
A Fermented Milk Product Containing B. lactis CNCM I-2494 Improves the Tolerance of a Plant-Based Diet in Patients with Disorders of Gut–Brain Interactions

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
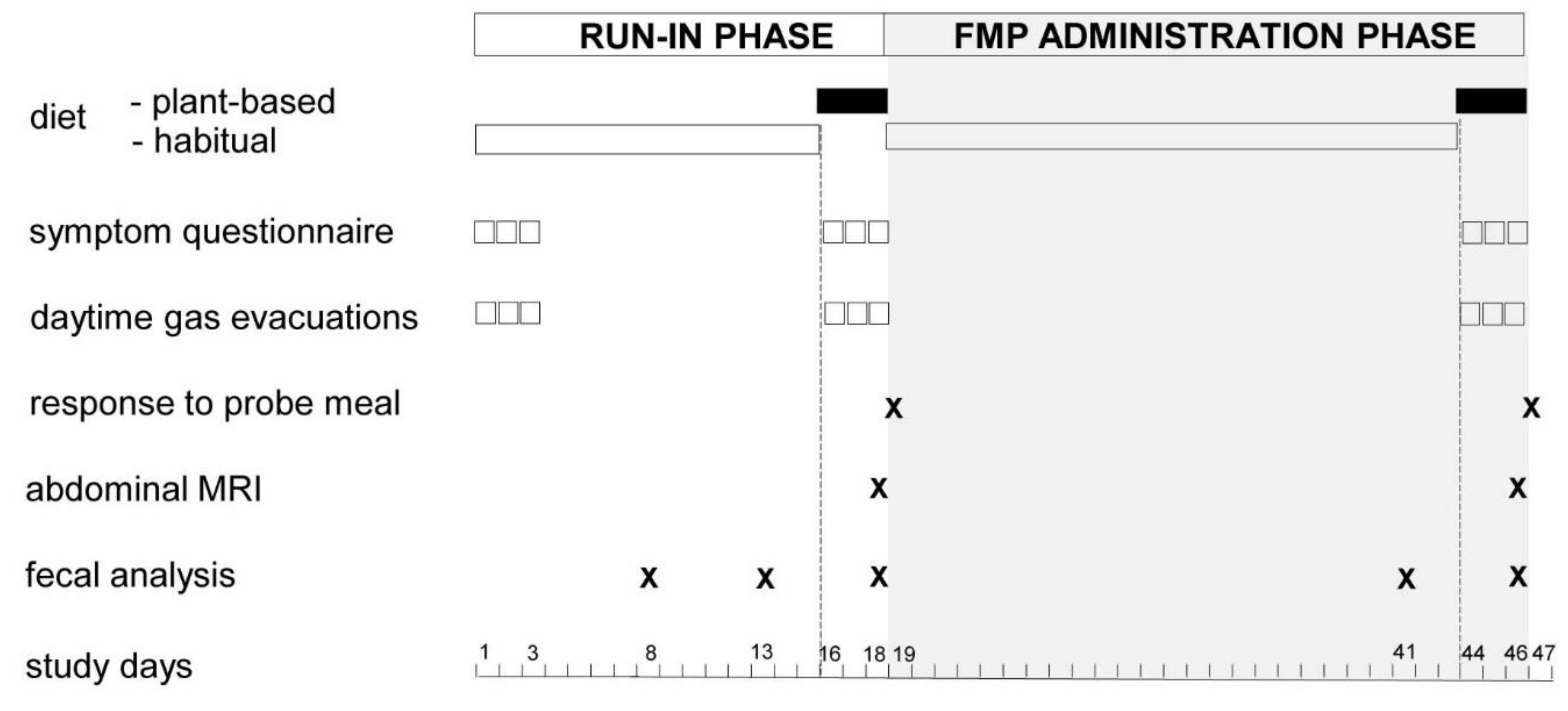
2.1. Study Design and General Procedure
2.2. Participants
2.3. Plant-Based Diet
2.4. Study Product
2.5. Main Outcomes
2.5.1. Daily Symptoms Questionnaire
2.5.2. Number of Anal Gas Evacuations
2.5.3. Volume of Anal Gas Production after a Probe Meal (Gas Production Test)
2.6. Exploratory Outcomes
2.6.1. Colonic Gas Content
2.6.2. Faecal Microbiota Analysis
2.7. Statistical Analysis
3. Results
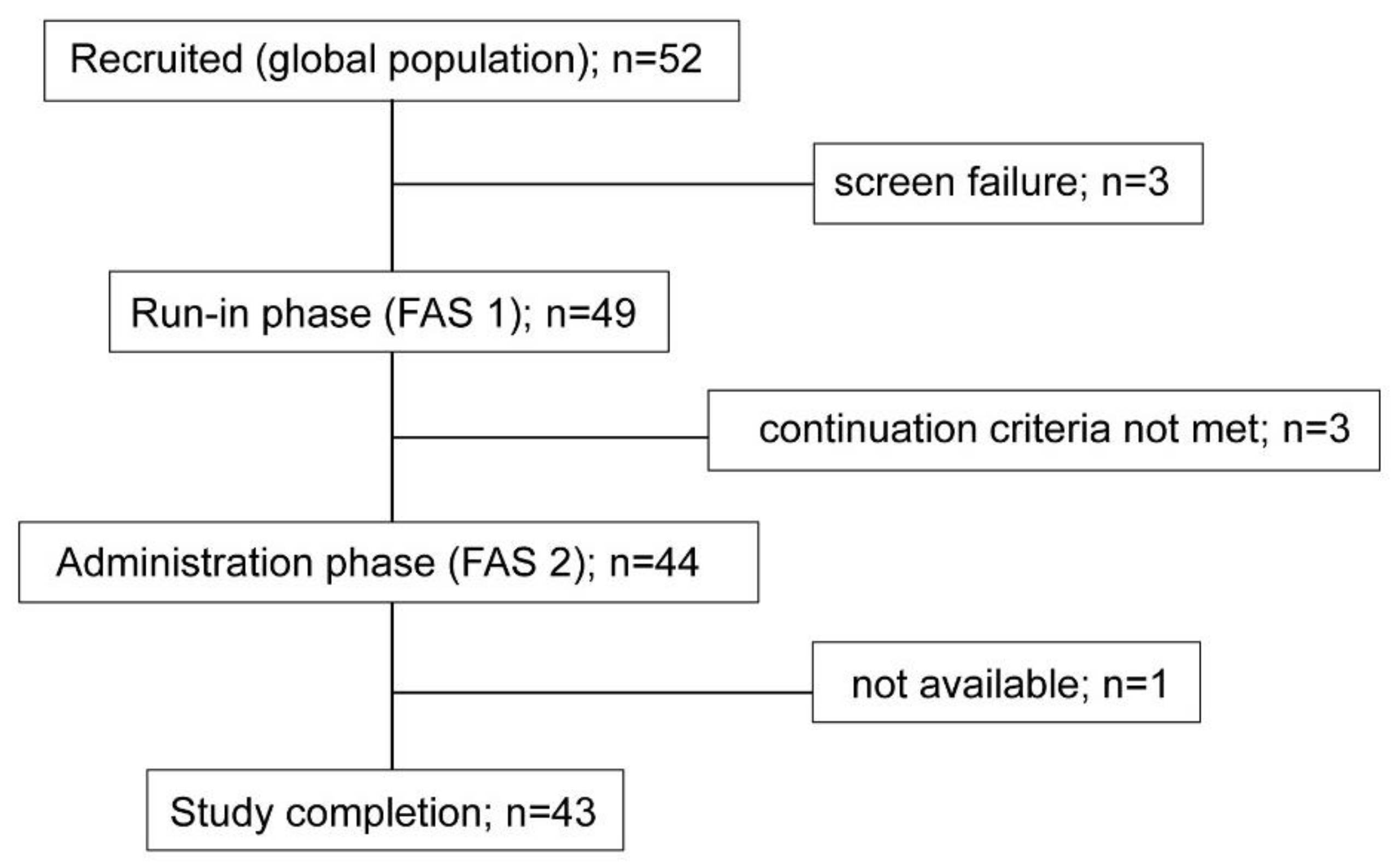
3.1. Demographics and Compliance to Study Procedures
3.2. Effect of the Plant-Based Diet during the Run-In Phase
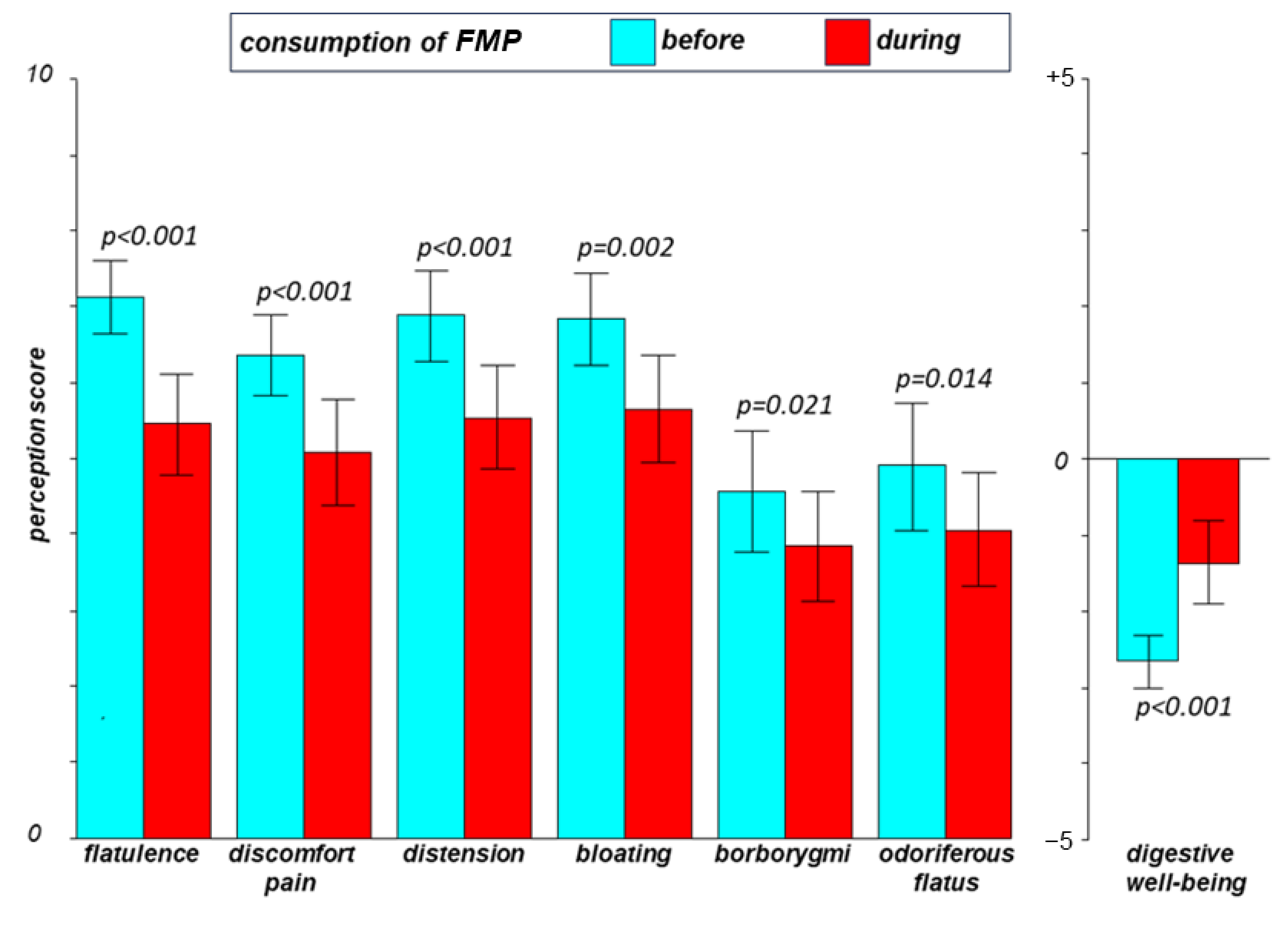
3.3. Effect of the Fermented Milk Product on the Tolerance of the Plant-Based Diet
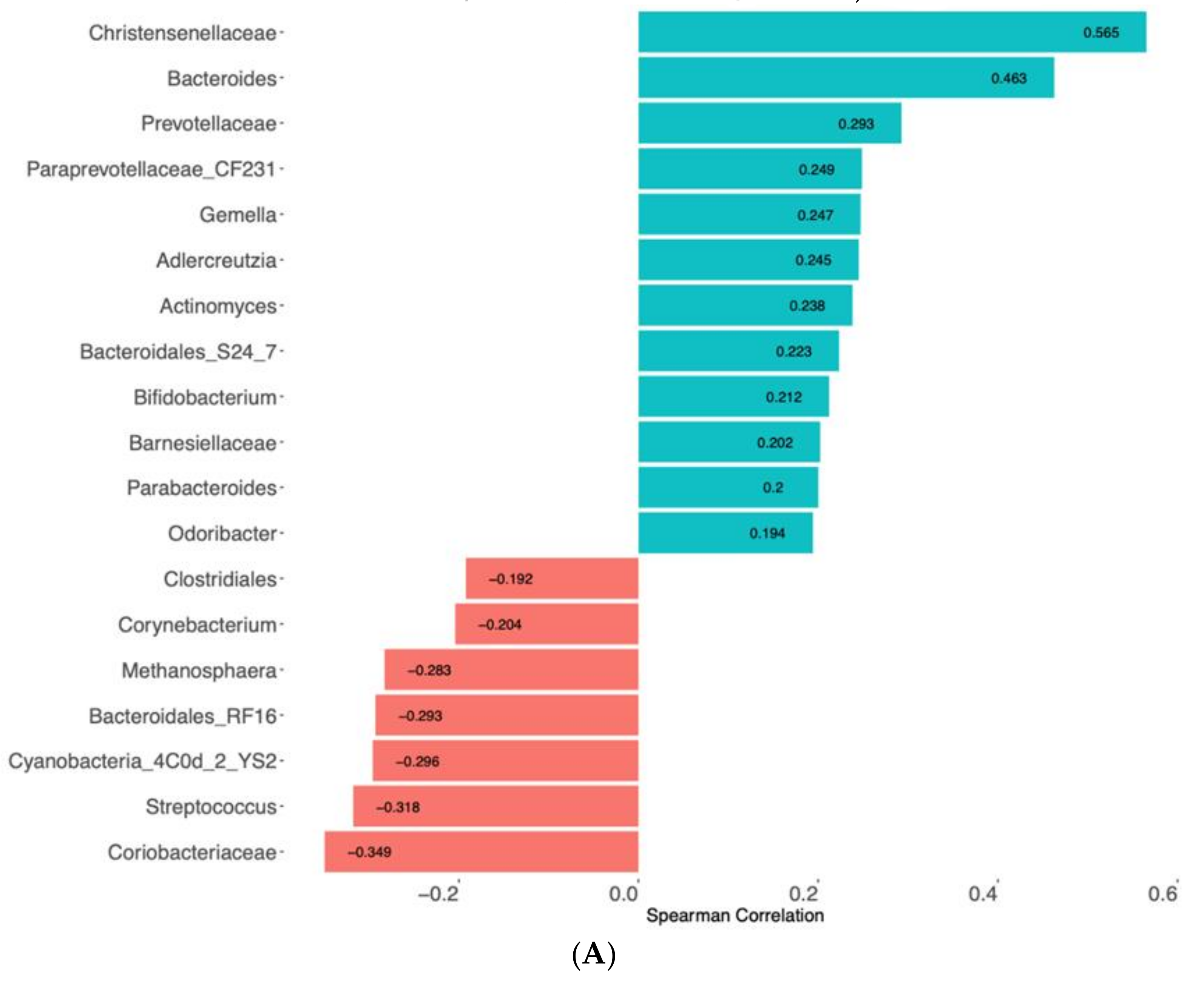
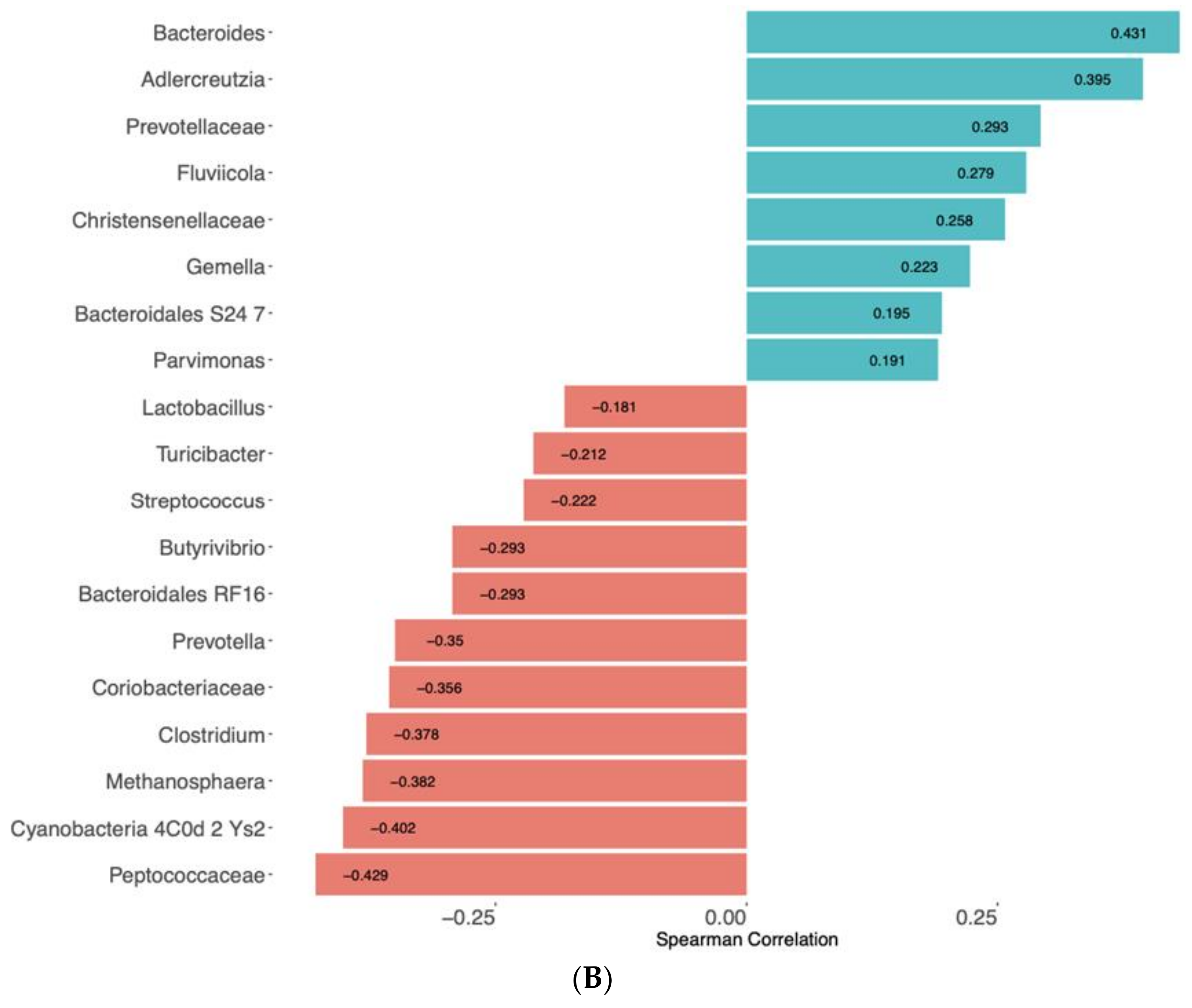
3.4. Faecal Microbiota
4. Discussion
Limitations
5. Clinical Inferences and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guyonnet, D.; Schlumberger, A.; Mhamdi, L.; Jakob, S.; Chassany, O. Fermented milk containing bifidobacterium lactis dn-173 010 improves gastrointestinal well-being and digestive symptoms in women reporting minor digestive symptoms: A randomised, double-blind, parallel, controlled study. Br. J. Nutr. 2009, 102, 1654–1662. [Google Scholar] [CrossRef] [PubMed]
- Guyonnet, D.; Woodcock, A.; Stefani, B.; Trevisan, C.; Hall, C. Fermented milk containing bifidobacterium lactis dn-173 010 improved self-reported digestive comfort amongst a general population of adults. A randomized, open-label, controlled, pilot study. J. Dig. Dis. 2009, 10, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Guyonnet, D.; Lafaye de Micheaux, P.; Gelu, S. A randomized, double-blind, controlled study and pooled analysis of two identical trials of fermented milk containing probiotic bifidobacterium lactis cncm i-2494 in healthy women reporting minor digestive symptoms. Neurogastroenterol. Motil. 2013, 25, 331-e252. [Google Scholar] [CrossRef]
- Marteau, P.; Le Neve, B.; Quinquis, L.; Pichon, C.; Whorwell, P.J.; Guyonnet, D. Consumption of a fermented milk product containing bifidobacterium lactis cncm i-2494 in women complaining of minor digestive symptoms: Rapid response which is independent of dietary fibre intake or physical activity. Nutrients 2019, 11, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, A.; Houghton, L.A.; Morris, J.; Reilly, B.; Guyonnet, D.; Goupil Feuillerat, N.; Schlumberger, A.; Jakob, S.; Whorwell, P.J. Clinical trial: The effects of a fermented milk product containing bifidobacterium lactis dn-173 010 on abdominal distension and gastrointestinal transit in irritable bowel syndrome with constipation. Aliment. Pharmacol. Ther. 2009, 29, 104–114. [Google Scholar] [CrossRef]
- Guyonnet, D.; Chassany, O.; Ducrotte, P.; Picard, C.; Mouret, M.; Mercier, C.H.; Matuchansky, C. Effect of a fermented milk containing bifidobacterium animalis dn-173 010 on the health-related quality of life and symptoms in irritable bowel syndrome in adults in primary care: A multicentre, randomized, double-blind, controlled trial. Aliment. Pharmacol. Ther. 2007, 26, 475–486. [Google Scholar] [CrossRef]
- Le Nevé, B.; Derrien, M.; Tap, J.; Brazeilles, R.; Cools Portier, S.; Guyonnet, D.; Ohman, L.; Störsrud, S.; Törnblom, H.; Simrén, M. Fasting breath h2 and gut microbiota metabolic potential are associated with the response to a fermented milk product in irritable bowel syndrome. PLoS ONE 2019, 14, e0214273. [Google Scholar] [CrossRef]
- Le Neve, B.; de la Torre, A.M.; Tap, J.; Derrien, M.; Cotillard, A.; Barba, E.; Mego, M.; Nieto Ruiz, A.; Hernandez-Palet, L.; Dornic, Q.; et al. A fermented milk product with b. Lactis cncm i-2494 and lactic acid bacteria improves gastrointestinal comfort in response to a challenge diet rich in fermentable residues in healthy subjects. Nutrients 2020, 12, 320. [Google Scholar] [CrossRef] [Green Version]
- Barba, E.; Burri, E.; Accarino, A.; Cisternas, D.; Quiroga, S.; Monclus, E.; Navazo, I.; Malagelada, J.R.; Azpiroz, F. Abdomino-thoracic mechanisms of functional abdominal distension and correction by biofeedback. Gastroenterology 2015, 148, 732–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burri, E.; Barba, E.; Huaman, J.W.; Cisternas, D.; Accarino, A.; Soldevilla, A.; Malagelada, J.R.; Azpiroz, F. Mechanisms of postprandial abdominal bloating and distension in functional dyspepsia. Gut 2014, 63, 395–400. [Google Scholar] [CrossRef]
- Malagelada, C.; Drozdzal, M.; Segui, S.; Mendez, S.; Vitria, J.; Radeva, P.; Santos, J.; Accarino, A.; Malagelada, J.R.; Azpiroz, F. Classification of functional bowel disorders by objective physiological criteria based on endoluminal image analysis. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 309, G413–G419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manichanh, C.; Eck, A.; Varela, E.; Roca, J.; Clemente, J.C.; Gonzalez, A.; Knights, D.; Knight, R.; Estrella, S.; Hernandez, C.; et al. Anal gas evacuation and colonic microbiota in patients with flatulence: Effect of diet. Gut 2014, 63, 401–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mego, M.; Accarino, A.; Tzortzis, G.; Vulevic, J.; Gibson, G.; Guarner, F.; Azpiroz, F. Colonic gas homeostasis: Mechanisms of adaptation following host-g904 galactooligosaccharide use in humans. Neurogastroenterol Mot. 2017, 29, e13080. [Google Scholar] [CrossRef]
- Serra, J.; Azpiroz, F.; Malagelada, J.R. Intestinal gas dynamics and tolerance in humans. Gastroenterology 1998, 115, 542–550. [Google Scholar] [CrossRef]
- Pascal, V.; Pozuelo, M.; Borruel, N.; Casellas, F.; Campos, D.; Santiago, A.; Martinez, X.; Varela, E.; Sarrabayrouse, G.; Machiels, K.; et al. A microbial signature for crohn’s disease. Gut 2017, 66, 813. [Google Scholar] [CrossRef] [PubMed]
- Barber, C.; Mego, M.; Sabater, C.; Vallejo, F.; Bendezu, R.A.; Masihy, M.; Guarner, F.; Espin, J.C.; Margolles, A.; Azpiroz, F. Differential effects of western and mediterranean-type diets on gut microbiota: A metagenomics and metabolomics approach. Nutrients 2021, 13, 2638. [Google Scholar] [CrossRef] [PubMed]
- Bendezu, R.A.; Mego, M.; Monclus, E.; Merino, X.; Accarino, A.; Malagelada, J.R.; Navazo, I.; Azpiroz, F. Colonic content: Effect of diet, meals, and defecation. Neurogastroenterol. Motil. 2017, 29, e12930. [Google Scholar] [CrossRef] [PubMed]
- Agostini, S.; Goubern, M.; Tondereau, V.; Salvador-Cartier, C.; Bezirard, V.; Lévèque, M.; Keränen, H.; Theodorou, V.; Bourdu-Naturel, S.; Goupil-Feuillerat, N.; et al. A marketed fermented dairy product containing bifidobacterium lactis cncm i-2494 suppresses gut hypersensitivity and colonic barrier disruption induced by acute stress in rats. Neurogastroenterol. Motil. 2012, 24, 376-e172. [Google Scholar] [CrossRef]
- Tillisch, K.; Labus, J.; Kilpatrick, L.; Jiang, Z.; Stains, J.; Ebrat, B.; Guyonnet, D.; Legrain–Raspaud, S.; Trotin, B.; Naliboff, B.; et al. Consumption of fermented milk product with probiotic modulates brain activity. Gastroenterology 2013, 144, 1394–1401.e1394. [Google Scholar] [CrossRef] [Green Version]
- Wastyk, H.C.; Fragiadakis, G.K.; Perelman, D.; Dahan, D.; Merrill, B.D.; Yu, F.B.; Topf, M.; Gonzalez, C.G.; Van Treuren, W.; Han, S.; et al. Gut-microbiota-targeted diets modulate human immune status. Cell 2021, 184, 4137–4153.e4114. [Google Scholar] [CrossRef] [PubMed]
- Huaman, J.W.; Mego, M.; Manichanh, C.; Canellas, N.; Canueto, D.; Segurola, H.; Jansana, M.; Malagelada, C.; Accarino, A.; Vulevic, J.; et al. Effects of prebiotics vs a diet low in fodmaps in patients with functional gut disorder. Gastroenterology 2018, 155, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Azpiroz, F.; Hernandez, C.; Guyonnet, D.; Accarino, A.; Santos, J.; Malagelada, J.R.; Guarner, F. Effect of a low-flatulogenic diet in patients with flatulence and functional digestive symptoms. Neurogastroenterol. Motil. 2014, 26, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Bohn, L.; Storsrud, S.; Liljebo, T.; Collin, L.; Lindfors, P.; Tornblom, H.; Simren, M. Diet low in fodmaps reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: A randomized controlled trial. Gastroenterology 2015, 149, 1399–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in fodmaps reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75. [Google Scholar] [CrossRef]
- Brokes, S.; Costa, M. Functional neuroanatomy. In Pathophysiology of the Enteric Nervous System; Spiller, R., Grundy, D., Eds.; Blackwell: Oxford, UK, 2004; pp. 126–133. [Google Scholar]
- Ford, A.C.; Quigley, E.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Moayyedi, P. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: Systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 1547–1561. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Habitual Diet (n = 48) | Plant-Based Diet (n = 47) | p Value | |
|---|---|---|---|
| Flatulence * | 5.8 [5.2; 6.32] | 6.8 [6.2; 7.4] | p < 0.001 |
| Abdominal discomfort/pain * | 5.3 [4.7; 5.9] | 6.2 [5.7; 6.7] | p < 0.001 |
| Abdominal distension * | 5.8 [5.1; 6.4] | 6.7 [6.1; 7.3] | p < 0.001 |
| Bloating * | 5.7 [5.0; 6.3] | 6.7 [6.1; 7.3] | p < 0.001 |
| Borborygmi * | 4.0 [3.2; 4.8] | 4.5 [3.8; 5.3] | p < 0.001 |
| Odor of flatus * | 4.3 [3.5; 5.1] | 4.7 [3.9; 5.5] | p >0.05 |
| Digestive well-being * | −1.8 [−2.3; −1.2] | −2.5 [−2.9; −2.1] | p < 0.005 |
| Anal gas evacuations * | 16.5 [13.5; 19.4] | 22.3 [18.6; 26.0] | p < 0.001 |
| Bowel movements ** | 1.4 [1.2; 1.6] | 1.4 [1.2; 1.6] | p > 0.05 |
| Stool consistency ** | 4.0 [3.6; 4.3] | 4.0 [3.6; 4.4] | p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevé, B.L.; Martinez-De la Torre, A.; Tap, J.; Ruiz, A.N.; Derrien, M.; Cotillard, A.; Faurie, J.-M.; Barba, E.; Mego, M.; Dornic, Q.; et al. A Fermented Milk Product Containing B. lactis CNCM I-2494 Improves the Tolerance of a Plant-Based Diet in Patients with Disorders of Gut–Brain Interactions. Nutrients 2021, 13, 4542. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124542
Nevé BL, Martinez-De la Torre A, Tap J, Ruiz AN, Derrien M, Cotillard A, Faurie J-M, Barba E, Mego M, Dornic Q, et al. A Fermented Milk Product Containing B. lactis CNCM I-2494 Improves the Tolerance of a Plant-Based Diet in Patients with Disorders of Gut–Brain Interactions. Nutrients. 2021; 13(12):4542. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124542
Chicago/Turabian StyleNevé, Boris Le, Adrian Martinez-De la Torre, Julien Tap, Adoración Nieto Ruiz, Muriel Derrien, Aurélie Cotillard, Jean-Michel Faurie, Elizabeth Barba, Marianela Mego, Quentin Dornic, and et al. 2021. "A Fermented Milk Product Containing B. lactis CNCM I-2494 Improves the Tolerance of a Plant-Based Diet in Patients with Disorders of Gut–Brain Interactions" Nutrients 13, no. 12: 4542. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124542