
The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes

 ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
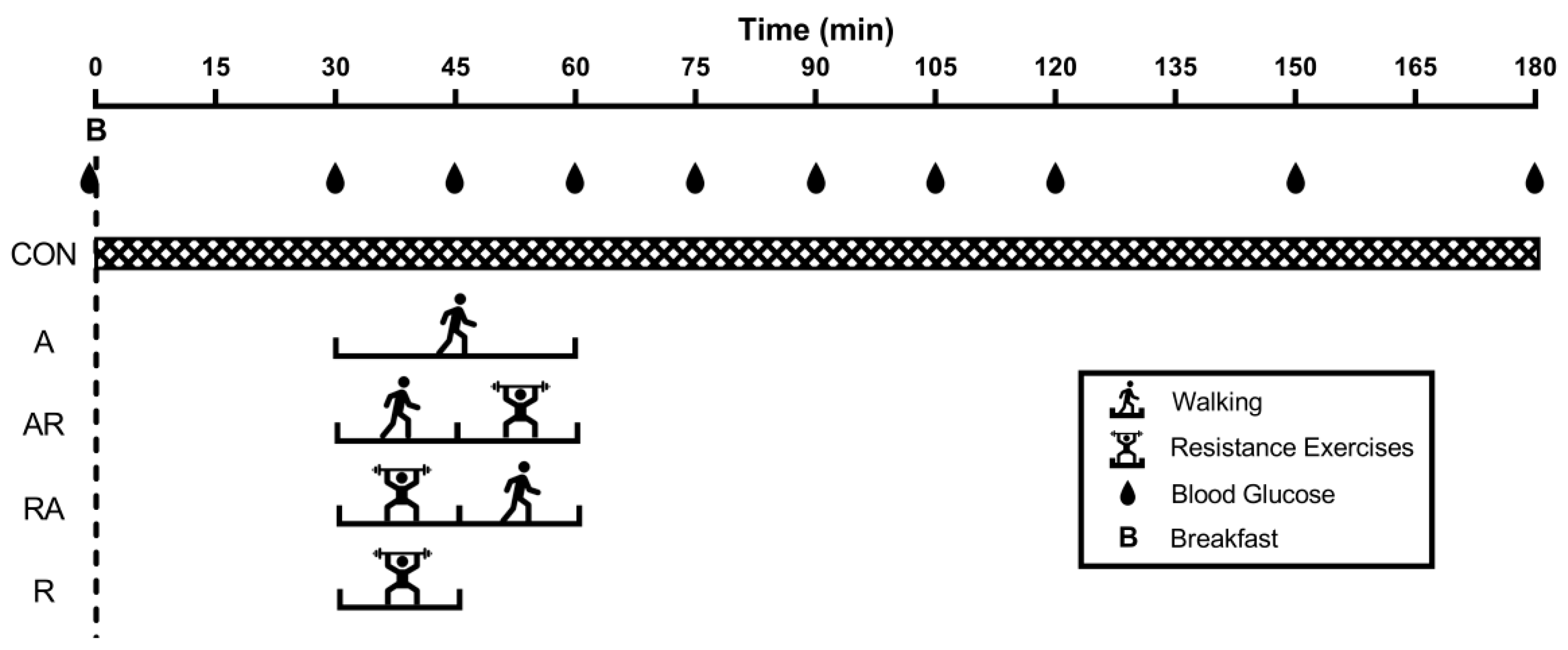
2.2. Study Design
2.3. Familiarization
2.4. Breakfast
2.5. Exercise and Sitting Time
2.6. Glycemic Assessment
2.7. Calculation and Statistical Analysis
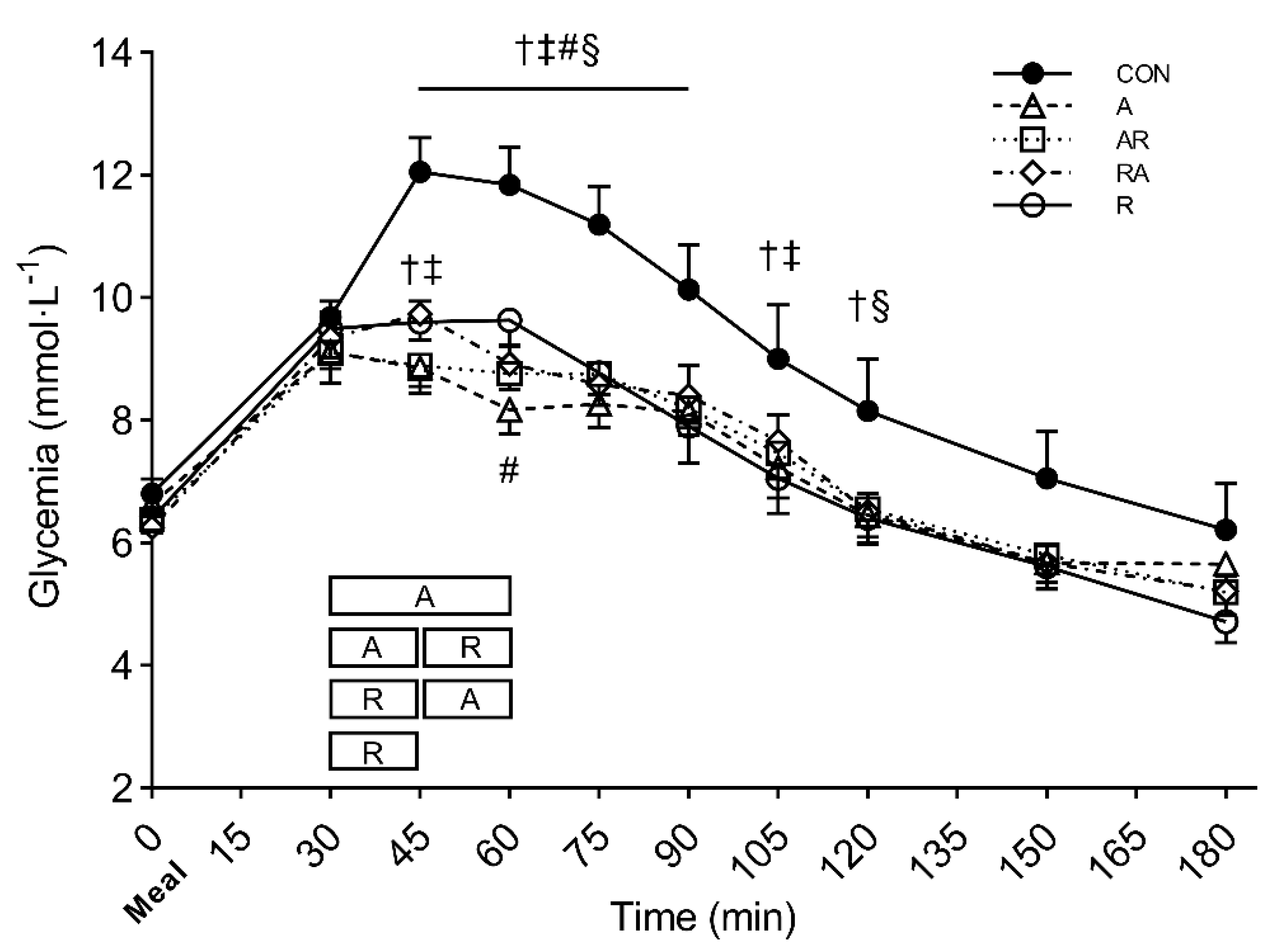
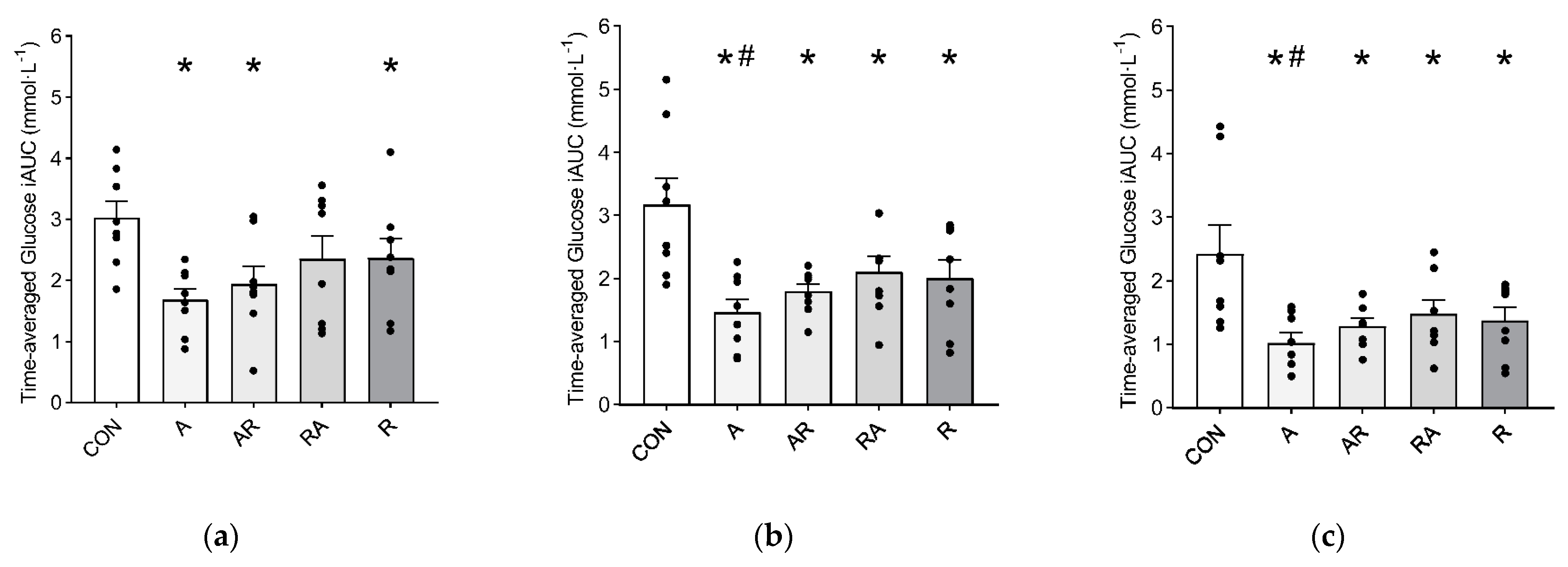
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ceriello, A.; Esposito, K.; Piconi, L.; Ihnat, M.A.; Thorpe, J.E.; Testa, R.; Boemi, M.; Giugliano, D. Oscillating Glucose Is More Deleterious to Endothelial Function and Oxidative Stress Than Mean Glucose in Normal and Type 2 Diabetic Patients. Diabetes 2008, 57, 1349–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceriello, A.; Genovese, S. Atherogenicity of Postprandial Hyperglycemia and Lipotoxicity. Rev. Endocr. Metab. Disord. 2016, 17, 111–116. [Google Scholar] [CrossRef]
- Zanuso, S.; Sacchetti, M.; Sundberg, C.J.; Orlando, G.; Benvenuti, P.; Balducci, S. Exercise in Type 2 Diabetes: Genetic, Metabolic and Neuromuscular Adaptations. A Review of the Evidence. Br. J. Sports Med. 2017, 51, 1533–1538. [Google Scholar] [CrossRef] [PubMed]
- Bellini, A.; Nicolò, A.; Bazzucchi, I.; Sacchetti, M. Effects of Different Exercise Strategies to Improve Postprandial Glycemia in Healthy Individuals. Med. Sci. Sports Exerc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Aqeel, M.; Forster, A.; Richards, E.; Hennessy, E.; McGowan, B.; Bhadra, A.; Guo, J.; Gelfand, S.; Delp, E.; Eicher-Miller, H. The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review. Nutrients 2020, 12, 221. [Google Scholar] [CrossRef] [Green Version]
- Sacchetti, M.; Haxhi, J.; Sgrò, P.; Scotto di Palumbo, A.; Nicolò, A.; Bellini, A.; Bazzucchi, I.; di Luigi, L. Effects of Exercise before and/or after a Mixed Lunch on Postprandial Metabolic Responses in Healthy Male Individuals. Eur. J. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Haxhi, J.; Scotto di Palumbo, A.; Sacchetti, M. Exercising for Metabolic Control: Is Timing Important. Ann. Nutr. Metab. 2013, 62, 14–25. [Google Scholar] [CrossRef]
- Chacko, E. Exercising Tactically for Taming Postmeal Glucose Surges. Scientifica 2016, 2016, 4045717. [Google Scholar] [CrossRef]
- Balducci, S.; Sacchetti, M.; Haxhi, J.; Orlando, G.; D’Errico, V.; Fallucca, S.; Menini, S.; Pugliese, G. Physical Exercise as Therapy for Type 2 Diabetes Mellitus: Exercise as Therapy for Type 2 Diabetes. Diabetes Metab. Res. Rev. 2014, 30, 13–23. [Google Scholar] [CrossRef]
- Zanuso, S.; Jimenez, A.; Pugliese, G.; Corigliano, G.; Balducci, S. Exercise for the Management of Type 2 Diabetes: A Review of the Evidence. Acta Diabetol. 2010, 47, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effects of Aerobic Training, Resistance Training, or Both on Glycemic Control in Type 2 Diabetes: A Randomized Trial. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar] [CrossRef]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q.; et al. Effects of Aerobic and Resistance Training on Hemoglobin A1c Levels in Patients with Type 2 Diabetes: A Randomized Controlled Trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [Green Version]
- Praet, S.F.; Manders, R.J.; Lieverse, A.G.; Kuipers, H.; Stehouwer, C.D.; Keizer, H.A.; Van Loon, L.J. Influence of Acute Exercise on Hyperglycemia in Insulin-Treated Type 2 Diabetes. Med. Sci. Sports Exerc. 2006, 38, 2037–2044. [Google Scholar] [CrossRef]
- Figueira, F.R.; Umpierre, D.; Casali, K.R.; Tetelbom, P.S.; Henn, N.T.; Ribeiro, J.P.; Schaan, B.D. Aerobic and Combined Exercise Sessions Reduce Glucose Variability in Type 2 Diabetes: Crossover Randomized Trial. PLoS ONE 2013, 8, e57733. [Google Scholar] [CrossRef] [PubMed]
- Yardley, J.E.; Kenny, G.P.; Perkins, B.A.; Riddell, M.C.; Malcolm, J.; Boulay, P.; Khandwala, F.; Sigal, R.J. Effects of Performing Resistance Exercise before Versus after Aerobic Exercise on Glycemia in Type 1 Diabetes. Diabetes Care 2012, 35, 669–675. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Yardley, J.E.; Hay, J.; Abou-Setta, A.M.; Marks, S.D.; McGavock, J. A Systematic Review and Meta-Analysis of Exercise Interventions in Adults with Type 1 Diabetes. Diabetes Res. Clin. Pract. 2014, 106, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Rowe, D.A.; Welk, G.J.; Heil, D.P.; Mahar, M.T.; Kemble, C.D.; Calabró, M.A.; Camenisch, K. Stride Rate Recommendations for Moderate-Intensity Walking. Med. Sci. Sports Exerc. 2011, 43, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Klaff, L.J.; Brazg, R.; Hughes, K.; Tideman, A.M.; Schachner, H.C.; Stenger, P.; Pardo, S.; Dunne, N.; Parkes, J.L. Accuracy Evaluation of Contour Next Compared with Five Blood Glucose Monitoring Systems across a Wide Range of Blood Glucose Concentrations Occurring in a Clinical Research Setting. Diabetes Technol. Ther. 2015, 17, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Narang, B.J.; Atkinson, G.; Gonzalez, J.T.; Betts, J.A. A Tool to Explore Discrete-Time Data: The Time Series Response Analyser. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 374–381. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Solomon, T.P.; Eves, F.F.; Laye, M.J. Targeting Postprandial Hyperglycemia with Physical Activity May Reduce Cardiovascular Disease Risk. But What Should We Do, and When Is the Right Time to Move? Front. Cardiovasc. Med. 2018, 5, 99. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.Y.; Kanaley, J.A.; Guelfi, K.J.; Cook, S.B.; Hebert, J.J.; Forrest, M.R.; Fairchild, T.J. Exercise Timing in Type 2 Diabetes Mellitus: A Systematic Review. Med. Sci. Sports Exerc. 2018, 50, 2387–2397. [Google Scholar] [CrossRef]
- Peddinti, G.; Bergman, M.; Tuomi, T.; Groop, L. 1-Hour Post-OGTT Glucose Improves the Early Prediction of Type 2 Diabetes by Clinical and Metabolic Markers. J. Clin. Endocrinol. Metab. 2019, 104, 1131–1140. [Google Scholar] [CrossRef] [Green Version]
- Gurudut, P.; Rajan, A.P. Immediate Effect of Passive Static Stretching versus Resistance Exercises on Postprandial Blood Sugar Levels in Type 2 Diabetes Mellitus: A Randomized Clinical Trial. J. Exerc. Rehabil. 2017, 13, 581–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heden, T.D.; Winn, N.C.; Mari, A.; Booth, F.W.; Rector, R.S.; Thyfault, J.P.; Kanaley, J.A. Postdinner Resistance Exercise Improves Postprandial Risk Factors More Effectively than Predinner Resistance Exercise in Patients with Type 2 Diabetes. J. Appl. Physiol. 2015, 118, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borror, A.; Zieff, G.; Battaglini, C.; Stoner, L. The Effects of Postprandial Exercise on Glucose Control in Individuals with Type 2 Diabetes: A Systematic Review. Sports Med. 2018, 48, 1479–1491. [Google Scholar] [CrossRef]
- Yardley, J.E.; Sigal, R.J.; Riddell, M.C.; Perkins, B.A.; Kenny, G.P. Performing Resistance Exercise before versus after Aerobic Exercise Influences Growth Hormone Secretion in Type 1 Diabetes. Appl. Physiol. Nutr. Metab. 2014, 39, 262–265. [Google Scholar] [CrossRef]
- Sylow, L.; Kleinert, M.; Richter, E.A.; Jensen, T.E. Exercise-Stimulated Glucose Uptake—Regulation and Implications for Glycaemic Control. Nat. Rev. Endocrinol. 2017, 13, 133–148. [Google Scholar] [CrossRef]
- Bergouignan, A.; Latouche, C.; Heywood, S.; Grace, M.S.; Reddy-Luthmoodoo, M.; Natoli, A.K.; Owen, N.; Dunstan, D.W.; Kingwell, B.A. Frequent Interruptions of Sedentary Time Modulates Contraction- and Insulin-Stimulated Glucose Uptake Pathways in Muscle: Ancillary Analysis from Randomized Clinical Trials. Sci. Rep. 2016, 6, 32044. [Google Scholar] [CrossRef] [PubMed]
- Holst, J.J.; Gribble, F.; Horowitz, M.; Rayner, C.K. Roles of the Gut in Glucose Homeostasis. Diabetes Care 2016, 39, 884–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiavon, M.; Hinshaw, L.; Mallad, A.; Man, C.D.; Sparacino, G.; Johnson, M.; Carter, R.; Basu, R.; Kudva, Y.; Cobelli, C.; et al. Postprandial Glucose Fluxes and Insulin Sensitivity during Exercise: A Study in Healthy Individuals. Am. J. Physiol. Endocrinol. Metab. 2013, 305, E557–E566. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, A.; Nicolò, A.; Bulzomì, R.; Bazzucchi, I.; Sacchetti, M. The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes. Nutrients 2021, 13, 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051440
Bellini A, Nicolò A, Bulzomì R, Bazzucchi I, Sacchetti M. The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes. Nutrients. 2021; 13(5):1440. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051440
Chicago/Turabian StyleBellini, Alessio, Andrea Nicolò, Rocco Bulzomì, Ilenia Bazzucchi, and Massimo Sacchetti. 2021. "The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes" Nutrients 13, no. 5: 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13051440