Prevalence and Correlates of Vitamin D Deficiency and Insufficiency in Luxembourg Adults: Evidence from the Observation of Cardiovascular Risk Factors (ORISCAV-LUX) Study

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Participants
2.2. Demographic Variables
2.3. Lifestyle-Related Variables
2.4. Vitamin D Measures
2.5. Definition of Vitamin D Status
2.6. Ethical Aspects
2.7. Statistical Analysis
3. Results
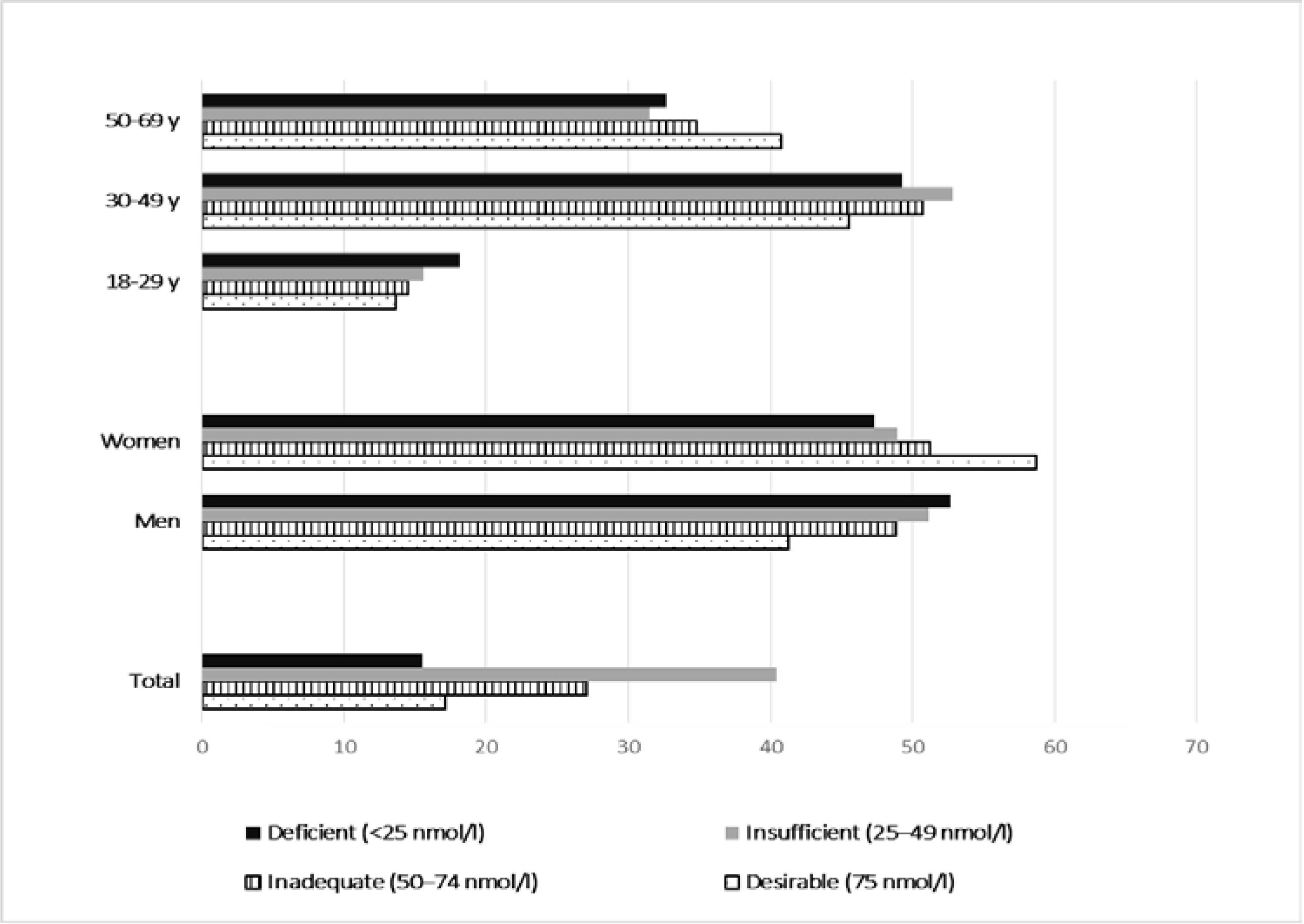
3.1. Vitamin D Status

3.2. Prevalence of Vitamin D Deficiency and Insufficiency by Risk Factors
3.3. Independent Correlates to Vitamin D Deficiency and Insufficiency

{kind=link}
| Vitamin D Deficiency | Vitamin D Insufficiency | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Total Subjects | No. (%) of Subjects with Vitamin D Insufficiency * | Age and sex adjusted OR † | 95%CI | p-Value | Total Subjects | No. (%) of Subjects with Vitamin D Insufficiency * | Age and Sex Adjusted OR † | 95%CI | p-Value |
| Level of education | 0.27 | 0.53 | ||||||||
| Tertiary | 351 | 47 (13.4%) | Ref. | 351 | 187 (53.3%) | Ref. | ||||
| Secondary | 625 | 95 (15.2%) | 1.41 | 0.92–2.14 | 625 | 347 (55.5%) | 1.11 | 0.85–1.44 | ||
| Primary | 345 | 60 (17.4%) | 1.168 | 0.8–1.7 | 345 | 194 (56.2%) | 1.18 | 0.87–1.6 | ||
| Country of birth | 0.21 | 0.02 | ||||||||
| Luxembourg | 813 | 126 (15.5%) | Ref | 813 | 440 (54.1%) | Ref. | ||||
| Other European country | 159 | 25 (15.7%) | 0.99 | 0.62–1.6 | 288 | 145 (50.3%) | 0.86 | 0.66–1.13 | ||
| No European country | 288 | 37 (12.9%) | 0.81 | 0.54–1.2 | 75 | 50 (66.7%) | 1.65 | 1.002–2.74 | ||
| Portugal | 75 | 17 (22.7%) | 1.58 | 0.9–2.9 | 159 | 100 (62.9%) | 1.38 | 0.97–1.97 | ||
| Economic status | 0.58 | 0.26 | ||||||||
| Above risk of poverty threshold | 907 | 138 (15.2%) | Ref. | 907 | 494 (54.5%) | Ref. | ||||
| Below risk of poverty threshold | 251 | 42 (16.7%) | 1.11 | 0.76–1.63 | 251 | 148 (58.9%) | 1.17 | 0.88–1.56 | ||
| Smoking status | 0.0002 | 0.02 | ||||||||
| Non–smokers | 1049 | 140 (13.4%) | Ref | 1049 | 558 (53.2%) | Ref. | ||||
| Current smokers | 286 | 65 (22.7%) | 1.88 | 1.35–2.63 | 286 | 177 (38.1%) | 1.37 | 1.044–1.79 | ||
| Alcohol consumption | 0.81 | 0.03 | ||||||||
| Non-drinker | 226 | 35 (15.5%) | Ref | 226 | 137 (60.6%) | Ref. | ||||
| Drinker | 1109 | 170 (15.3%) | 0.95 | 0.63–1.42 | 1109 | 598 (53.92%) | 0.72 | 0.53–0.97 | ||
| Physical activity | 0.63 | 0.58 | ||||||||
| Active | 1052 | 161 (15.3%) | Ref | 1052 | 575 (54.7%) | Ref. | ||||
| Inactive | 221 | 37 (16.7%) | 1.1 | 0.74–1.62 | 221 | 126 (57%) | 1.08 | 0.81–1.45 | ||
| Obesity status | 0.02 | <0.0001 | ||||||||
| Underweight | 21 | 5 (23.8%) | 1.93 | 0.66–5.61 | 21 | 13 (61.9%) | 1.52 | 0.58–3.950 | ||
| Normal weight | 566 | 77 (13.6%) | Ref | 566 | 280 (49.5%) | Ref. | ||||
| Overweight | 446 | 61 (13.7%) | 1.02 | 0.69–1.48 | 446 | 239 (53.6%) | 1.24 | 0.96–1.62 | ||
| Obesity | 301 | 62 (20.6%) | 1.72 | 1.16–2.55 | 301 | 202 (67.11%) | 2.33 | 1.71–3.18 | ||
| Abdominal obesity § | 0.021 | <0.0001 | ||||||||
| No Obese | 611 | 83 (13.6%) | Ref | 611 | 315 (51.5%) | Ref. | ||||
| Obese | 723 | 122 (16.9%) | 1.44 | 1.05–1.99 | 723 | 419 (57.95%) | 1.71 | 1.33–2.2 | ||
| HDL level £ | 0.026 | 0.001 | ||||||||
| High HDL-C | 1064 | 150 (14.10%) | Ref | 1064 | 563 (52.9%) | Ref. | ||||
| Reduced HDL-C | 243 | 48 (19.75%) | 1.54 | 1.05–2.26 | 243 | 154 (63.4%) | 1.64 | 1.22–2.21 | ||
| Self–perceived health | 0.0005 | 0.0049 | ||||||||
| Excellent/good | 818 | 103 (12.6%) | Ref | 818 | 425 (51.96%) | Ref. | ||||
| Fair/Poor | 485 | 96 (19.8%) | 1.74 | 1.28–2.36 | 485 | 289 (59.59%) | 1.39 | 1.10–1.75 | ||
| Vitamin D intake, µg/day | 9.3 [9.1–9.6] | 0.51 | 0.29–0.87 | 0.01 | 2.6 [1.4–4.6] | 0.97 | 0.93–1.009 | 0.12 | ||
| Serum Ca, mg/dL | 1.2 [0.7–2.05] | 1.022 | 0.9–1.15 | 0.73 | 9.3 [9.1–9.6] | 0.95 | 0.72–1.25 | 0.71 | ||
| Dairy intake, servings/day | 2.6 [1.4–4.6] | 0.92 | 0.87–0.98 | 0.01 | 1.2 [0.7–2.05] | 1.008 | 0.9–1.09 | 0.83 | ||
| Vitamin D Deficiency * | ||||
|---|---|---|---|---|
| Characteristics | Fully adjusted OR † | 95%CI | p-value | |
| Sex | Men v. women | 1.29 | 0.9–1.8 | 0.13 |
| Age, years | 0.99 | 0.98–1.007 | 0.36 | |
| HDL level | Low level v. high level | 1.24 | 0.83–1.84 | 0.29 |
| Obesity status | 0.16 | |||
| Underweight v. normal weight | 1.43 | 0.45–4.54 | ||
| Overweight v. normal weight | 0.82 | 0.52–1.29 | ||
| Obesity v. normal weight | 1.32 | 0.76–2.27 | ||
| Abdominal obesity | Abdominally obese v. no-abdominally obese | 1.28 | 0.81–2.03 | 0.28 |
| Smoking status | Smokers v. non-smokers | 1.80 | 1.26–2.57 | 0.0012 |
| Health perception | Fair/poor v. excellent/good health | 1.37 | 0.99–1.89 | 0.060 |
| Vitamin D Insufficiency * | ||||
|---|---|---|---|---|
| Characteristics | Fully adjusted OR † | 95% CI | p-value | |
| Sex | Men v. women | 1.25 | 0.97–1.60 | 0.081 |
| Age, years | 0.99 | 0.98–0.99 | 0.023 | |
| HDL level | Low level v. high level | 0.083 | ||
| Country of birth | Other European country v. Luxembourg | 0.87 | 0.66–1.16 | 0.07 |
| Non–European country v. Luxembourg | 1.70 | 1.009–2.87 | ||
| Portugal v. Luxembourg | 1.26 | 0.87–1.84 | ||
| Obesity status | 0.0046 | |||
| Underweight v. normal weight | 1.43 | 0.56–3.63 | ||
| Obesity v. normal weight | 1.94 | 1.29–2.93 | ||
| Overweight v. normal weight | 1.11 | 0.81–1.53 | ||
| Alcohol consumption | Drinker v. non-drinker | 0.79 | 0.58–1.09 | 0.16 |
| Abdominal obesity | Abdominally obese v. no-abdominally obese | 1.11 | 0.81–1.52 | 0.53 |
| Smoking status | Smokers v. non-smokers | 1.28 | 0.96–1.71 | 0.093 |
| Health perception | Fair/poor v. excellent/good health | 1.08 | 0.84–1.38 | 0.54 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Palacios, C. The role of nutrients in bone health, from A to Z. Crit. Rev. Food Sci. Nutr. 2006, 46, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. BNF 2014, 39, 322–350. [Google Scholar] [CrossRef] [PubMed]
- Dunnigan, M.G.; Henderson, J.B.; Hole, D. Serum 25-hydroxyvitamin D and colon cancer. Lancet 1990, 335, 111–112. [Google Scholar] [CrossRef]
- Garland, C.F.; Garland, F.C.; Gorham, E.D.; Lipkin, M.; Newmark, H.; Mohr, S.B.; Holick, M.F. The role of vitamin D in cancer prevention. Am. J. Public Health 2006, 96, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Laaksi, I.; Ruohola, J.P.; Tuohimaa, P.; Auvinen, A.; Haataja, R.; Pihlajamaki, H.; Ylikomi, T. An association of serum vitamin D concentrations <40 nmol/L with acute respiratory tract infection in young Finnish men. Am. J. Clin. Nutr. 2007, 86, 714–717. [Google Scholar] [PubMed]
- Munger, K.L.; Levin, L.I.; Hollis, B.W.; Howard, N.S.; Ascherio, A. Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 2006, 296, 2832–2838. [Google Scholar] [CrossRef] [PubMed]
- Poole, K.E.; Loveridge, N.; Barker, P.J.; Halsall, D.J.; Rose, C.; Reeve, J.; Warburton, E.A. Reduced vitamin D in acute stroke. Stroke 2006, 37, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Boniol, M.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Autier, P.; Gandini, S. Vitamin D supplementation and total mortality: A meta-analysis of randomized controlled trials. Arch. Intern. Med. 2007, 167, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Lappe, J.M.; Travers-Gustafson, D.; Davies, K.M.; Recker, R.R.; Heaney, R.P. Vitamin D and calcium supplementation reduces cancer risk: Results of a randomized trial. Am. J. Clin. Nutr. 2007, 85, 1586–1591. [Google Scholar] [PubMed]
- Lips, P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: Consequences for bone loss and fractures and therapeutic implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef] [PubMed]
- Daly, R.M.; Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Sikaris, K.A.; Zimmet, P.Z.; Ebeling, P.R.; Shaw, J.E. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: A national, population-based study. Clin. Endocrinol. 2012, 77, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; de Peter, K.C.; Feldman, H.A.; Grace, E.; Emans, S.J. Prevalence of vitamin D deficiency among healthy adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Sauvageot, N.; Donneau, A.F.; Lair, M.L.; Couffignal, S.; Beissel, J.; Delagardelle, C.; Wagener, Y.; Albert, A.; Guillaume, M. First nationwide survey on cardiovascular risk factors in Grand-Duchy of Luxembourg (ORISCAV-LUX). BMC Public Health 2010, 10, 468. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Sauvageot, N.; Couffignal, S.; Albert, A.; Lair, M.L.; Guillaume, M. Comparison of participants and non-participants to the ORISCAV-LUX population-based study on cardiovascular risk factors in Luxembourg. BMC Med. Res. Methodol. 2010, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Donneau, A.F.; Sauvageot, N.; Lair, M.L.; Albert, A.; Guillaume, M. Dietary, behavioural and socio-economic determinants of the metabolic syndrome among adults in Luxembourg: Findings from the ORISCAV-LUX study. Public Health Nutr. 2012, 15, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Committee, I.R. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. Available online: http://wwwipaqkise/scoringpdf (accessed on 15 June 2015).
- Alberti, K.G.; Zimmet, P.; Shaw, J.; Group IDFETFC. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B., Jr.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C.; National Heart, Lung, and Blood Institute; American Heart Association. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Sauvageot, N.; Alkerwi, A.; Albert, A.; Guillaume, M. Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: Validation with biomarkers. Nutr. J. 2013, 12, 143. [Google Scholar] [CrossRef] [PubMed]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J.; et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [PubMed]
- Forsythe, L.K.; Livingstone, M.B.; Barnes, M.S.; Horigan, G.; McSorley, E.M.; Bonham, M.P.; Magee, P.J.; Hill, T.R.; Lucey, A.J.; Cashman, K.D.; et al. Effect of adiposity on vitamin D status and the 25-hydroxycholecalciferol response to supplementation in healthy young and older Irish adults. Br. J. Nutr. 2012, 107, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Compston, J.E.; Vedi, S.; Ledger, J.E.; Webb, A.; Gazet, J.C.; Pilkington, T.R. Vitamin D status and bone histomorphometry in gross obesity. Am. J. Clin. Nutr. 1981, 34, 2359–2363. [Google Scholar] [PubMed]
- Liel, Y.; Ulmer, E.; Shary, J.; Hollis, B.W.; Bell, N.H. Low circulating vitamin D in obesity. Calcif. Tissue Int. 1988, 43, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Brot, C.; Jorgensen, N.R.; Sorensen, O.H. The influence of smoking on vitamin D status and calcium metabolism. Eur. J. Clin. Nutr. 1999, 53, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Cutillas-Marco, E.; Fuertes-Prosper, A.; Grant, W.B.; Morales-Suarez-Varela, M. Vitamin D deficiency in South Europe: Effect of smoking and aging. Photodermatol. Photoimmunol. Photomed. 2012, 28, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.M.; Davis, J.W.; Nomura, A.; Wasnich, R.D.; Ross, P.D. The effects of smoking on bone mass and the rates of bone loss among elderly Japanese-American men. J. Bone Miner. Res. 1997, 12, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Law, M.R.; Hackshaw, A.K. A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: Recognition of a major effect. BMJ 1997, 315, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Daniel, M.; Martin, A.D.; Drinkwater, D.T. Cigarette smoking, steroid hormones, and bone mineral density in young women. Calcif. Tissue Int. 1992, 50, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Thorlindsson, T.; Vilhjalmsson, R. Factors related to cigarette smoking and alcohol use among adolescents. Adolescence 1991, 26, 399–418. [Google Scholar] [PubMed]
- Alkerwi, A.; Sauvageot, N.; Nau, A.; Lair, M.L.; Donneau, A.F.; Albert, A.; Guillaume, M. Population compliance with national dietary recommendations and its determinants: Findings from the ORISCAV-LUX study. Br. J. Nutr. 2012, 108, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.A.; Frost, P.J.; Iida-Klein, A.; Hahn, T.J. Effects of nicotine on cellular Function in UMR 106-01 osteoblast-like cells. Bone 1991, 12, 283–286. [Google Scholar] [CrossRef]
- Gannage-Yared, M.H.; Chedid, R.; Khalife, S.; Azzi, E.; Zoghbi, F.; Halaby, G. Vitamin D in relation to metabolic risk factors, insulin sensitivity and adiponectin in a young Middle-Eastern population. Eur. J. Endocrinol. Eur. Fed. Endocr. Soc. 2009, 160, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Grimnes, G. Vitamin D and metabolic health with special reference to the effect of vitamin D on serum lipids. Prog. Lipid Res. 2011, 50, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Figenschau, Y.; Hutchinson, M.; Emaus, N.; Grimnes, G. High serum 25-hydroxyvitamin D concentrations are associated with a favorable serum lipid profile. Eur. J. Clin. Nutr. 2010, 64, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Ponda, M.P.; Huang, X.; Odeh, M.A.; Breslow, J.L.; Kaufman, H.W. Vitamin D may not improve lipid levels: A serial clinical laboratory data study. Circulation 2012, 126, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A. Vitamin D and disease prevention with special reference to cardiovascular disease. Prog. Biophys. Mol. Biol. 2006, 92, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A. Vitamin D and cardiovascular disease. Anticancer Res. 2014, 34, 4641–4648. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J. Clinical practice. Vitamin D insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Kazlauskaite, R.; Powell, L.H.; Mandapakala, C.; Cursio, J.F.; Avery, E.F.; Calvin, J. Vitamin D is associated with atheroprotective high-density lipoprotein profile in postmenopausal women. J. Clin. Lipidol. 2010, 4, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Rye, K.A.; Bursill, C.A.; Lambert, G.; Tabet, F.; Barter, P.J. The metabolism and anti-atherogenic properties of HDL. J. Lipid Res. 2009, 50, S195–S200. [Google Scholar] [CrossRef] [PubMed]
- Sweetnam, P.M.; Bolton, C.H.; Yarnell, J.W.; Bainton, D.; Baker, I.A.; Elwood, P.C.; Miller, N.E. Associations of the HDL2 and HDL3 cholesterol subfractions with the development of ischemic heart disease in British men. The Caerphilly and Speedwell Collaborative Heart Disease Studies. Circulation 1994, 90, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Yarnell, J.W.; Sweetnam, P.; Bolton, C.H. High density lipoprotein subfractions and the risk of coronary heart disease: 9-years follow-up in the Caerphilly Study. Atherosclerosis 2003, 166, 331–338. [Google Scholar] [CrossRef]
- Parish, S.; Offer, A.; Clarke, R.; Hopewell, J.C.; Hill, M.R.; Otvos, J.D.; Armitage, J.; Collins, R.; Heart Protection Study Collaborative Group. Lipids and lipoproteins and risk of different vascular events in the MRC/BHF Heart Protection Study. Circulation 2012, 125, 2469–2478. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Khokhar, A.A.; May, H.T.; Kulkarni, K.R.; Blaha, M.J.; Joshi, P.H.; Toth, P.P.; Muhlestein, J.B.; Anderson, J.L.; Knight, S.; et al. HDL cholesterol subclasses, myocardial infarction, and mortality in secondary prevention: The Lipoprotein Investigators Collaborative. Eur. Heart J. 2015, 36, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.A.; Cooper, C.; Ebeling, P.R.; Eggersdorfer, M.; Hilger, J.; Hoffmann, K.; Josse, R.; Kanism, J.A.; Mithal, A.; Pierroz, D.D.; et al. A global representation of vitamin D status in healthy populations. Arch. Osteoporos. 2012, 7, 155–172. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkerwi, A.; Sauvageot, N.; Gilson, G.; Stranges, S. Prevalence and Correlates of Vitamin D Deficiency and Insufficiency in Luxembourg Adults: Evidence from the Observation of Cardiovascular Risk Factors (ORISCAV-LUX) Study. Nutrients 2015, 7, 6780-6796. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7085308
Alkerwi A, Sauvageot N, Gilson G, Stranges S. Prevalence and Correlates of Vitamin D Deficiency and Insufficiency in Luxembourg Adults: Evidence from the Observation of Cardiovascular Risk Factors (ORISCAV-LUX) Study. Nutrients. 2015; 7(8):6780-6796. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7085308
Chicago/Turabian StyleAlkerwi, Ala'a, Nicolas Sauvageot, Georges Gilson, and Saverio Stranges. 2015. "Prevalence and Correlates of Vitamin D Deficiency and Insufficiency in Luxembourg Adults: Evidence from the Observation of Cardiovascular Risk Factors (ORISCAV-LUX) Study" Nutrients 7, no. 8: 6780-6796. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7085308