
Pathogenesis of Musculoskeletal Deficits in Children and Adults with Inflammatory Bowel Disease

 and
and
Abstract
:1. Introduction
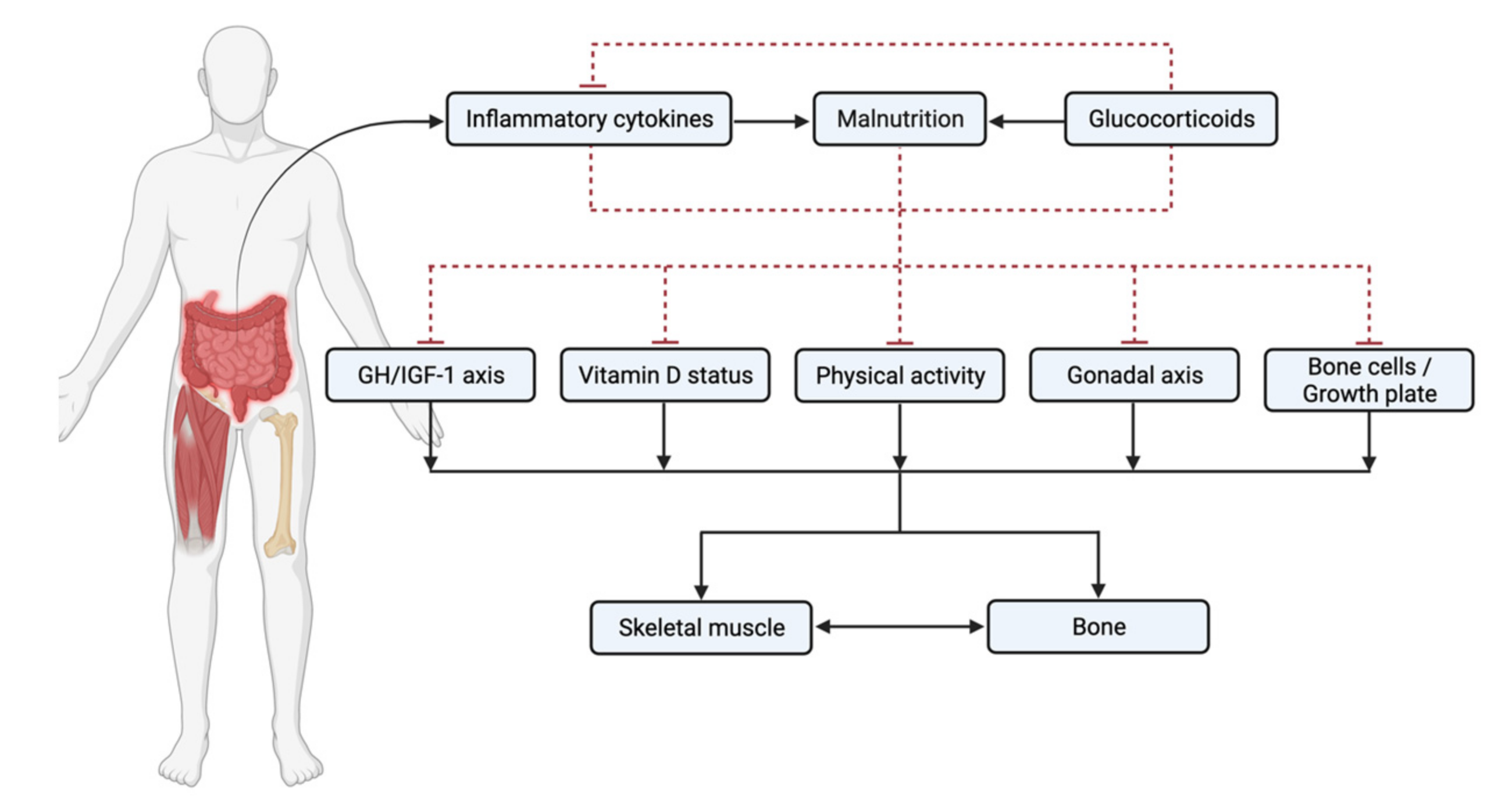
2. Pathogenesis of Musculoskeletal Deficits in IBD
2.1. Inflammation/Cytokines
2.2. Nutrition
2.3. Glucocorticoids
2.4. Vitamin D
2.5. GH/IGF-1
2.6. Delayed Puberty and Sex Steroid Deficiency
2.7. Low Muscle Mass
2.8. Physical Inactivity
3. Clinical Studies of Bone Health in IBD
4. Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dempster, D.W.; Marcus, R.; Bouxsein, M.L. Chapter 1—The nature of osteoporosis. In Marcus and Feldman’s Osteoporosis, 5th ed.; Dempster, D.W., Cauley, J.A., Bouxsein, M.L., Cosman, F., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 3–13. [Google Scholar]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Mirza, F.; Canalis, E. Management of endocrine disease: Secondary osteoporosis: Pathophysiology and management. Eur. J. Endocrinol. 2015, 173, R131–R151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, L.M.; Weber, D.R.; Munns, C.F.; Högler, W.; Zemel, B.S. A Contemporary View of the Definition and Diagnosis of Osteoporosis in Children and Adolescents. J. Clin. Endocrinol. Metab. 2020, 105, e2088–e2097. [Google Scholar] [CrossRef] [PubMed]
- Steell, L.; Johnston, B.A.; Dewantoro, D.; Foster, J.E.; Gaya, D.R.; Macdonald, J.; McMillan, M.; Russell, R.K.; Seenan, J.P.; Ahmed, S.F.; et al. Muscle deficits with normal bone microarchitecture and geometry in young adults with well-controlled childhood-onset Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.M.; Ma, J.; Rauch, F.; Benchimol, E.I.; Hay, J.; Leonard, M.B.; Matzinger, M.A.; Shenouda, N.; Lentle, B.; Cosgrove, H.; et al. Musculoskeletal health in newly diagnosed children with Crohn’s disease. Osteoporos. Int. 2017, 28, 3169–3177. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.Q.; Varma, P.; Strauss, B.J.G.; Rajadurai, A.S.; Moore, G.T. Low muscle mass at initiation of anti-TNF therapy for inflammatory bowel disease is associated with early treatment failure: A retrospective analysis. Eur. J. Clin. Nutr. 2017, 71, 773–777. [Google Scholar] [CrossRef]
- Ding, N.S.; Malietzis, G.; Lung, P.F.C.; Penez, L.; Yip, W.M.; Gabe, S.; Jenkins, J.T.; Hart, A. The body composition profile is associated with response to anti-TNF therapy in Crohn’s disease and may offer an alternative dosing paradigm. Aliment. Pharmacol. Ther. 2017, 46, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, S.; Kavanagh, R.G.; Carey, B.W.; Maher, M.M.; O’Connor, O.J.; Andrews, E.J. The impact of sarcopenia and myosteatosis on postoperative outcomes in patients with inflammatory bowel disease. Eur. Radiol. Exp. 2018, 2, 37. [Google Scholar] [CrossRef]
- Grillot, J.; D’Engremont, C.; Parmentier, A.L.; Lakkis, Z.; Piton, G.; Cazaux, D.; Gay, C.; De Billy, M.; Koch, S.; Borot, S.; et al. Sarcopenia and visceral obesity assessed by computed tomography are associated with adverse outcomes in patients with Crohn’s disease. Clin. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kirk, B.; Feehan, J.; Lombardi, G.; Duque, G. Muscle, Bone, and Fat Crosstalk: The Biological Role of Myokines, Osteokines, and Adipokines. Curr. Osteoporos. Rep. 2020. [Google Scholar] [CrossRef]
- Bechtold, S.; Alberer, M.; Arenz, T.; Putzker, S.; Filipiak-Pittroff, B.; Schwarz, H.P.; Koletzko, S. Reduced Muscle Mass and Bone Size in Pediatric Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2010, 16, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, F.A.; Wyzga, N.; Hyams, J.S.; Davis, P.M.; Lerer, T.; Vance, K.; Hawker, G.; Griffiths, A.M. Natural history of bone metabolism and bone mineral density in children with inflammatory bowel disease. Inflamm. Bowel Dis. 2007, 13, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.M.; Rauch, F.; Matzinger, M.A.; Benchimol, E.I.; Boland, M.; Mack, D.R. Iliac bone histomorphometry in children with newly diagnosed inflammatory bowel disease. Osteoporos. Int. 2010, 21, 331–337. [Google Scholar] [CrossRef]
- Thearle, M.; Horlick, M.; Bilezikian, J.P.; Levy, J.; Gertner, J.M.; Levine, L.S.; Harbison, M.; Berdon, W.; Oberfield, S.E. Osteoporosis: An Unusual Presentation of Childhood Crohn’s Disease1. J. Clin. Endocrinol. Metab. 2000, 85, 2122–2126. [Google Scholar] [CrossRef] [Green Version]
- Kwan Tat, S.; Padrines, M.; Theoleyre, S.; Heymann, D.; Fortun, Y. IL-6, RANKL, TNF-alpha/IL-1: Interrelations in bone resorption pathophysiology. Cytokine Growth Factor Rev. 2004, 15, 49–60. [Google Scholar]
- Krela-Kazmierczak, I.; Szymczak-Tomczak, A.; Lykowska-Szuber, L.; Wysocka, E.; Michalak, M.; Stawczyk-Eder, K.; Waszak, K.; Linke, K.; Eder, P. Interleukin 6, osteoprotegerin, sRANKL and bone metabolism in inflammatory bowel diseases. Adv. Clin. Exp. Med. 2018, 27, 449–453. [Google Scholar] [CrossRef]
- Oostlander, A.E.; Bravenboer, N.; Lems, W.F.; Klein-Nulend, J.; Schulten, E.A.; van Bodegraven, A.A.; Lips, P. Effect of proinflammatory cytokines and serum of Crohn’s disease patients on primary human osteoblast proliferation. Calcified Tissue Int. 2008, 82, S113. [Google Scholar]
- Marahleh, A.; Kitaura, H.; Ohori, F.; Kishikawa, A.; Ogawa, S.; Shen, W.-R.; Qi, J.; Noguchi, T.; Nara, Y.; Mizoguchi, I. TNF-α directly enhances osteocyte RANKL expression and promotes osteoclast formation. Front. Immunol. 2019, 10, 2925. [Google Scholar] [CrossRef] [Green Version]
- Luo, G.; Li, F.; Li, X.; Wang, Z.G.; Zhang, B. TNF-α and RANKL promote osteoclastogenesis by upregulating RANK via the NF-κB pathway. Mol. Med. Rep. 2018, 17, 6605–6611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschen, A.R.; Kaser, A.; Enrich, B.; Ludwiczek, O.; Gabriel, M.; Obrist, P.; Wolf, A.M.; Tilg, H. The RANKL/OPG system is activated in inflammatory bowel disease and relates to the state of bone loss. Gut 2005, 54, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Varghese, S.; Wyzga, N.; Griffiths, A.M.; Sylvester, F.A. Effects of serum from children with newly diagnosed Crohn disease on primary cultures of rat osteoblasts. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Turk, N.; Cukovic-Cavka, S.; Korsic, M.; Turk, Z.; Vucelic, B. Proinflammatory cytokines and receptor activator of nuclear factor kappa B-ligand/osteoprotegerin associated with bone deterioration in patients with Crohn’s disease. Eur. J. Gastroen. Hepat. 2009, 21, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvester, F.A.; Wyzga, N.; Hyams, J.S.; Gronowicz, G.A. Effect of Crohn’s disease on bone metabolism in vitro: A role for interleukin-6. J. Bone Miner. Res. 2002, 17, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Holgersen, K.; Dobie, R.; Farquharson, C.; van’t Hof, R.; Ahmed, S.F.; Hansen, A.K.; Holm, T.L. Piroxicam treatment augments bone abnormalities in interleukin-10 knockout mice. Inflamm. Bowel Dis. 2015, 21, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Bravenboer, N.; Oostlander, A.E.; van Bodegraven, A.A. Bone loss in patients with inflammatory bowel disease: Cause, detection and treatment. Curr. Opin. Gastroen. 2021, 37, 128–134. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef] [Green Version]
- Neurath, M.F. Cytokines in inflammatory bowel disease. Nat. Rev. Immunol. 2014, 14, 329–342. [Google Scholar] [CrossRef]
- Thoma, A.; Lightfoot, A.P. NF-kB and Inflammatory Cytokine Signalling: Role in Skeletal Muscle Atrophy. Adv. Exp. Med. Biol. 2018, 1088, 267–279. [Google Scholar] [CrossRef]
- Szalay, K.; Rázga, Z.; Duda, E. TNF inhibits myogenesis and downregulates the expression of myogenic regulatory factors myoD and myogenin. Eur. J. Cell Biol. 1997, 74, 391–398. [Google Scholar]
- Palacios, D.; Mozzetta, C.; Consalvi, S.; Caretti, G.; Saccone, V.; Proserpio, V.; Marquez, V.E.; Valente, S.; Mai, A.; Forcales, S.V.; et al. TNF/p38alpha/polycomb signaling to Pax7 locus in satellite cells links inflammation to the epigenetic control of muscle regeneration. Cell Stem Cell 2010, 7, 455–469. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.E.; Jin, B.; Li, Y.P. TNF-alpha regulates myogenesis and muscle regeneration by activating p38 MAPK. Am. J. Physiol. Cell Physiol. 2007, 292, C1660–C1671. [Google Scholar] [CrossRef] [PubMed]
- Vasseur, F.; Gower-Rousseau, C.; Vernier-Massouille, G.; Dupas, J.L.; Merle, V.; Merlin, B.; Lerebours, E.; Savoye, G.; Salomez, J.L.; Cortot, A.; et al. Nutritional status and growth in pediatric Crohn’s disease: A population-based study. Am. J. Gastroenterol. 2010, 105, 1893–1900. [Google Scholar] [CrossRef]
- Sawczenko, A.; Sandhu, B.K. Presenting features of inflammatory bowel disease in Great Britain and Ireland. Arch. Dis. Child. 2003, 88, 995–1000. [Google Scholar] [CrossRef] [Green Version]
- Shamir, R. Nutritional Aspects in Inflammatory Bowel Disease. J. Pediatr. Gastr. Nutr. 2009, 48, S86–S88. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Munsell, M.; Harris, M.L. Nationwide prevalence and prognostic significance of clinically diagnosable protein-calorie malnutrition in hospitalized inflammatory bowel disease patients. Inflamm. Bowel Dis. 2008, 14, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Wong, S.C.; Bishop, J.; Hassan, K.; McGrogan, P.; Ahmed, S.F.; Russell, R.K. Improvement in Growth of Children With Crohn Disease Following Anti-TNF-alpha Therapy Can Be Independent of Pubertal Progress and Glucocorticoid Reduction. J. Pediatr. Gastr. Nutr. 2011, 52, 31–37. [Google Scholar] [CrossRef]
- Borrelli, O.; Cordischi, L.; Cirulli, M.; Paganelli, M.; Labalestra, V.; Uccini, S.; Russo, P.M.; Cucchiara, S. Polymeric diet alone versus corticosteroids in the treatment of active pediatric Crohn’s disease: A randomized controlled open-label trial. Clin. Gastroenterol. Hepatol. 2006, 4, 744–753. [Google Scholar] [CrossRef]
- Swaminath, A.; Feathers, A.; Ananthakrishnan, A.N.; Falzon, L.; Li Ferry, S. Systematic review with meta-analysis: Enteral nutrition therapy for the induction of remission in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2017, 46, 645–656. [Google Scholar] [CrossRef] [Green Version]
- Svolos, V.; Hansen, R.; Nichols, B.; Quince, C.; Ijaz, U.Z.; Papadopoulou, R.T.; Edwards, C.A.; Watson, D.; Alghamdi, A.; Brejnrod, A.; et al. Treatment of Active Crohn’s Disease With an Ordinary Food-based Diet That Replicates Exclusive Enteral Nutrition. Gastroenterology 2019, 156, 1354–1367.e1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerasimidis, K.; McGrogan, P.; Hassan, K.; Edwards, C.A. Dietary modifications, nutritional supplements and alternative medicine in paediatric patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2008, 27, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Gerasimidis, K.; McGrogan, P.; Edwards, C.A. The aetiology and impact of malnutrition in paediatric inflammatory bowel disease. J. Hum. Nutr. Diet. 2011, 24, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Casanova, M.J.; Chaparro, M.; Molina, B.; Merino, O.; Batanero, R.; Dueñas-Sadornil, C.; Robledo, P.; Garcia-Albert, A.M.; Gómez-Sánchez, M.B.; Calvet, X.; et al. Prevalence of Malnutrition and Nutritional Characteristics of Patients With Inflammatory Bowel Disease. J. Crohns Colitis 2017, 11, 1430–1439. [Google Scholar] [CrossRef]
- MacMaster, M.J.; Damianopoulou, S.; Thomson, C.; Talwar, D.; Stefanowicz, F.; Catchpole, A.; Gerasimidis, K.; Gaya, D.R. A prospective analysis of micronutrient status in quiescent inflammatory bowel disease. Clin. Nutr. 2021, 40, 327–331. [Google Scholar] [CrossRef]
- Vernia, P.; Loizos, P.; Di Giuseppantonio, I.; Amore, B.; Chiappini, A.; Cannizzaro, S. Dietary calcium intake in patients with inflammatory bowel disease. J. Crohns Colitis 2014, 8, 312–317. [Google Scholar] [CrossRef] [Green Version]
- Pierote, N.R.; Braz, A.F.; Barros, S.L.; Moita Neto, J.M.; Parente, J.M.L.; Silva, M.; Beserra, M.S.; Soares, N.R.M.; Marreiro, D.N.; do Noscimento Nogueira, N. Effect of mineral status and glucocorticoid use on bone mineral density in patients with Crohn’s disease. Nutrition 2018, 48, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Ates, Y.; Degertekin, B.; Erdil, A.; Yaman, H.; Dagalp, K. Serum ghrelin levels in inflammatory bowel disease with relation to disease activity and nutritional status. Dig. Dis. Sci. 2008, 53, 2215–2221. [Google Scholar] [CrossRef] [PubMed]
- Pons, R.; Whitten, K.E.; Woodhead, H.; Leach, S.T.; Lemberg, D.A.; Day, A.S. Dietary intakes of children with Crohn’s disease. Br. J. Nutr. 2009, 102, 1052–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghdassi, E.; Wendland, B.E.; Stapleton, M.; Raman, M.; Allard, J.P. Adequacy of Nutritional Intake in a Canadian Population of Patients with Crohn’s Disease. J. Am. Diet. Assoc. 2007, 107, 1575–1580. [Google Scholar] [CrossRef]
- Taylor, L.; Almutairdi, A.; Shommu, N.; Fedorak, R.; Ghosh, S.; Reimer, R.A.; Panaccione, R.; Raman, M. Cross-Sectional Analysis of Overall Dietary Intake and Mediterranean Dietary Pattern in Patients with Crohn’s Disease. Nutrients 2018, 10, 1761. [Google Scholar] [CrossRef] [Green Version]
- Nic Suibhne, T.; Raftery, T.C.; McMahon, O.; Walsh, C.; O’Morain, C.; O’Sullivan, M. High prevalence of overweight and obesity in adults with Crohn’s disease: Associations with disease and lifestyle factors. J. Crohns Colitis 2013, 7, e241–e248. [Google Scholar] [CrossRef] [Green Version]
- Flores, A.; Burstein, E.; Cipher, D.J.; Feagins, L.A. Obesity in Inflammatory Bowel Disease: A Marker of Less Severe Disease. Dig. Dis. Sci. 2015, 60, 2436–2445. [Google Scholar] [CrossRef]
- Greuter, T.; Porchet, F.; Braga-Neto, M.B.; Rossel, J.-B.; Biedermann, L.; Schreiner, P.; Scharl, M.; Schoepfer, A.M.; Safroneeva, E.; Straumann, A.; et al. Impact of obesity on disease activity and disease outcome in inflammatory bowel disease: Results from the Swiss inflammatory bowel disease cohort. United Eur. Gastroenterol. J. 2020, 8, 1196–1207. [Google Scholar] [CrossRef]
- Kugathasan, S.; Nebel, J.; Skelton, J.A.; Markowitz, J.; Keljo, D.; Rosh, J.; LeLeiko, N.; Mack, D.; Griffiths, A.; Bousvaros, A.; et al. Body mass index in children with newly diagnosed inflammatory bowel disease: Observations from two multicenter North American inception cohorts. J. Pediatr. 2007, 151, 523–527. [Google Scholar] [CrossRef]
- Long, M.D.; Crandall, W.V.; Leibowitz, I.H.; Duffy, L.; Del Rosario, F.; Kim, S.C.; Integlia, M.J.; Berman, J.; Grunow, J.; Colletti, R.B. Prevalence and epidemiology of overweight and obesity in children with inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 2162–2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindler, J.M.; Pollock, N.K.; Ross, H.L.; Modlesky, C.M.; Singh, H.; Laing, E.M.; Lewis, R.D. Obese Versus Normal-Weight Late-Adolescent Females have Inferior Trabecular Bone Microarchitecture: A Pilot Case-Control Study. Calcif. Tissue Int. 2017, 101, 479–488. [Google Scholar] [CrossRef]
- Hamrick, M.W.; McGee-Lawrence, M.E.; Frechette, D.M. Fatty Infiltration of Skeletal Muscle: Mechanisms and Comparisons with Bone Marrow Adiposity. Front. Endocrinol. (Lausanne) 2016, 7, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnham, J.M.; Shults, J.; Semeao, E.; Foster, B.J.; Zemel, B.S.; Stallings, V.A.; Leonard, M.B. Body-composition alterations consistent with cachexia in children and young adults with Crohn disease. Am. J. Clin. Nutr. 2005, 82, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, G.V.; Schmidt, S.; Mellstrom, D.; Ohlsson, C.; Karlsson, M.; Lorentzon, M.; Saalman, R. Altered body composition profiles in young adults with childhood-onset inflammatory bowel disease. Scand. J. Gastroentero. 2020, 55, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Thangarajah, D.; Hyde, M.J.; Konteti, V.K.S.; Santhakumaran, S.; Frost, G.; Fell, J.M.E. Systematic review: Body composition in children with inflammatory bowel disease. Aliment Pharm. Ther. 2015, 42, 142–157. [Google Scholar] [CrossRef] [Green Version]
- Canalis, E.; Mazziotti, G.; Giustina, A.; Bilezikian, J.P. Glucocorticoid-induced osteoporosis: Pathophysiology and therapy. Osteoporos. Int. 2007, 18, 1319–1328. [Google Scholar] [CrossRef]
- Jia, D.; O’Brien, C.A.; Stewart, S.A.; Manolagas, S.C.; Weinstein, R.S. Glucocorticoids act directly on osteoclasts to increase their life span and reduce bone density. Endocrinology 2006, 147, 5592–5599. [Google Scholar] [CrossRef] [Green Version]
- Schakman, O.; Gilson, H.; Thissen, J.P. Mechanisms of glucocorticoid-induced myopathy. J. Endocrinol. 2008, 197, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, D.B. Growth suppression by glucocorticoid therapy. Endocrin. Metab. Clin. 1996, 25, 699–717. [Google Scholar] [CrossRef]
- Ward, L.M. Glucocorticoid-Induced Osteoporosis: Why Kids Are Different. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Natsui, K.; Tanaka, K.; Suda, M.; Yasoda, A.; Sakuma, Y.; Ozasa, A.; Ozaki, S.; Nakao, K. High-dose glucocorticoid treatment induces rapid loss of trabecular bone mineral density and lean body mass. Osteoporos. Int. 2006, 17, 105–108. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.A.; Jia, D.; Plotkin, L.I.; Bellido, T.; Powers, C.C.; Stewart, S.A.; Manolagas, S.C.; Weinstein, R.S. Glucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strength. Endocrinology 2004, 145, 1835–1841. [Google Scholar] [CrossRef] [Green Version]
- Hofbauer, L.C.; Gori, F.; Riggs, B.L.; Lacey, D.L.; Dunstan, C.R.; Spelsberg, T.C.; Khosla, S. Stimulation of osteoprotegerin ligand and inhibition of osteoprotegerin production by glucocorticoids in human osteoblastic lineage cells: Potential paracrine mechanisms of glucocorticoid-induced osteoporosis. Endocrinology 1999, 140, 4382–4389. [Google Scholar] [CrossRef]
- Canalis, E. Mechanisms of glucocorticoid action in bone. Curr. Osteoporos. Rep. 2005, 3, 98–102. [Google Scholar] [CrossRef]
- Kao, K.T.; Denker, M.; Zacharin, M.; Wong, S.C. Pubertal abnormalities in adolescents with chronic disease. Best Pract. Res. Clin. Endocrinol. Metab. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chrysis, D.; Ritzen, E.M.; Sävendahl, L. Growth retardation induced by dexamethasone is associated with increased apoptosis of the growth plate chondrocytes. J. Endocrinol. 2003, 176, 331–337. [Google Scholar] [CrossRef]
- Bianchi, M.L.; Biggar, D.; Bushby, K.; Rogol, A.D.; Rutter, M.M.; Tseng, B. Endocrine aspects of Duchenne muscular dystrophy. Neuromuscul. Disord. 2011, 21, 298–303. [Google Scholar] [CrossRef]
- Minetto, M.A.; Botter, A.; Lanfranco, F.; Baldi, M.; Ghigo, E.; Arvat, E. Muscle fiber conduction slowing and decreased levels of circulating muscle proteins after short-term dexamethasone administration in healthy subjects. J. Clin. Endocrinol. Metab. 2010, 95, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Waddell, D.S.; Baehr, L.M.; Van Den Brandt, J.; Johnsen, S.A.; Reichardt, H.M.; Furlow, J.D.; Bodine, S.C. The glucocorticoid receptor and FOXO1 synergistically activate the skeletal muscle atrophy-associated MuRF1 gene. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E785–E797. [Google Scholar] [CrossRef]
- Sato, A.Y.; Richardson, D.; Cregor, M.; Davis, H.M.; Au, E.D.; McAndrews, K.; Zimmers, T.A.; Organ, J.M.; Peacock, M.; Plotkin, L.I. Glucocorticoids induce bone and muscle atrophy by tissue-specific mechanisms upstream of E3 ubiquitin ligases. Endocrinology 2017, 158, 664–677. [Google Scholar]
- Kapasi, R.; Glatter, J.; Lamb, C.A.; Acheson, A.G.; Andrews, C.; Arnott, I.D.; Barrett, K.J.; Bell, G.; Bhatnagar, G.; Bloom, S.; et al. Consensus standards of healthcare for adults and children with inflammatory bowel disease in the UK. Frontline Gastroenterol. 2020, 11, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The Role of Vitamin D in Inflammatory Bowel Disease: Mechanism to Management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef] [Green Version]
- Chatu, S.; Chhaya, V.; Holmes, R.; Neild, P.; Kang, J.Y.; Pollok, R.C.; Poullis, A. Factors associated with vitamin D deficiency in a multicultural inflammatory bowel disease cohort. Frontline Gastroenterol. 2013, 4, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frigstad, S.O.; Høivik, M.; Jahnsen, J.; Dahl, S.R.; Cvancarova, M.; Grimstad, T.; Berset, I.P.; Huppertz-Hauss, G.; Hovde, Ø.; Torp, R.; et al. Vitamin D deficiency in inflammatory bowel disease: Prevalence and predictors in a Norwegian outpatient population. Scand. J. Gastroenterol. 2017, 52, 100–106. [Google Scholar] [CrossRef]
- van Langenberg, D.R.; Della Gatta, P.; Hill, B.; Zacharewicz, E.; Gibson, P.R.; Russell, A.P. Delving into disability in Crohn’s disease: Dysregulation of molecular pathways may explain skeletal muscle loss in Crohn’s disease. J. Crohns Colitis 2014, 8, 626–634. [Google Scholar] [CrossRef]
- Hradsky, O.; Soucek, O.; Maratova, K.; Matyskova, J.; Copova, I.; Zarubova, K.; Bronsky, J.; Sumnik, Z. Supplementation with 2000 IU of Cholecalciferol Is Associated with Improvement of Trabecular Bone Mineral Density and Muscle Power in Pediatric Patients with IBD. Inflamm. Bowel Dis. 2017, 23, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, M.T.; Kantorovich, V.; Vasiliauskas, E.A.; Gruntmanis, U.; Matuk, R.; Daigle, K.; Chen, S.; Zehnder, D.; Lin, Y.C.; Yang, H.; et al. Measurement of vitamin D levels in inflammatory bowel disease patients reveals a subset of Crohn’s disease patients with elevated 1,25-dihydroxyvitamin D and low bone mineral density. Gut 2004, 53, 1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, D.; Duggan, P.; O’Brien, M.; Kiely, M.; McCarthy, J.; Shanahan, F.; Cashman, K.D. Seasonality of vitamin D status and bone turnover in patients with Crohn’s disease. Aliment. Pharm. Ther. 2005, 21, 1073–1083. [Google Scholar] [CrossRef]
- Abraham, B.; Malaty, H. Vitamin D Deficiency and Abnormal DEXA Scans in Inflammatory Bowel Disease Patients: 1221. Off. J. Am. Coll. Gastroenterol. ACG 2010, 105, S448. [Google Scholar] [CrossRef]
- Maratova, K.; Hradsky, O.; Matyskova, J.; Copova, I.; Soucek, O.; Sumnik, Z.; Bronsky, J. Musculoskeletal system in children and adolescents with inflammatory bowel disease: Normal muscle force, decreased trabecular bone mineral density and low prevalence of vertebral fractures. Eur. J. Pediatr. 2017, 176, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Bakker, S.F.; Dik, V.K.; Witte, B.I.; Lips, P.; Roos, J.C.; Van Bodegraven, A.A. Increase in bone mineral density in strictly treated Crohn’s disease patients with concomitant calcium and vitamin D supplementation. J. Crohns Colitis 2013, 7, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Eerden, B.C.; Karperien, M.; Wit, J.M. Systemic and local regulation of the growth plate. Endocr. Rev. 2003, 24, 782–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassem, M.; Blum, W.; Ristelli, J.; Mosekilde, L.; Eriksen, E. Growth hormone stimulates proliferation and differentiation of normal human osteoblast-like cells in vitro. Calcified Tissue Int. 1993, 52, 222–226. [Google Scholar] [CrossRef]
- Olney, R.C. Regulation of bone mass by growth hormone. Med. Pediatric Oncol. 2003, 41, 228–234. [Google Scholar] [CrossRef]
- Ahmed, S.F.; Farquharson, C. The effect of GH and IGF1 on linear growth and skeletal development and their modulation by SOCS proteins. J. Endocrinol. 2010, 206, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiaffino, S.; Mammucari, C. Regulation of skeletal muscle growth by the IGF1-Akt/PKB pathway: Insights from genetic models. Skelet. Muscle 2011, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.C.; Smyth, A.; McNeill, E.; Galloway, P.J.; Hassan, K.; McGrogan, P.; Ahmed, S.F. The growth hormone insulin-like growth factor 1 axis in children and adolescents with inflammatory bowel disease and growth retardation. Clin. Endocrinol. 2010, 73, 220–228. [Google Scholar] [CrossRef]
- Sanderson, I.R. Growth problems in children with IBD. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.; Macrae, V.; McGrogan, P.; Ahmed, S. The role of pro-inflammatory cytokines in inflammatory bowel disease growth retardation. J. Pediatr. Gastr. Nutr. 2006, 43, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Denson, L.A.; Menon, R.K.; Shaufl, A.; Bajwa, H.S.; Williams, C.R.; Karpen, S.J. TNF-α downregulates murine hepatic growth hormone receptor expression by inhibiting Sp1 and Sp3 binding. J. Clin. Investig. 2001, 107, 1451–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Benedetti, F.; Meazza, C.; Oliveri, M.; Pignatti, P.; Vivarelli, M.; Alonzi, T.; Fattori, E.; Garrone, S.; Barreca, A.; Martini, A. Effect of IL-6 on IGF binding protein-3: A study in IL-6 transgenic mice and in patients with systemic juvenile idiopathic arthritis. Endocrinology 2001, 142, 4818–4826. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Lustig, R.H.; Koh-n, M.A.; McCracken, M.; Vittinghoff, E. Sex differences in statural growth impairment in Crohn’s disease: Role of IGF-1. Inflamm. Bowel Dis. 2011, 17, 2318–2325. [Google Scholar] [CrossRef]
- Grønbek, H.; Thøgersen, T.; Frystyk, J.; Vilstrup, H.; Flyvbjerg, A.; Dahlerup, J.F. Low free and total insulinlike growth factor I (IGF-I) and IGF binding protein-3 levels in chronic inflammatory bowel disease: Partial normalization during prednisolone treatment. Am. J. Gastroenterol. 2002, 97, 673–678. [Google Scholar] [CrossRef]
- Katsanos, K.H.; Tsatsoulis, A.; Christodoulou, D.; Challa, A.; Katsaraki, A.; Tsianos, E.V. Reduced serum insulin-like growth factor-1 (IGF-1) and IGF-binding protein-3 levels in adults with inflammatory bowel disease. Growth Horm. IGF Res. 2001, 11, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Slonim, A.E.; Bulone, L.; Damore, M.B.; Goldberg, T.; Wingertzahn, M.A.; McKinley, M.J. A preliminary study of growth hormone therapy for Crohn’s disease. N. Engl. J. Med. 2000, 342, 1633–1637. [Google Scholar] [CrossRef]
- Compston, J.E. Sex Steroids and Bone. Physiol. Rev. 2001, 81, 419–447. [Google Scholar] [CrossRef] [Green Version]
- Riggs, B.L. The mechanisms of estrogen regulation of bone resorption. J. Clin. Investig. 2000, 106, 1203–1204. [Google Scholar] [CrossRef] [Green Version]
- Kameda, T.; Mano, H.; Yuasa, T.; Mori, Y.; Miyazawa, K.; Shiokawa, M.; Nakamaru, Y.; Hiroi, E.; Hiura, K.; Kameda, A.; et al. Estrogen inhibits bone resorption by directly inducing apoptosis of the bone-resorbing osteoclasts. J. Exp. Med. 1997, 186, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Khosla, S.; Oursler, M.J.; Monroe, D.G. Estrogen and the skeleton. Trends Endocrinol. Metab. TEM 2012, 23, 576–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, B.L.; Khosla, S. Androgens and bone. Steroids 2009, 74, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Abu, E.O.; Horner, A.; Kusec, V.; Triffitt, J.T.; Compston, J.E. The localization of androgen receptors in human bone. J. Clin. Endocrinol. Metab. 1997, 82, 3493–3497. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.A.; Rudman, D.; Wilson, C.R.; Drinka, P.J.; Basu, S.N.; Mattson, D.E.; Richardson, T.J. Observations on nursing home residents with a history of hip fracture. Am. J. Med. Sci. 1995, 310, 229–234. [Google Scholar] [PubMed]
- Popat, V.B.; Calis, K.A.; Vanderhoof, V.H.; Cizza, G.; Reynolds, J.C.; Sebring, N.; Troendle, J.F.; Nelson, L.M. Bone mineral density in estrogen-deficient young women. J. Clin. Endocrinol. Metab. 2009, 94, 2277–2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Lustig, R.H.; Kohn, M.A.; Vittinghoff, E. Menarche in pediatric patients with Crohn’s disease. Dig. Dis. Sci. 2012, 57, 2975–2981. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.; Malik, S.; Russell, R.K.; Bishop, J.; McGrogan, P.; Ahmed, S.F. Impact of inflammatory bowel disease on pubertal growth. Horm. Res. Paediatr. 2011, 76, 293–299. [Google Scholar] [CrossRef]
- Ballinger, A.B.; Savage, M.O.; Sanderson, I.R. Delayed puberty associated with inflammatory bowel disease. Pediatr. Res. 2003, 53, 205–210. [Google Scholar] [CrossRef]
- Karmiris, K.; Koutroubakis, I.E.; Xidakis, C.; Polychronaki, M.; Voudouri, T.; Kouroumalis, E.A. Circulating levels of leptin, adiponectin, resistin, and ghrelin in inflammatory bowel disease. Inflamm. Bowel Dis. 2006, 12, 100–105. [Google Scholar] [CrossRef]
- DeBoer, M.D.; Li, Y.; Cohn, S. Colitis causes delay in puberty in female mice out of proportion to changes in leptin and corticosterone. J. Gastroenterol. 2010, 45, 277–284. [Google Scholar] [CrossRef] [Green Version]
- DeBoer, M.D.; Thayu, M.; Griffin, L.M.; Baldassano, R.N.; Denson, L.A.; Zemel, B.S.; Denburg, M.R.; Agard, H.E.; Herskovitz, R.; Long, J. Increases in Sex Hormones during Anti-Tumor Necrosis Factor α Therapy in Adolescents with Crohn’s Disease. J. Pediatrics 2016, 171, 146–152.e142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, R.J.; Iqbal, S.J.; Al-Azzawi, F.; Abrams, K.; Mayberry, J.F. Sex hormone status and bone metabolism in men with Crohn’s disease. Aliment. Pharmacol. Ther. 1998, 12, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Klaus, J.; Reinshagen, M.; Adler, G.; Boehm, B.O.; von Tirpitz, C. Bones and Crohn’s: Estradiol deficiency in men with Crohn’s disease is not associated with reduced bone mineral density. BMC Gastroenterol. 2008, 8, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, S.; Bianchi, M.L.; Eisman, J.A.; Foldes, A.J.; Adami, S.; Wahl, D.A.; Stepan, J.J.; de Vernejoul, M.C.; Kaufman, J.M.; For the, I.O.F.C.o.S.A.W.G.o.O.P. Osteoporosis in young adults: Pathophysiology, diagnosis, and management. Osteoporos. Int. 2012, 23, 2735–2748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Yoon, H.; Oh, D.J.; Lee, J.M.; Choi, Y.J.; Shin, C.M.; Park, Y.S.; Kim, N.; Lee, D.H.; Kim, J.S. The prevalence of sarcopenia and its effect on prognosis in patients with Crohn’s disease. Intest. Res. 2020, 18, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.V.; Ooi, S.; Schultz, C.G.; Goess, C.; Grafton, R.; Hughes, J.; Lim, A.; Bartholomeusz, F.D.; Andrews, J.M. Low muscle mass and sarcopenia: Common and predictive of osteopenia in inflammatory bowel disease. Aliment. Pharm. Ther. 2015, 41, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Werkstetter, K.J.; Schatz, S.B.; Alberer, M.; Filipiak-Pittroff, B.; Koletzko, S. Influence of Exclusive Enteral Nutrition Therapy on Bone Density and Geometry in Newly Diagnosed Pediatric Crohn’s Disease Patients. Ann. Nutr. Metab. 2013, 63, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Dubner, S.E.; Shults, J.; Baldassano, R.N.; Zemel, B.S.; Thayu, M.; Burnham, J.M.; Herskovitz, R.M.; Howard, K.M.; Leonarda, M.B. Longitudinal Assessment of Bone Density and Structure in an Incident Cohort of Children With Crohn’s Disease. Gastroenterology 2009, 136, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altowati, M.M.A.; Shepherd, S.; McMillan, M.; McGrogan, P.; Russell, R.; Ahmed, S.F.; Wong, S.C. Persistence of Muscle-bone Deficits Following Anti-tumour Necrosis Factor Therapy in Adolescents With Crohn Disease. J. Pediatr. Gastr. Nutr. 2018, 67, 738–744. [Google Scholar] [CrossRef]
- Griffin, L.M.; Thayu, M.; Baldassano, R.N.; DeBoer, M.D.; Zemel, B.S.; Denburg, M.R.; Denson, L.A.; Shults, J.; Herskovitz, R.; Long, J.; et al. Improvements in Bone Density and Structure during Anti-TNF-alpha Therapy in Pediatric Crohn’s Disease. J. Clin. Endocr. Metab. 2015, 100, 2630–2639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, H.M. Bone Mass and the Mechanostat—A Proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Modlesky, C.M.; Subramanian, P.; Miller, F. Underdeveloped trabecular bone microarchitecture is detected in children with cerebral palsy using high-resolution magnetic resonance imaging. Osteoporos. Int. 2008, 19, 169–176. [Google Scholar] [CrossRef]
- Rittweger, J.; Frost, H.M.; Schiessl, H.; Ohshima, H.; Alkner, B.; Tesch, P.; Felsenberg, D. Muscle atrophy and bone loss after 90 days’ bed rest and the effects of flywheel resistive exercise and pamidronate: Results from the LTBR study. Bone 2005, 36, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Tew, G.A.; Jones, K.; Mikocka-Walus, A. Physical Activity Habits, Limitations, and Predictors in People with Inflammatory Bowel Disease: A Large Cross-sectional Online Survey. Inflamm. Bowel Dis. 2016, 22, 2933–2942. [Google Scholar] [CrossRef] [Green Version]
- DeFilippis, E.M.; Tabani, S.; Warren, R.U.; Christos, P.J.; Bosworth, B.P.; Scherl, E.J. Exercise and Self-Reported Limitations in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2016, 61, 215–220. [Google Scholar] [CrossRef]
- Gatt, K.; Schembri, J.; Katsanos, K.H.; Christodoulou, D.; Karmiris, K.; Kopylov, U.; Pontas, C.; Koutroubakis, I.E.; Foteinogiannopoulou, K.; Fabian, A.; et al. Inflammatory Bowel Disease [IBD] and Physical Activity: A Study on the Impact of Diagnosis on the Level of Exercise Amongst Patients With IBD. J. Crohns Colitis 2019, 13, 686–692. [Google Scholar] [CrossRef]
- van Langenberg, D.R.; Papandony, M.C.; Gibson, P.R. Sleep and physical activity measured by accelerometry in Crohn’s disease. Aliment. Pharm. Ther. 2015, 41, 991–1004. [Google Scholar] [CrossRef]
- Vogelaar, L.; Van den Berg-Emons, R.; Bussmann, H.; Rozenberg, R.; Timman, R.; Van der Woude, C.J. Physical fitness and physical activity in fatigued and non-fatigued inflammatory bowel disease patients. Scand. J. Gastroentero. 2015, 50, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Vanhelst, J.; Beghin, L.; Turck, D.; Labreuche, J.; Coopman, S.; Gottrand, F.; Ley, D. Daily physical activity patterns in children and adolescents with inflammatory bowel disease. Pediatr. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lamers, C.R.; de Roos, N.M.; Koppelman, L.J.M.; Hopman, M.T.E.; Witteman, B.J.M. Patient experiences with the role of physical activity in inflammatory bowel disease: Results from a survey and interviews. BMC Gastroenterol. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vanhelst, J.; Vidal, F.; Turck, D.; Drumez, E.; Djeddi, D.; Devouge, E.; Spyckerelle, C.; Zandzou, S.G.; Legrand, C.; Michaud, L.; et al. Physical activity is associated with improved bone health in children with inflammatory bowel disease. Clin. Nutr. 2020, 39, 1793–1798. [Google Scholar] [CrossRef]
- Robinson, R.J.; Krzywicki, T.; Almond, L.; Al-Azzawi, F.; Abrams, K.; Iqbal, S.J.; Mayberry, J.F. Effect of a low-impact exercise program on bone mineral density in Crohn’s disease: A randomized controlled trial. Gastroenterology 1998, 115, 36–41. [Google Scholar] [CrossRef]
- Jones, K.; Baker, K.; Speight, R.A.; Thompson, N.P.; Tew, G.A. Randomised clinical trial: Combined impact and resistance training in adults with stable Crohn’s disease. Aliment. Pharm. Ther. 2020, 52, 964–975. [Google Scholar] [CrossRef]
- Crabtree, N.J.; Shaw, N.J.; Bishop, N.J.; Adams, J.E.; Mughal, M.Z.; Arundel, P.; Fewtrell, M.S.; Ahmed, S.F.; Treadgold, L.A.; Hogler, W.; et al. Amalgamated Reference Data for Size-Adjusted Bone Densitometry Measurements in 3598 Children and Young Adults-the ALPHABET Study. J. Bone Miner. Res. 2017, 32, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Hill, R.J.; Brookes, D.S.; Lewindon, P.J.; Withers, G.D.; Ee, L.C.; Connor, F.L.; Cleghorn, G.J.; Davies, P.S. Bone health in children with inflammatory bowel disease: Adjusting for bone age. J. Pediatr. Gastr. Nutr. 2009, 48, 538–543. [Google Scholar] [CrossRef]
- Ahmed, S.; Horrocks, I.; Patterson, T.; Zaidi, S.; Ling, S.; McGrogan, P.; Weaver, L. Bone mineral assessment by dual energy X-ray absorptiometry in children with inflammatory bowel disease: Evaluation by age or bone area. J. Pediatr. Gastr. Nutr. 2004, 38, 276–280. [Google Scholar] [CrossRef]
- Pichler, J.; Huber, W.D.; Aufricht, C.; Bidmon-Fliegenschnee, B. Growth and bone health in paediatric patients with Crohn’s disease receiving subcutaneous tumor necrosis factor antibody. World J. Gastroenterol. 2015, 21, 6613–6620. [Google Scholar] [CrossRef] [PubMed]
- Laakso, S.; Valta, H.; Verkasalo, M.; Toiviainen-Salo, S.; Viljakainen, H.; Makitie, O. Impaired bone health in inflammatory bowel disease: A case-control study in 80 pediatric patients. Calcif. Tissue Int. 2012, 91, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Paski, S.; Issenman, R.; Webber, C. Lumbar spine bone mineral density at diagnosis and during follow-up in children with IBD. J. Clin. Densitom. 2004, 7, 290–295. [Google Scholar] [CrossRef]
- Pepe, J.; Zawadynski, S.; Herrmann, F.R.; Juillerat, P.; Michetti, P.; Ferrari-Lacraz, S.; Belli, D.; Ratib, O.; Rizzoli, R.; Chevalley, T.; et al. Structural Basis of Bone Fragility in Young Subjects with Inflammatory Bowel Disease: A High-resolution pQCT Study of the SWISS IBD Cohort (SIBDC). Inflamm. Bowel Dis. 2017, 23, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Haschka, J.; Hirschmann, S.; Kleyer, A.; Englbrecht, M.; Faustini, F.; Simon, D.; Figueiredo, C.P.; Schuster, L.; Muschitz, C.; Kocijan, R.; et al. High-resolution Quantitative Computed Tomography Demonstrates Structural Defects in Cortical and Trabecular Bone in IBD Patients. J. Crohns Colitis 2016, 10, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Targownik, L.E.; Bernstein, C.N.; Nugent, Z.; Leslie, W.D. Inflammatory bowel disease has a small effect on bone mineral density and risk for osteoporosis. Clin. Gastroenterol. Hepatol. 2013, 11, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Miller, N.; Rogala, L.; Bernstein, C.N. Vitamin D status and bone density in recently diagnosed inflammatory bowel disease: The Manitoba IBD Cohort Study. Am. J. Gastroenterol. 2008, 103, 1451–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, C.N.; Leslie, W.D.; Taback, S.P. Bone density in a population-based cohort of premenopausal adult women with early onset inflammatory bowel disease. Am. J. Gastroenterol. 2003, 98, 1094–1100. [Google Scholar] [CrossRef]
- Schoon, E.J.; Blok, B.M.; Geerling, B.J.; Russel, M.G.; Stockbrügger, R.W.; Brummer, R.J. Bone mineral density in patients with recently diagnosed inflammatory bowel disease. Gastroenterology 2000, 119, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.J.; Azzawi, F.A.; Iqbal, S.J.; Kryswcki, T.; Almond, L.; Abrams, K.; Mayberry, J.F. Osteoporosis and Determinants of Bone Density in Patients with Crohn’s Disease. Dig. Dis. Sci. 1998, 43, 2500–2506. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Cowen, S.; Hannan, W.J.; Ferguson, A. Low bone mineral density in Crohn’s disease, but not in ulcerative colitis, at diagnosis. Gastroenterology 1994, 107, 1031–1039. [Google Scholar] [CrossRef]
- Szafors, P.; Che, H.; Barnetche, T.; Morel, J.; Gaujoux-Viala, C.; Combe, B.; Lukas, C. Risk of fracture and low bone mineral density in adults with inflammatory bowel diseases. A systematic literature review with meta-analysis. Osteoporos. Int. 2018, 29, 2389–2397. [Google Scholar] [CrossRef]
- Oostlander, A.E.; Bravenboer, N.; Sohl, E.; Holzmann, P.J.; van der Woude, C.J.; Dijkstra, G.; Stokkers, P.C.; Oldenburg, B.; Netelenbos, J.C.; Hommes, D.W.; et al. Histomorphometric analysis reveals reduced bone mass and bone formation in patients with quiescent Crohn’s disease. Gastroenterology 2011, 140, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croucher, P.I.; Vedi, S.; Motley, R.J.; Garrahan, N.J.; Stanton, M.R.; Compston, J.E. Reduced bone formation in patients with osteoporosis associated with inflammatory bowel disease. Osteoporos. Int. 1993, 3, 236–241. [Google Scholar] [CrossRef]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns Colitis 2020. [Google Scholar] [CrossRef] [PubMed]
- Laakso, S.; Valta, H.; Verkasalo, M.; Toiviainen-Salo, S.; Makitie, O. Compromised Peak Bone Mass in Patients with Inflammatory Bowel Disease-A Prospective Study. J. Pediatr. 2014, 164, 1436–1443.e1. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Chen, X.; Chen, X.; Zhang, S.; Jiang, T.; Chang, J.; Gao, Y. Bone Loss Prevention of Bisphosphonates in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2017, 2017, 2736547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, L.M. Part 2: When Should Bisphosphonates Be Used in Children with Chronic Illness Osteoporosis? Curr. Osteoporos. Rep. 2021, 19, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Lyu, H.; Jundi, B.; Xu, C.; Tedeschi, S.K.; Yoshida, K.; Zhao, S.; Nigwekar, S.U.; Leder, B.Z.; Solomon, D.H. Comparison of Denosumab and Bisphosphonates in Patients With Osteoporosis: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Endocrinol. Metab. 2019, 104, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Miedany, Y.E.; Gaafary, M.E.; Toth, M.; Hegazi, M.O.; Aroussy, N.E.; Hassan, W.; Almedany, S.; Nasr, A.; Bahlas, S.; Galal, S.; et al. Is there a potential dual effect of denosumab for treatment of osteoporosis and sarcopenia? Clin. Rheumatol. 2021. [Google Scholar] [CrossRef]
- Khafipour, A.; Eissa, N.; Munyaka, P.M.; Rabbi, M.F.; Kapoor, K.; Kermarrec, L.; Khafipour, E.; Bernstein, C.N.; Ghia, J.-E. Denosumab Regulates Gut Microbiota Composition and Cytokines in Dinitrobenzene Sulfonic Acid (DNBS)-Experimental Colitis. Front. Microbiol. 2020, 11, 1405. [Google Scholar] [CrossRef]


{kind=link}
| Author (year) Country | Design | Participants (N) Age (years) | Methods | Current or Previous Glucocorticoids (%) | Bone/Muscle Findings | Comments |
|---|---|---|---|---|---|---|
| Altowati et al. (2018) [123] Scotland | Prospective cohort | 19 CD 14.9 (11.2, 17.2) | pQCT non-dominant radius and tibia DXA TB and LS | Current: 47%. | ↓ Trabecular vBMD ↔ Cortical vBMD ↓ Cortical thickness ↓ Muscle CSA (Radius only) ↓ TB and LS aBMD | No improvement in bone or muscle outcomes after 12 months anti-TNF-α. IGF-1 improved only in those with low levels at baseline. |
| Ward et al. (2017) [6] Canada | Cross-sectional cohort | 73 CD 13.9 (7, 17.7) | pQCT left tibia DXA TB and LS VF radiograph | Current: 64% | ↓ Trabecular vBMD ↑ Endosteal and ↓ Periosteal circ. ↓ Cortical thickness and Muscle CSA ↓ LS aBMD, BMAD and TB BMC 1 VF | Newly diagnosed <35 days of initial therapy. 90% moderate-to-severe disease. |
| Maratova et al. (2017) [86] Czech Republic | Cross-sectional cohort | 70 IBD (53 CD) 14.2 (IQR 12.7, 16.1) | pQCT non-dominant tibia VF radiograph | Current: NR Ever: 23% (within previous 12 months) | ↓ Trabecular vBMD ↓ Cortical Thickness ↑ Cortical vBMD and SSI 1 VF; ↓ vertebral height in 27%. | Height adjusted pQCT Z-scores. All remission or mild disease. |
| Griffin et al. (2015) [124] USA | Prospective cohort | 74 CD 14 (5, 21) | pQCT left tibia | Current: 32% | ↓ Trabecular vBMD ↔ Cortical vBMD ↓ Muscle CSA ↑ Endosteal and ↓ Periosteal circ. | Infliximab induction cohort. 50% severe disease. Trabecular vBMD improved but still low at 12 months. |
| Pichler et al. (2015) [141] Austria | Retrospective | 18 CD 14.4 (5.3, 19.1) | DXA LS | Current: 61% | ↓ LS aBMD and BMAD | No change in aBMD or BMAD after 12-months anti-TNF-α. |
| Laakso et al. (2012) [142] Finland | Cross-sectional cohort | 80 IBD (28 CD) 14.9 (5.1, 20.1) | DXA TB, LS, TH and VF | Current: 30% Ever: 81% | ↓ TB & LS aBMD ↔ TH aBMD 16 VF (across 9 participants) | No differences between CD and UC. DXA Z-scores adjusted for chronological age and bone age. Large within-group variation in disease duration and cumulative GC. |
| Werkstetter et al. (2013) [121] Germany | Prospective cohort | 10 CD 13.7 (10.6, 17.7) | pQCT non-dominant radius | GC naïve | ↔ Trabecular and cortical vBMD ↓ Muscle CSA After 12 weeks: Trabecular vBMD and Muscle CSA ↑, cortical vBMD ↓. No further changes at 52 weeks. | Newly diagnosed cohort. All subsequently treated with 8 weeks EEN induction therapy. Height adjusted pQCT Z-scores. Short-term improvements in bone turnover and IGF-1, no further change at 52 weeks. |
| Ward et al. (2010) [14] Canada | Cross-sectional cohort | 20 IBD (17 CD) 14.7 (8.4, 17.7) | Iliac biopsy histomorphometry DXA TB and LS VF radiograph | GC naïve | ↔ Trabecular bone volume ↑ Trabecular number ↓ Cortical thickness ↓ LS aBMD and BMAD ↓ TB lean mass No evidence of VF | Newly diagnosed cohort. DXA lean mass Z-scores adjusted for height. |
| Bechtold et al. (2010) [12] Germany | Cross-sectional cohort | 143 IBD (98 CD) New IBD: 13 ± 3.3 Established IBD: 14.7 ± 3.4 | pQCT non-dominant radius | New IBD: GC naïve Established IBD: NR | ↓ Trabecular vBMD ↑ Cortical vBMD ↓ Bone and Muscle CSA | All IBD vs controls. Muscle CSA Z-score lower in newly diagnosed vs established disease. GC history did not influence results. |
| Dubner et al. (2009) [122] USA | Prospective cohort | 78 CD 12.7 ± 2.8 | pQCT left tibia | GC naïve | ↓ Trabecular vBMD ↔ Cortical vBMD ↓ Muscle and Fat CSA ↑ Endosteal and ↓ Periosteal Circ. ↓ Section modulus (Zp) | Newly diagnosed cohort. pQCT geometry Z-scores adjusted for tibia length. 84% growth failure. Persistent deficits in trabecular vBMD and muscle CSA at 12-months follow-up. |
| Sylvester et al. (2007) [13] USA | Prospective cohort | 58 CD 13 ± 3 | DXA TB and LS | 56% GC during follow-up. | ↓ TB & LS aBMD. No change in Z-scores at 2-year follow-up. | Newly diagnosed cohort. Bone age delay ~1 year in CD. DXA adjusted for bone age. Elevated serum IL-6 associated with low aBMD. TB aBMD positively correlated with IGF-1. |
| Burnham et al. (2005) [58] USA | Cross-sectional cohort | 104 CD 15.4 ± 4.3 | DXA TB | Current: 11% Ever: 90% | ↓ TB BMC in sex, height and puberty adjusted models. ↔ TB BMC when + adjustment for lean mass. | DXA adjusted for bone size. Low BMI Z-score associated with low bone mass. GC history is not correlated with growth or bone outcomes. |
| Gupta et al. (2004) [143] Canada | Prospective cohort | 123 IBD (82 CD) 11.8 ± 2.6 | DXA LS | NR | ↓ LS aBMD Z-score in CD ↔ LS aBMD Z-score in UC | Incident cohort. Age-adjusted DXA Z-scores. Not adjusted for body size. |
| Author (year) Country | Design | Participants (N) Age (years) | Methods | Current or Previous Glucocorticoids (%) | Bone/Muscle Findings | Comments |
|---|---|---|---|---|---|---|
| Steell et al. (2020) [5] Scotland | Cross-sectional cohort | 27 CD 23.2 (18, 36) | MRI distal femur | Current: 4% Ever: 78% | ↔ Trabecular microarchitecture ↔ Cortical geometry ↓ Muscle CSA ↑ Muscle fat | Childhood-onset cohort. Comparison w/ age and sex-matched controls. GC exposure negatively associated w/ trabecular bone volume. Muscle CSA positively associated w/ trabecular bone volume. |
| Sigurdsson et al. (2020) [59] Sweden | Cross-sectional cohort | 94 IBD (29 CD) 21.8 (18.3, 27.7) | DXA TB, LS, FN, SMI | Current: NR Ever: 93% | ↓ TB, LS, FN aBMD Z-scores in male CD and UC. ↓ SMI Z-score in male CD, not UC. ↔ TB, LS, FN aBMD and SMI Z-scores in female CD and UC. | Childhood-onset cohort. DXA not adjusted for body size. Myopenia and myopenic-obesity associated with low aBMD at all sites. |
| Pepe et al. (2018) [144] Switzerland | Cross-sectional cohort | 102 IBD (75 CD) 23.1 ± 5.8 | HR-pQCT non-dominant distal radius and tibia DXA LS, FN, PF and Radius, VF | Current: 17%. Ever: NR | ↓ aBMD at all sites. ↓ Total and trabecular vBMD ↓ Trabecular number and Cortical thickness at the tibia. ↑ Trabecular separation at radius and tibia 5 VF | Includes paediatric and adult IBD. Fractured IBD had lower total and trabecular vBMD and trabecular thickness vs non-fractured. |
| Haschka et al. (2016) [145] Germany | Cross-sectional cohort | 98 IBD (59 CD) 42.8 (IQR 30, 54) | HR-pQCT dominant ultra-distal radius | Current: 14% | ↓ Cortical vBMD in CD and UC. ↓ Cortical thickness in CD and UC. ↓ Cortical area in CD, not UC. ↓ Total and trabecular vBMD in CD, not UC. ↓ Trabecular bone volume and thickness in CD, not UC. | Poorer vBMD and structural outcomes in CD vs UC. 50% history of chronic high-dose GC. Low BMD, female sex, and lack of remission associated with a low cortical area. |
| Targownik et al. (2013) [146] Canada | Retrospective | 1230 IBD (719 CD) 49 (IQR 38, 57) | DXA LS, FN, TH | Current: 23% | ↓ aBMD T-scores at all sites in CD, not UC. | Increased risk of osteoporosis for CD vs controls in adjusted regression (OR: 1.47 (1.2, 1.78)). aBMD T-scores negatively associated with GC at all sites. |
| Leslie et al. (2008) [147] Canada | Prospective cohort | 101 IBD (56 CD) 46.9 ± 15.5 | DXA TB, LS and TH | Current: NR Ever: 60% | ↓ LS and TH aBMD T-scores ↔ TB aBMD T-scores ↔ TB, LS and TH aBMD Z-scores | Mean LS aBMD T-score at the lower end of normal (−0.76 ± 1.2). Men lower Z-scores vs women at LS. |
| Bernstein et al. (2003) [148] Canada | Cross-sectional cohort | 70 IBD (58 CD) 33 ± 7.4 | DXA TB, LS, FN and TH | Current: NR Ever: 82% | ↔ aBMD T-scores at all sites 25/70 (36%) osteopenic T-scores at ≥1 site. | ‘Early onset’ IBD (diagnosed <20 years). CD & UC presented together. Manufacturer reference data. Low BMD associated with recent amenorrhea and low body weight. |
| Schoon et al. (2000) [149] Netherlands | Cross-sectional cohort | 68 IBD (24 CD) 29.7 ± 10.4 | DXA TB, LS and TH | Current: 33% | ↔ aBMD Z-scores at all sites 18/68 (26%) osteopenic T-scores at ≥1 site. | Incident cohort <6 months from diagnosis. Mean T-scores not reported. 12.5% active disease at the time of DXA. Local controls for Z-scores (n = 68). |
| Robinson et al. (1998) [150] England | Cross-sectional cohort | 117 CD 40.6 ± 13.3 | DXA LS, PF | Current: 22% Ever: 86% | ↔ aBMD Z-scores at all sites 34/117 (29%) osteopenic, 14/117 (12%) osteoporotic (Z-scores) | DXA age- and sex-adjusted Z-scores. aBMD negative association with GC history. |
| Ghosh et al. (1994) [151] Scotland | Prospective cohort | 30 IBD (15 CD) 24 (14, 83) | DXA LS, right arm | Current: 47% | ↓ LS & arm aBMD Z-scores in CD | Newly diagnosed cohort. No change in Z-scores after 12 months follow-up. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steell, L.; Gray, S.R.; Russell, R.K.; MacDonald, J.; Seenan, J.P.; Wong, S.C.; Gaya, D.R. Pathogenesis of Musculoskeletal Deficits in Children and Adults with Inflammatory Bowel Disease. Nutrients 2021, 13, 2899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082899
Steell L, Gray SR, Russell RK, MacDonald J, Seenan JP, Wong SC, Gaya DR. Pathogenesis of Musculoskeletal Deficits in Children and Adults with Inflammatory Bowel Disease. Nutrients. 2021; 13(8):2899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082899
Chicago/Turabian StyleSteell, Lewis, Stuart R. Gray, Richard K. Russell, Jonathan MacDonald, John Paul Seenan, Sze Choong Wong, and Daniel R. Gaya. 2021. "Pathogenesis of Musculoskeletal Deficits in Children and Adults with Inflammatory Bowel Disease" Nutrients 13, no. 8: 2899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082899