
Evaluation of a Novel Artificial Intelligence System to Monitor and Assess Energy and Macronutrient Intake in Hospitalised Older Patients

 and
and
Abstract
:1. Introduction
2. Materials and Methods
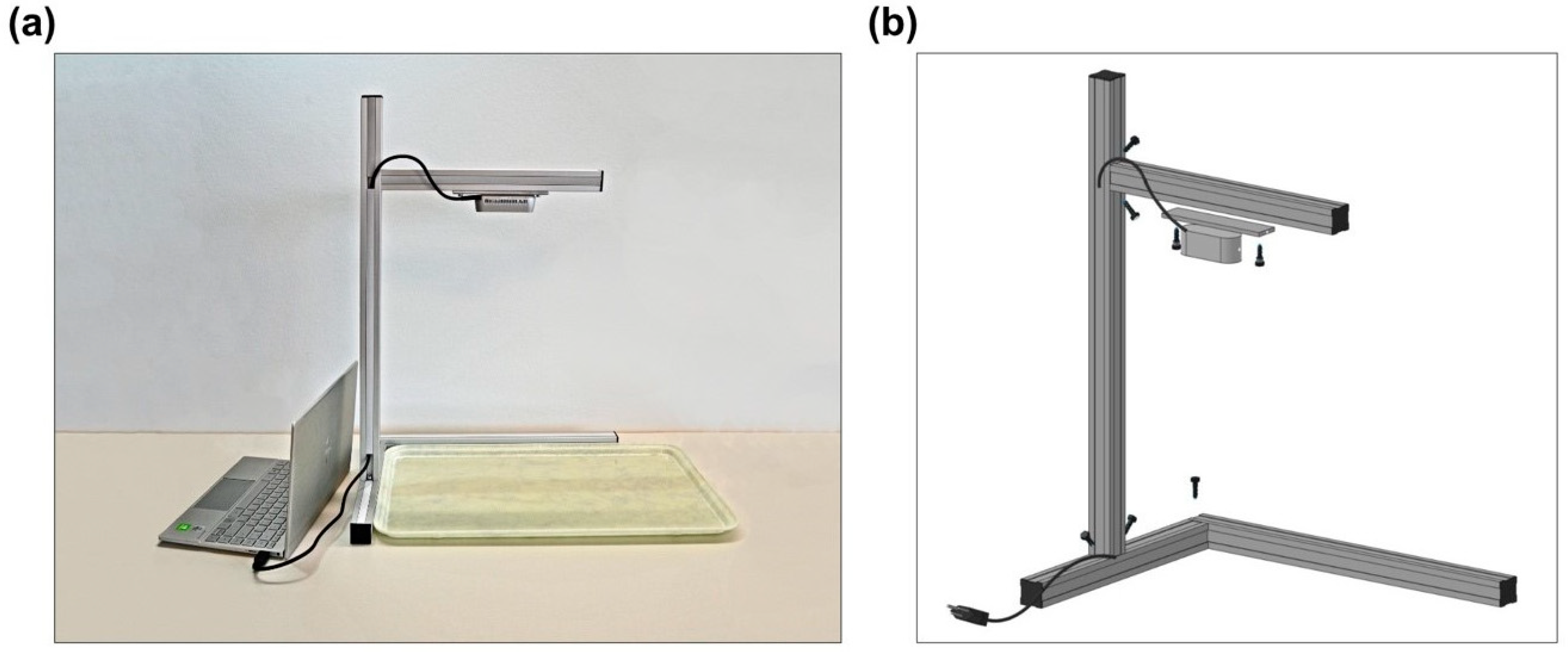
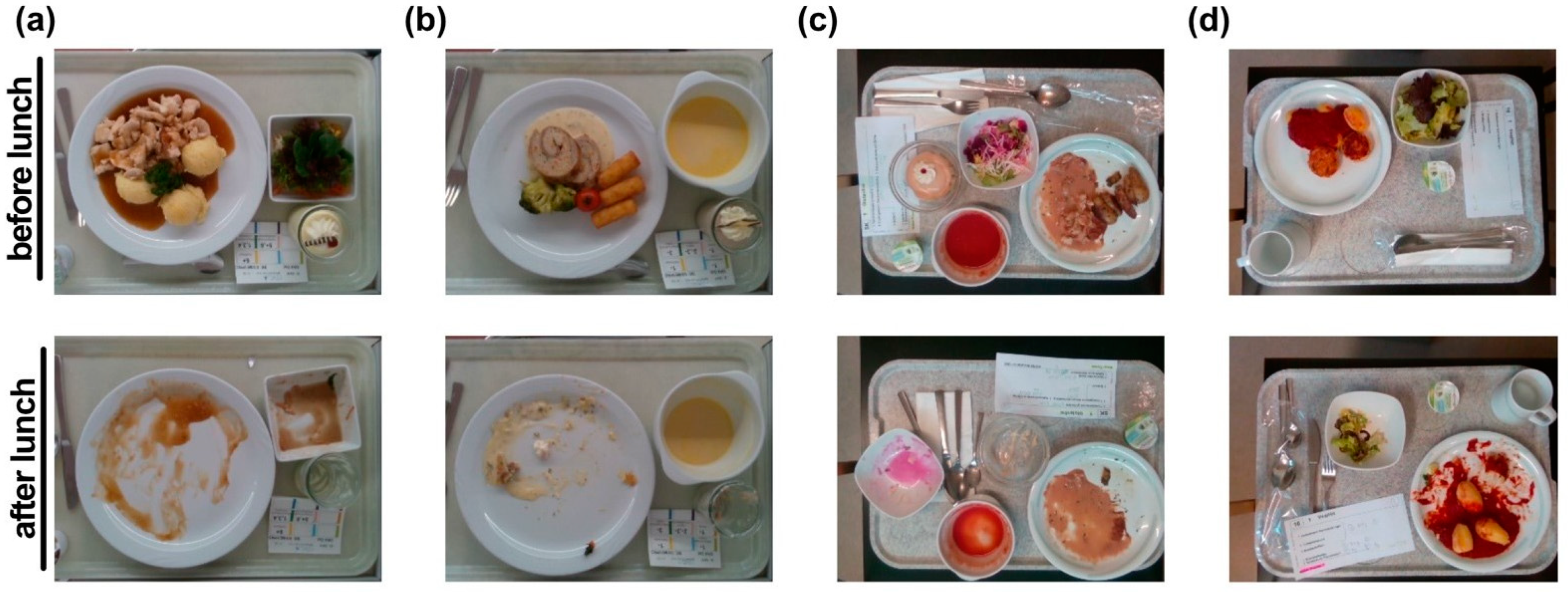
2.1. Data Collection
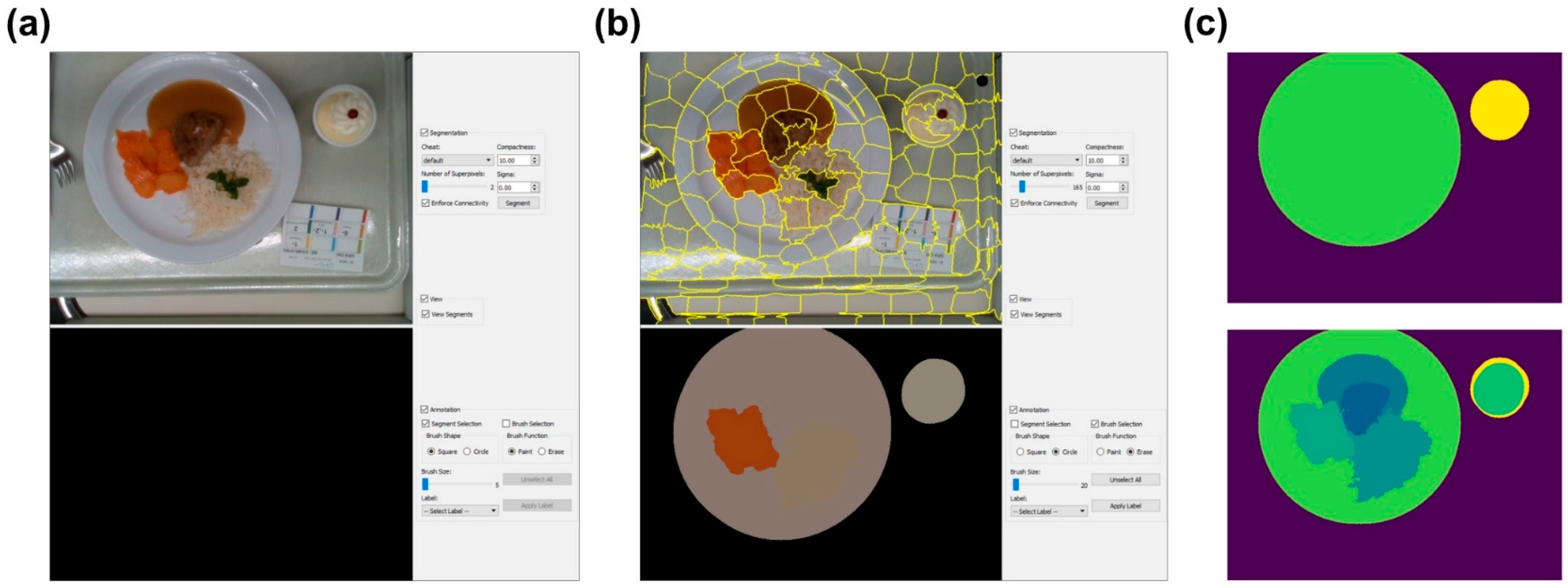
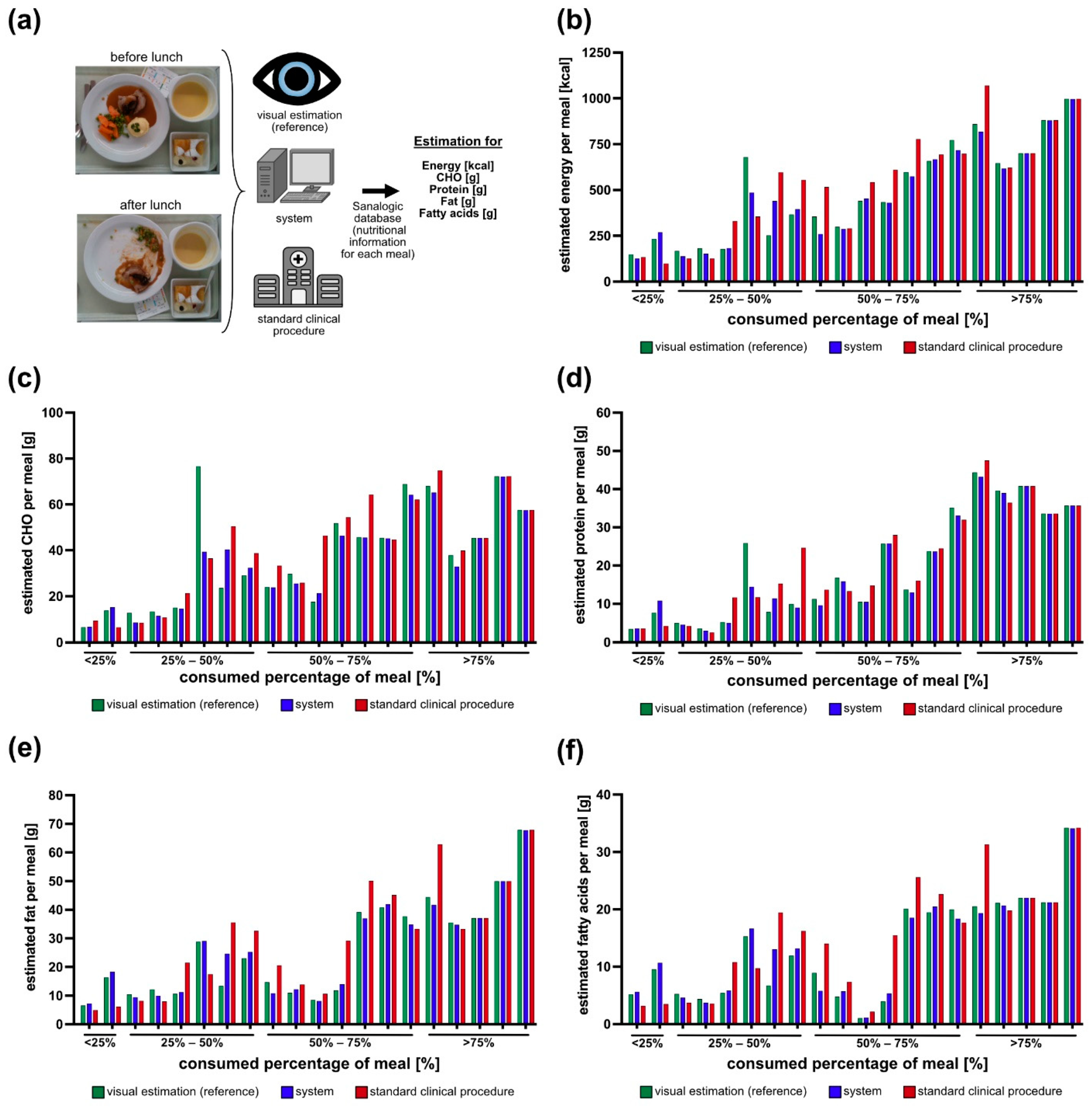
2.2. Dietary Meal Analysis
2.3. Food Segmentation Network
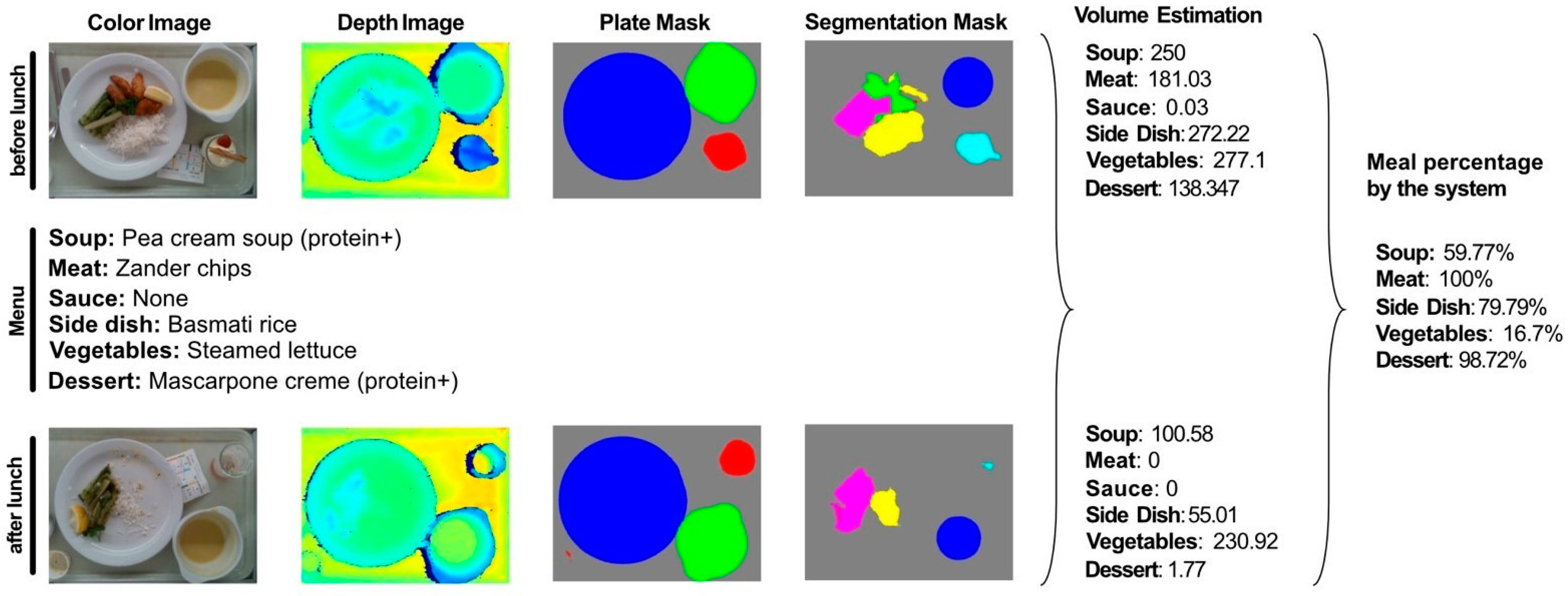
2.4. Automatic Volume and Macronutrient Estimation
3. Results
3.1. Food Segmentation
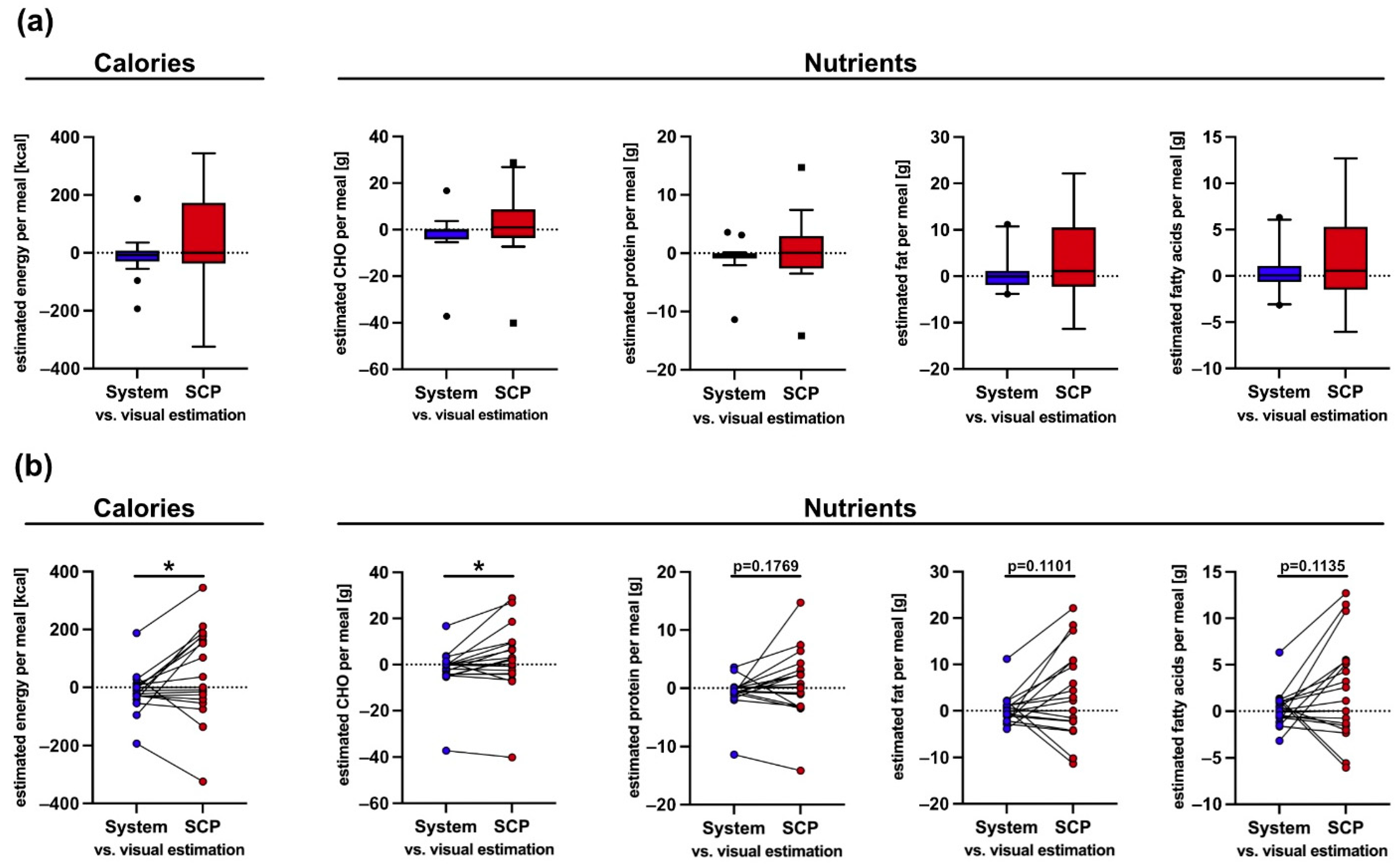
3.2. Macronutrient Estimation Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Pirlich, M.; Schütz, T.; Norman, K.; Gastell, S.; Lübke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Güldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef]
- Imoberdorf, R.; Rühlin, M.; Beerli, A.; Ballmer, P.E. Mangelernährung Unterernährung. Swiss Med. Forum 2011, 11, 782–786. [Google Scholar] [CrossRef]
- Imoberdorf, R.; Meier, R.; Krebs, P.; Hangartner, P.J.; Hess, B.; Stäubli, M.; Wegmann, D.; Rühlin, M.; Ballmer, P.E. Prevalence of undernutrition on admission to Swiss hospitals. Clin. Nutr. 2010, 29, 38–41. [Google Scholar] [CrossRef]
- Imoberdorf, R.; Rühlin, M.; Ballmer, P.E. Unterernährung im Krankenhaus-Häufigkeit, Auswirkungen und Erfassungsmöglichkeiten. Klinikarzt 2004, 33, 342–345. [Google Scholar] [CrossRef] [Green Version]
- Mühlethaler, R.; Stuck, A.E.; Minder, C.E.; Frey, B.M. The prognostic significance of protein-energy malnutrition in geriatric patients. Age Ageing 1995, 24, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlandoni, P.; Venturini, C.; Jukic Peladic, N.; Costantini, A.; Di Rosa, M.; Cola, C.; Giorgini, N.; Basile, R.; Fagnani, D.; Sparvoli, D.; et al. Malnutrition upon hospital admission in geriatric patients: Why assess it? Front. Nutr. 2017, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Mendes, A.; Serratrice, C.; Herrmann, F.R.; Gold, G.; Graf, C.E.; Zekry, D.; Genton, L. Nutritional risk at hospital admission is associated with prolonged length of hospital stay in old patients with COVID-19. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Gomes, F.; Schuetz, P.; Bounoure, L.; Austin, P.; Ballesteros-Pomar, M.; Cederholm, T.; Fletcher, J.; Laviano, A.; Norman, K.; Poulia, K.-A.; et al. ESPEN guidelines on nutritional support for polymorbid internal medicine patients. Clin. Nutr. 2018, 37, 336–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guenter, P.; Abdelhadi, R.; Anthony, P.; Blackmer, A.; Malone, A.; Mirtallo, J.M.; Phillips, W.; Resnick, H.E. Malnutrition diagnoses and associated outcomes in hospitalized patients: United States, 2018. Nutr. Clin. Pract. 2021, 36, 957–969. [Google Scholar] [CrossRef]
- Schuetz, P.; Seres, D.; Lobo, D.N.; Gomes, F.; Kaegi-Braun, N.; Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet 2021, 398, 1927–1938. [Google Scholar] [CrossRef]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R. Readmission and mortality in malnourished, older, hospitalized adults treated with a specialized oral nutritional supplement: A randomized clinical trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Hoess, C.; Pavlicek, V.; et al. Design and rationale of the effect of early nutritional therapy on frailty, functional outcomes and recovery of malnourished medical inpatients trial (EFFORT): A pragmatic, multicenter, randomized-controlled trial. Int. J. Clin. Trials 2018, 5, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Merker, M.; Gomes, F.; Stanga, Z.; Schuetz, P. Evidence-based nutrition for the malnourished, hospitalised patient: One bite at a time. Swiss Med. Wkly. 2019, 149, w20112. [Google Scholar] [CrossRef]
- Monacelli, F.; Sartini, M.; Bassoli, V.; Becchetti, D.; Biagini, A.L.; Nencioni, A.; Cea, M.; Borghi, R.; Torre, F.; Odetti, P. Validation of the photography method for nutritional intake assessment in hospitalized elderly subjects. J. Nutr. Health Aging 2017, 21, 614–621. [Google Scholar] [CrossRef]
- Thibault, R.; Chikhi, M.; Clerc, A.; Darmon, P.; Chopard, P.; Genton, L.; Kossovsky, M.P.; Pichard, C. Assessment of food intake in hospitalised patients: A 10-year comparative study of a prospective hospital survey. Clin. Nutr. 2011, 30, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Rüfenacht, U.; Rühlin, M.; Imoberdorf, R.; Ballmer, P.E. Unser Tellerdiagramm–Ein einfaches Instrument zur Erfassung ungenügender Nahrungszufuhr bei unterernährten, hospitalisierten Patienten. Aktuel Ernahr. 2005, 30, 33. [Google Scholar] [CrossRef]
- Williamson, D.A.; Allen, H.R.; Martin, P.D.; Alfonso, A.J.; Gerald, B.; Hunt, A. Comparison of digital photography to weighed and visual estimation of portion sizes. J. Am. Diet. Assoc. 2003, 103, 1139–1145. [Google Scholar] [CrossRef]
- Sullivan, S.C.; Bopp, M.M.; Weaver, D.L.; Sullivan, D.H. Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients. Nutrients 2016, 8, 412. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.; Walton, K. Plate waste in hospitals and strategies for change. e-SPEN Eur. e-J. Clin. Nutr. Metab. 2011, 6, e235–e241. [Google Scholar] [CrossRef] [Green Version]
- Bjornsdottir, R.; Oskarsdottir, E.S.; Thordardottir, F.R.; Ramel, A.; Thorsdottir, I.; Gunnarsdottir, I. Validation of a plate diagram sheet for estimation of energy and protein intake in hospitalized patients. Clin. Nutr. 2013, 32, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Akamatsu, R.; Tamaura, Y.; Sakai, M.; Fujiwara, K.; Tsutsuura, S. Differences in the validity of a visual estimation method for determining patients’ meal intake between various meal types and supplied food items. Clin. Nutr. 2019, 38, 213–219. [Google Scholar] [CrossRef]
- Smoliner, C.; Volkert, D.; Wirth, R. Management of malnutrition in geriatric hospital units in Germany. Z. Gerontol. Geriatr. 2013, 46, 48–50. [Google Scholar] [CrossRef]
- Lu, Y.; Stathopoulou, T.; Vasiloglou, M.F.; Christodoulidis, S.; Stanga, Z.; Mougiakakou, S. An artificial intelligence-based system to assess nutrient intake for hospitalised patients. IEEE Trans. Multimed. 2020, 23, 1136–1147. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 3, 321–336. [Google Scholar] [CrossRef]
- SANALOGIC Solutions GmbH. Available online: https://www.sanalogic.com/ (accessed on 7 September 2021).
- Zhao, H.; Shi, J.; Qi, X.; Wang, X.; Jia, J. Pyramid scene parsing network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 2881–2890. [Google Scholar]
- Chen, L.C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking atrous convolution for semantic image segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Dehais, J.; Anthimopoulos, M.; Shevchik, S.; Mougiakakou, S. Two-view 3D reconstruction for food volume estimation. IEEE Trans. Multimed. 2016, 19, 1090–1099. [Google Scholar] [CrossRef] [Green Version]
- Makhsous, S.; Bharadwaj, M.; Atkinson, B.E.; Novosselov, I.V.; Mamishev, A.V. Dietsensor: Automatic dietary intake measurement using mobile 3D scanning sensor for diabetic patients. Sensors 2020, 20, 3380. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meal | Soup | Meat/Fish | Side Dish | Sauce | Salad | Dessert |
|---|---|---|---|---|---|---|
| A | Potato and carrot cream soup (protein+) | Trout fillet | Potato wedges | / | Creamed spinach | Pineapple mousse (protein+) |
| B | Potato and carrot cream soup (protein+) | / | Pappardelle noodles (soft homogenous) | Bolognaise Sauce | / | Pineapple mousse (protein+) |
| C | Potato and carrot cream soup (protein+) | Trout fillet | Potato wedges | / | Creamed spinach | / |
| Segmentation Network | Mean Intersection over Union (%) | Accuracy (%) | Fmin (%) | Fsum (%) |
|---|---|---|---|---|
| DeepLabv3 | 70.2 | 80.3 | 65.1 | 92.4 |
| DeepLabv3 w/plates | 70.8 | 80.8 | 65.2 | 92.5 |
| ResNet + PSPNet | 70.4 | 80.2 | 65.2 | 92.7 |
| ResNet + PSPNet w/plates | 70.7 | 81.1 | 65.5 | 92.9 |
| Encoder + PSPNet w/plates | 71.9 | 81.6 | 69.3 | 92.7 |
| Encoder + PSPNet w/plates w/pretraining | 69.7 | 78.6 | 68.2 | 92.1 |
| ResNet + PSPNet w/plates w/pretraining | 73.7 | 84.1 | 69.8 | 93.4 |
| System | Standard Clinical Procedure (SCP) | |||||
|---|---|---|---|---|---|---|
| Mean Absolute Error (Standard Deviation) | Mean Relative Error % | Correlation Coefficient | Mean Absolute Error (Standard Deviation) | Mean Relative Error % | Correlation Coefficient | |
| Energy (kcal) | 41 (54) | 11.64 | 0.967 | 112 (102) | 31.45 | 0.861 |
| CHO (g) | 4.6 (8.3) | 13.23 | 0.905 | 9.0 (10.8) | 33.88 | 0.790 |
| Protein (g) | 1.4 (2.5) | 10.47 | 0.979 | 3.7 (4.1) | 32.34 | 0.919 |
| Fat (g) | 1.9 (2.4) | 11.70 | 0.984 | 7.0 (6.4) | 41.29 | 0.877 |
| Fatty acids (g) | 1.2 (1.4) | 14.84 | 0.978 | 4.1 (3.7) | 56.42 | 0.841 |
| System Error (%) | Standard Clinical Procedure Error (%) | |
|---|---|---|
| Soup | 8.08 | 24.04 |
| Side dish | 9.50 | 12.67 |
| Meat/fish | 6.56 | 19.61 |
| Salad/vegetables | 7.46 | 21.50 |
| Dessert | 10.74 | 34.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papathanail, I.; Brühlmann, J.; Vasiloglou, M.F.; Stathopoulou, T.; Exadaktylos, A.K.; Stanga, Z.; Münzer, T.; Mougiakakou, S. Evaluation of a Novel Artificial Intelligence System to Monitor and Assess Energy and Macronutrient Intake in Hospitalised Older Patients. Nutrients 2021, 13, 4539. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124539
Papathanail I, Brühlmann J, Vasiloglou MF, Stathopoulou T, Exadaktylos AK, Stanga Z, Münzer T, Mougiakakou S. Evaluation of a Novel Artificial Intelligence System to Monitor and Assess Energy and Macronutrient Intake in Hospitalised Older Patients. Nutrients. 2021; 13(12):4539. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124539
Chicago/Turabian StylePapathanail, Ioannis, Jana Brühlmann, Maria F. Vasiloglou, Thomai Stathopoulou, Aristomenis K. Exadaktylos, Zeno Stanga, Thomas Münzer, and Stavroula Mougiakakou. 2021. "Evaluation of a Novel Artificial Intelligence System to Monitor and Assess Energy and Macronutrient Intake in Hospitalised Older Patients" Nutrients 13, no. 12: 4539. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124539