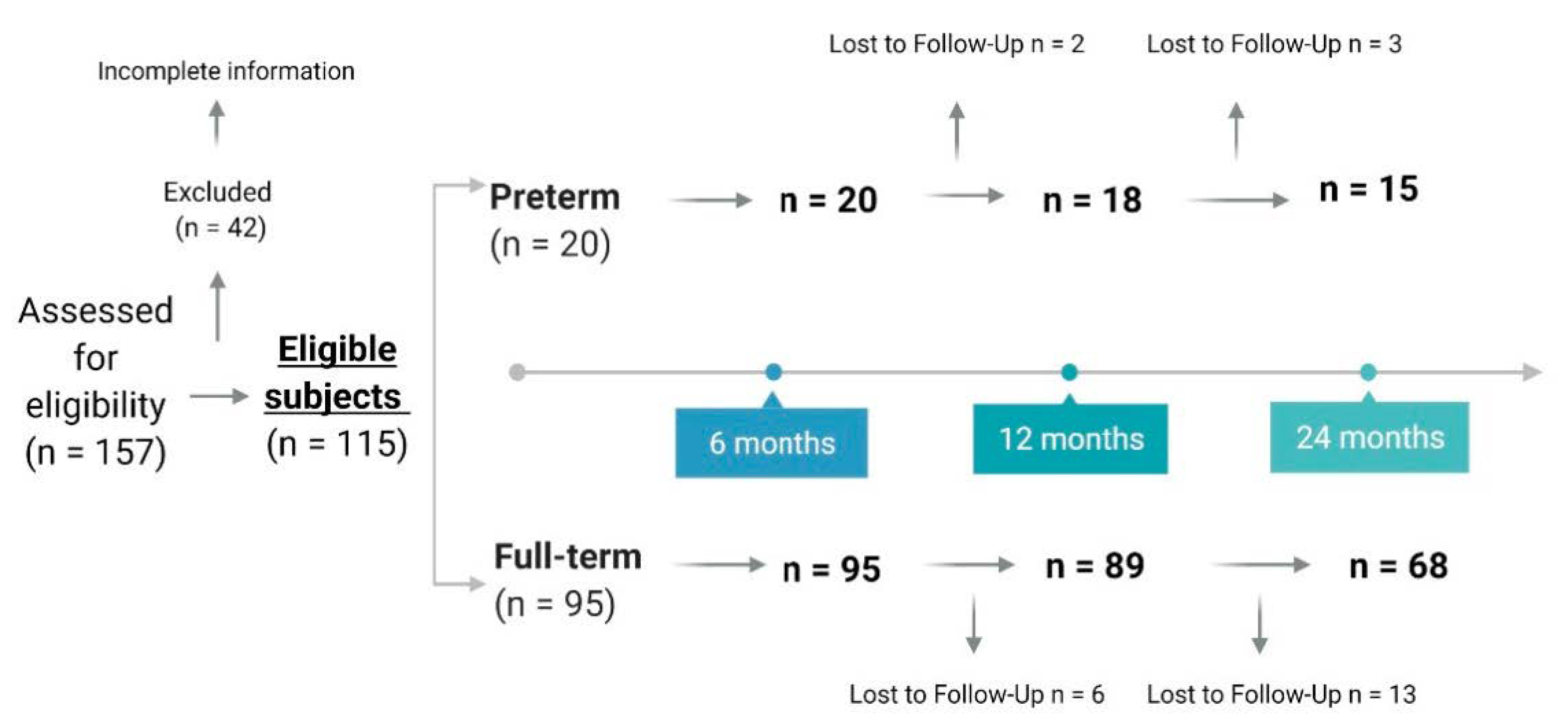
2.1. Design and Sample Recruitment
2.2. General Characteristics
2.3. Dietary Assessment and Nutritional Data Analysis
2.4. Anthropometric Measures
2.5. Statistical Analyses
3. Results
3.1. General Description of the Sample
3.2. Complementary Feeding
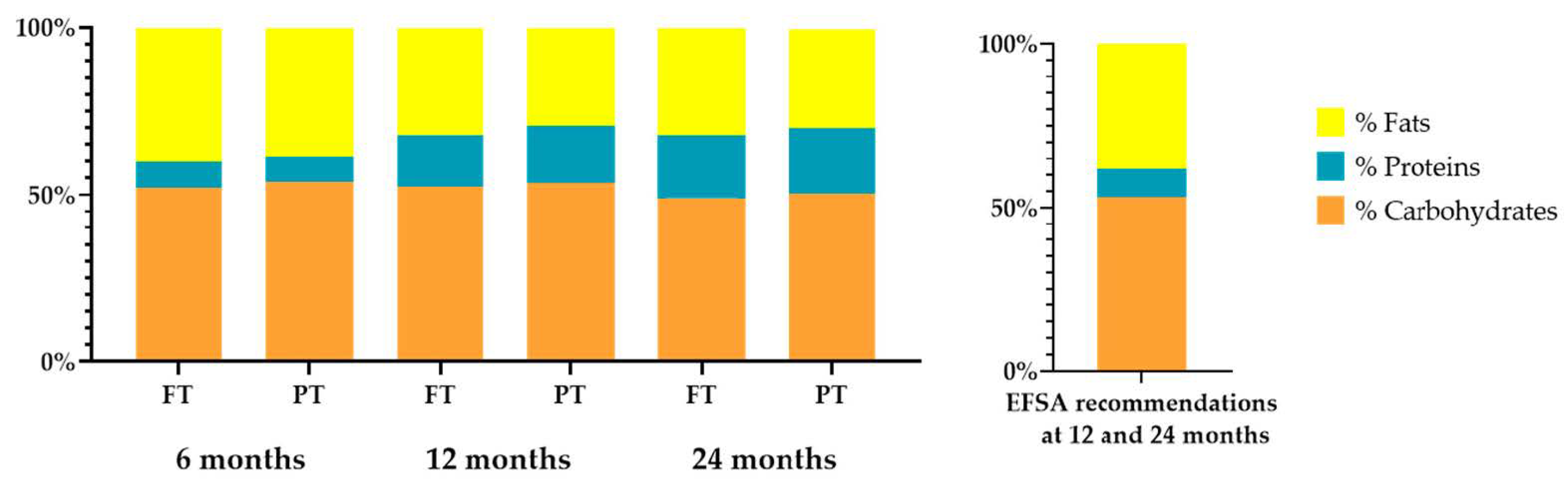
3.3. Nutritional Targets in Children
3.4. Bioactive Compounds
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [Green Version]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.; Christian, P.; et al. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205. [Google Scholar] [CrossRef]
- Abubakar, I.I.; Tillmann, T.; Banerjee, A. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Kumar, R.K.; Singhal, A.; Vaidya, U.; Banerjee, S.; Anwar, F.; Rao, S. Optimizing Nutrition in Preterm Low Birth Weight Infants—Consensus Summary. Front. Nutr. 2017, 4, 20. [Google Scholar] [CrossRef] [Green Version]
- Hanson, C.; Sundermeier, J.; Dugick, L.; Lyden, E.; Anderson-Berry, A.L. Implementation, Process, and Outcomes of Nutrition Best Practices for Infants. Nutr. Clin. Pract. 2011, 26, 614–624. [Google Scholar] [CrossRef]
- Donovan, R.; Puppala, B.; Angst, D.; Coyle, B.W. Outcomes of early nutrition support in extremely low-birth-weight infants. Nutr. Clin. Pract. 2006, 21, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. Complementary Feeding: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, K. Guiding Principles for Complementary Feeding of the Breastfeed Child. Available online: https://www.who.int/maternal_child_adolescent/documents/a85622/en/ (accessed on 15 February 2021).
- Liotto, N.; Cresi, F.; Beghetti, I.; Roggero, P.; Menis, C.; Corvaglia, L.; Mosca, F.; Aceti, A. Complementary Feeding in Preterm Infants: A Systematic Review. Nutrients 2020, 12, 1843. [Google Scholar] [CrossRef]
- Vissers, K.M.; Feskens, E.J.M.; Van Goudoever, J.B.; Janse, A.J. The timing of complementary feeding in preterm infants and the effect on overweight: Study protocol for a systematic review. Syst. Rev. 2016, 5, 149. [Google Scholar] [CrossRef] [Green Version]
- Naylor, A.J.; Morrow, A.L. Developmental readiness of normal full-term infants to progress from exclusive breast-feeding to the introduction of complementary foods reviews of the relevant literature concerning. Acad. Educ. Dev. 2001, 1–36. Available online: http://www.linkagesproject.org (accessed on 15 February 2021).
- Zielinska, M.A.; Rust, P.; Masztalerz-Kozubek, D.; Bichler, J.; Hamułka, J.; Rust; Kozubek, M. Factors Influencing the Age of Complementary Feeding—A Cross-Sectional Study from Two European Countries. Int. J. Environ. Res. Public Health 2019, 16, 3799. [Google Scholar] [CrossRef] [Green Version]
- Norris, F.; Larkin, M.; Williams, C.; Hampton, S.; Morgan, J. Factors affecting the introduction of complementary foods in the preterm infant. Eur. J. Clin. Nutr. 2002, 56, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Casey, P.H.; Bradley, R.H.; Whiteside-Mansell, L.; Barrett, K.; Gossett, J.M.; Simpson, P.M. Evolution of obesity in a low birth weight cohort. J. Perinatol. 2011, 32, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beluska-Turkan, K.; Korczak, R.; Hartell, B.; Moskal, K.; Maukonen, J.; Alexander, D.E.; Salem, N.; Harkness, L.; Ayad, W.; Szaro, J.; et al. Nutritional Gaps and Supplementation in the First 1000 Days. Nutrients 2019, 11, 2891. [Google Scholar] [CrossRef] [Green Version]
- Finch, C.W. Review of Trace Mineral Requirements for Preterm Infants. Nutr. Clin. Pract. 2014, 30, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Fernandez, J.; Ochoa, J.J.; Latunde-Dada, G.O.; Diaz-Castro, J. Iron Deficiency and Iron Homeostasis in Low Birth Weight Preterm Infants: A Systematic Review. Nutrients 2019, 11, 1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, W.W.J. Optimizing nutrition of the preterm infant. Zhongguo Dang Dai Er Ke Za Zhi 2017, 19, 1–21. [Google Scholar]
- Perrone, S.; Laschi, E.; Buonocore, G. Biomarkers of oxidative stress in the fetus and in the newborn. Free. Radic. Biol. Med. 2019, 142, 23–31. [Google Scholar] [CrossRef]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The effects of polyphenols and other bioactives on human health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocké, M.; De Boer, E.; Brants, H.; Van Der Laan, J.; Niekerk, M.; Van Rossum, C.; Temme, L.; Freisling, H.; Nicolas, G.; Casagrande, C.; et al. PANCAKE—Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe. EFSA Support. Publ. 2012, 9, 339. [Google Scholar] [CrossRef]
- Slimani, N.; Fahey, M.; Welch, A.A.; Wirfält, E.; Stripp, C.; Bergström, E.; Linseisen, J.; Schulze, M.B.; Bamia, C.; Chloptsios, Y.; et al. Diversity of dietary patterns observed in the European Prospective Investigation into Cancer and Nutrition (EPIC) project. Public Health Nutr. 2002, 5, 1311–1328. [Google Scholar] [CrossRef]
- European Food Safety Authority. Guidance on the EU Menu methodology. EFSA J. 2014, 12, 3944–4021. [Google Scholar] [CrossRef] [Green Version]
- Denney, L.; Afeiche, M.C.; Eldridge, A.L.; Villalpando-Carrión, S. Food Sources of Energy and Nutrients in Infants, Toddlers, and Young Children from the Mexican National Health and Nutrition Survey 2012. Nutrients 2017, 9, 494. [Google Scholar] [CrossRef]
- Devaney, B.; Kalb, L.; Briefel, R.; Zavitsky-Novak, T.; Clusen, N.; Ziegler, P. Feeding infants and toddlers study: Overview of the study design. J. Am. Diet. Assoc. 2004, 104, 8–13. [Google Scholar] [CrossRef]
- Farran, A.; Zamora, R.; Cervera, P. Tablas de Composición de Alimentos del CESNID; McGraw-Hill: New York, NY, USA, 2003. [Google Scholar]
- Gómez-Martín, M.; Arboleya, S.; Gueimonde, M.; González, S. Nutritional composition of processed baby foods targeted at infants from 0–12 months. J. Food Compos. Anal. 2019, 79, 55–62. [Google Scholar] [CrossRef]
- USDA. USDA Food Composition Databases. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 10 February 2020).
- Neveu, V.; Perez-Jimenez, J.; Vos, F.; Crespy, V.; Du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef] [PubMed]
- Marlett, J.A.; Cheung, T.-F. Database and Quick Methods of Assessing Typical Dietary Fiber Intakes using data for 228 Commonly Consumed Foods. J. Am. Diet. Assoc. 1997, 97, 1139–1151. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Child Growth Standards. Revista Chilena de Pediatría 2009, 80, 379–380. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation (WHO). WHO Anthro for Personal Computers. 2010. Available online: https://www.who.int/toolkits/child-growth-standards/software (accessed on 15 February 2021).
- World Health Organisation (WHO). WHO Training Course on Child Growth Assessment. Available online: https://www.who.int/childgrowth/training/en/ (accessed on 15 February 2021).
- Products, Epod, Nutrition, and Allergies (NDA). Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 1–103. [Google Scholar] [CrossRef] [Green Version]
- Cobo, T.; Vergara, A.; Collado, M.C.; Casals-Pascual, C.; Herreros, E.; Bosch, J.; Sánchez-García, A.B.; López-Parellada, R.; Ponce, J.; Gratacós, E. Characterization of vaginal microbiota in women with preterm labor with intra-amniotic inflammation. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Jónsdóttir, R.B.; Jónsdóttir, H.; Skúladóttir, A.; Thorkelsson, T.; Flacking, R. Breastfeeding progression in late preterm infants from birth to one month. Matern. Child Nutr. 2019, 16, e12893. [Google Scholar] [CrossRef] [PubMed]
- Habicht, J.-P. Expert Consultation on the Optimal Duration of Exclusive Breastfeeding. Tissue Eng. 2004, 554, 79–87. [Google Scholar]
- Schanler, R.J.; Lau, C.; Hurst, N.M.; Smith, E.O. Randomized Trial of Donor Human Milk Versus Preterm Formula as Substitutes for Mothers’ Own Milk in the Feeding of Extremely Premature Infants. Pediatrics 2005, 116, 400–406. [Google Scholar] [CrossRef]
- Su, B.-H. Optimizing Nutrition in Preterm Infants. Pediatr. Neonatol. 2014, 55, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- King, C. An evidence based guide to weaning preterm infants. Paediatr. Child Health 2009, 19, 405–414. [Google Scholar] [CrossRef]
- Morgan, J.B.; Williams, P.; Foote, K.D.; Marriott, L.D. Do mothers understand healthy eating principles for low-birth-weight infants? Public Health Nutr. 2006, 9, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Fanaro, S.; Borsari, G.; Vigi, V. Complementary Feeding Practices in Preterm Infants: An Observational Study in a Cohort of Italian Infants. J. Pediatr. Gastroenterol. Nutr. 2007, 45, S210–S214. [Google Scholar] [CrossRef]
- Marriott, L.D.; Foote, K.D.; Bishop, J.A.; Kimber, A.C.; Morgan, J.B. Weaning preterm infants: A randomised controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, D.; Makrides, M. Introducing Solid Foods to Preterm Infants in Developed Countries. Ann. Nutr. Metab. 2012, 60, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Gregory, K. Update on Nutrition for Preterm and Full-Term Infants. J. Obstet. Gynecol. Neonatal Nurs. 2005, 34, 98–108. [Google Scholar] [CrossRef]
- Worthington-White, D.A.; Behnke, M.; Gross, S. Premature infants require additional folate and vitamin B-12 to reduce the severity of the anemia of prematurity. Am. J. Clin. Nutr. 1994, 60, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Terrin, G.; Canani, R.B.; Di Chiara, M.; Pietravalle, A.; Aleandri, V.; Conte, F.; De Curtis, M. Zinc in Early Life: A Key Element in the Fetus and Preterm Neonate. Nutrients 2015, 7, 10427–10446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, E.K.; Dempsey, E.M.; Kiely, M.E. Iron supplementation in preterm and low-birth-weight infants: A systematic review of intervention studies. Nutr. Rev. 2019, 77, 865–877. [Google Scholar] [CrossRef]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the Healthy European Paediatric Population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexy, U.; Kersting, M.; Sichert-Hellert, W.; Manz, F.; Schöch, G. Macronutrient Intake of 3- to 36-Month-Old German Infants and Children: Results of the DONALD Study. Ann. Nutr. Metab. 1999, 43, 14–22. [Google Scholar] [CrossRef]
- Günther, A.L.B.; Buyken, A.E.; Kroke, A. Protein intake during the period of complementary feeding and early childhood and the association with body mass index and percentage body fat at 7 y of age. Am. J. Clin. Nutr. 2007, 85, 1626–1633. [Google Scholar] [CrossRef]
- Fanaro, S.; Vigi, V. Weaning Preterm Infants: An Open Issue. J. Pediatr. Gastroenterol. Nutr. 2007, 45, S204–S209. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Wong, W.W.; Hopkinson, J.M.; Smith, E.O.; Ellis, K.J. Infant Feeding Mode Affects Early Growth and Body Composition. Pediatrics 2000, 106, 1355–1366. [Google Scholar] [CrossRef]
- Nielsen, G.; Thomsen, B.; Michaelsen, K.F. Influence of breastfeeding and complementary food on growth between 5 and 10 months. Acta Paediatr. 1998, 87, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Tzounis, X.; Vulevic, J.; Kuhnle, G.G.C.; George, T.; Leonczak, J.; Gibson, G.R.; Kwik-Uribe, C.; Spencer, J.P.E. Flavanol monomer-induced changes to the human faecal microflora. Br. J. Nutr. 2007, 99, 782–792. [Google Scholar] [CrossRef] [Green Version]
- Pei, R.; Liu, X.; Bolling, B. Flavonoids and gut health. Curr. Opin. Biotechnol. 2020, 61, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.; Li, C.; Buys, N.; Wang, W.; Yin, C.; Sun, J. Effects of Probiotics in Preterm Infants: A Network Meta-analysis. Pediatrics 2021, 147, e20200706. [Google Scholar] [CrossRef] [PubMed]
- D’Hoe, K.; Conterno, L.; Fava, F.; Falony, G.; Vieira-Silva, S.; Vermeiren, J.; Tuohy, K.; Raes, J. Prebiotic Wheat Bran Fractions Induce Specific Microbiota Changes. Front. Microbiol. 2018, 9, 31. [Google Scholar] [CrossRef] [PubMed]
- Gila-Díaz, A.; Carrillo, G.H.; Cañas, S.; De Pipaón, M.S.; Martínez-Orgado, J.A.; Rodríguez-Rodríguez, P.; De Pablo, Á.L.L.; Martin-Cabrejas, M.A.; Ramiro-Cortijo, D.; Arribas, S.M. Influence of Maternal Age and Gestational Age on Breast Milk Antioxidants During the First Month of Lactation. Nutrients 2020, 12, 2569. [Google Scholar] [CrossRef]
- Gila-Diaz, A.; Arribas, S.M.; Algara, A.; Martín-Cabrejas, M.A.; De Pablo, Á.L.L.; De Pipaón, M.S.; Ramiro-Cortijo, D. A Review of Bioactive Factors in Human Breastmilk: A Focus on Prematurity. Nutrients 2019, 11, 1307. [Google Scholar] [CrossRef] [Green Version]
- Gila-Díaz, A.; Carrillo, G.H.; De Pablo, Á.L.L.; Arribas, S.M.; Ramiro-Cortijo, D. Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months. Int. J. Environ. Res. Public Health 2020, 17, 7153. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infant Factors | FT | PT | |
|---|---|---|---|
| Sex (N 95) (N 20) | Male | 54 (56.8) | 8 (40.0) |
| Female | 41 (43.2) | 12 (60.0) | |
| Weight for age z-score at birth (N 93) (N 19) | 0.00 ± 0.99 | −4.66 ± 0.74 * | |
| Height for age z-score (N 86) (N 16) | 0.13 ± 0.91 | −4.26 ± 1.40 * | |
| BMI z-score at birth (N 86) (N 16) | Severe underweight (<−3) | 2 (2.3) | 15 (93.8) * |
| Underweight (−3 to >−1) | 16 (18.6) | 0 | |
| Normal weight (−1 to 1) | 59 (68.6) | 1 (6.3) | |
| Overweight (>1 to 2) | 7 (8.1) | 0 | |
| Obese >2 | 2 (2.3) | 0 | |
| Maternal factors | |||
| Age (year) (N 87) (N 19) | 34.45 ± 5.02 | 34.58 ± 3.75 | |
| Education level (N 94) (N 20) | Primary | 4 (4.3) | 2 (7.1) |
| Secondary | 13 (13.8) | 1 (5.0) | |
| High school | 26 (27.7) | 7 (35.0) | |
| University | 51 (54.3) | 12 (60.0) | |
| Weight pre-pregnancy (kg) (N 94) (N 20) | 65.06 ± 12.29 | 64.64 ± 12.42 | |
| Weight at delivery (kg) (N 93) (N 18) | 76.57 ± 11.06 | 68.98 ± 18.07 | |
| Height (cm) (N 94) (N 19) | 1.64 ± 0.06 | 1.62 ± 0.05 | |
| Pre-pregnancy BMI (kg/m2) (N 94) (N 19) | Underweight (<18.5) | 2 (2.1) | 0 |
| Normal weight (18.5–25) | 64 (68.1) | 15 (78.9) | |
| Pre-obese (>25) | 20 (21.3) | 2 (10.5) | |
| Obese (>30) | 8 (8.5) | 2 (10.5) | |
| Chronic diseases (N 13) (N 20) | Hypothyroidism | 4 (30.8) | 0 |
| Asthma | 3 (23.1) | 0 | |
| Pregnancy diseases (N 93) (N 20) | Diabetes | 15 (16.1) | 0 * |
| Preeclampsia | 4 (4.3) | 3 (15.0) | |
| HT | 3 (3.2) | 5 (25.0) * | |
| Urinary infection | 10 (10.8) | 6 (30.0) * | |
| Gestational hypothyroidism | 11 (11.82) | 0 | |
| Pregnancy smoking status (N 94) (N 20) | Non-smokers | 79 (84.0) | 16 (80.0) |
| Not during pregnancy | 7 (7.4) | 3 (15.0) | |
| Yes | 8 (8.5) | 1 (5.0) | |
| Drugs intrapartum (N 94) (N 20) | Antibiotic | 23 (24.5) | 4 (20.0) |
| Corticosteroids | 0 | 4 (20.0) * | |
| Delivery | |||
| Type (N 94) (N 20) | Vaginal | 73 (77.7) | 12 (60.0) |
| Cesarean section | 21 (22.3) | 8 (40) | |
| Parity, n (N 94) (N 20) | 0 | 48 (51.1) | 17 (85.0) * |
| 1 | 38 (40.4) | 2 (10.0) | |
| 2 | 8 (8.5) | 1 (5.0) |
| 6 Months | 12 Months | 24 Months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FT (N 95) | PT (N 20) | FT (N 89) | PT (N 18) | FT (N 68) | PT (N 15) | |||||||
| % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | |
| Oils (g/d) | 36.8 | 9.75 ± 1.45 | 25.0 | 10.00 | 97.8 | 10.49 ± 3.49 | 94.4 | 10.59 ± 2.43 | 98.5 | 12.45 ± 5.76 | 100 | 11.33 ± 3.52 |
| Fruits (g/d) | 56.8 | 261.18 ± 140.18 | 65.0 | 263.25 ± 92.97 | 94.4 | 270.93 ± 160.23 | 83.3 | 352.86 ± 110.47 * | 97.1 | 222.37 ± 145.70 | 80 † | 257.51 ± 162.60 |
| Vegetables (g/d) | 44.2 | 159.90 ± 183.48 | 40.0 | 69.05 ± 33.24 | 98.9 | 145.51 ± 100.00 | 100 | 143.29 ± 83.28 | 94.0 | 91.53 ± 92.67 | 86.7 | 111.78 ± 114.32 |
| Potatoes and tubers (g/d) | 42.1 | 75.74 ± 78.64 | 35.0 | 31.59 ± 26.93 * | 95.5 | 43.32 ± 31.03 | 88.9 | 48.23 ± 20.16 | 100 | 20.54 ± 16.43 | 100 | 26.83 ± 23.31 |
| Cereals and cereal products (g/d) | 17.9 | 17.12 ± 38.63 | 5.0 | 1.42 | 95.5 | 44.16 ± 36.40 | 83.3 | 37.42 ± 23.23 | 100 | 70.52 ± 42.49 | 93.3 | 75.99 ± 32.83 |
| Legumes (g/d) | 4.2 | 20.36 ± 15.84 | 5.0 | 1.42 | 75.3 | 15.33 ± 13.86 | 66.7 | 16.74 ± 14.72 | 93.8 | 18.14 ± 18.60 | 100 | 27.71 ± 40.10 |
| Milk and dairy products 1 | 1.1 | 20.00 | 0.0 | - | 83.0 | 174.35 ± 187.24 | 83.3 | 209.40 ± 132.95 * | 97.1 | 386.69 ± 228.50 | 100 | 410.15 ± 164.45 |
| Meat and meat products (g/d) | 23.2 | 22.15 ± 21.45 | 40.0 | 15.08 ± 6.37 | 96.6 | 33.83 ± 26.76 | 100 | 49.03 ± 33.73 * | 100 | 35.58 ± 19.88 | 100 | 43.45 ± 23.58 |
| Fish (g/d) | 7.4 | 15.10 ± 17.76 | 0.0 | - | 93.3 | 33.53 ± 29.30 | 88.9 | 42.16 ± 37.33 | 92.6 | 39.19 ± 30.95 | 100 | 47.54 ± 44.18 |
| Egg (g/d) | 1.0 | 18.29 | 0.0 | - | 84.3 | 16.93 ± 10.79 | 83.3 | 13.41 ± 4.72 | 82.4 | 21.69 ± 8.44 | 93.3 | 16.96 ± 6.06 * |
| Breast milk (ml/d) | 42.1 | 635.62 ± 217.47 | 15.0 † | 740.00 ± 69.28 | 21.3 | 545.26 ± 113.84 | 11.1 | 450.00 ± 212.13 | - | - | ||
| Infant products | 81.1 | 615.25 ± 402.13 | 95.0 | 600.35 ± 267.13 | 87.6 | 425.49 ± 236.12 | 94.4 | 366.91 ± 215.32 | 57.6 | 108.62 ± 190.10 | 86.7 † | 94.11 ± 95.87 |
| Infant formula (mL) | 74.7 | 628.95 ± 390.08 | 90.0 | 613.06 ± 241.79 | 70.8 | 469.52 ± 139.47 | 72.2 | 419.19 ± 139.38 | 8.8 | 491.67 ± 180.05 | 13.3 | 225.00 ± 21.21 |
| Infant cereal (g/d) | 56.8 | 16.76 ± 13.44 | 90.0 † | 13.21 ± 10.65 | 71.9 | 22.34 ± 11.04 | 88.9 | 20.25 ± 7.53 | 43.1 | 16.28 ± 10.68 | 66.7 | 24.35 ± 9.91 * |
| Infant puree (g/d) | 17.9 | 105.91 ± 87.11 | 15.0 | 50.83 ± 30.21 | 21.3 | 114.02 ± 110.39 | 27.8 | 85.14 ± 59.37 | 2.9 | 98.22 ± 37.88 | 20 † | 45.24 ± 22.96 |
| Sweets and desserts | 8.4 | 3.75 ± 2.42 | 5.0 | 0.85 | 67.4 | 18.37 ± 19.98 | 55.6 | 15.41 ± 21.24 | 82.4 | 25.12 ± 23.88 | 60 | 27.25 ± 20.67 |
| 6 Months | 12 Months | 24 Months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FT (N 95) | PT (N 20) | FT (N 89) | PT (N 18) | FT (N 68) | PT (N 15) | |||||||
| % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | |
| Energy (kcal/d) | 100 | 711.59 ± 261.47 | 100 | 639.97 ± 195.20 | 100 | 1067.68 ± 213.93 | 100 | 1082.43 ± 257.70 | 100 | 1123.22 ± 280.28 | 100 | 1189.88 ± 351.51 |
| Macronutrients | ||||||||||||
| Fat (g/d) | 100 | 31.31 ± 11.35 | 100 | 27.14 ± 9.54 * | 100 | 37.74 ± 7.79 | 100 | 35.03 ± 5.41 | 100 | 39.91 ± 11.66 | 100 | 38.93 ± 5.74 |
| SFA (g/d) | 86.3 | 8.19 ± 6.21 | 95 | 7.86 ± 4.62 | 100 | 10.28 ± 5.05 | 100 | 10.08 ± 3.56 | 100 | 14.35 ± 5.65 | 100 | 14.23 ± 3.44 |
| MUFA (g/d) | 64.2 | 6.34 ± 6.04 | 60 | 5.38 ± 7.40 | 100 | 10.70 ± 3.47 | 100 | 11.36 ± 3.61 | 100 | 16.67 ± 5.36 | 100 | 15.80 ± 2.68 |
| PUFA (g/d) | 70.5 | 1.80 ± 2.80 | 75 | 1.37 ± 2.24 | 100 | 3.17 ± 1.82 | 100 | 3.27 ± 0.97 | 100 | 4.34 ± 1.32 | 100 | 4.61 ± 1.22 |
| Carbohydrate (g/d) | 100 | 92.63 ± 38.36 | 100 | 86.05 ± 29.91 | 100 | 139.92 ± 31.37 | 100 | 144.88 ± 52.07 | 100 | 137.67 ± 42.48 | 100 | 150.17 ± 65.40 |
| Dietary fiber (g/d) | 78.9 | 7.40 ± 5.74 | 95 | 5.27 ± 4.00 | 100 | 14.81 ± 5.14 | 100 | 17.58 ± 10.08 | 100 | 15.26 ± 5.68 | 100 | 19.55 ± 12.85 |
| Protein (g/d) | 100 | 13.62 ± 7.16 | 100 | 12.34 ± 4.29 | 100 | 41.05 ± 14.87 | 100 | 45.64 ± 16.18 | 100 | 52.76 ± 15.33 | 100 | 58.30 ± 18.23 |
| Animal protein (g/d) | 31.6 | 4.23 ± 4.94 | 40 | 3.16 ± 1.29 | 100 | 19.99 ± 12.34 | 100 | 26.09 ± 13.36 * | 100 | 32.88 ± 12.40 | 100 | 35.40 ± 10.41 |
| Vegetal protein (g/d) | 65.3 | 4.00 ± 3.41 | 75 | 2.25 ± 1.30 | 100 | 12.86 ± 5.23 | 100 | 12.72 ± 7.02 | 100 | 17.42 ± 6.79 | 100 | 19.55 ± 13.78 |
| Micronutrients | ||||||||||||
| Vitamin D (μg/d) | 100 | 6.89 ± 3.64 | 100 | 6.99 ± 2.89 | 100 | 6.24 ± 2.78 | 100 | 6.64 ± 2.56 | 100 | 3.13 ± 3.36 | 100 | 3.56 ± 2.08 |
| Vitamin E (mg/d) | 100 | 7.73 ± 4.71 | 100 | 8.09 ± 3.32 | 100 | 9.92 ± 5.19 | 100 | 9.79 ± 3.40 | 100 | 5.65 ± 2.64 | 100 | 6.48 ± 2.87 |
| Folate (μg/d) | 64.2 | 94.85 ± 96.68 | 75 | 68.07 ± 41.01 | 100 | 427.57 ± 209.95 | 100 | 546.95 ± 409.12 | 100 | 497.23 ± 208.35 | 100 | 768.83 ± 184.91 |
| Vitamin B12 (μg/d) | 100 | 2.33 ± 1.29 | 100 | 1.63 ± 1.11 * | 100 | 2.74 ± 1.16 | 100 | 2.68 ± 1.41 | 100 | 3.24 ± 1.67 | 100 | 3.16 ± 1.40 |
| Calcium (mg/d) | 100 | 421.37 ± 194.41 | 100 | 397.29 ± 189.51 | 100 | 678.72 ± 248.89 | 100 | 698.48 ± 172.74 | 100 | 726.71 ± 293.68 | 100 | 766.56 ± 184.91 |
| Selenium (μg/d) | 64.2 | 5.19 ± 9.40 | 75 | 3.10 ± 2.64 | 100 | 39.60 ± 20.12 | 100 | 42.82 ± 26.14 | 100 | 65.98 ± 22.60 | 100 | 73.07 ± 22.74 |
| Iron (mg/d) | 100 | 6.25 ± 3.26 | 100 | 5.70 ± 2.74 | 100 | 10.19 ± 2.90 | 100 | 10.97 ± 4.09 | 100 | 7.80 ± 3.12 | 100 | 10.47 ± 6.02 |
| Copper (mg/d) | 64.2 | 0.21 ± 0.16 | 75 | 0.16 ± 0.09 | 100 | 0.69 ± 0.30 | 100 | 0.82 ± 0.54 | 100 | 0.91 ± 0.32 | 100 | 1.20 ± 0.72 |
| Zinc (mg/d) | 100 | 3.89 ± 2.35 | 100 | 3.83 ± 2.00 | 100 | 6.32 ± 1.97 | 100 | 6.90 ± 1.68 | 100 | 6.63 ± 2.20 | 100 | 7.40 ± 2.92 |
| 6 Months | 12 Months | 24 Months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FT (N 95) | PT (N 20) | FT (N 89) | PT (N 18) | FT (N 68) | PT (N 15) | |||||||
| Bioactive Compounds | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD | % | Mean ± SD |
| Total phenols (mg/d) | 64.2 | 373.55 ± 254.14 | 75.0 | 369.46 ± 216.83 | 100 | 702.77 ± 347.54 | 100 | 896.36 ± 703.85 | 100 | 764.05 ± 361.12 | 100 | 834.57 ± 628.02 |
| Total (poly)phenols (mg/d) 1 | 65.3 | 142.50 ± 99.97 | 75.0 | 126.35 ± 72.60 | 100 | 134.16 ± 73.44 | 100 | 191.02 ± 161.90 | 100 | 127.33 ± 84.92 | 100 | 100.47 ± 78.43 |
| Flavonoids (mg/d) | 65.3 | 104.48 ± 78.26 | 75.0 | 102.54 ± 57.54 | 100 | 89.48 ± 55.96 | 100 | 131.00 ± 120.10 | 100 | 85.23 ± 68.84 | 100 | 66.07 ± 58.23 |
| Anthocyanins | 56.8 | 12.90 ± 8.18 | 70.0 | 11.61 ± 7.91 | 95.6 | 24.94 ± 27.58 | 88.8 | 44.20 ± 47.34 | 100 | 28.28 ± 32.78 | 86.7 | 23.74 ± 26.25 |
| Dihydrochalcones | 53.7 | 1.56 ± 0.97 | 60.0 | 1.53 ± 0.42 | 88.8 | 1.48 ± 1.22 | 77.8 | 2.25 ± 1.91 * | 82.4 | 1.29 ± 1.25 | 60 | 0.93 ± 1.02 |
| Flavanols | 64.2 | 74.07 ± 57.84 | 75.0 | 67.95 ± 40.11 | 100 | 44.32 ± 31.81 | 100 | 62.19 ± 57.00 | 100 | 38.93 ± 32.57 | 100 | 27.90 ± 27.77 |
| Flavanones | 58.9 | 20.98 ± 22.77 | 75.0 | 22.47 ± 18.39 | 96.6 | 19.78 ± 20.98 | 100 | 27.14 ± 42.38 | 100 | 15.78 ± 22.80 | 86.7 | 18.03 ± 21.15 |
| Flavones | 64.2 | 0.14 ± 0.24 | 75.0 | 0.05 ± 0.14 * | 100 | 0.56 ± 0.56 | 100 | 0.50 ± 0.40 | 100 | 0.53 ± 0.57 | 100 | 0.77 ± 0.98 |
| Flavonols | 64.2 | 6.86 ± 5.83 | 75.0 | 5.84 ± 4.36 | 100 | 19.96 ± 23.91 | 100 | 25.54 ± 32.79 | 100 | 18.13 ± 20.07 | 100 | 18.30 ± 21.68 |
| Isoflavanoids | 65.3 | 0.01 ± 0.01 | 75.0 | 0.00 ± 0.00 * | 100 | 0.34 ± 1.06 | 100 | 0.13 ± 0.18 | 100 | 0.65 ± 1.38 | 100 | 0.64 ± 0.63 |
| Phenolic acids (mg/d) | 63.2 | 35.93 ± 28.73 | 70.0 | 25.15 ± 15.71 | 100 | 43.38 ± 21.77 | 100 | 58.88 ± 42.11 | 100 | 40.08 ± 20.27 | 100 | 32.30 ± 21.66 |
| Lignans (mg/d) | 29.5 | 5.49 ± 11.30 | 10.0 | 1.13 ± 1.14 | 92.1 | 0.11 ± 0.15 | 100 | 0.13 ± 0.15 | 94.1 | 0.16 ± 0.20 | 100 | 0.15 ± 0.12 |
| Non-phenolic metabolites (mg/d) | 64.2 | 0.25 ± 0.31 | 75.0 | 0.20 ± 0.14 | 100 | 1.18 ± 0.60 | 100 | 1.52 ± 0.84 | 100 | 1.77 ± 0.56 | 100 | 2.07 ± 0.70 |
| Other polyphenols (mg/d) | 23.2 | 2.15 ± 1.15 | 5.0 | 2.75 | 84.3 | 1.43 ± 2.17 | 88.8 | 1.12 ± 1.36 | 91.1 | 2.06 ± 3.29 | 93.3 | 2.09 ± 2.63 |
| Dietary fiber (g/d) | 78.9 | 7.40 ± 5.74 | 95.0 | 5.25 ± 4.00 | 100 | 14.81 ± 5.12 | 100 | 17.58 ± 10.08 | 100 | 15.26 ± 5.68 | 100 | 19.55 ± 12.85 |
| Insoluble | 65.3 | 4.94 ± 3.34 | 75.0 | 4.10 ± 2.17 | 100 | 9.68 ± 4.22 | 100 | 11.74 ± 8.17 | 100 | 9.73 ± 3.93 | 100 | 11.59 ± 8.32 |
| Soluble | 66.3 | 1.47 ± 1.11 | 80.0 | 1.26 ± 1.23 | 100 | 2.15 ± 0.91 | 100 | 2.66 ± 1.26 * | 100 | 1.70 ± 0.67 | 100 | 2.82 ± 1.40 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Martín, M.; Herrero-Morín, D.; Solís, G.; Suarez, M.; Fernández, N.; Arboleya, S.; Gueimonde, M.; González, S. Longitudinal Study Depicting Differences in Complementary Feeding and Anthropometric Parameters in Late Preterm Infants up to 2 Years of Age. Nutrients 2021, 13, 982. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030982
Gómez-Martín M, Herrero-Morín D, Solís G, Suarez M, Fernández N, Arboleya S, Gueimonde M, González S. Longitudinal Study Depicting Differences in Complementary Feeding and Anthropometric Parameters in Late Preterm Infants up to 2 Years of Age. Nutrients. 2021; 13(3):982. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030982
Chicago/Turabian StyleGómez-Martín, María, David Herrero-Morín, Gonzalo Solís, Marta Suarez, Nuria Fernández, Silvia Arboleya, Miguel Gueimonde, and Sonia González. 2021. "Longitudinal Study Depicting Differences in Complementary Feeding and Anthropometric Parameters in Late Preterm Infants up to 2 Years of Age" Nutrients 13, no. 3: 982. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030982