
Development of Visceral and Subcutaneous-Abdominal Adipose Tissue in Breastfed Infants during First Year of Lactation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Design
2.2. Measurements of Infant Abdominal Adiposity
2.3. Measurements of Maternal Body Composition
2.4. Measurements of Human Milk Components
2.5. Statistical Analyses
3. Results
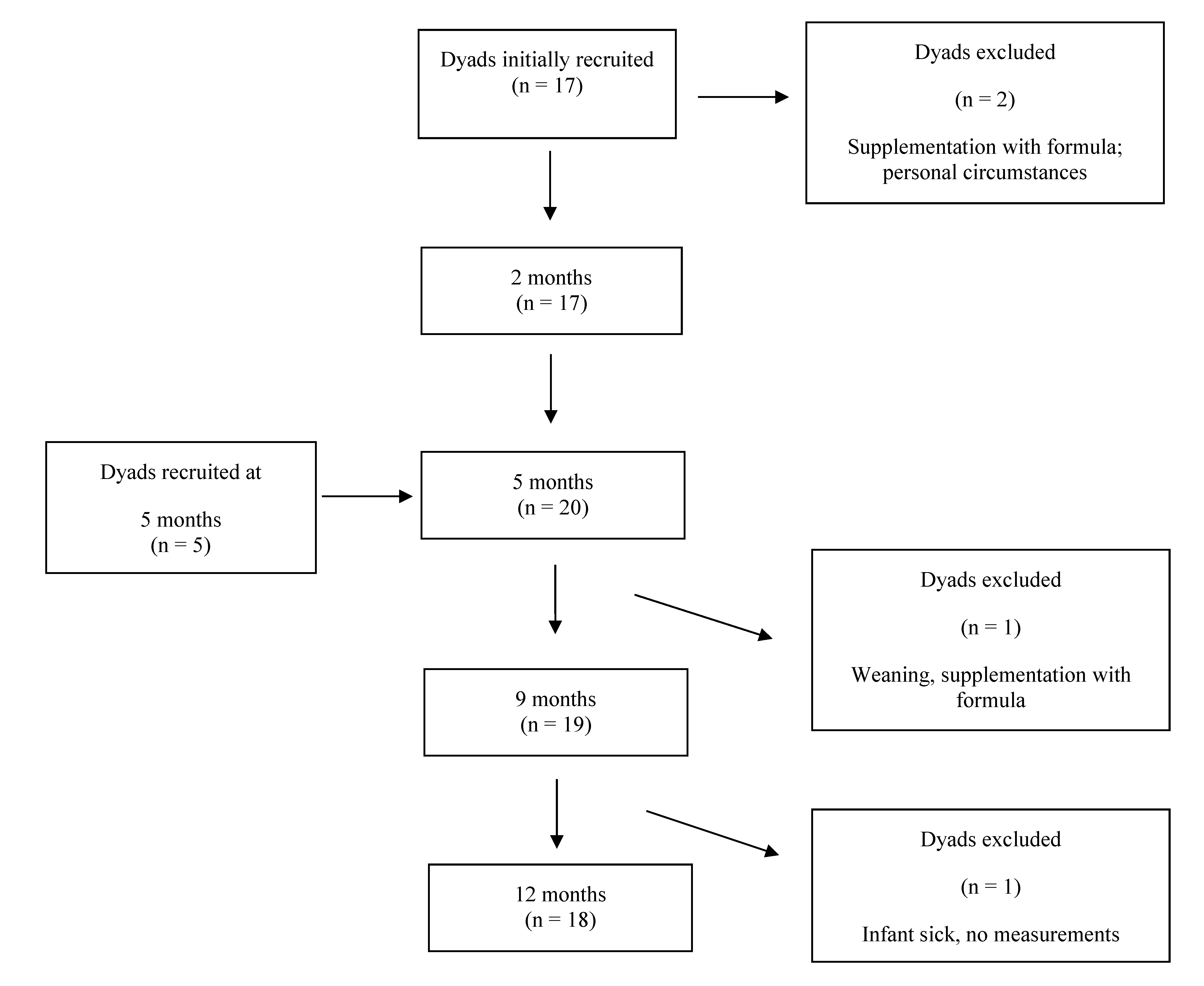
3.1. Subjects
3.2. Longitudinal Changes in Infant Abdominal Adiposity
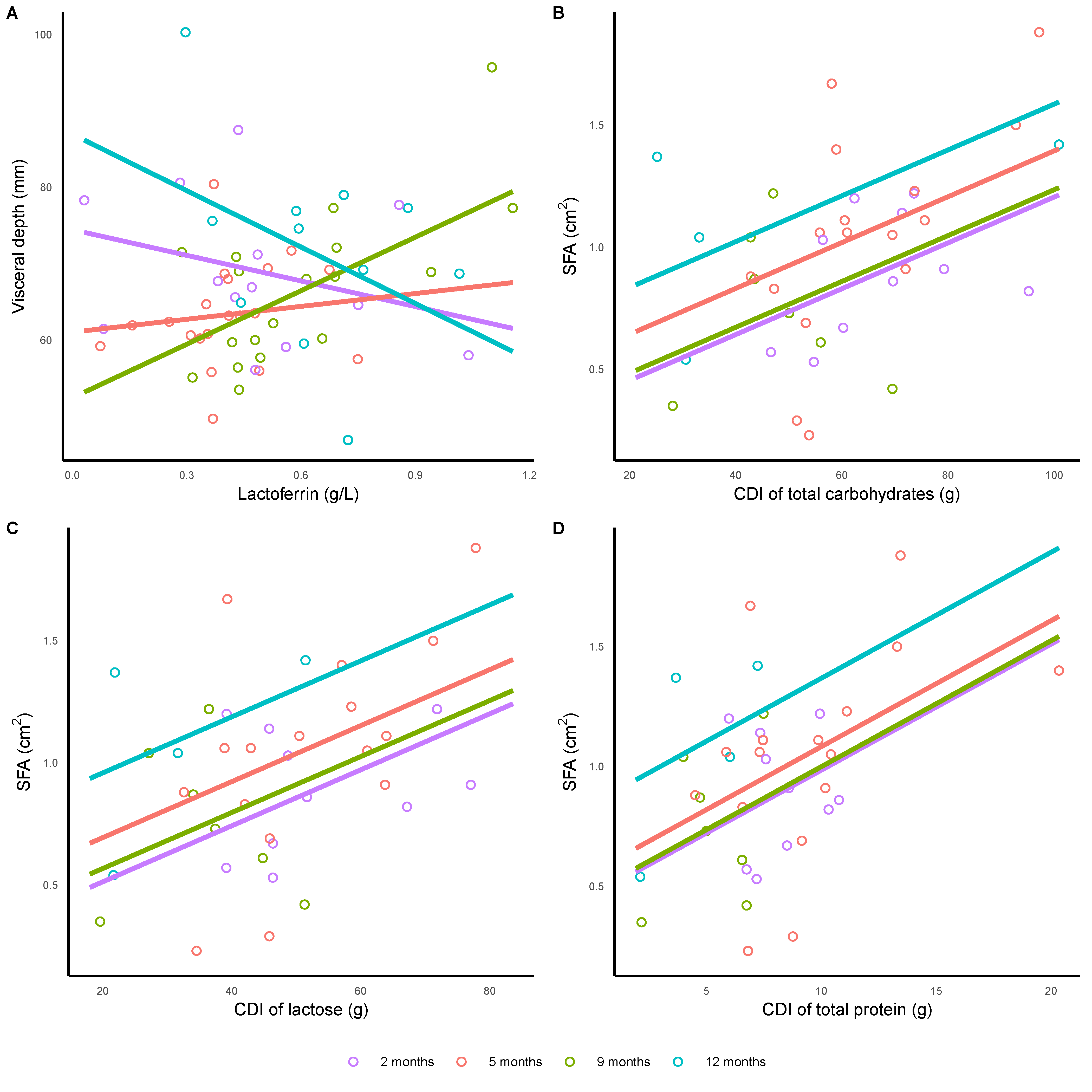
3.3. Human Milk Components and Infant Abdominal Adiposity
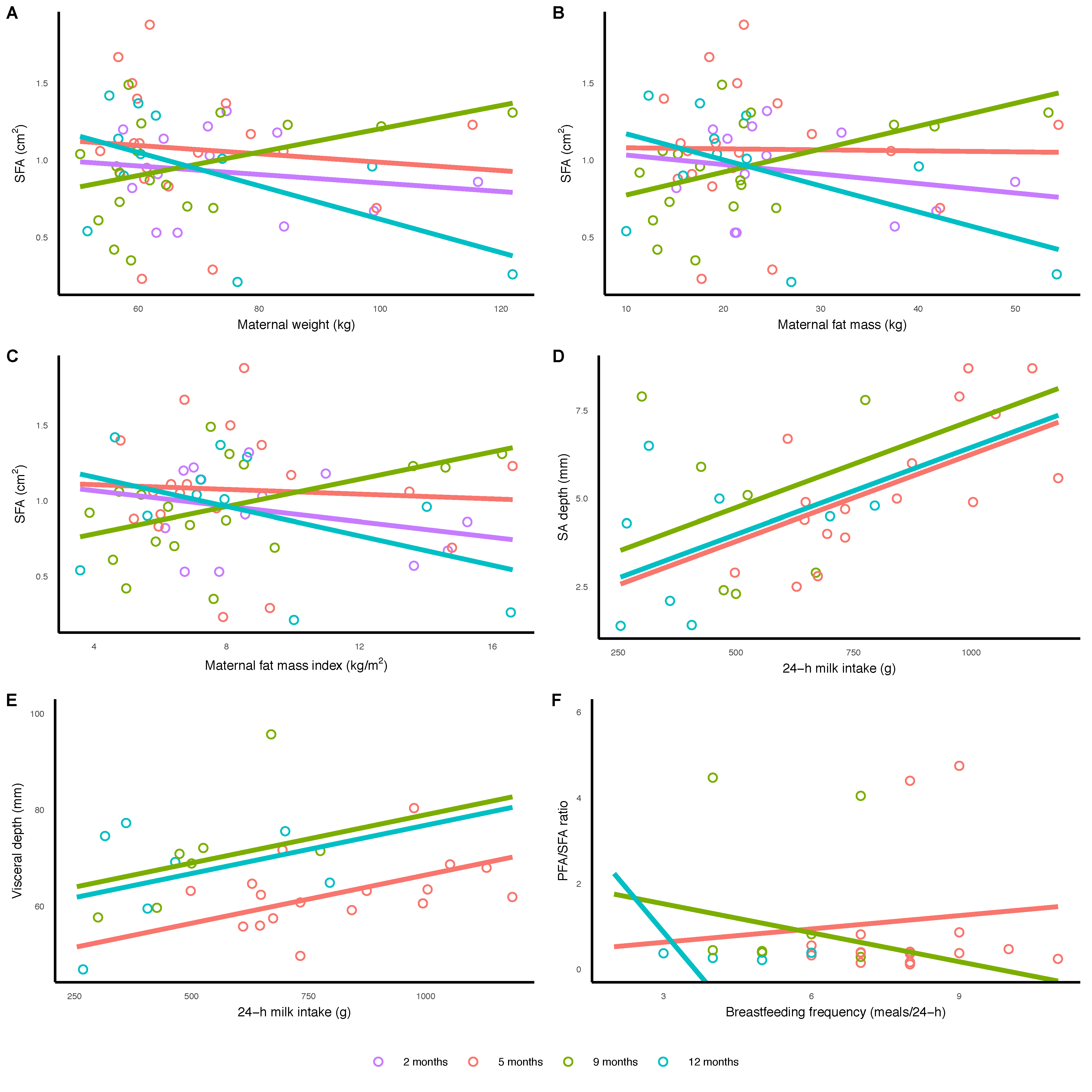
3.4. Breastfeeding Parameters and Infant Abdominal Adiposity
3.5. Maternal Body Composition and Infant Abdominal Adiposity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Després, J.-P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Hamdy, O.; Porramatikul, S.; Al-Ozairi, E. Metabolic obesity: The paradox between visceral and subcutaneous fat. Cur. Diabetes Rev. 2006, 2, 367–373. [Google Scholar]
- Golan, R.; Shelef, I.; Rudich, A.; Gepner, Y.; Shemesh, E.; Chassidim, Y.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Ben Avraham, S.; et al. Abdominal superficial subcutaneous fat: A putative distinct protective fat subdepot in type 2 diabetes. Diabetes Care 2012, 35, 640–647. [Google Scholar] [CrossRef] [Green Version]
- Leunissen, R.W.; Kerkhof, G.F.; Stijnen, T.; Hok-ken-Koelega, A. Timing and tempo of first- year rapid growth in relation to cardiovascular and metabolic risk profile in early adulthood. JAMA 2009, 301, 2234–2242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, A.P.; da Silva Junior, J.R.; Figueiroa, J.N.; Alves, J.G. Abdominal subcutaneous and visceral fat thickness in newborns: Correlation with anthropometric and metabolic profile. J. Perinatol. 2014, 34, 932–935. [Google Scholar] [CrossRef] [PubMed]
- Goran, M.I.; Gower, B.A. Relation between visceral fat and disease risk in children and adolescents. Am. J. Clin. Nutr. 1999, 70, 149S–156S. [Google Scholar] [CrossRef] [PubMed]
- Gesta, S.; Tseng, Y.H.; Kahn, C.R. Developmental origin of fat: Tracking obesity to its source. Cell 2007, 131, 242–256. [Google Scholar] [CrossRef] [Green Version]
- Gishti, O.; Gaillard, R.; Durmus, B.; Abrahamse, M.; van der Beek, E.M.; Hofman, A.; Franco, O.H.; de Jonge, L.L.; Jaddoe, V.W. BMI, total and abdominal fat distribution, and cardiovascular risk factors in school-age children. Pediatr. Res. 2015, 77, 710–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.H.; Chan, Y.L.; Chan, W.B.; Kong, W.L.; Kong, M.O.; Chan, J.C. Sonographic measurement of mesenteric fat thickness is a good correlate with cardiovascular risk factors: Comparison with subcutaneous and preperitoneal fat thickness, magnetic resonance imaging and anthropometric indexes. Int. J. Obes. 2003, 27, 1267–1273. [Google Scholar] [CrossRef] [Green Version]
- Butte, N.; Wong, W.; Hopkinson, J.; Smith, E.; Ellis, K. Infant feeding mode affects early growth and body composition. Pediatrics 2000, 16, 1355–1366. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.G.; Martin, J.M. Does breastfeeding protect against childhood obesity? Moving beyond observational evidence. Curr. Obes. Rep. 2015, 4, 207–216. [Google Scholar] [CrossRef]
- De Lucia Rolfe, E.; Modi, N.; Uthaya, S.; Hughes, I.A.; Dunger, D.B.; Acerini, C.; Stolk, R.P.; Ong, K.K. Ultrasound estimates of visceral and subcutaneous-abdominal adipose tissues in infancy. J. Obes. 2013, 2013, 951954. [Google Scholar] [CrossRef]
- Barros, V.O.; Amorim, M.R.; Melo, A.O.; Tavares, J.S.; Silva, A.C.; Alves, J.G. Abdominal fat distribution among breastfed and formula-fed infants. Breastfeed. Med. 2016, 11, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Breij, L.M.; Abrahamse-Berkeveld, M.; Acton, D.; De Lucia Rolfe, E.; Ong, K.K.; Hokken-Koelega, A.C.S. Impact of early infant growth, duration of breastfeeding and maternal factors on total body fat mass and visceral fat at 3 and 6 months of age. Ann. Nutr. Metab. 2017, 71, 203–210. [Google Scholar] [CrossRef]
- de Fluiter, K.; Kerkhof, G.F.; van Beijsterveldt, I.; Breij, L.M.; de Heijning, B.; Abrahamse-Berkeveld, M.; Hokken-Koelega, A. Longitudinal human milk macronutrients, body composition and infant appetite during early life. Clin. Nutr. 2020, 40, 3401–3408. [Google Scholar] [CrossRef] [PubMed]
- Arthur, P.; Hartmann, P.; Smith, M. Measurement of the milk intake of breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 1987, 6, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A.; Hartmann, P.E. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, e387–e395. [Google Scholar] [CrossRef] [Green Version]
- Holzhauer, S.; Zwijsen, M.L.; Jaddoe, V.W.V.; Boehm, G.; Moll, H.A.; Mulder, P.G.; Kleyburg-Linkers, V.A.; Hofman, A.; Witteman, J.C.M. Sonographic assessment of abdominal fat distribution in infancy. Eur. J. Epidemiol. 2009, 24, 521–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mook-Kanamori, D.O.; Holzhauer, S.; Hollestein, L.M.; Durmus, B.; Manniesing, R.; Koek, M.; Boehm, G.; van der Beek, E.M.; Hofman, A.; Witteman, J.C.; et al. Abdominal fat in children measured by ultrasound and computed tomography. Ultrasound Med. Biol. 2009, 35, 1938–1946. [Google Scholar] [CrossRef]
- Suzuki, R.; Watanabe, S.; Hirai, Y.; Akiyama, K.; Nishide, T.; Matsushima, Y.; Murayama, H.; Ohshima, H.; Shinomiya, M.; Shirai, K.; et al. Abdominal wall fat index, estimated by ultrasonography, for assessment of the ratio of visceral fat to subcutaneous fat in the abdomen. Am. J. Med. 1993, 95, 309–314. [Google Scholar] [CrossRef]
- McLeod, G.; Geddes, D.; Nathan, E.; Sherriff, J.; Simmer, K.; Hartmann, P. Feasibility of using ultrasound to measure preterm body composition and to assess macronutrient influences on tissue accretion rates. Early Hum. Dev. 2013, 89, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Rea, A.; Hepworth, A.R.; Ward, L.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Relationships between breastfeeding patterns and maternal and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Kugananthan, S.; Gridneva, Z.; Lai, C.T.; Hepworth, A.R.; Mark, P.J.; Kakulas, F.; Geddes, D.T. Associations between maternal body composition and appetite hormones and macronutrients in human milk. Nutrients 2017, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Van Itallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [Green Version]
- Kugananthan, S.; Lai, C.T.; Gridneva, Z.; Mark, P.J.; Geddes, D.T.; Kakulas, F. Leptin levels are higher in whole compared to skim human milk, supporting a cellular contribution. Nutrients 2016, 8, 711. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Kugananthan, S.; Rea, A.; Lai, C.T.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk adiponectin and leptin and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridneva, Z.; Tie, W.J.; Rea, A.; Lai, C.T.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk casein and whey protein and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridneva, Z.; Rea, A.; Tie, W.J.; Lai, C.T.; Kugananthan, S.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Carbohydrates in human milk and body composition of term infants during the first 12 months of lactation. Nutrients 2019, 11, 1472. [Google Scholar] [CrossRef] [Green Version]
- Gridneva, Z.; Lai, C.T.; Rea, A.; Tie, W.J.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk immunomodulatory proteins are related to development of infant body composition during the first year of lactation. Pediatr. Res. 2020, 89, 911–921. [Google Scholar] [CrossRef]
- Keller, R.; Neville, M. Determination of total protein in human milk: Comparison of methods. Clin. Chem. 1986, 32, 120–123. [Google Scholar] [CrossRef]
- Kunz, C.; Lonnerdal, B. Human milk proteins: Separation of whey proteins and their analysis by polyacrylamide gel electrophoresis, fast protein liquid chromatography (FPLC) gel filtration, and anion-exchange chromatography. Am. J. Clin. Nutr. 1989, 49, 464–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Casadio, Y.; Lai, C.; Prime, D.; Hepworth, A.; Trengove, N.; Hartmann, P. Investigation of short-term variations in casein and whey proteins in breast milk of term mothers. Hepat. Nutr. 2012, 55, 136–141. [Google Scholar] [CrossRef]
- Mitoulas, L.R.; Kent, J.C.; Cox, D.B.; Owens, R.A.; Sherriff, J.L.; Hartmann, P.E. Variation in fat, lactose and protein in human milk over 24 h and throughout the first year of lactation. Br J. Nutr. 2002, 88, 29–37. [Google Scholar] [CrossRef]
- Euber, J.; Brunner, J. Determination of lactose in milk products by high-performance liquid chromatography. J. Dairy Sci. 1979, 62, 685–690. [Google Scholar] [CrossRef]
- Albalasmeh, A.; Berhe, A.; Ghezzehei, T. A new method for rapid determination of carbohydrate and total carbon concentrations using UV spectrophotometry. Carbohydr. Polym. 2013, 97, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Selsted, M.; Martinez, R. A simple and ultrasensitive enzymatic assay for the quantitative determination of lysozyme in the picogram range. Anal. Biochem. 1980, 109, 67–70. [Google Scholar] [CrossRef]
- Zhang, G.; Lai, C.T.; Hartmann, P.; Oddy, W.H.; Kusel, M.M.H.; Sly, P.D.; Holt, P.G. Anti-infective proteins in breast milk and asthma-associated phenotypes during early childhood. Pediatr. Allergy Immunol. 2014, 25, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Tijssen, P. Practice and theory of immunoessays. In Laboratory Techniques in Biochemistry and Molecular Biology; Burdon, R.H., van Knippenberg, P.H., Eds.; Elsevier: New York, NY, USA, 1985. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Diggle, P.J.; Heagerty, P.J.; Liang, K.-Y.; Zeger, S.L. Analysis of Longitudinal Data; Oxford University Press Inc.: New York, NY, USA, 2002. [Google Scholar]
- Curran-Everett, D. Multiple comparisons: Philosophies and illustrations. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R1–R8. [Google Scholar] [CrossRef]
- Carberry, A.; Golditz, P.; Lingwood, B. Body composition from birth to 4.5 months in infants born to non-obese women. Pediatr. Res. 2010, 68, 84–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Cano, A.M.; Mier-Cabrera, J.; Allegre-Dávalos, A.L.; Muñoz-Manrique, C.; Perichart-Perera, O. Higher fat mass and fat mass accretion during the first six months of life in exclusively breastfed infants. Pediatr. Res. 2019, 87, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Magnuson, A.; Foster, M. Detrimental and protective fat: Body fat distribution and its relation to metabolic disease. Horm. Mol. Biol. Clin. Investig. 2014, 17, 13–27. [Google Scholar] [CrossRef]
- Hernell, O.; Lonnerdal, B. Iron status of infants fed low-iron formula: No effect of added bovine lactoferrin or nucleotides. Am. J. Clin. Nutr. 2002, 76, 858–864. [Google Scholar] [CrossRef]
- Johnston, W.H.; Ashley, C.; Yeiser, M.; Harris, C.L.; Stolz, S.I.; Wampler, J.L.; Wittke, A.; Cooper, T.R. Growth and tolerance of formula with lactoferrin in infants through one year of age: Double-blind, randomized, controlled trial. BMC Pediatr. 2015, 15, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.C.; Cummings, G.E.; Guo, N.; Triverdi, L.; Readmond, B.X.; Keane, V.; Feigelman, S.; de Waard, R. A double-blind, placebo-controlled, pilot study of bovine lactoferrin supplementation in bottle-fed infants. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.N.; Li, Y.; Sangild, P.T.; Bering, S.B.; Chatterton, D.E.W. Effects of bovine lactoferrin on the immature porcine intestine. Br. J. Nutr. 2014, 111, 321–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, W.V.; Eriksson, J.G.; Broekman, B.F.P. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Fields, D.A.; Schneider, C.R.; Pavela, G. A narrative review of the associations between six bioactive components in breast milk and infant adiposity. Obesity 2016, 24, 1213–1221. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2 Months | 5 Months | 9 Months | 12 Months |
|---|---|---|---|---|
| Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | |
| Mothers | (n = 14) | (n = 20) | (n = 18) | (n = 18) |
| Weight (kg) | 78.8 ± 19.3 a | 70.1 ± 17.8 | 63.0 ± 10.0 | 64.2 ± 17.3 |
| (57.5–116.2) | (53.7–115.3) | (50.4–121.9) | (51.4–121.9) | |
| BMI (kg/m2) | 27.2 ± 5.5 | 24.8 ± 5.0 | 22.7 ± 3.9 | 23.9 ± 5.9 |
| (20.4–35.5) | (19.0–35.2) | (17.9–37.2) | (18.2–37.2) | |
| Infants | (n = 15) | (n = 20) | (n = 19) | (n = 18) |
| Sex (M/F) | 9 M/6 F | 10 M/10 F | 10 M/9 F | 9 M/9 F |
| Age (months) | 2.04 ± 0.14 | 5.16 ± 0.22 | 9.22 ± 0.27 | 12.26 ± 0.28 |
| (1.87–2.33) | (4.77–5.47) | (8.83–9.77) | (11.63–12.67) | |
| Length (cm) | 58.1 ± 1.9 | 64.8 ± 2.3 | 71.7 ± 1.9 | 73.6 ± 3.2 |
| (54.2–60.0) | (60.5–69.5) | (66.0–74.0) | (69.0–78.5) | |
| Weight (kg) | 5.63 ± 0.66 | 7.431 ± 1.134 | 8.836 ± 0.975 | 9.650 ± 0.618 |
| (4.420–7.400) | (5.808–9.510) | (6.675–10.095) | (7.165–11.085) | |
| BMI (kg/m2) | 16.6 ± 1.2 | 17.6 ± 1.9 | 17.7 ± 1.7 | 17.8 ± 0.9 |
| (14.5–18.1) | (14.9–20.4) | (14.2–20.2) | (13.7–19.2) | |
| VD (mm) | 68.8 ± 9.7 | 63.3 ± 6.7 | 66.9 ± 10.3 | 71.3 ± 12.3 |
| (56.1–87.5) | (49.7–80.4) | (53.5–95.7) | (46.9–100.3) | |
| SAD (mm) | 4.0 ± 1.8 | 5.3 ± 1.8 ** | 4.6 ± 2.1 | 3.7 ± 1.9 ** |
| (1.5–7.2) | (2.5–8.7) | (2.1–8.4) | (1.4–8.5) | |
| VD/SAD ratio | 22.0 ± 14.2 * | 13.0 ± 5.0 *,** | 18.0 ± 8.8 | 22.6 ± 11.5 ** |
| (8.6–58.3) | (7.0–25.9) | (7.1–33.0) | (9.1–42.2) | |
| SFA (cm2) | 0.9 ± 0.3 | 1.1 ± 0.4 | 0.9 ± 0.3 | 0.9 ± 0.4 |
| (0.5–1.3) | (0.2–1.9) | (0.4–1.5) | (0.2–1.4) | |
| PFA (cm2) | 0.3 ± 0.1 | 0.5 ± 0.3 | 0.5 ± 0.5 | 0.4 ± 0.1 |
| (0.2–0.4) | (0.2–1.3) | (0.3–1.8) | (0.2–0.7) | |
| SFA/PFA ratio | 0.3 ± 0.1 | 0.8 ± 1.3 | 0.9 ± 1.4 | 0.6 ± 0.7 |
| (0.1–0.5) | (0.2–4.8) | (0.2–5.1) | (0.2–2.7) | |
| Age (months) | 2.04 ± 0.14 | 5.16 ± 0.22 | 9.22 ± 0.27 | 12.26 ± 0.28 |
| (1.87–2.33) | (4.77–5.47) | (8.83–9.77) | (11.63–12.67) | |
| Breastfeeding characteristics | ||||
| 24-h milk intake (g) | n/a b | (n = 17) | (n = 8) | (n = 8) |
| 818.8 ± 204.9 | 478.3 ± 154.0 | 451.1 ± 215.7 | ||
| (498–1185) | (300–775) | (255–795) | ||
| 24-h feeding frequency (24-h MP) | n/a b | (n = 17) | (n = 8) | (n = 9) |
| 8.1 ± 1.4 | 5.4 ± 1.3 | 4.4 ± 2.1 | ||
| (6–11) | (4–7) | (2–8) | ||
| Feeding frequency (SR) c | (n = 11) | (n = 19) | (n = 17) | (n = 13) |
| 2.3 ± 0.4 | 2.8 ± 0.8 | 3.7 ± 1.2 | 5.4 ± 2.9 | |
| (1.5–3.0) | (1.5–4.0) | (2.0–6.0) | (2.2–12.0) | |
| Predictor | 2 Months | 5 Months | 9 Months | 12 Months | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Concentrations | (n = 14) | (n = 20) | (n = 17) | (n = 13) | (n = 20) | ||||||
| Subcutaneous-abdominal depth (mm), significance at <0.041 d | |||||||||||
| Adiponectin, g/L | 5.3 (1.14) | −0.102 (0.098) a | 3.19 (1.14) | 0.221 (0.112) | 5.43 (2.26) | −0.106 (0.254) | 5.58 (1.33) | −0.17 (0.112) | 0.64 | 0.038 | 0.041 b |
| Visceral depth (mm), significance at <0.019 | |||||||||||
| Lactoferrin, g/L | 74.5 (4.93) | −11.2 (8.85) | 61.0 (5.55) | 5.61 (12.8) | 52.4 (5.49) | 23.4 (8.44) | 86.9 (8.47) | −24.6 (12.7) | 0.70 | 0.084 | 0.003 |
| Lysozyme, g/L | 73.3 (3.06) | −32.5 (14.1) | 65.9 (2.65) | −32.5 (14.1) | 71.2 (2.96) | −32.5 (14.1) | 77.6 (4.03) | −32.5 (14.1) | 0.019 c | 0.007 | 0.67 |
| Visceral/subcutaneous-abdominal depths ratio, significance at <0.006 | |||||||||||
| Total protein, g/L | −16.2 (16.8) | 3.55 (1.6) | 12.7 (6.61) | 0.063 (0.554) | 5.6 (11.4) | 1.17 (1.08) | 48.9 (11.5) | −2.58 (1.07) | 0.93 | 0.003 | 0.006 |
| Preperitoneal fat area (cm2), significance at <0.013 | |||||||||||
| Total protein, g/L | 0.539 (0.622) | −0.024 (0.057) | 0.317 (0.254) | 0.016 (0.021) | 1.96 (0.441) | −0.137 (0.042) | 0.43 (0.397) | −0.008 (0.034) | 0.40 | 0.059 | 0.013 |
| sIgA, g/L | 0.378 (0.248) | −0.164 (0.426) | 0.462 (0.21) | 0.088 (0.388) | 1.25 (0.22) | −1.17 (0.341) | 0.38 (0.34) | −0.062 (0.50) | 0.038 | 0.045 | 0.049 |
| Calculated daily intakes | (n = 12) | (n = 17) | (n = 8) | (n = 8) | (n = 17) | ||||||
| Subcutaneous-abdominal depth (mm), significance at <0.005 | |||||||||||
| Adiponectin, g | 4.59 (1.12) | −0.00005 (0.0001) | 2.69 (0.97) | 0.0003 (0.0001) | 6.3 (2.06) | −0.0003 (0.0004) | 4.05 (2.08) | −0.0001 (0.0005) | 0.094 | 0.079 | 0.027 |
| Casein, g | 2.66 (0.845) | 1.34 (0.555) | 3.43 (0.928) | 1.34 (0.555) | 3.98 (0.794) | 1.34 (0.555) | 2.86 (0.744) | 1.34 (0.555) | 0.021 | 0.45 | 0.91 |
| Lactose, g | 1.18 (1.38) | 0.054 (0.023) | 2.46 (1.35) | 0.054 (0.023) | 2.9 (1.1) | 0.054 (0.023) | 2.02 (0.976) | 0.054 (0.023) | 0.021 | 0.17 | 0.27 |
| sIgA, g | 4.97 (1.33) | −2.82 (3.34) | 4.2 (1.04) | 2.97 (2.39) | 9.09 (1.76) | −15.1 (5.78) | 4.36 (2.33) | −2.36 (8.51) | 0.70 | 0.11 | 0.029 |
| Total carbohydrates, g | 0.524 (1.32) | 0.047 (0.018) | 2.27 (1.24) | 0.047 (0.018) | 2.59 (1.08) | 0.047 (0.018) | 1.67 (1.0) | 0.047 (0.018) | 0.005 | 0.042 | 0.16 |
| Subcutaneous-abdominal fat area (cm2), significance at <0.027 | |||||||||||
| Casein, g | 0.632 (0.161) | 0.235 (0.103) | 0.713 (0.175) | 0.235 (0.103) | 0.608 (0.148) | 0.235 (0.103) | 0.951 (0.188) | 0.235 (0.103) | 0.027 | 0.45 | 0.79 |
| Lactose, g | 0.283 (0.269) | 0.012 (0.005) | 0.464 (0.253) | 0.012 (0.005) | 0.338 (0.211) | 0.012 (0.005) | 0.729 (0.226) | 0.012 (0.005) | 0.013 | 0.16 | 0.36 |
| sIgA, g | 0.604 (0.186) | 0.742 (0.379) | 0.757 (0.177) | 0.742 (0.379) | 0.551 (0.173) | 0.742 (0.379) | 0.921 (0.206) | 0.742 (0.379) | 0.042 | 0.20 | 0.44 |
| Total carbohydrates, g | 0.266 (0.251) | 0.009 (0.003) | 0.455 (0.233) | 0.009 (0.003) | 0.296 (0.473) | 0.009 (0.003) | 0.647 (0.234) | 0.009 (0.003) | 0.004 | 0.18 | 0.20 |
| Total protein, g | 0.459 (0.203) | 0.053 (0.021) | 0.557 (0.214) | 0.053 (0.021) | 0.473 (0.169) | 0.053 (0.021) | 0.842 (0.198) | 0.053 (0.021) | 0.013 | 0.31 | 0.81 |
| Preperitoneal/subcutaneous-abdominal fat areas ratio, significance at <0.028 | |||||||||||
| Lactoferrin, g | 1.44 (0.828) | −2.52 (2.28) | 0.057 (0.813) | 2.92 (2.38) | 2.23 (0.757) | −2.36 (1.88) | −4.91 (2.24) | 14.2 (7.28) | 0.52 | 0.001 | 0.028 |
| Predictor | 2 Months | 5 Months | 9 Months | 12 Months | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Breastfeeding parameters | (n = 17) | (n = 7) | (n = 8) | (n = 17) | |||||||
| Subcutaneous-abdominal depth (mm), significance at <0.005 d | |||||||||||
| 24-h milk intake, g e | n/a e | 1.32 (1.56) | 0.005 (0.002) a | 2.27 (1.18) | 0.005 (0.002) | 1.51 (1.04) | 0.005 (0.002) | 0.007b | 0.57 | 0.30 | |
| Subcutaneous-abdominal fat area (cm2), significance at <0.022 | |||||||||||
| 24-h milk intake, g | n/a | 0.295 (0.347) | 0.001 (0.0004) | 0.252 (0.262) | 0.001 (0.0004) | 0.641 (0.277) | 0.001 (0.0004) | 0.022 | 0.24 | 0.31 | |
| Visceral depth (mm), significance at < 0.05 | |||||||||||
| 24-h milk intake, g | n/a | 46.50 (7.35) | 0.02 (0.009) | 59.00 (5.33) | 0.02 (0.009) | 56.8 (5.12) | 0.02 (0.009) | 0.013 | 0.007 | 0.068 | |
| Preperitoneal fat area (cm2), significance at <0.047 | |||||||||||
| Breastfeeding Frequency e | n/a | 096 (0.491) | −0.046 (0.059) | 1.06 (0.346) | −0.046 (0.059) | 0.23 (0.31) | −0.046 (0.059) | 0.047 | <0.001 | 0.082 | |
| Preperitoneal/subcutaneous-abdominal fat areas ratio, significance at <0.05 | |||||||||||
| Breastfeeding frequency | n/a | 0.37 (2.1) | 0.097 (0.257) | 2.85 (1.54) | −0.305 (0.276) | 4.81 (1.72) | −1.34 (0.372) | 0.19 | <0.001 | 0.002c | |
| Maternal body composition | (n = 14) | (n = 20) | (n = 18) | (n = 17) | (n = 20) | ||||||
| Subcutaneous-abdominal fat area (cm2), significance at <0.048 | |||||||||||
| Fat mass, kg | 1.10 (0.276) | −0.006 (0.01) | 1.09 (2.03) | −0.0007 (0.008) | 0.625 (0.189) | 0.015 (0.008) | 1.34 (0.221) | −0.017 (0.008) | 0.91 | 0.46 | 0.010 |
| Fat mass, % | 1.42 (0.644) | −0.014 (0.018) | 0.839 (0.443) | 0.007 (0.013) | 0.087 (0.393) | 0.027 (0.012) | 1.62 (0.474) | −0.021 (0.015) | 0.57 | 0.49 | 0.019 |
| Weight, kg | 1.13 (0.447) | −0.003 (0.006) | 1.26 (0.366) | −0.003 (0.005) | 0.446 (0.325) | 0.008 (0.005) | 1.70 (0.369) | −0.011 (0.005) | 0.66 | 0.49 | 0.020 |
| Fat mass index, kg/m2 | 1.17 (0.308) | −0.026 (0.031) | 1.14 (0.227) | −0.008 (0.025) | 0.599 (0.209) | 0.045 (0.024) | 1.35 (0.257) | −0.049 (0.028) | 0.88 | 0.48 | 0.023 |
| Fat-free mass, kg | 1.06 (0.657) | −0.003 (0.014) | 1.76 (0.60) | −0.015 (0.013) | 0.464 (0.489) | 0.011 (0.010) | 2.21 (0.569) | −0.027 (0.012) | 0.39 | 0.54 | 0.048 |
| Visceral depth (mm), significance at <0.045 | |||||||||||
| Fat mass, kg | 74.40 (7.47) | −0.201 (0.274) | 63.10 (5.45) | 0.009 (0.214) | 69.20 (5.19) | −0.127 (0.208) | 58.30 (5.65) | 0.512- (0.225) | 0.65 | 0.077 | 0.045 |
| Weight, kg | 76.60 (11.70) | −0.101 (0.157) | 62.40 (9.82) | 0.014 (0.14) | 68.90 (8.84) | −0.038 (0.127) | 48.30 (9.31) | 0.319 (0.132) | 0.48 | 0.081 | 0.049 |
| Preperitoneal/subcutaneous-abdominal fat areas ratio, significance at <0.022 | |||||||||||
| Fat mass, kg | 0.757 (0.853) | −0.012 (0.030) | 1.34 (0.639) | −0.020 (0.025) | 1.57 (0.595) | −0.032 (0.024) | −0.859 (0.685) | 0.053 (0.026) | 0.82 | 0.35 | 0.022 |
| Weight, kg | 0.88 (1.39) | −0.006 (0.018) | 1.49 (1.15) | −0.009 (0.016) | 1.95 (1.02) | −0.016 (0.015) | −1.81 (1.15) | 0.031 (0.016) | 0.99 | 0.37 | 0.042 |
| Fat mass, % | 1.42 (1.98) | −0.029 (0.056) | 2.23 (1.39) | −0.041 (0.041) | 2.85 (1.23) | −0.063 (0.038) | −2.06 (1.46) | 0.076 (0.045) | 0.54 | 0.35 | 0.045 |
| Fat-free mass index, kg/m2 | −2.25 (1.37) | 0.16 (0.081) | −1.72 (1.32) | 0.16 (0.081) | −1.72 (1.32) | 0.16 (0.081) | −2.20 (1.39) | 0.16 (0.081) | 0.046 | 0.29 | 0.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gridneva, Z.; Rea, A.; Lai, C.T.; Tie, W.J.; Kugananthan, S.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Development of Visceral and Subcutaneous-Abdominal Adipose Tissue in Breastfed Infants during First Year of Lactation. Nutrients 2021, 13, 3294. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093294
Gridneva Z, Rea A, Lai CT, Tie WJ, Kugananthan S, Murray K, Hartmann PE, Geddes DT. Development of Visceral and Subcutaneous-Abdominal Adipose Tissue in Breastfed Infants during First Year of Lactation. Nutrients. 2021; 13(9):3294. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093294
Chicago/Turabian StyleGridneva, Zoya, Alethea Rea, Ching Tat Lai, Wan Jun Tie, Sambavi Kugananthan, Kevin Murray, Peter E. Hartmann, and Donna T. Geddes. 2021. "Development of Visceral and Subcutaneous-Abdominal Adipose Tissue in Breastfed Infants during First Year of Lactation" Nutrients 13, no. 9: 3294. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093294