Persistent Intraepithelial Lymphocytosis in Celiac Patients Adhering to Gluten-Free Diet Is Not Abolished Despite a Gluten Contamination Elimination Diet


Abstract
:1. Introduction
2. Materials and methods
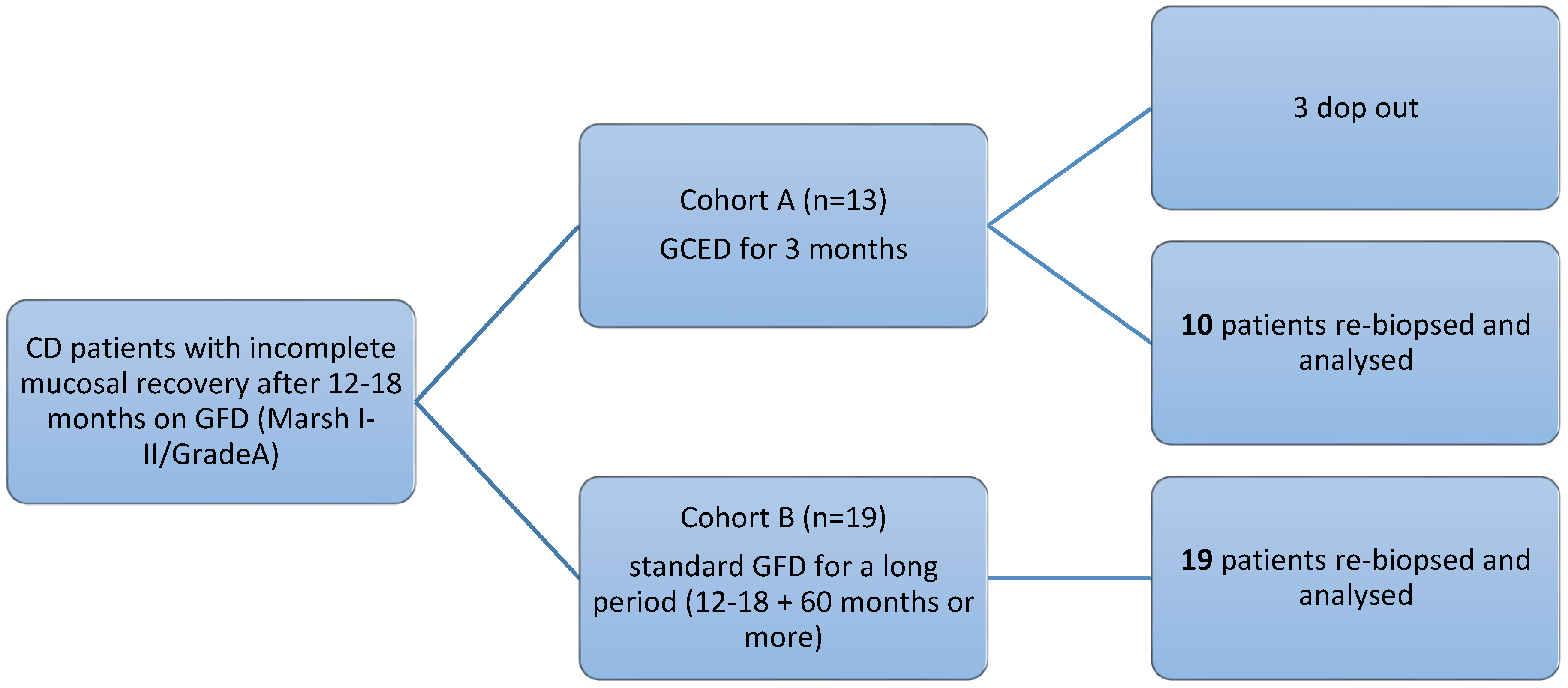
2.1. Recruitment
2.2. Serology
2.3. Histology
2.4. Statistics
2.5. Ethics
3. Results
3.1. Patients’ Characteristics
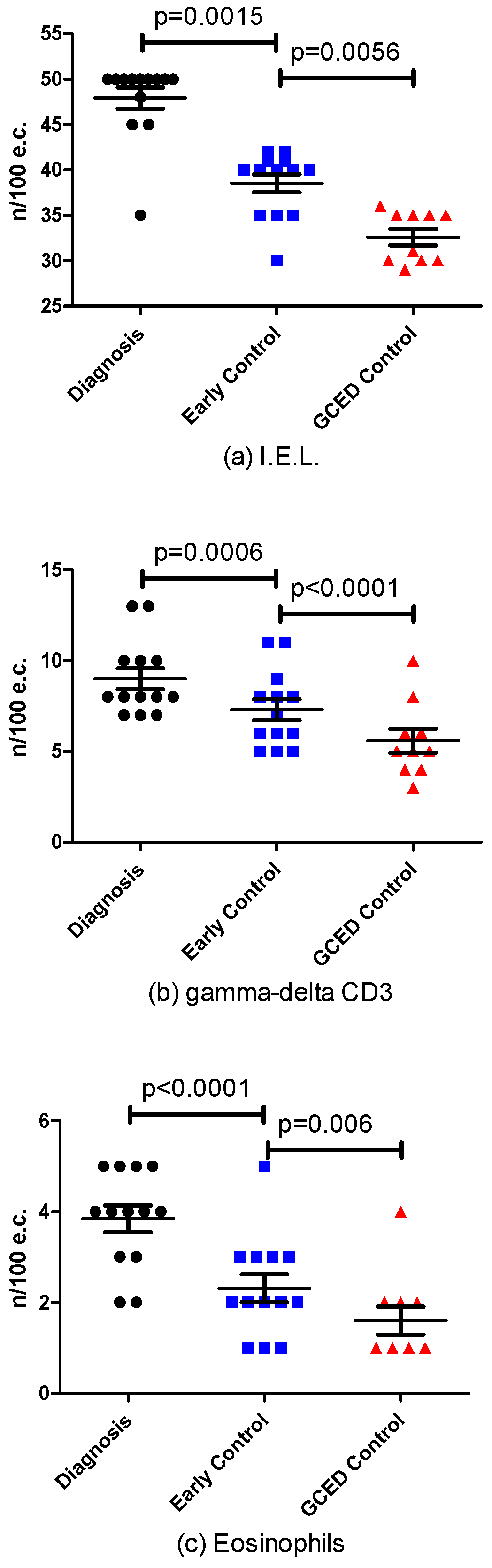
3.2. Effect of GCED: Cohort A
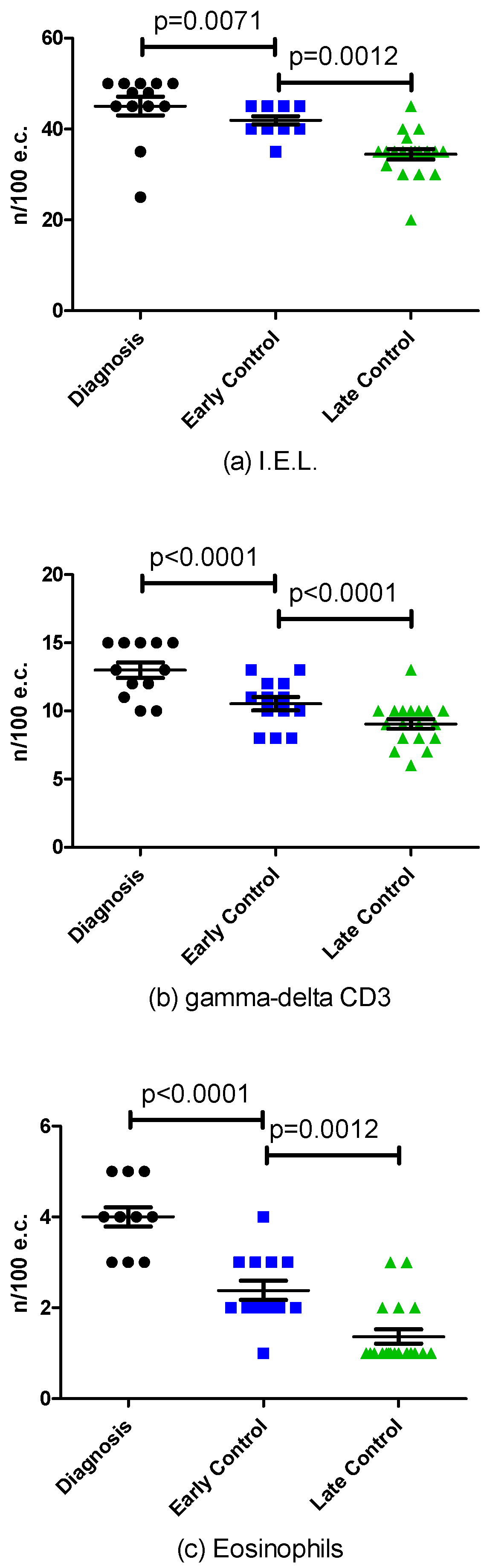
3.3. Effect of Long Term GFD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Marsh, M.N. Gluten, major histocompatibility complex and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity (celiac sprue). Gastroenterology 1992, 102, 330–354. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Volgelsang, H. The histopathology of celiac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Villanacci, V. Coeliac Disease. Some considerations on the histological classification. J. Clin. Pathol. 2005, 58, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Villanacci, V.; Zambelli, C.; Milione, M.; Luinetti, O.; Vindigni, C.; Chioda, C.; Albarello, L.; Bartolini, D.; Donato, F. Comparison of the interobserver reproducibility with different histologic criteria used in celiac disease. Clin. Gastroenterol. Hepatol. 2007, 5, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Villanacci, V.; Ceppa, P.; Tavani, E.; Vindigni, C.; Volta, U.; Gruppo Italiano Patologi Apparato Digerente (GIPAD); Società Italiana di Anatomia Patologica e Citopatologia Diagnostica/International Academy of Pathology, Italian division (SIAPEC/IAP). Coeliac disease: The histology report. Dig. Liver. Dis. 2011, 43, S385–S395. [Google Scholar] [CrossRef]
- Wahab, P.J.; Meijer, J.W.; Mulder, C.J. Histologic follow-up of people with celiac disease on a gluten free diet: Slow and incomplete recovery. Am. J. Clin. Pathol. 2002, 118, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Lanzini, A.; Lanzarotto, F.; Villanacci, V.; Mora, A.; Bertolazzi, S.; Turini, D.; Carella, G.; Malagoli, A.; Ferrante, G.; Cesana, B.M.; et al. Complete recovery of intestinal mucosa occurs very rarely in adult celiac patients despite adherence to gluten free diet. Aliment. Pharmacol. Ther. 2009, 29, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Ciacci, C.; Cirillo, M.; Cavallaro, R.; Mazzacca, G. Long term follow-up of celiac adults on gluten-free diet: Prevalence and correlates of intestinal damage. Digestion 2002, 66, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Lo, W.; Memeo, L.; Rotterdam, H.; Green, P.H. Duodenal histology in patients with celiac disease after treatment with a gluten-free diet. Gastrointest Endosc. 2003, 57, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Bardella, M.T.; Velio, P.; Cesana, B.M.; Prampolini, L.; Casella, G.; Di Bella, C.; Lanzini, A.; Gambarotti, M.; Bassotti, G.; Villanacci, V. Coelic disease: A histological follow-up study. Histopathology 2007, 50, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Koning, F.; Mol, M.; Mearin, M.L. The million-dollar question: Is gluten-free food safe for patients with celiac disease? Am. J. Clin. Nutr. 2013, 97, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Fabiani, E.; Iacono, G.; D’Agate, C.; Francavilla, K.; Biagi, F.; Volta, U.; Accomando, S.; Picarelli, A.; De Vitis, I.; et al. A prospective, double-blind, placebo-controlled trial to estabilish a safe gluten threshold for patients with celiac disease. Am. J. Clin. Nutr. 2007, 85, 160–166. [Google Scholar] [PubMed]
- Biagi, F.; Campanella, J.; Martucci, S.; Pezzimenti, D.; Ciclitira, P.J.; Ellis, H.J.; Corazza, G.R. A milligram of gluten a day keeps the mucosal recovery away: A case report. Nutr. Rev. 2004, 62, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Akobneg, A.K.; Thomas, A.G. Systematic review: Tolerable amount of gluten for people with celiac disease. Aliment. Pharmacol. Ther. 2008, 27, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Hollon, J.R.; Cureton, P.A.; Martin, M.L.; Puppa, E.L.; Fasano, A. Trace gluten contamination may play a role in mucosal and clinical recovery in a subgroup of diet-adherent non-responsive celiac disease patients. BMC Gastroenterol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS-A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Zanini, B.; Ricci, C.; Bandera, F.; Caselani, F.; Magni, A.; Laronga, A.M.; Lanzini, A. Incidence of post-infectious irritable bowel syndrome and functional intestinal disorders following a water-borne viral gastroenteritis outbreak. Am. J. Gastroenterol. 2012, 107, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Zanini, B.; Lanzarotto, F.; Mora, A.; Bertolazzi, F.; Turini, D.; Cesana, B.; Donato, F.; Ricci, C.; Lonati, F.; Vassallo, F.; et al. Five years time course of celiac disease serology during gluten free diet: Results of a community based “CD.Watch” program. Dig. Liv. Dis. 2010, 42, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Lonardi, S.; Villanacci, V.; Lorenzi, L.; Lanzini, A.; Lanzarotto, F.; Carabellese, N.; Volta, U.; Facchetti, F. Anti-TCR gamma antibody in celiac disease. The value of count on formalin-fixed paraffin-embedded biopsies. Virchows Arch. 2013, 463, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Saukkonen, J.; Kaikinen, K.; Koivisto, A.M.; Maki, M.; Laurila, K.; Sievänen, H.; Collin, P.; Kurppa, K. Clinical characteristics and the dietary response in celiac disease patients presenting with or without anemia. J. Clin. Gastroenterol. 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T.; Lee, A.R.; Grace, T. Gluten contamination of grains, seeds, and flours in the United States: A pilot study. J. Am. Diet. Assoc. 2010, 110, 937–940. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.; Schuppan, D.; Pallav, K.; Najarian, R.; Goldsmith, J.D.; Hansen, J.; Kabbani, T.; Dennis, M.; Kelly, C.P. Kinetics of the histological, serological and symptomatic responses to gluten challenge in adults with coeliac disease. Gut 2013, 62, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Sanchez, J.P.; Cabrera-Chavez, F.; de la Barca, A.M. Maize prolamins could induce a gluten-like cellular immune response in some celiac disease patients. Nutrients 2013, 5, 4174–4183. [Google Scholar] [CrossRef] [PubMed]
- Galipeau, H.J.; McCarville, J.L.; Huebener, S.; Litwin, O.; Meisel, M.; Jabri, B.; Sanz, Y.; Murray, J.A.; Jordana, M.; Alaedini, A.; et al. Intestinal microbiota modulates gluten-induced immunopathology in humanized mice. Am. J. Pathol. 2015, 185, 2969–2982. [Google Scholar] [CrossRef] [PubMed]
- Mowat, A.M.; Agace, W.W. Regional specialization within the intestinal immune system. Nat. Rev. Immunol. 2014, 14, 667–685. [Google Scholar] [CrossRef] [PubMed]
- Verdu, E.F.; Galipeau, H.J.; Jabri, B. Novel players in coeliac disease pathogenesis: Role of the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Decker, E.; Hornef, M.; Stockinger, S. Cesarean delivery is associated with celiac disease but not inflammatory bowel disease in children. Gut Microb. 2011, 2, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, A.; Persson, L.A.; Nystrom, L.; Ascher, H.; Cavell, B.; Danielsson, L.; Dannaeus, A.; Lindberg, T.; Lindquist, B.; Stenhammar, L.; et al. Epidemic of coeliac disease in Swedish children. Acta. Paediatr. 2000, 89, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Emilsson, L.; Magnus, M.C.; Stordal, K. Perinatal risk factors for development of celiac disease in children, based on the prospective Norwegian Mother and Child Cohort Study. Clin. Gastroenterol. Hepatol. 2015, 13, 921–922. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Castellaneta, S.; Francavilla, R.; Pulvirenti, A.; Tonutti, E.; Amarri, S.; Barbato, M.; Barbera, C.; Barera, G.; Bellantoni, A.; et al. Introduction of gluten, HLA status, and the risk of celiac disease in children. N. Engl. J. Med. 2014, 371, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Vriezinga, S.L.; Auricchio, R.; Bravi, E.; Castillejo, G.; Chmielewska, A.; Crespo, E.P.; Kolacek, S.; Koletzko, S.; Korponay-Szabo, I.R.; Mummert, E.; et al. Randomized feeding intervention in infants at high risk for celiac disease. N. Engl. J. Med. 2014, 371, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Collado, M.C.; Donat, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Specific duodenal and faecal bacterial groups associated with paediatric coeliac disease. J. Clin. Pathol. 2009, 62, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Nadal, I.; Donat, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Imbalance in the composition of the duodenal microbiota of children with coeliac disease. J. Med. Microbiol. 2007, 56, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, E.; Donat, E.; Ribes-Koninckx, C.; Fernandez-Murga, M.L.; Sanz, Y. Duodenal-mucosal bacteria associated with celiac disease in children. Appl. Environ. Microbiol. 2013, 79, 5472–5479. [Google Scholar] [CrossRef] [PubMed]
- Wacklin, P.; Kaukinen, K.; Tuovinen, E.; Collin, P.; Lindfors, K.; Partanen, J.; Maki, M.; Matto, J. The duodenal microbiota composition of adult celiac disease patients is associated with the clinical manifestation of the disease. Inflamm. Bowel. Dis. 2013, 19, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Nistal, E.; Caminero, A.; Herran, A.R.; Arias, L.; Vivas, S.; de Morales, J.M.; Calleja, S.; de Miera, L.E.; Arroyo, P.; Casqueiro, J. Differences of small intestinal bacteria populations in adults and children with/without celiac disease: Effect of age, gluten diet, and disease. Inflamm. Bowel. Dis. 2012, 18, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Zoetendal, E.G.; Raes, J.; van den Bogert, B.; Arumugam, M.; Booijink, C.C.; Troost, F.J.; Bork, P.; Wels, M.; de Vos, W.M.; Kleerebezem, M. The human small intestinal microbiota is driven by rapid uptake and conversion of simple carbohydrates. ISME J. 2012, 6, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- Wacklin, P.; Laurikka, P.; Lindfors, K.; Collin, P.; Salmi, T.; Lahdeaho, M.L.; Saavalainen, P.; Maki, M.; Matto, J.; Kurppa, K.; et al. Altered duodenal microbiota composition in celiac disease patients suffering from persistent symptoms on a long-term gluten-free diet. Am. J. Gastroenterol. 2014, 109, 1933–1941. [Google Scholar] [CrossRef] [PubMed]
- Tjellstrom, B.; Stenhammar, L.; Sundqvist, T.; Falth-Magnusson, K.; Hollen, E.; Magnusson, K.E.; Norin, E.; Midtvedt, T.; Hogberg, L. The effects of oats on the function of gut microflora in children with coeliac disease. Aliment. Pharmacol. Ther. 2014, 39, 1156–1160. [Google Scholar] [CrossRef] [PubMed]
- Tuire, I.; Marja-Leena, L.; Teea, S.; Katri, H.; Jukka, P.; Päivi, S.; Heini, H.; Markku, M.; Pekka, C.; Katri, K. Persistent duodenal intraepithelial lymphocytosis despite a long-term strict gluten-free diet in celiac disease. Am. J. Gastroenterol. 2012, 107, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Evans, K.E.; Hopper, A.D.; Smillie, D.M.; Sanders, D.S. A prospective study into the aetiology of lymphocytic duodenosis. Aliment. Pharmacol. Ther. 2010, 32, 1392–1397. [Google Scholar] [CrossRef] [PubMed]
- Pekki, H.; Kurppa, K.; Maki, M.; Huhtala, H.; Sievanen, H.; Laurila, K.; Collin, P.; Kaukinen, K. Predictors and significance of incomplete mucosal recovery in celiac disease after 1 year on a Gluten-Free diet. Am. J. Gastroenterol. 2015, 110, 1078–1085. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cohort A | Cohort B | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Gender | Age | Marsh | NC | n | Gender | Age | Marsh | NC |
| 1 | M | 23 | 3a | B1 | 1 | F | 38 | 3c | B2 |
| 2 | M | 30 | 3c | B2 | 2 | F | 34 | 3c | B2 |
| 3 | F | 22 | 3c | B2 | 3 | M | 38 | 3c | B2 |
| 4 | F | 30 | 3a | B1 | 4 | M | 46 | 3c | B2 |
| 5 | F | 30 | 3a | B1 | 5 | F | 45 | 3c | B2 |
| 6 | F | 43 | 3b | B1 | 6 | F | 22 | 3a | B1 |
| 7 | F | 47 | 3b | B1 | 7 | F | 46 | 3a | B1 |
| 8 | F | 49 | 3c | B2 | 8 | F | 19 | 3 | B1 |
| 9 | F | 26 | 3a | B1 | 9 | F | 25 | 3c | B2 |
| 10 | F | 68 | 3b | B1 | 10 | F | 42 | 3b | B1 |
| 11 | M | 44 | 3a | B1 | 11 | F | 20 | 3b | B1 |
| 12 | F | 29 | 3c | B2 | 12 | F | 44 | 2 | A |
| 13 | M | 58 | 2 | A | 13 | M | 32 | 3b | B1 |
| 14 | M | 29 | 3b | B1 | |||||
| 15 | F | 26 | 3c | B2 | |||||
| 16 | F | 30 | 3c | B2 | |||||
| 17 | F | 26 | 3c | B2 | |||||
| 18 | F | 52 | 3b | B1 | |||||
| 19 | F | 38 | 3c | B2 | |||||
| Time of Diagnosis | Early Control (after 1 Year GFD) | GCED Control (after 3 Months of Restricted Diet) | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | BMI | Ttg | VH/CD | IEL | γδ | Eos | Months | BMI | Ttg | Marsh | NC | VH/CD | IEL | γδ | Eos | Days | BMI | Marsh | NC | VH/CD | IEL | γδ | Eos |
| 1 | 19.3 | >100/16 | <2 | 35 | 8 | 3 | 13 | 19.0 | 13/16 | 2 | A | ≥2 | 30 | 7 | 2 | 95 | 18.5 | 2 | A | ≥2 | 29 | 6 | 1 |
| 2 | 38.0 | >100/16 | <2 | 50 | 10 | 4 | 13 | 36.3 | 5.1/16 | 2 | A | ≥2 | 41 | 8 | 2 | 109 | 32.4 | 2 | A | ≥2 | 35 | 5 | 1 |
| 3 | 19.7 | >100/16 | <2 | 50 | 10 | 4 | 13 | 19.7 | 8.2/16 | 2 | A | ≥2 | 41 | 8 | 2 | d.o. | - | - | - | - | - | - | - |
| 4 | 18.6 | 7.5/7 | <2 | 48 | 8 | 3 | 14 | 19.0 | 3.4/16 | 2 | A | ≥2 | 40 | 5 | 2 | 92 | 18.4 | A | ≥2 | 35 | 4 | 1 | |
| 5 | 21.1 | >100/16 | <2 | 50 | 13 | 5 | 14 | 23.5 | 4.2/16 | 2 | A | ≥2 | 40 | 11 | 3 | 79 | 23.0 | 2 | A | ≥2 | 36 | 10 | 2 |
| 6 | 19.4 | 8.1/7 | <2 | 50 | 13 | 5 | 16 | 20.0 | 5./16 | 2 | A | ≥2 | 40 | 11 | 3 | d.o. | - | - | - | - | - | - | - |
| 7 | 28.3 | >100/16 | <2 | 50 | 8 | 2 | 13 | 31.4 | 7.7/16 | 2 | A | ≥2 | 42 | 5 | 1 | 85 | 29.2 | 2 | A | ≥2 | 35 | 3 | 1 |
| 8 | 19.8 | 18/16 | <2 | 50 | 8 | 2 | 15 | 19.2 | 5./16 | 2 | A | ≥2 | 42 | 5 | 1 | d.o. | - | - | - | - | - | - | - |
| 9 | 25.0 | 11.6/16 | <2 | 45 | 10 | 5 | 15 | 24.6 | 3.2/16 | 2 | A | ≥2 | 35 | 8 | 3 | 109 | 24.1 | 2 | A | ≥2 | 30 | 6 | 2 |
| 10 | 20.0 | 29/16 | <2 | 45 | 7 | 5 | 13 | 20.5 | 3.0/16 | 2 | A | ≥2 | 35 | 6 | 3 | 92 | 20.9 | 2 | A | ≥2 | 31 | 5 | 2 |
| 11 | 22.7 | 80/16 | <2 | 50 | 8 | 4 | 14 | 22.3 | 4./16 | 2 | A | ≥2 | 40 | 6 | 2 | 95 | 21.7 | 2 | A | ≥2 | 30 | 5 | 1 |
| 12 | 19.3 | >100/16 | <2 | 50 | 7 | 4 | 15 | 19.7 | 7.9/16 | 2 | A | ≥2 | 40 | 6 | 1 | 99 | 20.4 | 2 | A | ≥2 | 35 | 4 | 1 |
| 13 | 22.9 | 8.8/16 | <2 | 50 | 7 | 4 | 29 | 22.9 | 5.9/16 | 2 | A | ≥2 | 35 | 9 | 5 | 95 | 20.9 | 2 | A | ≥2 | 30 | 8 | 4 |
| Time of Diagnosis | Early Control (after 1 Year GFD) | Late Control (after Longer Period of GFD) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | VH/CD | IEL | γδ | Eos | Months | Marsh | NC | VH/CD | IEL | γδ | Eos | Months | Marsh | NC | VH/CD | IEL | γδ | Eos |
| 1 | <2 | 45 | 10 | 3 | 13 | 2 | A | ≥2 | 40 | 8 | 2 | 103 | 2 | A | ≥2 | 35 | 6 | 1 |
| 2 | <2 | 50 | 15 | 4 | 12 | 2 | A | ≥2 | 45 | 12 | 3 | 54 | 2 | A | ≥2 | 35 | 10 | 2 |
| 3 | <2 | 48 | 12 | 4 | 13 | 2 | A | ≥2 | 45 | 10 | 2 | 102 | 2 | A | ≥2 | 40 | 8 | 1 |
| 4 | <2 | 48 | 13 | 5 | 16 | 2 | A | ≥2 | 45 | 11 | 3 | 78 | 2 | A | ≥2 | 40 | 10 | 1 |
| 5 | <2 | 45 | 10 | 3 | 14 | 2 | A | ≥2 | 40 | 8 | 2 | 67 | 2 | A | ≥2 | 38 | 7 | 1 |
| 6 | n.a | >25 | n.a | n.a | 12 | 2 | A | n.a | >25 | n.a | n.a | 204 | 2 | A | ≥2 | 35 | 10 | 1 |
| 7 | n.a | >25 | n.a | n.a | 12 | 2 | A | ≥2 | 45 | 10 | 4 | 54 | 1 | A | ≥2 | 35 | 8 | 3 |
| 8 | <2 | 50 | 15 | 4 | 12 | 2 | A | n.a | >25 | n.a | n.a | 216 | 2 | A | ≥2 | 45 | 13 | 1 |
| 9 | <2 | 50 | 15 | 4 | 12 | 2 | A | ≥2 | 45 | 13 | 3 | 48 | 1 | A | ≥2 | 20 | 8 | 1 |
| 10 | n.a | >25 | n.a | n.a | 12 | 2 | A | ≥2 | 40 | 11 | 2 | 63 | 2 | A | ≥2 | 35 | 9 | 1 |
| 11 | n.a | >25 | n.a | n.a | 24 | 2 | A | ≥2 | 40 | 8 | 1 | 85 | 2 | A | ≥2 | 35 | 7 | 1 |
| 12 | ≥2 | 35 | 11 | 5 | 15 | 2 | A | n.a | >25 | n.a | n.a | 80 | 2 | A | ≥2 | 32 | 9 | 3 |
| 13 | n.a | >25 | n.a | n.a | 12 | 2 | A | n.a | >25 | n.a | n.a | 60 | 2 | A | ≥2 | 35 | 9 | 2 |
| 14 | <2 | 45 | 15 | 4 | 12 | 1 | A | n.a | >25 | n.a | n.a | 63 | 2 | A | ≥2 | 30 | 10 | 1 |
| 15 | <2 | 50 | 13 | 3 | 16 | 2 | A | ≥2 | 45 | 11 | 2 | 90 | 2 | A | ≥2 | 35 | 10 | 1 |
| 16 | <2 | 50 | 12 | 5 | 13 | 2 | A | ≥2 | 40 | 10 | 3 | 116 | 2 | A | ≥2 | 35 | 9 | 2 |
| 17 | n.a | >25 | n.a | n.a | 36 | 2 | A | n.a | n.a | n.a | n.a | 137 | 2 | A | ≥2 | 30 | 9 | 1 |
| 18 | n.a | >25 | n.a | n.a | 22 | 2 | A | ≥2 | 35 | 13 | 2 | 85 | 2 | A | ≥2 | 30 | 10 | 1 |
| 19 | <2 | 45 | 15 | 4 | 19 | 2 | A | ≥2 | 40 | 12 | 2 | 113 | 0 | 0 | ≥2 | 35 | 10 | 1 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanini, B.; Marullo, M.; Villanacci, V.; Salemme, M.; Lanzarotto, F.; Ricci, C.; Lanzini, A. Persistent Intraepithelial Lymphocytosis in Celiac Patients Adhering to Gluten-Free Diet Is Not Abolished Despite a Gluten Contamination Elimination Diet. Nutrients 2016, 8, 525. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090525
Zanini B, Marullo M, Villanacci V, Salemme M, Lanzarotto F, Ricci C, Lanzini A. Persistent Intraepithelial Lymphocytosis in Celiac Patients Adhering to Gluten-Free Diet Is Not Abolished Despite a Gluten Contamination Elimination Diet. Nutrients. 2016; 8(9):525. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090525
Chicago/Turabian StyleZanini, Barbara, Monica Marullo, Vincenzo Villanacci, Marianna Salemme, Francesco Lanzarotto, Chiara Ricci, and Alberto Lanzini. 2016. "Persistent Intraepithelial Lymphocytosis in Celiac Patients Adhering to Gluten-Free Diet Is Not Abolished Despite a Gluten Contamination Elimination Diet" Nutrients 8, no. 9: 525. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090525