
Acute Administration of Bioavailable Curcumin Alongside Ferrous Sulphate Supplements Does Not Impair Iron Absorption in Healthy Adults in a Randomised Trial


Abstract
:
1. Introduction
2. Materials and Methods
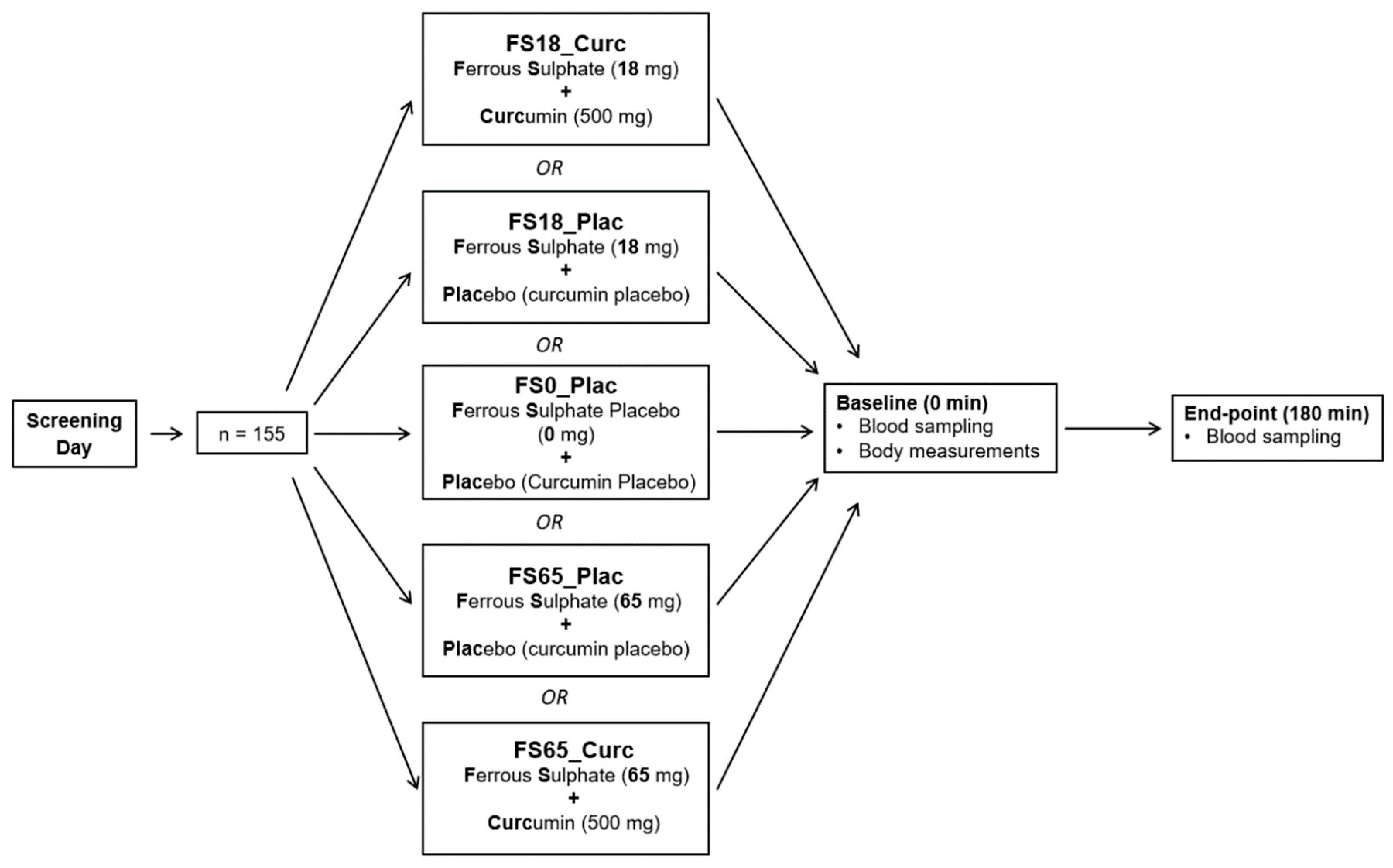
2.1. Study Design
2.2. Ethics Approval and Study Registration
2.3. Inclusion and Exclusion Criteria
2.4. Safety Screening
2.5. Participants
2.6. Supplements
2.7. Physical Examination
2.8. Blood Sample Collection and Processing
2.9. Analysis of Serum Ferritin Concentration
2.10. Analysis of Serum Iron Profile
2.11. Analysis of Whole Blood Haemoglobin (HGB) Concentration
2.12. Analysis of Serum Thiobarbituric Acid Reactive Substances (TBARS) Concentration
2.13. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Baseline Levels of Assessed Biomarkers
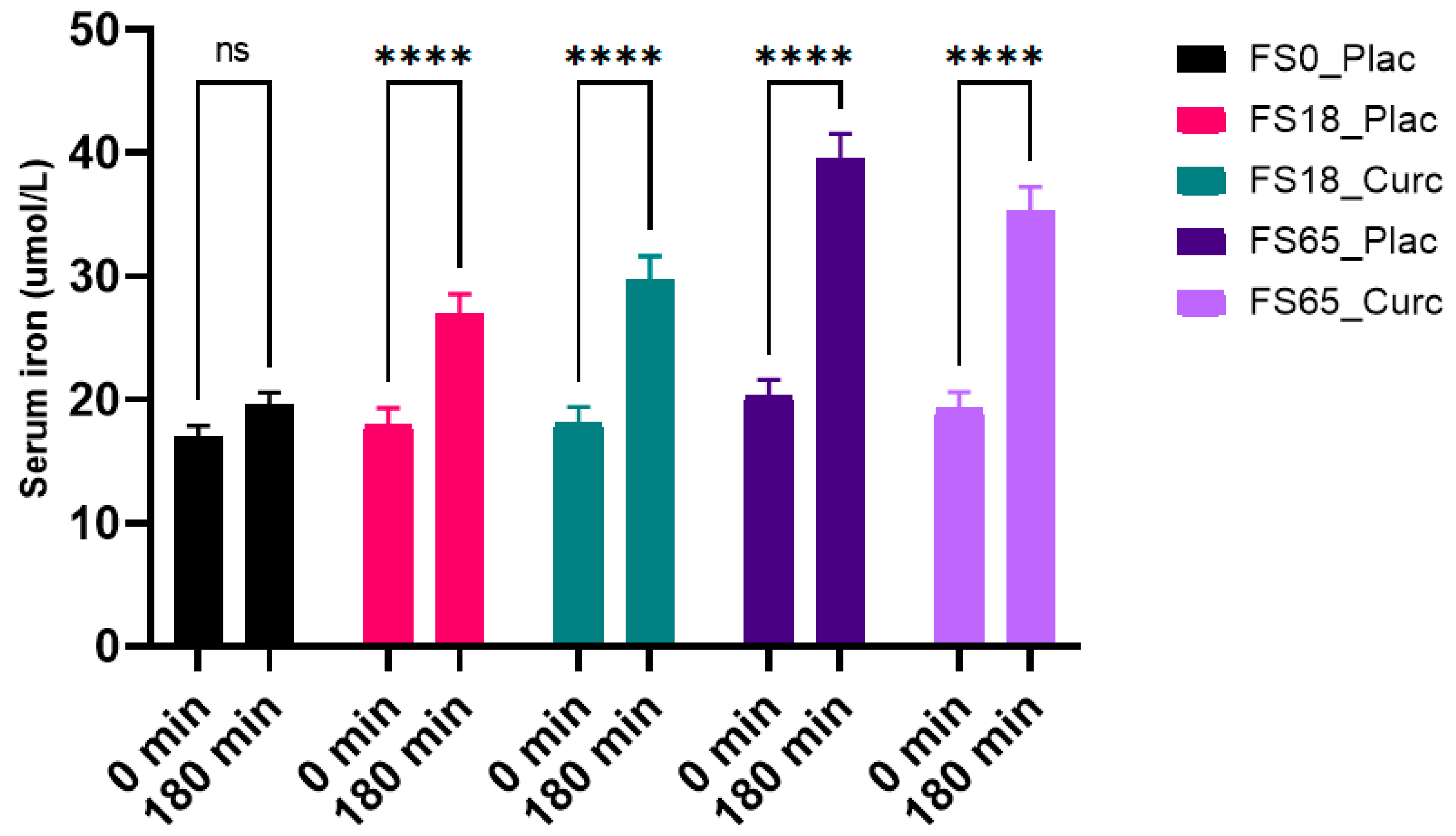
3.3. Effects of Acute Supplementation on Serum Iron Levels
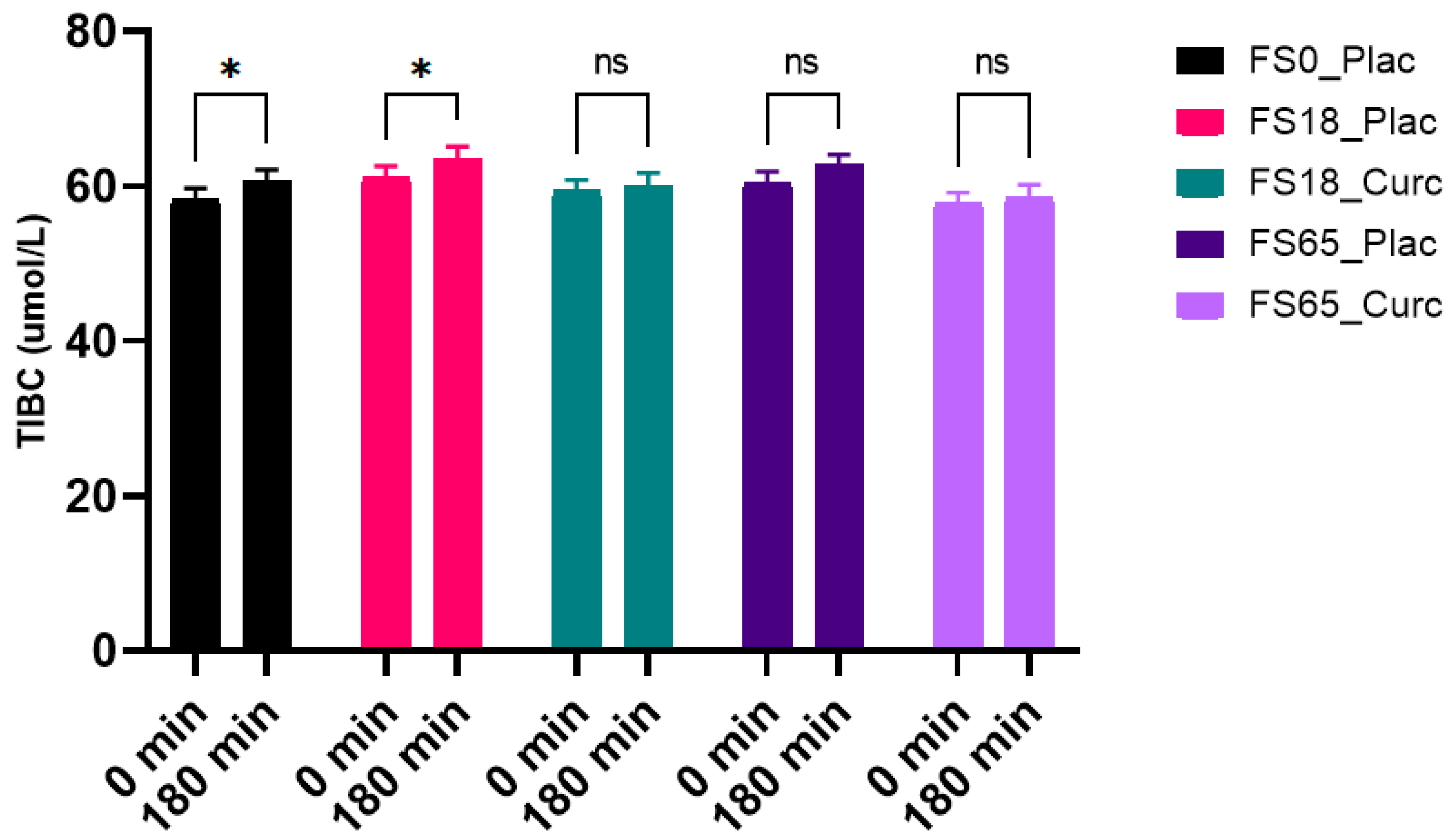
3.4. Effects of Acute Supplementation on Serum TIBC Levels
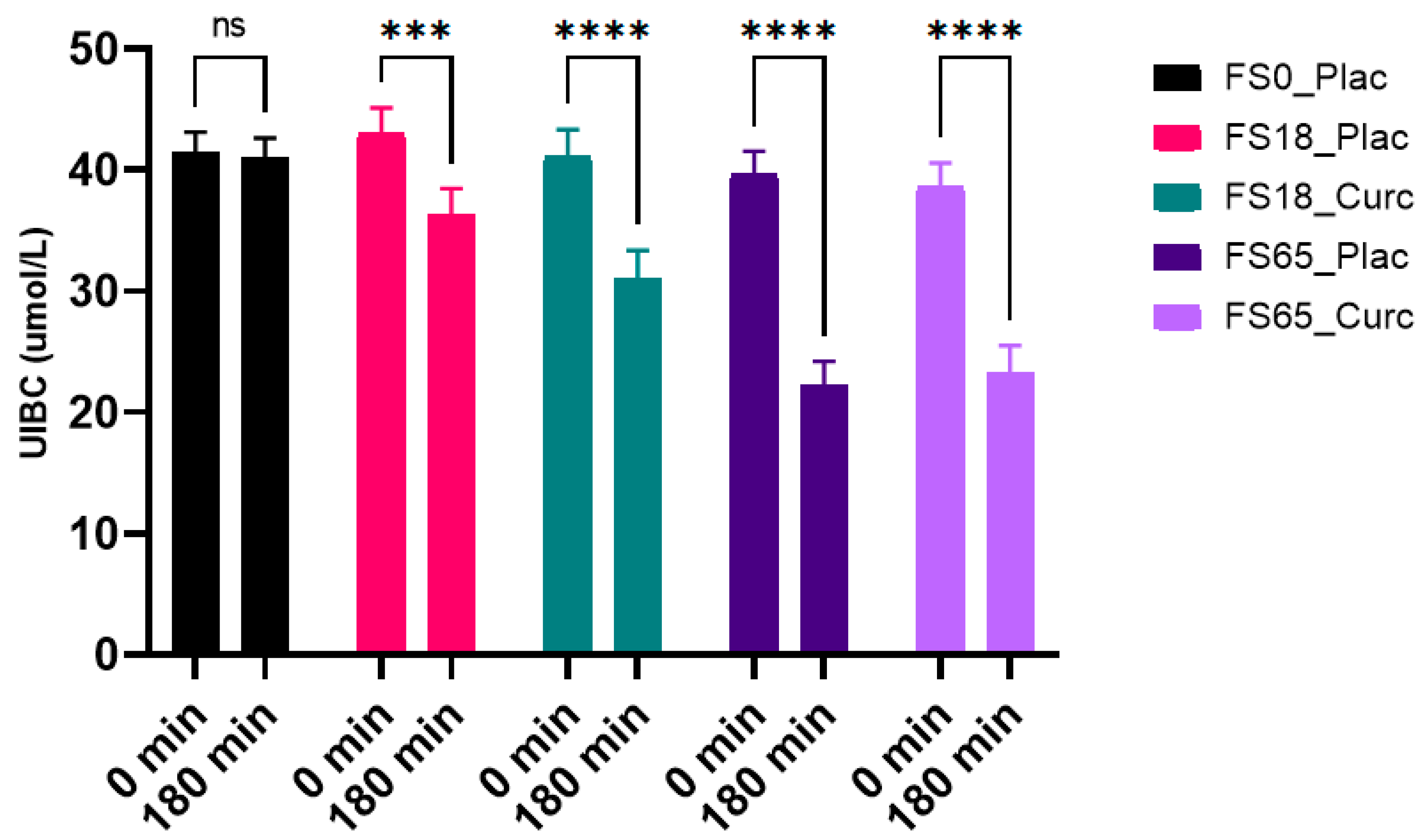
3.5. Effects of Acute Supplementation on Serum UIBC Levels
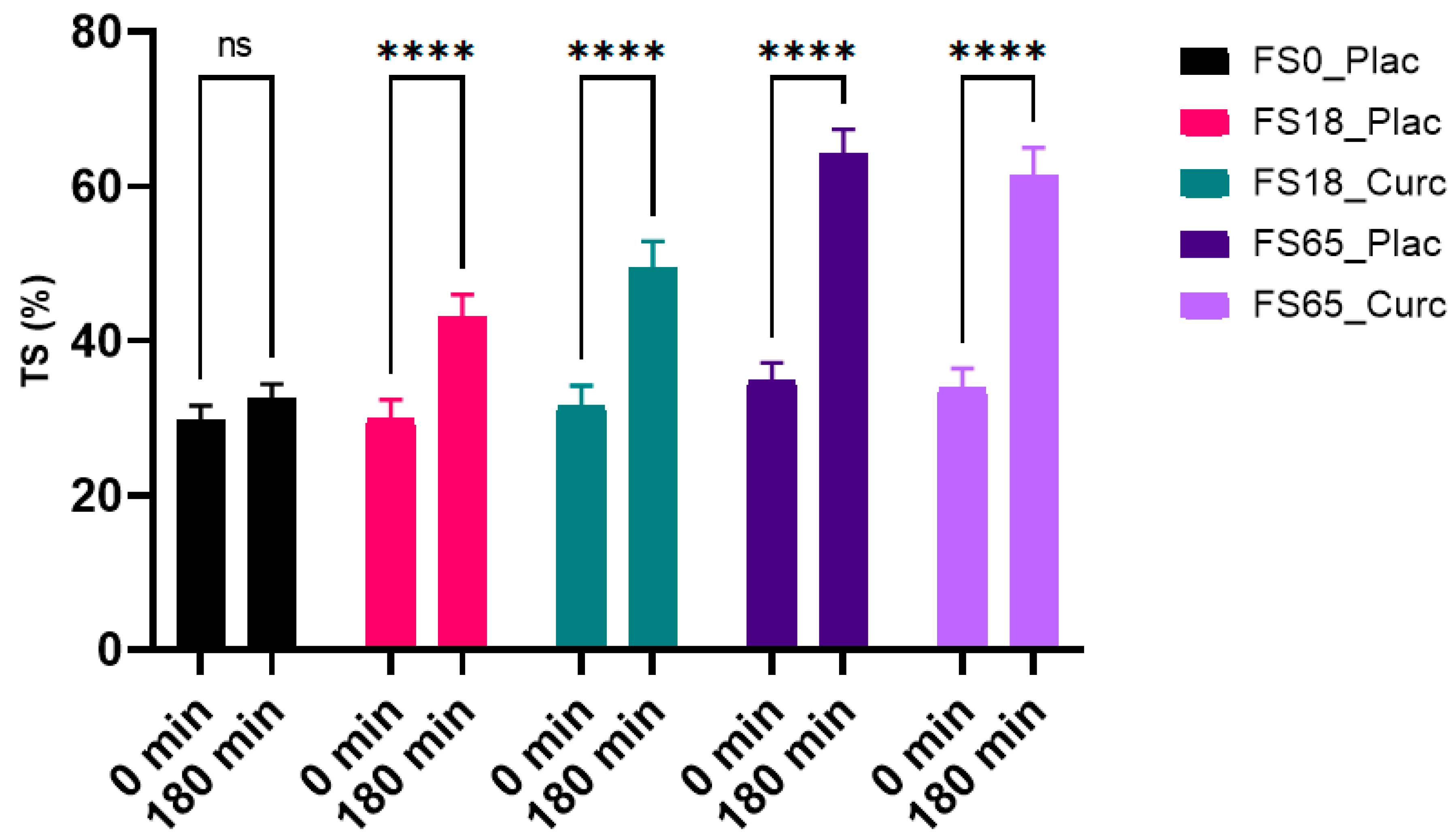
3.6. Effects of Acute Supplementation on Serum Transferrin Saturation (TS) %
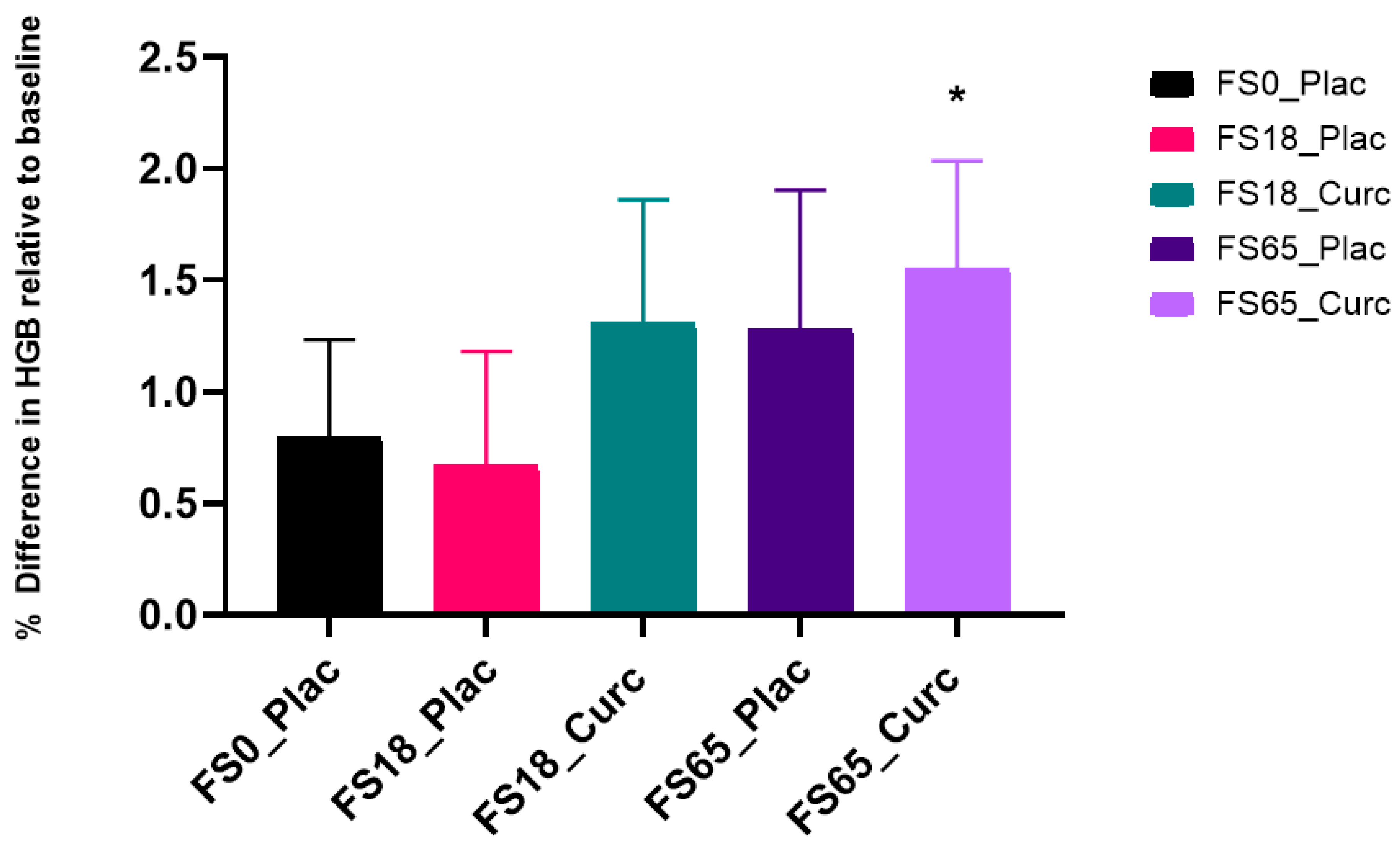
3.7. Effects of Acute Supplementation on Whole Blood HGB Levels
3.8. Effects of Acute Supplementation on Serum TBARS Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aisen, P.; Enns, C.; Wessling-Resnick, M. Chemistry and Biology of Eukaryotic Iron Metabolism. Int. J. Biochem. Cell Biol. 2001, 33, 940–959. [Google Scholar] [CrossRef]
- Lieu, P.T.; Heiskala, M.; Peterson, P.A.; Yang, Y. The Roles of Iron in Health and Disease. Mol. Asp. Med. 2001, 22, 1–87. [Google Scholar] [CrossRef]
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron Deficiency Anaemia. Lancet 2016, 387, 907–916. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Nutritional Anaemias: Tools for Effective Prevention and Control; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Roberts, D.J.; Weatherall, D.J. Introduction: The Complexity and Challenge of Preventing, Treating, and Managing Blood Diseases in the Developing Countries. Hematol. Oncol. Clin. North Am. 2016, 30, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Haas, J.D.; Brownlie IV, T. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownlie IV, T.; Utermohlen, V.; Hinton, P.S.; Giordano, C.; Haas, J.D. Marginal Iron Deficiency without Anemia Impairs Aerobic Adaptation among Previously Untrained Women. Am. J. Clin. Nutr. 2002, 75, 734–742. [Google Scholar] [CrossRef]
- Jáuregui-Lobera, I. Iron Deficiency and Cognitive Functions. Neuropsychiatr. Dis. Treat. 2014, 10, 2087–2095. [Google Scholar] [CrossRef] [Green Version]
- Patterson, A.J.; Brown, W.J.; Powers, J.R.; Roberts, D.C.K. Iron Deficiency, General Health and Fatigue: Results from the Australian Longitudinal Study on Women’s Health. Qual. Life Res. 2000, 9, 491–497. [Google Scholar] [CrossRef]
- Enjuanes, C.; Klip, I.T.; Bruguera, J.; Cladellas, M.; Ponikowski, P.; Banasiak, W.; Van Veldhuisen, D.J.; Van Der Meer, P.; Jankowska, E.A.; Comín-Colet, J. Iron Deficiency and Health-Related Quality of Life in Chronic Heart Failure: Results from a Multicenter European Study. Int. J. Cardiol. 2014, 174, 268–275. [Google Scholar] [CrossRef]
- NICE Anaemia—Iron Deficiency. Available online: https://cks.nice.org.uk/topics/anaemia-iron-deficiency/ (accessed on 12 May 2021).
- Tolkien, Z.; Stecher, L.; Mander, A.P.; Pereira, D.I.A.; Powell, J.J. Ferrous Sulfate Supplementation Causes Significant Gastrointestinal Side-Effects in Adults: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0117383. [Google Scholar] [CrossRef] [Green Version]
- Gastearena, M.A.I.; Gil, A.G.; Azqueta, A.; Coronel, M.P.; Gimeno, M. A Comparative Study on the Gastroduodenal Tolerance of Different Antianaemic Preparations. Hum. Exp. Toxicol. 2003, 22, 137–141. [Google Scholar] [CrossRef] [PubMed]
- De Souza, A.I.; Filho, M.B.; Bresani, C.C.; Ferreira, L.O.C.; Figueiroa, J.N. Adherence and Side Effects of Three Ferrous Sulfate Treatment Regimens on Anemic Pregnant Women in Clinical Trials. Cad. Saude Publica 2009, 25, 1225–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLoughery, T.G. Safety of Oral and Intravenous Iron. Acta Haematol. 2019, 142, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Wessling-Resnick, M. Excess Iron: Considerations Related to Development and Early Growth. Am. J. Clin. Nutr. 2017, 106, 1600S–1605S. [Google Scholar] [CrossRef] [PubMed]
- Assunção, M.; Santos-Marques, M.J.; Carvalho, F.; Andrade, J.P. Green Tea Averts Age-Dependent Decline of Hippocampal Signaling Systems Related to Antioxidant Defenses and Survival. Free Radic. Biol. Med. 2010, 48, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Fahnestock, M.; Marchese, M.; Head, E.; Pop, V.; Michalski, B.; Milgram, W.N.; Cotman, C.W. BDNF Increases with Behavioral Enrichment and an Antioxidant Diet in the Aged Dog. Neurobiol. Aging 2012, 33, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, R.; Deshpande, A.; Saxena, K.; Varma, M.; Sinha, A.R. Ginger Supplementary Therapy for Iron Absorption in Iron Deficiency Anemia. Indian J. Tradit. Knowl. 2012, 11, 78–80. [Google Scholar]
- Ramezani, M.; Hatamipour, M.; Sahebkar, A. Promising Anti-Tumor Properties of Bisdemethoxycurcumin: A Naturally Occurring Curcumin Analogue The Present Review Discusses the Findings on the Anti-Tumor Effects of BDMC, Underlying Mechanisms, and the Relevance of Finding for Translational Studies in Human. Wiley Online Libr. 2017, 233, 880–887. [Google Scholar] [CrossRef]
- Pulla Reddy, A.C.; Lokesh, B.R. Studies on Spice Principles as Antioxidants in the Inhibition of Lipid Peroxidation of Rat Liver Microsomes. Mol. Cell. Biochem. 1992, 111, 117–124. [Google Scholar] [CrossRef]
- Hjorth Tønnesen, H.; Smistad, G.; Ågren, T.; Karlsen, J. Studies on Curcumin and Curcuminoids. XXIII: Effects of Curcumin on Liposomal Lipid Peroxidation. Int. J. Pharm. 1993, 90, 221–228. [Google Scholar] [CrossRef]
- Borsari, M.; Ferrari, E.; Grandi, R.; Saladini, M. Curcuminoids as Potential New Iron-Chelating Agents: Spectroscopic, Polarographic and Potentiometric Study on Their Fe(III) Complexing Ability. Inorg. Chim. Acta 2002, 328, 61–68. [Google Scholar] [CrossRef]
- Bernabé-Pineda, M.; Ramírez-Silva, M.T.; Romero-Romo, M.A.; González-Vergara, E.; Rojas-Hernández, A. Spectrophotometric and Electrochemical Determination of the Formation Constants of the Complexes Curcumin-Fe(III)-Water and Curcumin-Fe(II)-Water. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2004, 60, 1105–1113. [Google Scholar] [CrossRef]
- Salem, M.; Rohani, S.; Gillies, E.R. Curcumin, a Promising Anti-Cancer Therapeutic: A Review of Its Chemical Properties, Bioactivity and Approaches to Cancer Cell Delivery. RSC Adv. 2014, 4, 10815–10829. [Google Scholar] [CrossRef]
- Buhrmann, C.; Mobasheri, A.; Busch, F.; Aldinger, C.; Stahlmann, R.; Montaseri, A.; Shakibaei, M. Curcumin Modulates Nuclear Factor ΚB (Nf-ΚB)-Mediated Inflammation in Human Tenocytes in Vitro: Role of the Phosphatidylinositol 3-Kinase/Akt Pathway. J. Biol. Chem. 2011, 286, 28556–28566. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.; Palanivelu, K. The Effect of Curcumin (Turmeric) on Alzheimer’s Disease: An Overview. Ann. Indian Acad. Neurol. 2008, 11, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Sarraf, P.; Parohan, M.; Javanbakht, M.H.; Ranji-Burachaloo, S.; Djalali, M. Short-Term Curcumin Supplementation Enhances Serum Brain-Derived Neurotrophic Factor in Adult Men and Women: A Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials. Nutr. Res. 2019, 69, 1–8. [Google Scholar] [CrossRef]
- Tiekou Lorinczova, H.; Fitzsimons, O.; Mursaleen, L.; Renshaw, D.; Begum, G.; Zariwala, M.G. Co-Administration of Iron and a Bioavailable Curcumin Supplement Increases Serum BDNF Levels in Healthy Adults. Antioxidants 2020, 9, 645. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Huebbe, P.; Frank, J.; Rimbach, G.; Pallauf, K. Curcumin May Impair Iron Status When Fed to Mice for Six Months. Redox Biol. 2014, 2, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Cory, H.; Passarelli, S.; Szeto, J.; Tamez, M.; Mattei, J. The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Front. Nutr. 2018, 5, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samba-Mondonga, M.; Constante, M.; Fragoso, G.; Calvé, A.; Santos, M.M. Curcumin Induces Mild Anemia in a DSS-Induced Colitis Mouse Model Maintained on an Iron-Sufficient Diet. PLoS ONE 2019, 14, e0208677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuntipopipat, S.; Zeder, C.; Siriprapa, P.; Charoenkiatkul, S. Inhibitory Effects of Spices and Herbs on Iron Availability. Int. J. Food Sci. Nutr. 2009, 60, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Bich, V.T.; Thuy, N.T.; Binh, N.T.; Huong, N.T.M.; Yen, P.N.D.; Luong, T.T. Structural and Spectral Properties of Curcumin and Metal- Curcumin Complex Derived from Turmeric (Curcuma Longa). In Physics and Engineering of New Materials; Springer Proceedings in Physics; Springer Science and Business Media, LLC: Berlin, Germany, 2009; Volume 127, pp. 271–278. [Google Scholar]
- Ferrari, E.; Benassi, R.; Sacchi, S.; Pignedoli, F.; Asti, M.; Saladini, M. Curcumin Derivatives as Metal-Chelating Agents with Potential Multifunctional Activity for Pharmaceutical Applications. J. Inorg. Biochem. 2014, 139, 38–48. [Google Scholar] [CrossRef]
- Srichairatanakool, S.; Thephinlap, C.; Phisalaphong, C.; Porter, J.; Fucharoen, S. Curcumin Contributes to In Vitro Removal of Non-Transferrin Bound Iron by Deferiprone and Desferrioxamine in Thalassemic Plasma. Med. Chem. 2007, 3, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Study Randomizer App.Studyrandomizer.Com. Available online: https://app.studyrandomizer.com (accessed on 12 May 2021).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Dooley, J.; Worwood, M. Guidelines on Diagnosis and Therapy: Genetic Haemochromatosis; British Committee for Standards in Haematology: London, UK, 2000; pp. 1–33. [Google Scholar]
- Fitzsimons, E.J.; Cullis, J.O.; Thomas, D.W.; Tsochatzis, E.; Griffiths, W.J.H. Diagnosis and Therapy of Genetic Haemochromatosis (Review and 2017 Update). Br. J. Haematol. 2018, 181, 293–303. [Google Scholar] [CrossRef]
- Blood Pressure UK. Available online: http://www.bloodpressureuk.org/your-blood-pressure/understanding-your-blood-pressure/what-do-the-numbers-mean/ (accessed on 12 May 2021).
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). J. Hypertens 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goddard, A.F.; James, M.W.; McIntyre, A.S.; Scott, B.B. Guidelines for the Management of Iron Deficiency Anaemia. Gut 2011, 60, 1309–1316. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration (FDA) Center for Food Safety and Applied Nutrition. Guidance for Industry: A Food Labeling Guide; Food and Drug Administration: College Park, MD, USA, 2013. [Google Scholar]
- Briskey, D.; Sax, A.; Mallard, A.R.; Rao, A. Increased Bioavailability of Curcumin Using a Novel Dispersion Technology System (LipiSperse®). Eur. J. Nutr. 2019, 58, 2087–2097. [Google Scholar] [CrossRef]
- Coudène, P.; Marson, B.; Badiou, S.; Flavier, S.; Anelli, S.; Cristol, J.P.; Dupuy, A.M. Evaluation of the ABX Pentra 400: A Newly Available Clinical Chemistry Analyser. Clin. Chem. Lab. Med. 2005, 43, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Simó, J.M.; Joven, J.; Clivillé, X.; Sans, T. Automated Latex Agglutination Immunoassay of Serum Ferritin with a Centrifugal Analyzer. Clin. Chem. 1994, 40, 625–629. [Google Scholar] [CrossRef]
- Elsayed, M.E.; Sharif, M.U.; Stack, A.G. Transferrin Saturation: A Body Iron Biomarker. In Advances in Clinical Chemistry; Academic Press Inc.: Cambridge, MA, USA, 2016; Volume 75, pp. 71–97. [Google Scholar]
- Van Dievoet, M.A.; Louagie, H.; Ghys, T. Performance Evaluation of the Sysmex® XP-300 in an Oncology Setting: Evaluation and Comparison of Hematological Parameters with the Sysmex® XN-3000. Int. J. Lab. Hematol. 2016, 38, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Glass, G.V.; Peckham, P.D.; Sanders, J.R. Consequences of Failure to Meet Assumptions Underlying the Fixed Effects Analyses of Variance and Covariance. Rev. Educ. Res. 1972, 42, 237–288. [Google Scholar] [CrossRef]
- Harwell, M.R.; Rubinstein, E.N.; Hayes, W.S.; Olds, C.C. Summarizing Monte Carlo Results in Methodological Research: The One- and Two-Factor Fixed Effects ANOVA Cases. J. Educ. Stat. 1992, 17, 315–339. [Google Scholar] [CrossRef]
- Lix, L.M.; Keselman, J.C.; Keselman, H.J. Consequences of Assumption Violations Revisited: A Quantitative Review of Alternatives to the One-Way Analysis of Variance F Test. Rev. Educ. Res. 1996, 66, 579–619. [Google Scholar] [CrossRef]
- WHO. Physical Status: The Use and Interpretation of Anthropometry, Report of a World Health Organization (WHO) Expert Committe. In World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 1995; Volume 854, p. 452. [Google Scholar]
- WHO. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. In World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 2000; Volume 894. [Google Scholar]
- Hewlings, S.; Kalman, D. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef]
- Prasad, S.; Gupta, S.C.; Tyagi, A.K.; Aggarwal, B.B. Curcumin, a Component of Golden Spice: From Bedside to Bench and Back. Biotechnol. Adv. 2014, 32, 1053–1064. [Google Scholar] [CrossRef]
- Zhongfa, L.; Chiu, M.; Wang, J.; Chen, W.; Yen, W.; Fan-Havard, P.; Yee, L.D.; Chan, K.K.; Zhongfa, L.; Chiu, Á.M.; et al. Enhancement of Curcumin Oral Absorption and Pharmacokinetics of Curcuminoids and Curcumin Metabolites in Mice. Cancer Chemother Pharm. 2012, 69, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Zupančič, Š.; Kocbek, P.; Zariwala, M.G.; Renshaw, D.; Gul, M.O.; Elsaid, Z.; Taylor, K.M.G.; Somavarapu, S. Design and Development of Novel Mitochondrial Targeted Nanocarriers, Dqasomes for Curcumin Inhalation. Mol. Pharm. 2014, 11, 2334–2345. [Google Scholar] [CrossRef]
- Mursaleen, L.; Somavarapu, S.; Zariwala, M.G. Deferoxamine and Curcumin Loaded Nanocarriers Protect Against Rotenone-Induced Neurotoxicity. J. Parkinson’s Dis. 2020, 10, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Wilkinson IV, J.; Di, X.; Wang, W.; Hatcher, H.; Kock, N.D.; D’Agostino, R.; Knovich, M.A.; Torti, F.M.; Torti, S.V. Curcumin, a Cancer Chemopreventive and Chemotherapeutic Agent, Is a Biologically Active Iron Chelator. Blood 2009, 113, 462–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badria, F.A.; Ibrahim, A.S.; Badria, A.F.; Elmarakby, A.A. Curcumin Attenuates Iron Accumulation and Oxidative Stress in the Liver and Spleen of Chronic Iron-Overloaded Rats. PLoS ONE 2015, 10, e0134156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ak, T.; Gülçin, I. Antioxidant and Radical Scavenging Properties of Curcumin. Chem. Biol. Interact. 2008, 174, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Höglund, S. Iron Absorption in Apparently Healthy Men and Women: III. Studies in Iron Absorption. Acta Med. Scand. 1969, 186, 487–491. [Google Scholar] [CrossRef]
- Ekenved, G.; Norrby, A.; Sölvell, L. Serum Iron Increase as a Measure of Iron Absorption—Studies on the Correlation with Total Absorption. Scand. J. Haematol. 1976, 17, 31–49. [Google Scholar] [CrossRef]
- Wick, M.; Pinggera, W.; Lehmann, P. Iron Metabolism: Diagnosis and Therapy of Anemias; Springer Science & Business Media: Wien, Austria, 1996; ISBN 9783709136881. [Google Scholar]
- Alleyne, M.; Horne, M.K.; Miller, J.L. Individualized Treatment for Iron-Deficiency Anemia in Adults. Am. J. Med. 2008, 121, 943–948. [Google Scholar] [CrossRef] [Green Version]
- Pstras, L.; Debowska, M.; Wojcik-Zaluska, A.; Zaluska, W.; Waniewski, J. Hemodialysis-Induced Changes in Hematocrit, Hemoglobin and Total Protein: Implications for Relative Blood Volume Monitoring. PLoS ONE 2019, 14, e0220764. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.J.; Frazer, D.M. Current Understanding of Iron Homeostasis. Am. J. Clin. Nutr. 2017, 106, 1559S–1566S. [Google Scholar] [CrossRef] [Green Version]
- Schoorl, M.; Schoorl, M.; van der Gaag, D.; Bartels, P.C.M. Effects of Iron Supplementation on Red Blood Cell Hemoglobin Content in Pregnancy. Hematol. Rep. 2012, 4, 91–94. [Google Scholar] [CrossRef]
- Porter, R.; FitzSimons, D.W. Iron Metabolism; Elsevier/Experta Medica: Amsterdam, The Netherlands, 1977; Volume 51, ISBN 9021940574. [Google Scholar]
- Santiago, P. Ferrous versus Ferric Oral Iron Formulations for the Treatment of Iron Deficiency: A Clinical Overview. Sci. World J. 2012, 2012, 846824. [Google Scholar] [CrossRef] [PubMed]
- Stengle, J.M.; Schade, A.L. Diurnal-Nocturnal Variations of Certain Blood Constituents in Normal Human Subjects: Plasma Iron, Siderophilin, Bilirubin, Copper, Total Serum Protein and Albumin, Haemoglobin and Haematocrit. Br. J. Haematol. 1957, 3, 117–124. [Google Scholar] [CrossRef]
- Sinniah, R.; Doggart, J.R.; Neill, D.W. Diurnal Variations of the Serum Iron in Normal Subjects and in Patients with Haemochromatosis. Br. J. Haematol. 1969, 17, 351–358. [Google Scholar] [CrossRef]
- Casale, G.; de Nicola, P. Circadian Rhythms in the Aged: A Review. Arch. Gerontol. Geriatr. 1984, 3, 267–284. [Google Scholar] [CrossRef]
- Andersen, S.L.; Gyrup, C.; Handberg, A.; Nielsen, G.L. Oral Iron Absorption Test Should Not Be Performed with Iron Drops Containing Ferric Iron. Dan. Med J. 2015, 62, A5116. [Google Scholar]
- Ginanjar, E.; Indrawati, L.; Setianingsih, I.; Atmakusumah, D.; Harahap, A.; Timan, I.S.; Marx, J.J.M. Iron Absorption in Iron-Deficient Women, Who Received 65 Mg Fe with an Indonesian Breakfast, Is Much Better from NaFe(III)EDTA than from Fe(II)SO4, with an Acceptable Increase of Plasma NTBI. A Randomized Clinical Trial. Pharmaceuticals 2018, 11, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | FS0_Plac | FS18_Plac | FS18_Curc | FS65_Plac | FS65_Curc | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| Age (years) | 25.87 ± 1.18 | 26.73 ± 1.31 | 26.11 ± 1.27 | 25.08 ± 1.47 | 25.60 ± 1.13 | 23.53 ± 1.24 | 26.92 ± 1.25 | 27.06 ± 1.14 | 27.12 ± 1.35 | 26.36 ± 1.08 | 26.32 ± 0.55 | 25.81 ± 0.56 |
| (n = 15) | (n = 16) | (n = 18) | (n = 13) | (n = 15) | (n = 16) | (n = 13) | (n = 17) | (n = 17) | (n = 14) | (n = 78) | (n = 76) | |
| Height (m) | 1.77 ± 0.02 | 1.67 ± 0.02 | 1.76 ± 0.01 | 1.64 ± 0.01 | 1.77 ± 0.02 | 1.59 ± 0.02 | 1.78 ± 0.01 | 1.63 ± 0.02 | 1.78 ± 0.2 | 1.65 ± 0.02 | 1.77 ± 0.01 | 1.64 ± 0.01 |
| (n = 15) | (n = 15) | (n = 18) | (n = 12) | (n = 15) | (n = 15) | (n =13) | (n = 17) | (n = 17) | (n = 14) | (n = 78) | (n = 73) | |
| Weight (kg) | 75.22 ± 3.15 | 66.36 ± 3.25 | 80.70 ± 3.70 | 60.08 ± 3.07 | 74.58 ± 2.78 | 57.76 ± 2.64 | 77.13 ± 2.27 | 60.27 ± 2.89 | 75.24 ± 2.26 | 58.54 ± 1.91 | 76.69 ± 1.32 | 60.64 ± 1.28 |
| (n = 15) | (n = 15) | (n = 18) | (n = 12) | (n =15) | (n = 15) | (n = 13) | (n =17) | (n = 17) | (n = 14) | (n = 78) | (n = 73) | |
| BMI (kg/m2) | 24.06 ± 0.83 | 23.72 ± 0.85 | 25.94 ± 1.06 | 22.38 ± 1.21 | 23.71 ± 0.79 | 22.93 ± 1.03 | 24.32 ± 0.56 | 22.46 ± 0.82 | 23.95 ± 0.77 | 21.48 ± 0.65 | 24.44 ± 0.38 | 22.61 ± 0.41 |
| (n = 15) | (n = 15) | (n = 18) | (n = 12) | (n = 15) | (n = 15) | (n = 13) | (n = 17) | (n =17) | (n =14) | (n = 78) | (n = 73) | |
| Body Fat (%) | 18.37 ± 1.68 | 32.16 ± 1.57 | 21.97 ± 2.02 | 29.45 ± 2.44 | 18.35 ± 1.86 | 30.29 ± 2.07 | 19.13 ± 1.51 | 27.95 ± 1.52 | 19.44 ± 1.85 | 28.18 ± 1.25 | 19.56 ± 0.82 | 29.59 ± 0.79 |
| (n = 15) | (n = 15) | (n = 18) | (n = 12) | (n = 15) | (n =15) | (n = 13) | (n = 17) | (n = 17) | (n = 14) | (n = 78) | (n = 73) | |
| Groups | MD ± SED | Sig. * | p−Value | ||
|---|---|---|---|---|---|
| FS0_Plac | vs. | FS18_Plac | −7.18 ± 2.18 | ** | 0.0096 |
| FS0_Plac | vs. | FS18_Curc | −10.02 ± 2.16 | **** | <0.0001 |
| FS0_Plac | vs. | FS65_Plac | −19.88 ± 2.17 | **** | < 0.0001 |
| FS0_Plac | vs. | FS65_Curc | −15.63 ± 2.16 | **** | <0.0001 |
| FS18_Plac | vs. | FS18_Curc | −2.84 ± 2.19 | NS | 0.6917 |
| FS18_Plac | vs. | FS65_Plac | −12.71 ± 2.19 | **** | <0.0001 |
| FS18_Plac | vs. | FS65_Curc | −8.45 ± 2.19 | ** | 0.0013 |
| FS18_Curc | vs. | FS65_Plac | −9.86 ± 2.18 | **** | <0.0001 |
| FS18_Curc | vs. | FS65_Curc | −5.61 ± 2.18 | NS | 0.0771 |
| FS65_Plac | vs. | FS65_Curc | 4.25 ± 2.18 | NS | 0.2935 |
| Groups | MD ± SED | Sig. * | p-Value | ||
|---|---|---|---|---|---|
| FS0_Plac | vs. | FS18_Plac | 4.57 ± 2.80 | NS | 0.4782 |
| FS0_Plac | vs. | FS18_Curc | 9.56 ± 2.78 | ** | 0.0062 |
| FS0_Plac | vs. | FS65_Plac | 19.43 ± 2.83 | **** | <0.0001 |
| FS0_Plac | vs. | FS65_Curc | 18.10 ± 2.81 | **** | <0.0001 |
| FS18_Plac | vs. | FS18_Curc | 4.99 ± 2.83 | NS | 0.3944 |
| FS18_Plac | vs. | FS65_Plac | 7.00 ± 2.86 | **** | <0.0001 |
| FS18_Plac | vs. | FS65_Curc | 13.53 ± 2.85 | **** | <0.0001 |
| FS18_Curc | vs. | FS65_Plac | 9.87 ± 2.85 | ** | 0.0055 |
| FS18_Curc | vs. | FS65_Curc | 8.54 ± 2.84 | * | 0.0235 |
| FS65_Plac | vs. | FS65_Curc | −1.33 ± 2.87 | NS | 0.9906 |
| Groups | MD ± SED | Sig. * | p−Value | ||
|---|---|---|---|---|---|
| FS0_Plac | vs. | FS18_Plac | −10.06 ± 3.78 | NS | 0.0627 |
| FS0_Plac | vs. | FS18_Curc | −16.30 ± 3.76 | *** | 0.0002 |
| FS0_Plac | vs. | FS65_Plac | −32.20 ± 3.82 | **** | <0.0001 |
| FS0_Plac | vs. | FS65_Curc | −29.21± 3.80 | **** | <0.0001 |
| FS18_Plac | vs. | FS18_Curc | −6.24 ± 3.82 | NS | 0.4772 |
| FS18_Plac | vs. | FS65_Plac | −22.14 ± 3.88 | **** | <0.0001 |
| FS18_Plac | vs. | FS65_Curc | −19.14 ± 3.85 | **** | <0.0001 |
| FS18_Curc | vs. | FS65_Plac | −15.90 ± 3.86 | *** | 0.0005 |
| FS18_Curc | vs. | FS65_Curc | −12.90 ± 3.83 | ** | 0.0077 |
| FS65_Plac | vs. | FS65_Curc | 2.99 ± 3.89 | NS | 0.9388 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorinczova, H.T.; Begum, G.; Renshaw, D.; Zariwala, M.G. Acute Administration of Bioavailable Curcumin Alongside Ferrous Sulphate Supplements Does Not Impair Iron Absorption in Healthy Adults in a Randomised Trial. Nutrients 2021, 13, 2300. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072300
Lorinczova HT, Begum G, Renshaw D, Zariwala MG. Acute Administration of Bioavailable Curcumin Alongside Ferrous Sulphate Supplements Does Not Impair Iron Absorption in Healthy Adults in a Randomised Trial. Nutrients. 2021; 13(7):2300. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072300
Chicago/Turabian StyleLorinczova, Helena Tiekou, Gulshanara Begum, Derek Renshaw, and Mohammed Gulrez Zariwala. 2021. "Acute Administration of Bioavailable Curcumin Alongside Ferrous Sulphate Supplements Does Not Impair Iron Absorption in Healthy Adults in a Randomised Trial" Nutrients 13, no. 7: 2300. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072300