
Associations of Dietary Patterns with Incident Depression: The Maastricht Study

 , , ,
, , ,  , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
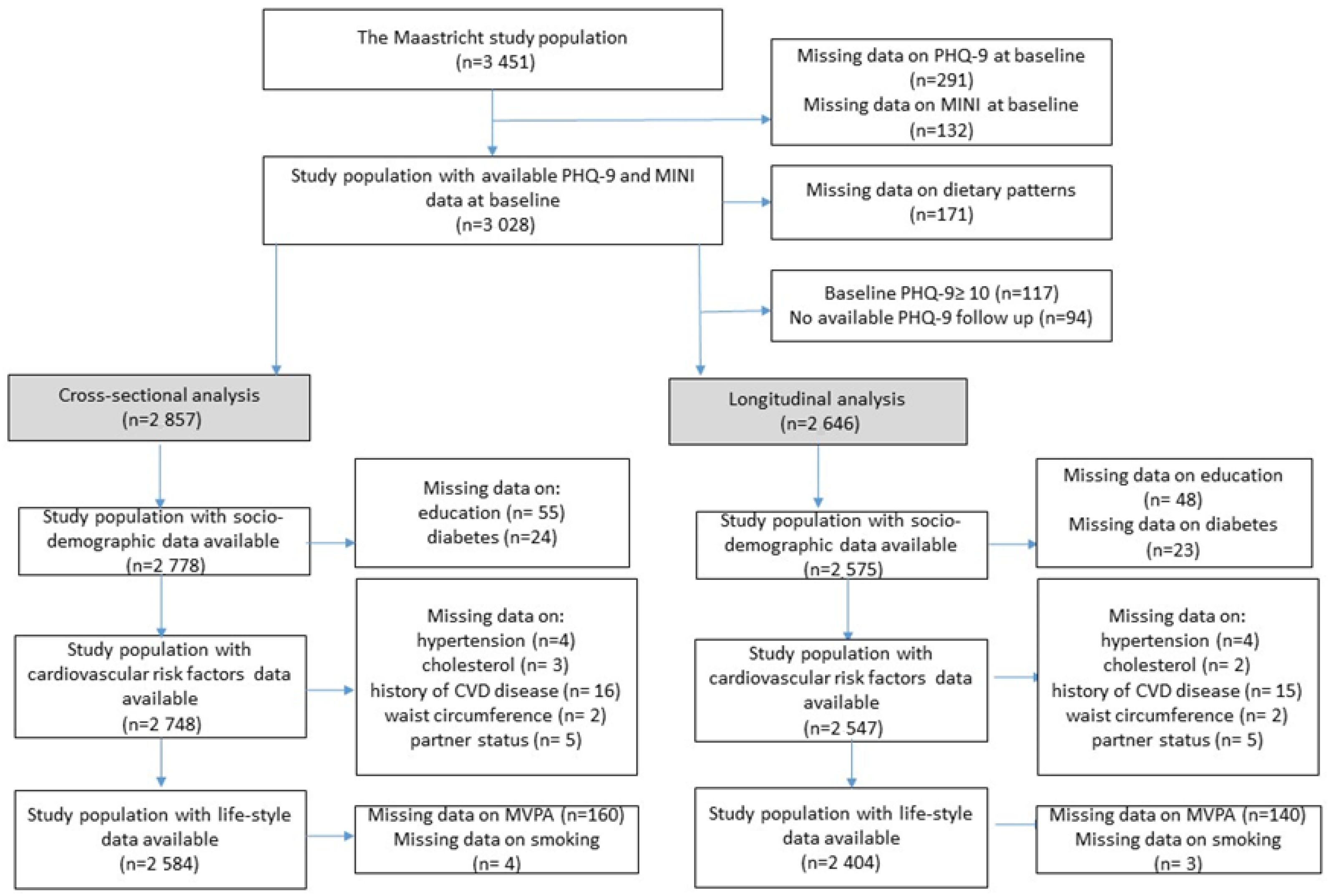
2.1. Study Population and Design
2.2. Assessment of Depression at Baseline
2.3. Assessment of Depression during Follow-Up
2.4. Assessment of Dietary Patterns
2.4.1. Dutch Healthy Diet Score
2.4.2. Mediterranean Diet and Dietary Approaches to Stop Hypertension Scores
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Descriptive Characteristics of the Population
3.2. Dietary Patterns and Incident and Prevalent Depressive Symptoms
3.3. Sensitivity Analysis
4. Discussion
4.1. Potential Biological Mechanisms
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Lancet. Global Burden of Disease Study 2015 Assesses the State of the World’s Health. 2016. Available online: http://www.thelancet.com/gbd (accessed on 15 December 2020).
- Deane, K.H.O.; Jimoh, O.F.; Biswas, P.; O’Brien, A.; Hanson, S.; Abdelhamid, A.S.; Fox, C.; Hooper, L. Omega-3 and polyunsaturated fat for prevention of depression and anxiety symptoms: Systematic review and meta-analysis of randomised trials. Br. J. Psychiatry 2021, 218, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, F.; Salari-Moghaddam, A.; Larijani, B.; Esmaillzadeh, A. Adherence to the Mediterranean diet and risk of depression: A systematic review and updated meta-analysis of observational studies. Nutr. Rev. 2019, 77, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Nicolaou, M.; Colpo, M.; Vermeulen, E.; Elstgeest, L.E.M.; Cabout, M.; Gibson-Smith, D.; Knuppel, A.; Sini, G.; Schoenaker, D.A.J.M.; Mishra, G.D.; et al. Association of a priori dietary patterns with depressive symptoms: A harmonised meta-analysis of observational studies. Psychol. Med. 2019, 50, 1872–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khayyatzadeh, S.S.; Mehramiz, M.; Mirmousavi, S.J.; Mazidi, M.; Ziaee, A.; Kazemi-Bajestani, S.M.R.; Ferns, G.A.; Moharreri, F.; Ghayour-mobarhan, M. Adherence to a Dash-style diet in relation to depression and aggression in adolescent girls. Psychiatry Res. 2018, 259, 104–109. [Google Scholar] [CrossRef]
- Perez-Cornago, A.; Sanchez-Villegas, A.; Bes-Rastrollo, M.; Gea, A.; Molero, P.; Lahortiga-Ramos, F.; Martinez-Gonzalez, M.Á. Relationship between adherence to Dietary Approaches to Stop Hypertension (DASH) diet indices and incidence of depression during up to 8 years of follow-up. Public Health Nutr. 2017, 20, 2383–2392. [Google Scholar] [CrossRef] [Green Version]
- Looman, M.; Feskens, E.J.; de Rijk, M.; Meijboom, S.; Biesbroek, S.; Temme, E.H.; de Vries, J.; Geelen, A. Development and evaluation of the Dutch Healthy Diet index 2015. Public Health Nutr. 2017, 20, 2289–2299. [Google Scholar] [CrossRef]
- Vogtschmidt, Y.D.; Nefs, G.; Speight, J.; Bot, M.; Pouwer, F.; Soedamah-Muthu, S.S. Depressive and anxiety symptoms and following of the Dutch Dietary Guidelines 2015 in adults with diabetes: Results from Diabetes MILES-The Netherlands. J. Psychosom. Res. 2020, 135, 110160. [Google Scholar] [CrossRef]
- Sanchez-Villegas, A.; Martinez-Gonzalez, M.A. Diet, a new target to prevent depression? BMC Med. 2013, 11, 3. [Google Scholar] [CrossRef] [Green Version]
- Schram, M.T.; Sep, S.J.; van der Kallen, C.J.; Dagnelie, P.C.; Koster, A.; Schaper, N.; Henry, R.M.A.; Stehouwer, C.D.A. The Maastricht Study: An extensive phenotyping study on determinants of type 2 diabetes, its complications and its comorbidities. Eur. J. Epidemiol. 2014, 29, 439–451. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Smolderen, K.G.; Spertus, J.A.; Reid, K.J.; Buchanan, D.M.; Krumholz, H.M.; Denollet, J.; Vaccarino, V.; Chan, P.S. The association of cognitive and somatic depressive symptoms with depression recognition and outcomes after myocardial infarction. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 328–337. [Google Scholar] [CrossRef] [Green Version]
- Pettersson, A.; Bostrom, K.B.; Gustavsson, P.; Ekselius, L. Which instruments to support diagnosis of depression have sufficient accuracy? A systematic review. Nord. J. Psychiatry 2015, 69, 497–508. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33; quiz 34–57. [Google Scholar] [PubMed]
- Molag, M.L.; de Vries, J.H.; Duif, N.; Ocke, M.C.; Dagnelie, P.C.; Goldbohm, R.A.; van’t Veer, P. Selecting informative food items for compiling food-frequency questionnaires: Comparison of procedures. Br. J. Nutr. 2010, 104, 446–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dongen, M.C.; Wijckmans-Duysens, N.E.G.; den Biggelaar, L.J.; Ocke, M.C.; Meijboom, S.; Brants, H.A.; de Vries, J.H.M.; Feskens, E.J.M.; Bueno-de-Mesquita, H.B.; Geelen, A.; et al. The Maastricht FFQ: Development and validation of a comprehensive food frequency questionnaire for the Maastricht study. Nutrition 2019, 62, 39–46. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Public Health and the Environment Ministry of Health Welfare and Sport. Dutch Food Composition Database 2011; National Institute for Public Health and the Environment Ministry of Health Welfare and Sport: Bilhoven, The Netherlands, 2011.
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocke, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Global Burden of Disease: 2004 Update; Health Statistics and Information Systems: Geneva, Switzerland, 2008. [Google Scholar]
- Cherian, L.; Wang, Y.; Holland, T.; Agarwal, P.; Aggarwal, N.; Morris, M.C. DASH and Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) Diets are Associated with Fewer Depressive Symptoms Over Time. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, 151–156. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nucci, D.; Fatigoni, C.; Amerio, A.; Odone, A.; Gianfredi, V. Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6686. [Google Scholar] [CrossRef] [PubMed]
- Van Dooren, F.E.; Schram, M.T.; Schalkwijk, C.G.; Stehouwer, C.D.; Henry, R.M.; Dagnelie, P.C.; Schaper, N.C.; van der Kallen, C.J.H.; Koster, A.; Sep, S.J.S.; et al. Associations of low grade inflammation and endothelial dysfunction with depression—The Maastricht Study. Brain Behav. Immun. 2016, 56, 390–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Agtmaal, M.J.M.; Houben, A.; Pouwer, F.; Stehouwer, C.D.A.; Schram, M.T. Association of Microvascular Dysfunction With Late-Life Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry 2017, 74, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Geraets, A.F.J.; van Agtmaal, M.J.M.; Stehouwer, C.D.A.; Sorensen, B.M.; Berendschot, T.; Webers, C.A.B.; Schaper, N.C.; Henry, R.M.A.; van der Kallen, C.J.H.; Eussen, S.J.P.M.; et al. Association of Markers of Microvascular Dysfunction With Prevalent and Incident Depressive Symptoms: The Maastricht Study. Hypertension 2020, 76, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Geraets, A.F.J.; Kohler, S.; Muzambi, R.; Schalkwijk, C.G.; Oenema, A.; Eussen, S.; Dagnelie, P.C.; Stehouwer, C.D.A.; Schaper, N.C.; Henry, R.M.A.; et al. The association of hyperglycaemia and insulin resistance with incident depressive symptoms over 4 years of follow-up: The Maastricht Study. Diabetologia 2020, 63, 2315–2328. [Google Scholar] [CrossRef]
- Van Dooren, F.E.; Pouwer, F.; Schalkwijk, C.G.; Sep, S.J.; Stehouwer, C.D.; Henry, R.M.; Dagnelie, P.C.; Schaper, N.C.; van der Kallen, C.J.H.; Koster, A.; et al. Advanced Glycation End Product (AGE) Accumulation in the Skin is Associated with Depression: The Maastricht Study. Depress. Anxiety 2017, 34, 59–67. [Google Scholar] [CrossRef]
- Bot, M.; Milaneschi, Y.; Al-Shehri, T.; Amin, N.; Garmaeva, S.; Onderwater, G.L.J.; Pool, R.; Thesing, C.S.; Vijfhuizen, L.S.; Vogelzangs, N.; et al. Metabolomics Profile in Depression: A Pooled Analysis of 230 Metabolic Markers in 5283 Cases With Depression and 10,145 Controls. Biol. Psychiatry 2020, 87, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Lima, B.B.; Hammadah, M.; Kim, J.H.; Uphoff, I.; Shah, A.; Levantsevych, O.; Almuwaqqat, Z.; Moazzami, K.; Sullivan, S.; Ward, L.; et al. Association of Transient Endothelial Dysfunction Induced by Mental Stress With Major Adverse Cardiovascular Events in Men and Women with Coronary Artery Disease. JAMA Cardiol. 2019, 4, 988–996. [Google Scholar] [CrossRef]
- Gianfredi, V.; Blandi, L.; Cacitti, S.; Minelli, M.; Signorelli, C.; Amerio, A.; Odone, A. Depression and Objectively Measured Physical Activity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3738. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | No Incident Depressive Symptoms (PHQ-9 < 10 during Follow-Up) n = 2331 | Incident Clinically Relevant Depressive Symptoms (PHQ-9 ≥ 10) during Follow-Up n = 315 | p-Value |
|---|---|---|---|
| Sex (women) | 1154 (49.5) | 157 (49.8) | 0.911 |
| Age (years) | 59.92 ± 8.02 | 59.78 ± 8.35 | 0.767 |
| Education | 0.000 | ||
| Low | 680 (29.7) | 123 (39.9) | |
| Medium | 650 (28.4) | 98 (31.8) | |
| High | 960 (41.9) | 87 (28.8) | |
| Smoking | 0.000 | ||
| Never | 850 (36.9) | 100 (32.2) | |
| Former | 1223 (53.2) | 153 (49.2) | |
| Current | 228 (9.9) | 58 (18.6) | |
| Waist circumference (cm) * | 94.55 ± 12.96 | 99.46 ± 14.91 | 0.000 |
| BMI (kg/m2) | 26.64 (4.23) | 28.28 (4.93) | 0.000 |
| Hypertension | 1267 (54.4) | 202 (64.1) | 0.001 |
| Total cholesterol-to-HDL cholesterol ratio * | 3.63 ± 1.15 | 3.77 ± 1.24 | 0.037 |
| History of CVD | 350 (15.3) | 72 (23.3) | 0.000 |
| Diabetes | 0.000 | ||
| No diabetes | 1422 (61.5) | 141 (45.8) | |
| Pre-diabetes | 362 (15.7) | 44 (14.3) | |
| T2DM | 529 (22.9) | 123 (39.9) | |
| MVPA (hours/week) * | 5.76 ± 4.33 | 4.45 ± 4.05 | 0.000 |
| Having a partner (yes) | 1975 (85.8) | 257 (83.4) | 0.262 |
| Depression | |||
| Depression score at baseline (PHQ-9 score) * | 1.95 ± 20.7 | 4.25 ± 2.72 | 0.000 |
| Major depressive disorder at baseline (MINI) | 21 (0.9) | 18 (5.7) | 0.000 |
| Use of antidepressants at baseline | 103 (4.4) | 45 (14.3) | 0.000 |
| Diet * | |||
| Energy intake (Kcal) | 2177 ± 595 | 2232 ± 630 | 0.125 |
| Protein total (g/day) | 85.6 ± 22.5 | 87.4 ± 25.0 | 0.196 |
| Carbohydrates total (g/day) | 231.8 ± 68.1 | 238.0 ± 74.6 | 0.135 |
| Fat total (g/day) | 83.9 ± 30.7 | 88.3 ± 32.1 | 0.018 |
| Fatty acids total saturated (g/day) | 29.4 ± 11.9 | 31.3 ± 12.4 | 0.011 |
| Fatty acids total monounsaturated (d/day) | 29.6 ± 11.3 | 30.8 ± 11.2 | 0.059 |
| Fatty acids total polyunsaturated (g/day) | 17.6 ± 7.7 | 18.6 ± 8.4 | 0.044 |
| Alcohol intake (g/day) | 12.8 ± 13.8 | 10.5 ± 14.5 | 0.003 |
| DHD, (range 0–140) | 84.37 ± 14.50 | 79.68 ± 15.11 | 0.000 |
| Mediterranean Diet Score, (range 0–9) | 4.61 ± 1.64 | 4.32 ± 1.60 | 0.003 |
| DASH score, (range 8–40) | 24.24 ± 4.51 | 23.11 ± 4.37 | 0.000 |
| Incident Clinically Relevant Depressive Symptoms (PHQ-9 ≥ 10) | Incident Rate Per 1000 Person Years n = 2646 | Model 1 HR (95% CI) n = 315/2273 | Model 2 HR (95% CI) n = 298/2249 | Model 3 HR (95% CI) n = 280/2124 |
|---|---|---|---|---|
| DHD-score | ||||
| Standardized score * | 0.75 (0.67–0.85) | 0.78 (0.69–0.89) | 0.83 (0.73–0.96) | |
| Tertiles | ||||
| Low (≤77.27) | [n = 139] 9.15 | Ref | Ref | Ref |
| Medium (77.27–90.43) | [n = 96] 6.32 | 0.70 (0.53–0.91) | 0.74 (0.56–0.97) | 0.83 (0.63–1.12) |
| High(>90.43) | [n = 80] 5.27 | 0.61 (0.45–0.82) | 0.66 (0.49–0.90) | 0.77 (0.55–1.06) |
| Linear trend p-value + | 0.006 | 0.031 | 0.246 | |
| Mediterranean Diet Score | ||||
| Standardized score * | 0.87 (0.77–0.98) | 0.89 (0.79–1.01) | 0.92 (0.81–1.05) | |
| Cut-off ** | ||||
| Low (0–3) | [n = 94] 6.18 | Ref | Ref | Ref |
| Medium (4–6) | [n = 72] 4.74 | 0.90 (0.66–1.23) | 0.93 0.68–1.28) | 0.94 (0.68–1.31) |
| High (6–9) | [n = 149] 9.81 | 0.82 (0.63–1.07) | 0.88 (0.67–1.16) | 0.96 (0.72–1.28) |
| Linear trend p-value + | 0.354 | 0.570 | 0.758 | |
| DASH score * | ||||
| Standardized score | 0.85 (0.75–0.95) | 0.87 (0.77–0.98) | 0.95 (0.83–1.07) | |
| Tertiles | ||||
| Low (≤22) | [n = 139] 9.15 | Ref | Ref | Ref |
| Medium (22–26) | [n = 110] 7.24 | 0.94 (0.73–1.22) | 0.97 (0.75–1.26) | 1.06 (0.81–1.39) |
| High (>26) | [n = 66] 4.35 | 0.66 (0.49–0.90) | 0.71 (0.52–0.97) | 0.83 (0.60–1.15) |
| Linear trend p-value + | 0.024 | 0.076 | 0.477 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianfredi, V.; Koster, A.; Odone, A.; Amerio, A.; Signorelli, C.; Schaper, N.C.; Bosma, H.; Köhler, S.; Dagnelie, P.C.; Stehouwer, C.D.A.; et al. Associations of Dietary Patterns with Incident Depression: The Maastricht Study. Nutrients 2021, 13, 1034. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031034
Gianfredi V, Koster A, Odone A, Amerio A, Signorelli C, Schaper NC, Bosma H, Köhler S, Dagnelie PC, Stehouwer CDA, et al. Associations of Dietary Patterns with Incident Depression: The Maastricht Study. Nutrients. 2021; 13(3):1034. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031034
Chicago/Turabian StyleGianfredi, Vincenza, Annemarie Koster, Anna Odone, Andrea Amerio, Carlo Signorelli, Nicolaas C. Schaper, Hans Bosma, Sebastian Köhler, Pieter C. Dagnelie, Coen D.A. Stehouwer, and et al. 2021. "Associations of Dietary Patterns with Incident Depression: The Maastricht Study" Nutrients 13, no. 3: 1034. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13031034