Beverage Consumption Patterns among Norwegian Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Assessment of Beverage Intake
2.3. Meal Types and Categorization of Beverage Types
2.4. Background Variables
2.5. Days of the Week
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Patterns of Beverage Consumption Related to Meals
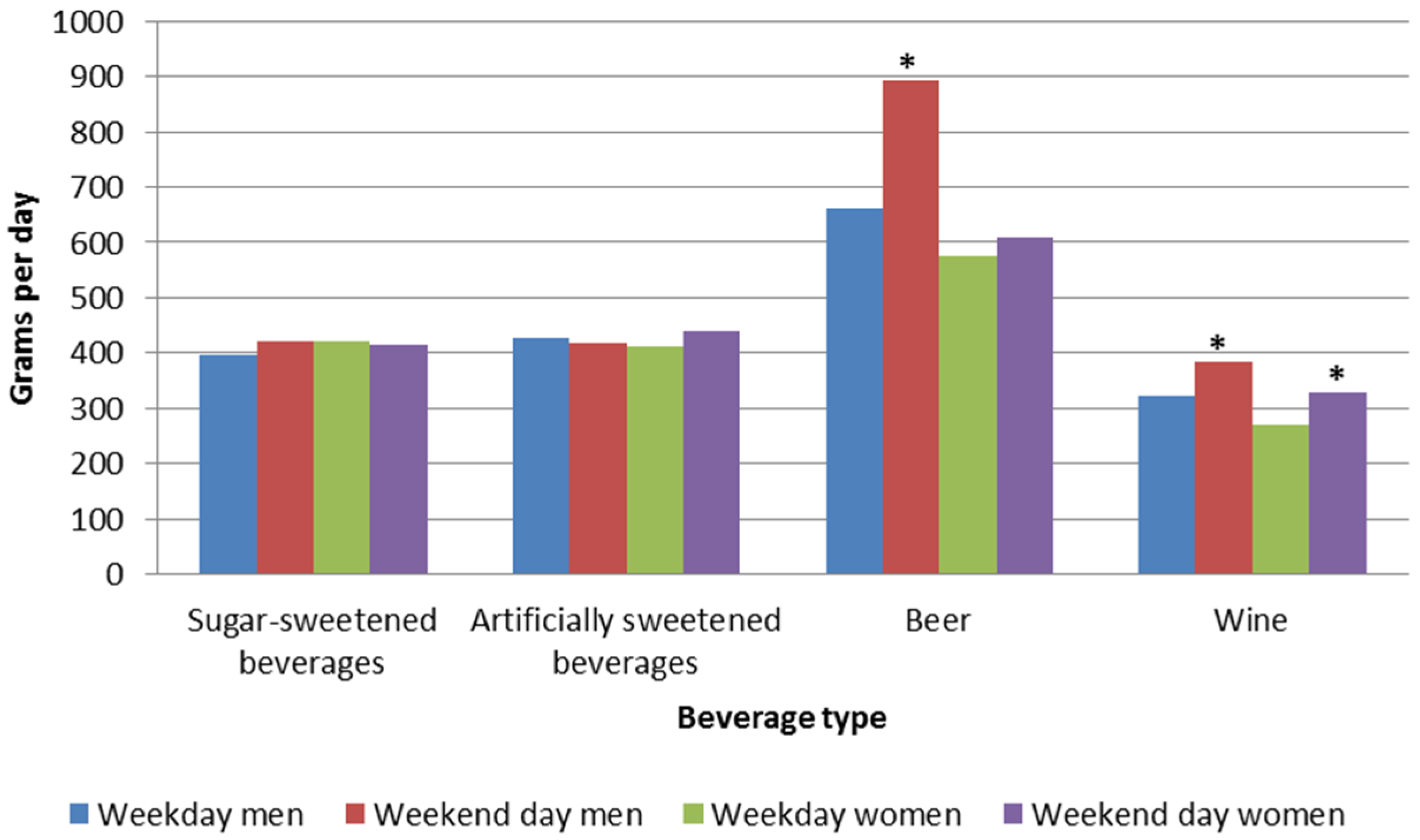
3.3. Patterns of Beverage Consumption on Weekdays vs. Weekend Days
3.4. Background Variables Associated with Intake of Different Types of Beverages
4. Discussion
4.1. Patterns of Beverage Consumption Related to Meals
4.2. Patterns of Beverage Consumption on Weekdays Compared to Weekend Days
4.3. Background Variables Associated with the Intake of Different Types of Beverages
4.4. Strengths and Limitations
4.5. Practical Implications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kerver, J.M.; Yang, E.J.; Obayashi, S.; Bianchi, L.; Song, W.O. Meal and snack patterns are associated with dietary intake of energy and nutrients in US adults. J. Am. Diet. Assoc. 2006, 106, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Pobocik, R.S.; Trager, A.; Monson, L.M. Dietary patterns and food choices of a population sample of adults on Guam. Asia Pac. J. Clin. Nutr. 2008, 17, 94–100. [Google Scholar] [PubMed]
- Venci, B.; Hodac, N.; Lee, S.Y.; Shidler, M.; Krikorian, R. Beverage consumption patterns and micronutrient and caloric intake from beverages in older adults with mild cognitive impairment. J. Nutr. Gerontol. Geriatr. 2015, 34, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Coudray, B. The contribution of dairy products to micronutrient intakes in France. J. Am. Coll. Nutr. 2011, 30, 410S–414S. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The contribution of milk and milk products to micronutrient density and affordability of the US Diet. J. Am. Coll. Nutr. 2011, 30, 422S–428S. [Google Scholar] [CrossRef] [PubMed]
- Huth, P.J.; Fulgoni, V.L.; Keast, D.R.; Park, K.; Auestad, N. Major food sources of calories, added sugars, and saturated fat and their contribution to essential nutrient intakes in the US Diet: Data from the national health and nutrition examination survey (2003–2006). Nutr. J. 2013, 12, 116. [Google Scholar] [CrossRef] [PubMed]
- Vissers, P.A.; Streppel, M.T.; Feskens, E.J.; de Groot, L.C. The contribution of dairy products to micronutrient intake in The Netherlands. J. Am. Coll. Nutr. 2011, 30, 415S–421S. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Directorate of Health. Utviklingen I Norsk Kosthold 2015. Available online: https://helsedirektoratet.no/Lists/Publikasjoner/Attachments/1021/Utviklingen-i-norsk-kosthold-2015-IS-2382.pdf (accessed on 10 December 2015).
- Hu, F.B.; Malik, V.S. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: Epidemiologic evidence. Physiol. Behav. 2010, 100, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [PubMed]
- Woodward-Lopez, G.; Kao, J.; Ritchie, L. To what extent have sweetened beverages contributed to the obesity epidemic? Public Health Nutr. 2011, 14, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S. Sugar-sweetened soft drinks and obesity: A systematic review of the evidence from observational studies and interventions. Nutr. Res. Rev. 2008, 21, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Mattes, R.D.; Shikany, J.M.; Kaiser, K.A.; Allison, D.B. Nutritively sweetened beverage consumption and body weight: A systematic review and meta-analysis of randomized experiments. Obes. Rev. 2011, 12, 346–365. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Baliunas, D.; Borges, G.L.; Graham, K.; Irving, H.; Kehoe, T.; Parry, C.D.; Patra, J.; Popova, S.; Poznyak, V. The relation between different dimensions of alcohol consumption and burden of disease: An overview. Addiction 2010, 105, 817–843. [Google Scholar] [CrossRef] [PubMed]
- Holman, C.; English, D.R.; Milne, E.; Winter, M.G. Meta-analysis of alcohol and all-cause mortality: A validation of nhmrc recommendations. Med. J. Aust. 1996, 164, 141–145. [Google Scholar] [PubMed]
- Knott, C.S.; Coombs, N.; Stamatakis, E.; Biddulph, J.P. All cause mortality and the case for age specific alcohol consumption guidelines: Pooled analyses of up to 10 population based cohorts. BMJ 2015, 350, h384. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, T.; Zhao, J.; Panwar, S.; Roemer, A.; Naimi, T.; Chikritzhs, T. Do “moderate” drinkers have reduced mortality risk? A systematic review and meta-analysis of alcohol consumption and all-cause mortality. J. Stud. Alcohol Drugs 2016, 77, 185–198. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Directorate of Health. Kostråd for å Fremme Folkehelsen og Forebygge Kroniske Sykdommer: Metodologi og Vitenskapelig Kunnskapsgrunnlag. Available online: https://fido.nrk.no/5070725ea6c90cbb7d02b12dd53955b754904a13a5ba80e83464533b457f8e0f/Kosthold.pdf (accessed on 10 December 2015).
- Food and Agriculture Organization of the United Nations. Food-Based Dietary Guidelines. Available online: http://www.fao.org/nutrition/nutrition-education/food-dietary-guidelines/en/ (accessed on 8 January 2016).
- Kit, B.K.; Fakhouri, T.H.; Park, S.; Nielsen, S.J.; Ogden, C.L. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am. J. Clin. Nutr. 2013, 98, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Ni Mhurchu, C.; Jebb, S.A.; Popkin, B.M. Patterns and trends of beverage consumption among children and adults in great britain, 1986–2009. Br. J. Nutr. 2012, 108, 536–551. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Directorate of Health. Anbefalinger om Kosthold, Ernæring og Fysisk Aktivitet. Available online: https: //helsedirektoratet.no/publikasjoner/anbefalinger-om-kosthold-ernering-og-fysisk-aktivitet (accessed on 8 January 2016).
- Holmback, I.; Ericson, U.; Gullberg, B.; Wirfalt, E. Five meal patterns are differently associated with nutrient intakes, lifestyle factors and energy misreporting in a sub-sample of the Malmo Diet and Cancer Cohort. Food Nutr. Res. 2009. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J.M.; Hulshof, K.F.; Gibney, M.J. Eating patterns—Temporal distribution, converging and diverging foods, meals eaten inside and outside of the home—Implications for developing FBDG. Public Health Nutr. 2001, 4, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Myhre, J.B.; Loken, E.B.; Wandel, M.; Andersen, L.F. Meal types as sources for intakes of fruits, vegetables, fish and whole grains among Norwegian adults. Public Health Nutr. 2015, 18, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [PubMed]
- Hjartaker, A.; Lund, E. Relationship between dietary habits, age, lifestyle, and socio-economic status among adult Norwegian women. The Norwegian Women and Cancer Study. Eur. J. Clin. Nutr. 1998, 52, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Thelle, D.S.; Solvoll, K.; Bjorneboe, G.E.; Drevon, C.A. Healthy dietary habits in relation to social determinants and lifestyle factors. Br. J. Nutr. 1999, 81, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Powell, L.M. Consumption patterns of sugar-sweetened beverages in the United States. J. Acad. Nutr. Diet. 2013, 113, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Mullie, P.; Aerenhouts, D.; Clarys, P. Demographic, socioeconomic and nutritional determinants of daily versus non-daily sugar-sweetened and artificially sweetened beverage consumption. Eur. J. Clin. Nutr. 2012, 66, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Blanck, H.M.; Sherry, B.; Brener, N.; O’Toole, T. Factors associated with sugar-sweetened beverage intake among United States high school students. J. Nutr. 2012, 142, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Rehm, C.D.; Matte, T.D.; Van Wye, G.; Young, C.; Frieden, T.R. Demographic and behavioral factors associated with daily sugar-sweetened soda consumption in New York City adults. J. Urban Health 2008, 85, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Myhre, J.B.; Loken, E.B.; Wandel, M.; Andersen, L.F. Eating location is associated with the nutritional quality of the diet in Norwegian adults. Public Health Nutr. 2014, 17, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Food Safety Authority; Norwegian Directorate of Health; University of Oslo. The Norwegian Food Composition Table. Available online: http://www.matportalen.no/verktoy/the_norwegian_food_composition_table/old_tables (accessed on 23 October 2015).
- Kjærnes, U. Eating Patterns: A Day in the Lives of Nordic Peoples; National Instititute for Consumer Research: Lysaker, Norway, 2001. [Google Scholar]
- Sieri, S.; Agudo, A.; Kesse, E.; Klipstein-Grobusch, K.; San-Jose, B.; Welch, A.A.; Krogh, V.; Luben, R.; Allen, N.; Overvad, K.; et al. Patterns of alcohol consumption in 10 European countries participating in the European Prospective Investigation Into Cancer and Nutrition (EPIC) project. Public Health Nutr. 2002, 5, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Thornton, S.N.; Hebel, P.; Denizeau, M.; Tahiri, M. A study of fluid intake from beverages in a sample of healthy French children, adolescents and adults. Eur. J. Clin. Nutr. 2010, 64, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.; Shirreffs, S.M. Beverage consumption habits “24/7” among British adults: Association with total water intake and energy intake. Nutr. J. 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- An, R. Weekend-weekday differences in diet among US Adults, 2003–2012. Ann. Epidemiol. 2016, 26, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Rothausen, B.W.; Matthiessen, J.; Hoppe, C.; Brockhoff, P.B.; Andersen, L.F.; Tetens, I. Differences in Danish children’s diet quality on weekdays v. Weekend days. Public Health Nutr. 2012, 15, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Lillegaard, I.T.L.; Øverby, N.; Andersen, L.F. Er det forskjell på hva barn spiser på hverdager og i helgen. Barn 2003, 2, 89–98. [Google Scholar]
- Bjelland, M.; Lien, N.; Grydeland, M.; Bergh, I.H.; Anderssen, S.A.; Ommundsen, Y.; Klepp, K.I.; Andersen, L.F. Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (HEalth in Adolescents) study. Public Health Nutr. 2011, 14, 2156–2165. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I.; Atchison, E.A. Intakes of plain water, moisture in foods and beverages, and total water in the adult US population—Nutritional, meal pattern, and body weight correlates: National Health and Nutrition Examination Surveys 1999–2006. Am. J. Clin. Nutr. 2009, 90, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Beverage consumption of Canadian adults. Health Rep. 2008, 19, 23–29. [Google Scholar] [PubMed]
- Sousa, A.G.; da Costa, T.H. Usual coffee intake in Brazil: Results from the national dietary survey 2008–9. Br. J. Nutr. 2015, 113, 1615–1620. [Google Scholar] [CrossRef] [PubMed]
- De Castro, J.M.; Taylor, T. Smoking status relationships with the food and fluid intakes of free-living humans. Nutrition 2008, 24, 109–119. [Google Scholar] [CrossRef] [PubMed]
- McPhillips, J.B.; Eaton, C.B.; Gans, K.M.; Derby, C.A.; Lasater, T.M.; McKenney, J.L.; Carleton, R.A. Dietary differences in smokers and nonsmokers from two southeastern New England communities. J. Am. Diet. Assoc. 1994, 94, 287–292. [Google Scholar] [CrossRef]
- Whichelow, M.J.; Erzinclioglu, S.W.; Cox, B.D. A comparison of the diets of non-smokers and smokers. Br. J. Addict. 1991, 86, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.C.; Wang, C.J.; Cheng, S.H.; Sun, Z.J.; Chen, P.S.; Lee, C.T.; Lin, S.H.; Yang, Y.K.; Yang, Y.C. Tea-drinking habit among new university students: Associated factors. Kaohsiung J. Med. Sci. 2014, 30, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.L.; Han, B.; Cohen, D.A. Associations between eating occasions and places of consumption among adults. Appetite 2015, 87, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Mullie, P.; Clarys, P.; Hulens, M.; Vansant, G. Dietary patterns and socioeconomic position. Eur. J. Clin. Nutr. 2010, 64, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Leon-Munoz, L.M.; Galan, I.; Donado-Campos, J.; Sanchez-Alonso, F.; Lopez-Garcia, E.; Valencia-Martin, J.L.; Guallar-Castillon, P.; Rodriguez-Artalejo, F. Patterns of alcohol consumption in the older population of Spain, 2008–2010. J. Acad. Nutr. Diet. 2015, 115, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Myhre, J.B.; Loken, E.B.; Wandel, M.; Andersen, L.F. The contribution of snacks to dietary intake and their association with eating location among Norwegian adults—Results from a cross-sectional dietary survey. BMC Public Health 2015, 15, 369. [Google Scholar] [CrossRef] [PubMed]
- Guelinckx, I.; Ferreira-Pego, C.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Intake of water and different beverages in adults across 13 countries. Eur. J. Nutr. 2015, 54, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Ruano, C.; Serra-Majem, L. Validation of beverage intake methods vs. Hydration biomarkers; a short review. Nutr. Hosp. 2013, 28, 1815–1819. [Google Scholar] [PubMed]
- Poppitt, S.D.; Swann, D.; Black, A.E.; Prentice, A.M. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, T.; Donath, S.; Cooper-Stanbury, M.; Chikritzhs, T.; Catalano, P.; Mateo, C. Under-reporting of alcohol consumption in household surveys: A comparison of quantity-frequency, graduated-frequency and recent recall. Addiction 2004, 99, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Graubard, B.I.; Kahle, L.L.; Subar, A.F.; Cleveland, L.E.; Ballard-Barbash, R. Low energy reporters vs others: A comparison of reported food intakes. Eur. J. Clin. Nutr. 2000, 54, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Nyholm, M.; Gullberg, B.; Merlo, J.; Lundqvist-Persson, C.; Rastam, L.; Lindblad, U. The validity of obesity based on self-reported weight and height: Implications for population studies. Obesity 2007, 15, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Scribani, M.; Shelton, J.; Chapel, D.; Krupa, N.; Wyckoff, L.; Jenkins, P. Comparison of bias resulting from two methods of self-reporting height and weight: A validation study. JRSM Open 2014. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | |||
|---|---|---|---|---|
| (n = 862) | (n = 925) | |||
| n | % | n | % | |
| Age group (n = 1787) | ||||
| 18–34 years | 199 | 23 | 208 | 22 |
| 35–54 years | 355 | 41 | 461 | 50 |
| 55–70 years | 308 | 36 | 256 | 28 |
| BMI (n = 1756) | ||||
| <25 kg/m2 | 344 | 40 | 544 | 61 |
| ≥25 kg/m2 | 517 | 60 | 351 | 39 |
| Education level (n = 1784) | ||||
| High school, technical school, trade | 432 | 50 | 414 | 45 |
| school or lower | ||||
| University or college | 429 | 50 | 509 | 55 |
| Interest in a healthy diet (n = 1786) | ||||
| No, low or moderate | 447 | 52 | 335 | 36 |
| High or very high | 414 | 48 | 590 | 64 |
| Smoking habits (n = 1787) | ||||
| Non-smokers | 686 | 80 | 724 | 78 |
| Smokers | 176 | 20 | 201 | 22 |
| Breakfast | Lunch | Dinner | Supper | Snack | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (g) | 95% CI | Mean (g) | 95% CI | Mean (g) | 95% CI | Mean (g) | 95% CI | Mean (g) | 95% CI | |
| Water | 120 * | 112, 129 | 128 * | 120, 136 | 266 * | 255, 278 | 73 * | 66, 80 | 476 | 454, 499 |
| Coffee | 121 * | 113, 128 | 76 * | 70, 81 | 24 * | 20, 27 | 18 * | 14, 21 | 282 | 267, 298 |
| Tea men | 36 | 29, 42 | 27 * | 22, 32 | 1 * | NA | 11 * | 8, 15 | 33 | 25, 41 |
| Tea women | 57 * | 49, 64 | 53 * | 46, 60 | 7 * | 4, 10 | 36 * | 31, 41 | 85 | 73, 96 |
| Milk | 125 | 118, 132 | 47 * | 43, 52 | 32 * | 29, 35 | 45 * | 41, 50 | 37 * | 33, 42 |
| Fruit juice | 55 | 50, 59 | 21 * | 18, 24 | 7 * | 6, 9 | 8 * | 6, 10 | 15 * | 13, 17 |
| Sugar sweetened beverages | 3 * | 1, 4 | 12 * | 10, 15 | 50 | 45, 56 | 11 * | 9, 14 | 41 * | 36, 46 |
| Artificially sweetened beverages | 5 * | 4, 7 | 12 * | 10, 15 | 38 * | 34, 43 | 12 * | 10, 15 | 44 | 37, 50 |
| Beer | 0 * | NA | 1 * | NA | 26 * | 19, 33 | 9 * | 5, 12 | 47 | 36, 58 |
| Wine | 0 * | NA | 1 * | NA | 22 | 19, 25 | 6 * | 4, 7 | 17 * | 14, 20 |
| Sugar-Sweetened Beverages | Artificially Sweetened Beverages | Beer | Wine | |||||
|---|---|---|---|---|---|---|---|---|
| % | n | % | n | % | n | % | n | |
| Women | 28.8 | 260 | 26.2 | 242 | 9.2 | 85 | 22.1 | 204 |
| Men | 41.0 | 353 | 22.2 | 191 | 21.1 | 182 | 18.1 | 156 |
| Background Variables | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|
| Water | Milk | Juice | Coffee | Tea | ||||||
| Gender | ||||||||||
| Men | 809 (94) | 1.00 | 737 (86) | 1.00 | 393 (46) | 1.00 | 720 (84) | 1.00 | 242 (28) | 1.00 |
| Women | 900 (97) | 1.92 (1.16–3.19) | 764 (83) | 0.78 (0.54–1.13) | 465 (50) | 1.03 (0.84–1.23) | 731 (79) | 0.69 (0.53–0.90) | 493 (53) | 2.76 (2.24–3.41) |
| Age (years) | ||||||||||
| 18–34 | 397 (98) | 1.00 | 352 (87) | 1.00 | 218 (54) | 1.00 | 263 (65) | 1.00 | 141 (35) | 1.00 |
| 35–54 | 780 (96) | 0.48 (0.23–1.00) | 680 (83) | 0.81 (0.57–1.15) | 409 (50) | 0.87 (0.68–1.12) | 681 (84) | 2.70 (2.0–3.6) | 356 (44) | 1.41 (1.07–1.84) |
| 55–70 | 532 (94) | 0.42 (0.20–0.88) | 469 (83) | 0.78 (0.54–1.13) | 231 (41) | 0.67 (0.51–0.88) | 507 (90) | 4.9 (3.4–7.1) | 238 (42) | 1.62 (1.2–2.2) |
| p trend | 0.028 | 0.207 | 0.003 | <0.001 | 0.002 | |||||
| BMI | ||||||||||
| <25 kg/m2 | 874 (97) | 1.00 | 760 (84) | 1.00 | 496 (55) | 1.00 | 722 (80) | 1.00 | 424 (47) | 1.00 |
| ≥25 kg/m2 | 804 (94) | 0.71 (0.43–1.17) | 718 (84) | 0.98 (0.75–1.29) | 350 (41) | 0.63 (0.51–0.77) | 707 (83) | 0.89 (0.68–1.16) | 297 (35) | 0.70 (0.57–0.87) |
| Education | ||||||||||
| No or lower degree | 790 (93) | 1.00 | 709 (84) | 1.00 | 323 (38) | 1.00 | 670 (79) | 1.00 | 282 (33) | 1.00 |
| University or college | 916 (98) | 2.46 (1.47–4.14) | 789 (84) | 1.00 (0.77–1.30) | 535 (57) | 2.03 (1.67–2.48) | 778 (83) | 1.26 (0.98–1.63) | 451 (48) | 1.58 (1.28–1.95) |
| Interest in healthy diet | ||||||||||
| No, low or moderate | 732 (94) | 1.00 | 649 (83) | 1.00 | 345 (44) | 1.00 | 601 (77) | 1.00 | 254 (33) | 1.00 |
| High or very high | 976 (97) | 1.81 (1.11–2.96) | 851 (85) | 1.21 (0.93–1.58) | 513 (51) | 1.17 (0.96–1.43) | 849 (85) | 1.57 (1.2–2.0) | 481 (48) | 1.46 (1.18–1.80) |
| Smoking habits | ||||||||||
| Non-smokers | 1362 (97) | 1.00 | 1186 (84) | 1.00 | 702 (50) | 1.00 | 1129 (80) | 1.00 | 632 (45) | 1.00 |
| Smokers | 1709 (92) | 0.48 (0.29–0.78) | 315 (84) | 0.97 (0.60–1.02) | 156 (41) | 0.78 (0.61–0.99) | 322 (85) | 1.7 (1.2–2.4) | 103 (27) | 0.46 (0.36–0.61) |
| Sugar-sweetened beverages 1 | Artificially sweetened beverages 2 | Beer | Wine | |||||||
| Gender | ||||||||||
| Men | 353 (41) | 1.00 | 191 (22) | 1.00 | 182 (21) | 1.00 | 156 (18) | 1.00 | ||
| Women | 260 (28) | 0.57 (0.46–0.71) | 242 (26) | 1.38 (1.10–1.75) | 85 (9) | 0.34 (0.25–0.46) | 204 (22) | 1.13 (0.88–1.15) | ||
| Age (years) | ||||||||||
| 18–34 | 221 (54) | 1.00 | 113 (28) | 1.00 | 69 (17) | 1.00 | 41 (10) | 1.00 | ||
| 35–54 | 260 (32) | 0.43 (0.33–0.56) | 225 (28) | 0.95 (0.72–1.25) | 120 (15) | 0.91 (0.65–1.28) | 165 (20) | 2.28 (1.56–3.33) | ||
| 55–70 | 132 (23) | 0.24 (0.18–0.33) | 95 (17) | 0.47 (0.34–0.65) | 78 (14) | 0.81 (0.56–1.17) | 154 (27) | 3.78 (2.57–5.57) | ||
| p trend | <0.001 | <0.001 | 0.255 | <0.001 | ||||||
| BMI | ||||||||||
| <25 kg/m2 | 318 (35) | 1.00 | 185 (21) | 1.00 | 140 (16) | 1.00 | 206 (23) | 1.00 | ||
| ≥25 kg/m2 | 287 (34) | 0.95 (0.76–1.18) | 239 (28) | 1.70 (1.35–2.15) | 123 (14) | 0.76 (0.58–1.01) | 148 (17) | 0.66 (0.51–0.85) | ||
| Education | ||||||||||
| No or lower degree | 343 (41) | 1.00 | 223 (26) | 1.00 | 115 (14) | 1.00 | 130 (15) | 1.00 | ||
| University or college | 270 (29) | 0.65 (0.53–0.81) | 209 (22) | 0.83 (0.66–1.04) | 151 (16) | 1.43 (1.08–1.89) | 230 (25) | 1.67 (1.29–2.15) | ||
| Interest in healthy diet | ||||||||||
| No, low or moderate | 345 (44) | 1.00 | 211 (27) | 1.00 | 131 (17) | 1.00 | 120 (15) | 1.00 | ||
| High or very high | 267 (27) | 0.56 (0.45–0.69) | 222 (22) | 0.79 (0.63–0.98) | 136 (14) | 0.89 (0.67–1.17) | 240 (24) | 1.48 (1.14–1.91) | ||
| Smoking habits | ||||||||||
| Non-smokers | 472 (34) | 1.00 | 328 (23) | 1.00 | 189 (13) | 1.00 | 282 (20) | 1.00 | ||
| Smokers | 141 (37) | 1.05 (0.81–1.35) | 105 (28) | 1.17 (0.90–1.54) | 78 (21) | 1.79 (1.31–2.43) | 78 (21) | 1.17 (0.87–1.58) | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulsen, M.M.; Myhre, J.B.; Andersen, L.F. Beverage Consumption Patterns among Norwegian Adults. Nutrients 2016, 8, 561. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090561
Paulsen MM, Myhre JB, Andersen LF. Beverage Consumption Patterns among Norwegian Adults. Nutrients. 2016; 8(9):561. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090561
Chicago/Turabian StylePaulsen, Mari Mohn, Jannicke Borch Myhre, and Lene Frost Andersen. 2016. "Beverage Consumption Patterns among Norwegian Adults" Nutrients 8, no. 9: 561. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8090561