Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area—The Salt Intake in Northern Greece (SING) Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Recruitment
2.2. Data Collection
2.3. Adherence to Mediterranean Diet
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
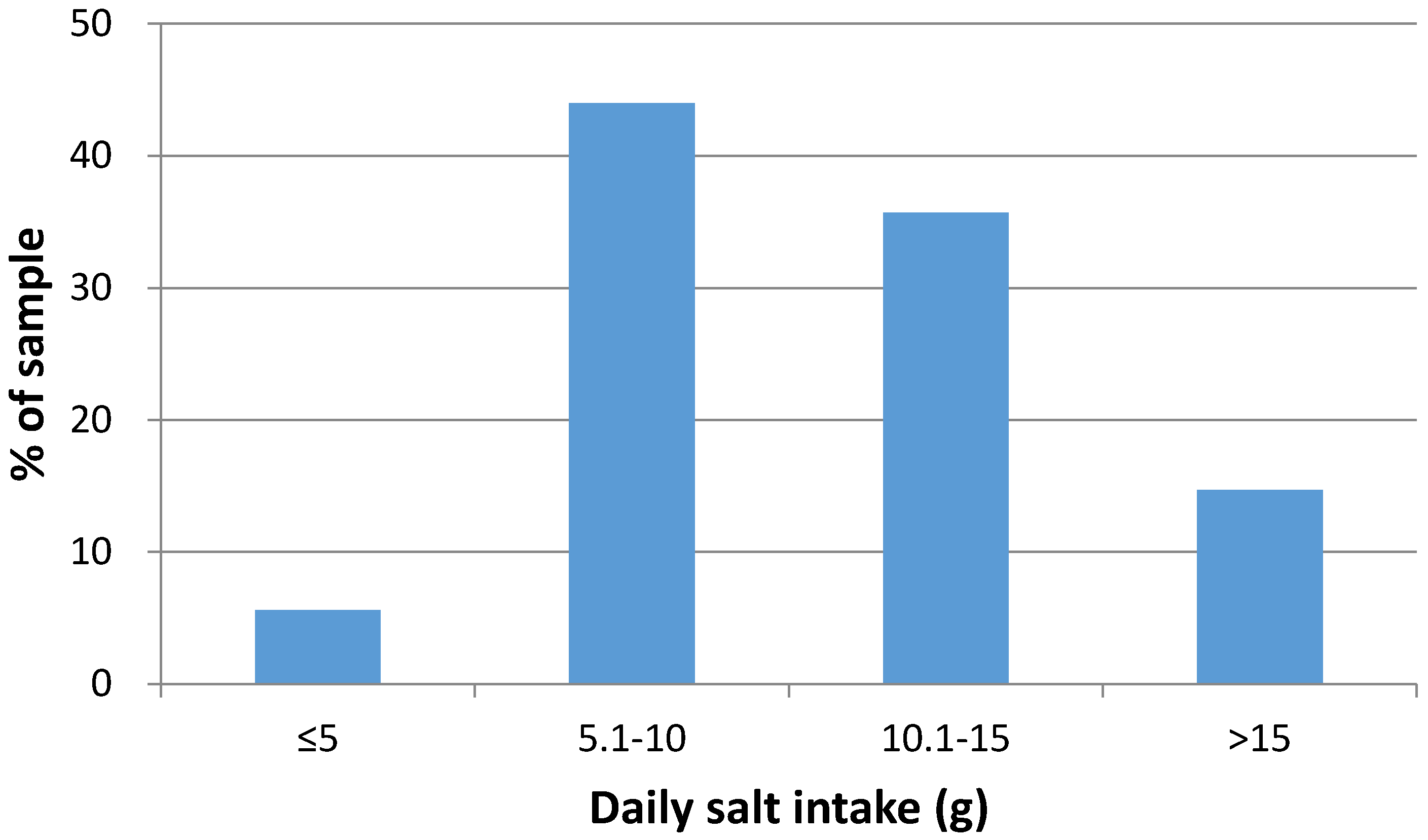
3.2. Sodium and Potassium Intakes
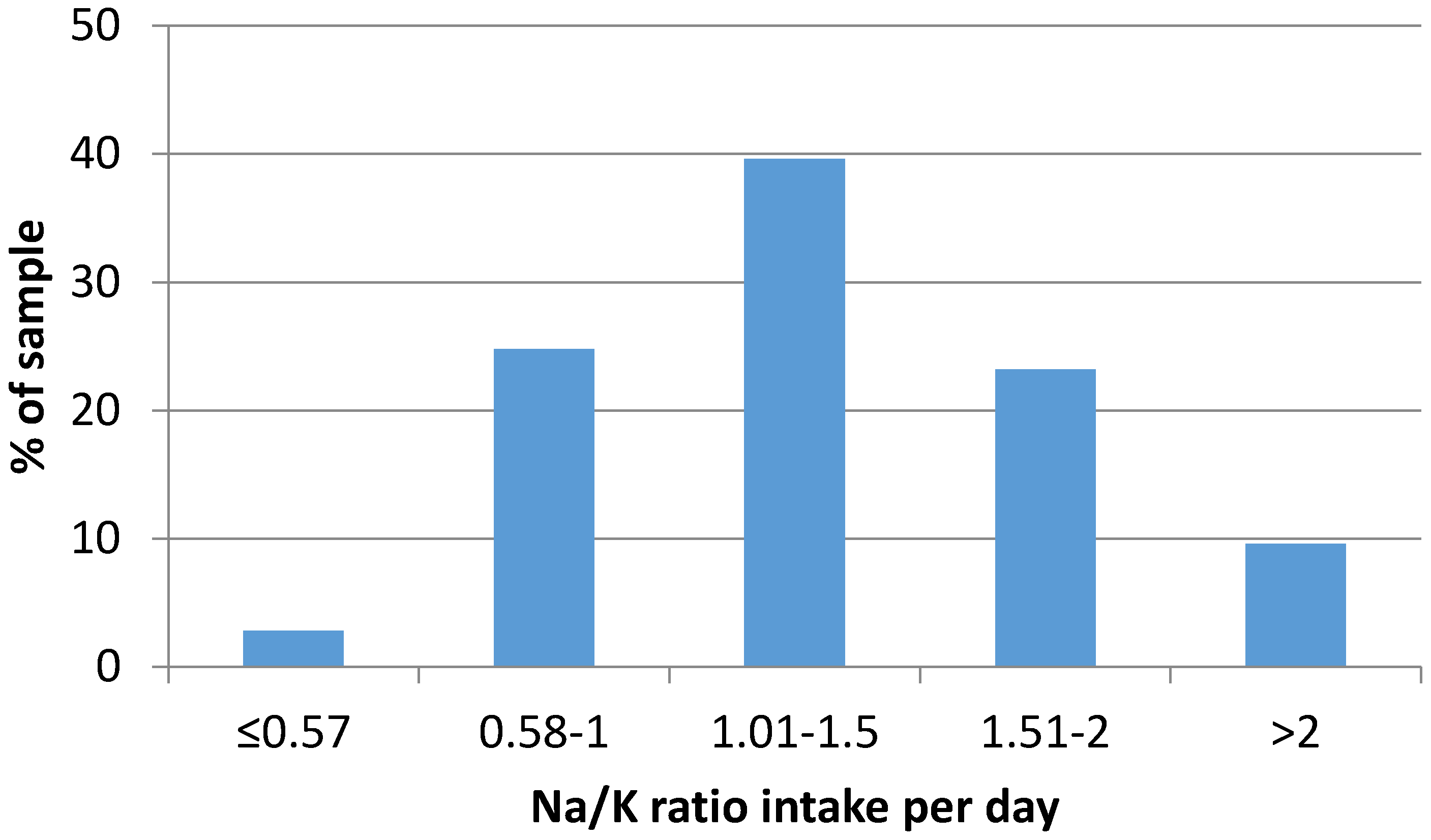
3.3. Sodium-to-Potassium Ratio
3.4. Salt Intake and Adherence to the Mediterranean Diet
4. Discussion
Limitations of the Study
5. Conclusions
Acknowledgments
Author Contributions
Conflict of Interest
References
- Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Available online: http://www.healthdata.org/greece (accessed on 5 March 2017).
- Hellenic Health Foundation. HYDRIA Project. Conclusions, Remarks and Recommendations for Policy Measures. Available online: http://www.hhf-greece.gr/images/book-hydria-120516print.pdf (accessed on 11 November 2016).
- Cook, N.R.; Cutler, J.A.; Obarzanek, E.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the Trials of Hypertension Prevention (TOHP). BMJ 2007, 334, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Strazzullo, P.; D’Elia, L.; Kandala, N.B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. BMJ 2009, 339, b4567. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analysis. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- Mente, A.; O’Donnell, M.; Rangarajan, S.; Dagenais, G.; Lear, S.; McQueen, M.; Diaz, R.; Avezum, A.; Lopez-Jaramillo, P.; Lanas, F.; et al. For the PURE, EPIDREAM and ONTARGET/TRANSCEND Investigators. Associations of urinary sodium excretion with cardiovascular events in individuals with and without hypertension: A pooled analysis of data from four studies. Lancet 2016, 388, 465–475. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Campbell, N.R.C. Population dietary salt reduction and the risk of cardiovascular disease: A commentary on recent evidence. J. Clin. Hypertens. 2017, 19, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P. Cardiovascular and other effects of salt consumption. Kidney Int. Suppl. 2013, 3, 312–315. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline. Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Capewell, S. Facts, Issues, and Controversies in Salt Reduction for the Prevention of Cardiovascular Disease. Funct. Food Rev. 2015, 7, 41–61. [Google Scholar]
- WHO Regional Office for Europe. Mapping Salt Reduction Initiatives in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Intersalt cooperative research group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar]
- Land, M.A.; Webster, J.; Christoforou, A.; Praveen, D.; Jeffery, P.; Chalmers, J.; Smith, W.; Woodward, M.; Barzi, F.; Nowson, C.; et al. Salt intake assessed by 24 h urinary sodium excretion in a random and opportunistic sample in Australia. BMJ Open 2014, 4, e003720. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: A meta-analysis of randomized controlled trials. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Ekmekcioglu, C.; Elmadfa, I.; Meyer, A.L.; Moeslinger, T. The role of dietary potassium in hypertension and diabetes. J. Physiol. Biochem. 2016, 72, 93–106. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, L.; Barba, G.; Cappuccio, F.P.; Strazzullo, P. Potassium Intake, Stroke, and Cardiovascular Disease. A meta-analysis of Prospective Studies. J. Am. Coll. Cardiol. 2011, 57, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Young, D.B.; Lin, H.; McCabe, R.D. Potassium’s cardiovascular protective mechanisms. Am. J. Physiol. 1995, 268 (4 Pt 2), R825–R837. [Google Scholar] [PubMed]
- Morris, R.C., Jr.; Schmidlin, O.; Frassetto, L.A.; Sebastian, A. Relationship and interaction between sodium and potassium. J. Am. Coll. Nutr. 2006, 25, 262S–270S. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The Trials of Hypertension Prevention follow-up study. Arch. Int. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M. Potassium and Health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M. Uber den Niederschlag welchen Pikrinsaure in normalen Harn erzeug und uber eine neue Raction des Creatinins. Z. Physiol. Chem. 1986, 10, 391–400. [Google Scholar]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization—World Health Organization. Salt-Smart Americas: A Guide for Country-Level Action; Pan American Health Organization: Washington, DC, USA, 2013; pp. 1–159. [Google Scholar]
- World Health Organization. Guideline. Potassium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012; pp. 1–42. [Google Scholar]
- Sahan, C.; Sozmen, K.; Unal, B.; O’Flaherty, M.; Critchley, J. Potential benefits of healthy food and lifestyle policies for reducing coronary heart disease mortality in Turkish adults by 2025: A modelling study. BMJ Open 2016, 6, e011217. [Google Scholar] [CrossRef] [PubMed]
- Ribič, C.H.; Zakotnik, J.M.; Vertnik, L.; Vegnuti, M.; Cappuccio, F.P. Salt intake of the Slovene population assessed by 24 h urinary sodium excretion. Public Health Nutr. 2010, 13, 1803–1809. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Diet, Nutrition and the Prevention of Chronic Disease; Report of a Joint WHO/FAO Expert Consultation; World Health Organization (WHO): Geneva, Switzerland, 2003. [Google Scholar]
- Yang, Q.; Liu, T.; Kuklina, E.V.; Flanders, W.D.; Hong, Y.; Gillespie, C.; Chang, M.H.; Gwinn, M.; Dowling, N.; Khoury, M.J.; et al. Sodium and potassium intake and mortality among US adults: Prospective data from the Third National Health and Nutrition Examination Survey. Arch. Int. Med. 2011, 171, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.S.; Curtis, C.J.; Angell, S.Y.; Anderson, C.A.; Jung, M.; Kansagra, S.M. Highlighting the ratio of sodium to potassium in population-level dietary assessments: Cross-sectional data from New York City, USA. Public Health Nutr. 2014, 17, 2484–2488. [Google Scholar] [CrossRef] [PubMed]
- Mariolis, A.; Foscolou, A.; Tyrovolas, S.; Piscopo, S.; Valacchi, G.; Tsakountakis, N.; Zeimbekis, A.; Bountziouka, V.; Gotsis, E.; Metallinos, G.; et al. MEDIS study group. Successful Aging among Elders Living in the Mani Continental Region vs. Insular Areas of the Mediterranean: The MEDIS Study. Aging Dis. 2016, 7, 285–294. [Google Scholar] [PubMed]
- Girvalaki, C.; Vardavas, C.I.; Tsimpinos, G.; Dimitreli, G.; Hassapidou, M.N.; Kafatos, A. Nutritional and chemical quality of traditional spreads and pies of Mediterranean diet of Greece. J. Food Nutr. Disor. 2013, 2, 1. [Google Scholar]
- Birukov, A.; Rakova, N.; Lerchl, K.; Engberink, R.H.; Johannes, B.; Wabel, P.; Moissl, U.; Rauh, M.; Luft, F.C.; Titze, J. Ultra-long-term human salt balance studies reveal interrelations between sodium, potassium, and chloride intake and excretion. Am. J. Clin. Nutr. 2016, 104, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, A.; Bochud, M.; Glatz, N.; Vuistiner, P.; Paccaud, F.; Burnier, M. Swiss Survey on Salt Intake: Main Results. 2011. Available online: http://my.unil.ch/serval/document/BIB_16AEF897B618.pdf (accessed on 8 March 2017).
- Ortega, R.M.; Lopez-Sobaler, A.M.; Ballesteros, J.M.; Pérez-Farinós, N.; Rodríguez-Rodríguez, E.; Aparicio, A.; Perea, J.M.; Andrés, P. Estimation of salt intake by 24 h urinary sodium excretion in a representative sample of Spanish adults. Br. J. Nutr. 2011, 105, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Cooper, R.; McKeever, J.; McKeever, P.; Byington, R.; Soltero, I.; Stamler, R.; Gosch, F.; Stevens, E.; Stamler, J. Assessment of the association between habitual salt intake and high blood pressure: Methodological problems. Am. J. Epidemiol. 1979, 110, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Lerchl, K.; Rakova, N.; Dahlmann, A.; Rauh, M.; Goller, U.; Basner, M.; Dinges, D.F.; Beck, L.; Agureev, A.; Larina, I.; et al. Agreement between 24-hour salt ingestion and sodium excretion in a controlled environment. Hypertension 2015, 66, 850–857. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 252) | Men (n = 114) | Women (n = 138) | |
|---|---|---|---|
| Mean Age (years) | 46.6 (16.6) | 47.0 (16.2) | 46.2 (17.0) |
| % in the range 18–34 | 26.8 | 27.4 | 27.0 |
| % in the range 35–49 | 25.6 | 24.8 | 25.6 |
| % in the range 50–64 | 35.6 | 36.3 | 35.0 |
| % in the range 65–75 | 12.0 | 11.5 | 12.4 |
| Height (cm) | 169.3 (9.5) | 176.8 (6.6) | 163.1 (6.6) **** |
| Weight (kg) | 77.0 (15.7) | 85.2 (14.6) | 70.3 (13.1) **** |
| BMI (kg/m2) | 26.8 (4.7) | 27.2 (4.1) | 26.5 (5.1) |
| Waist circumference (cm) | 87.6 (14.7) | 94.8 (13.1) | 81.6 (13.1) **** |
| Level of education (%) | |||
| Non university graduates | 60.3 | 51.8 | 67.4 |
| University graduates | 39.7 | 48.2 | 32.6 * |
| Self-assessment of personal diet quality (%) | |||
| Good | 61.3 | 62.0 | 60.7 |
| Moderate | 37.1 | 34.5 | 39.3 |
| Bad | 1.6 | 3.5 | 0 |
| Systolic BP (mmHg) | 126.5 (16.4) | 129.9 (16.8) | 123.7 (15.5) ** |
| Diastolic BP (mmHg) | 79.8 (11.9) | 82.5 (12.5) | 77.6 (10.9) *** |
| MedDietScore | 30.5 (5.1) | 31.8 (5.4) | 29.4 (4.6) **** |
| Total (n = 252) | Men (n = 114) | Women (n = 138) | |
|---|---|---|---|
| Urinary excretions | |||
| Volume (mL/24 h) | 1800 (807) | 1782 (858) | 1814 (767) |
| Creatinine (g/24 h) | 1.36 (0.51) | 1.66 (0.53) | 1.11 (0.33) **** |
| Sodium (mmol/24 h) | 174.7 (72.2) | 194.3 (76.8) | 158.5 (64.1) **** |
| Potassium (mmol/24 h) | 65.1 (24.6) | 70.8 (26.0) | 60.5 (22.4) *** |
| Sodium-to-potassium ratio (mmol/mmol) | 2.82 (1.07) | 2.87 (1.02) | 2.77 (1.12) |
| Dietary estimates | |||
| Sodium intake † (mg/24 h) | 4220 (1745) | 4694 (1855) | 3828 (1548) **** |
| Potassium intake † (mg/24 h) | 3303 (1247) | 3589 (1321) | 3067 (1134) *** |
| Na/K intake ratio (mg/mg) | 1.34 (0.51) | 1.37 (0.48) | 1.32 (0.53) |
| Salt intake (g/day) | 10.7 (4.4) | 11.9 (4.7) | 9.7 (3.9) **** |
| MedDietScore Quartiles | Sodium Intake (mg Per Day) | Potassium Intake (mg Per Day) | Sodium-to-Potassium Intake Ratio |
|---|---|---|---|
| 1 (≤28) | 4079 (1893) 3661–4498 | 3241 (1268) 2961–3522 | 1.32 (0.48) 1.21–1.42 |
| 2 (>28, ≤31) | 4361 (1746) 3931–4790 | 3303 (1369) 2964–3642 | 1.42 (0.61) 1.27–1.57 |
| 3 (>31, ≤34) | 3972 (1565) 3532–4413 | 3215 (1275) 2856–3573 | 1.29 (0.44) 1.17–1.41 |
| 4 (>34) | 4424 (1636) 3954–4894 | 3465 (995) 3180–3751 | 1.33 (0.51) 1.19–1.48 |
| p by ANOVA | 0.453 | 0.735 | 0.532 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.A.; Cappuccio, F.P. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area—The Salt Intake in Northern Greece (SING) Study. Nutrients 2017, 9, 417. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9040417
Vasara E, Marakis G, Breda J, Skepastianos P, Hassapidou M, Kafatos A, Rodopaios N, Koulouri AA, Cappuccio FP. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area—The Salt Intake in Northern Greece (SING) Study. Nutrients. 2017; 9(4):417. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9040417
Chicago/Turabian StyleVasara, Eleni, Georgios Marakis, Joao Breda, Petros Skepastianos, Maria Hassapidou, Anthony Kafatos, Nikolaos Rodopaios, Alexandra A. Koulouri, and Francesco P. Cappuccio. 2017. "Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area—The Salt Intake in Northern Greece (SING) Study" Nutrients 9, no. 4: 417. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9040417