Optimal Energy Delivery, Rather than the Implementation of a Feeding Protocol, May Benefit Clinical Outcomes in Critically Ill Patients

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
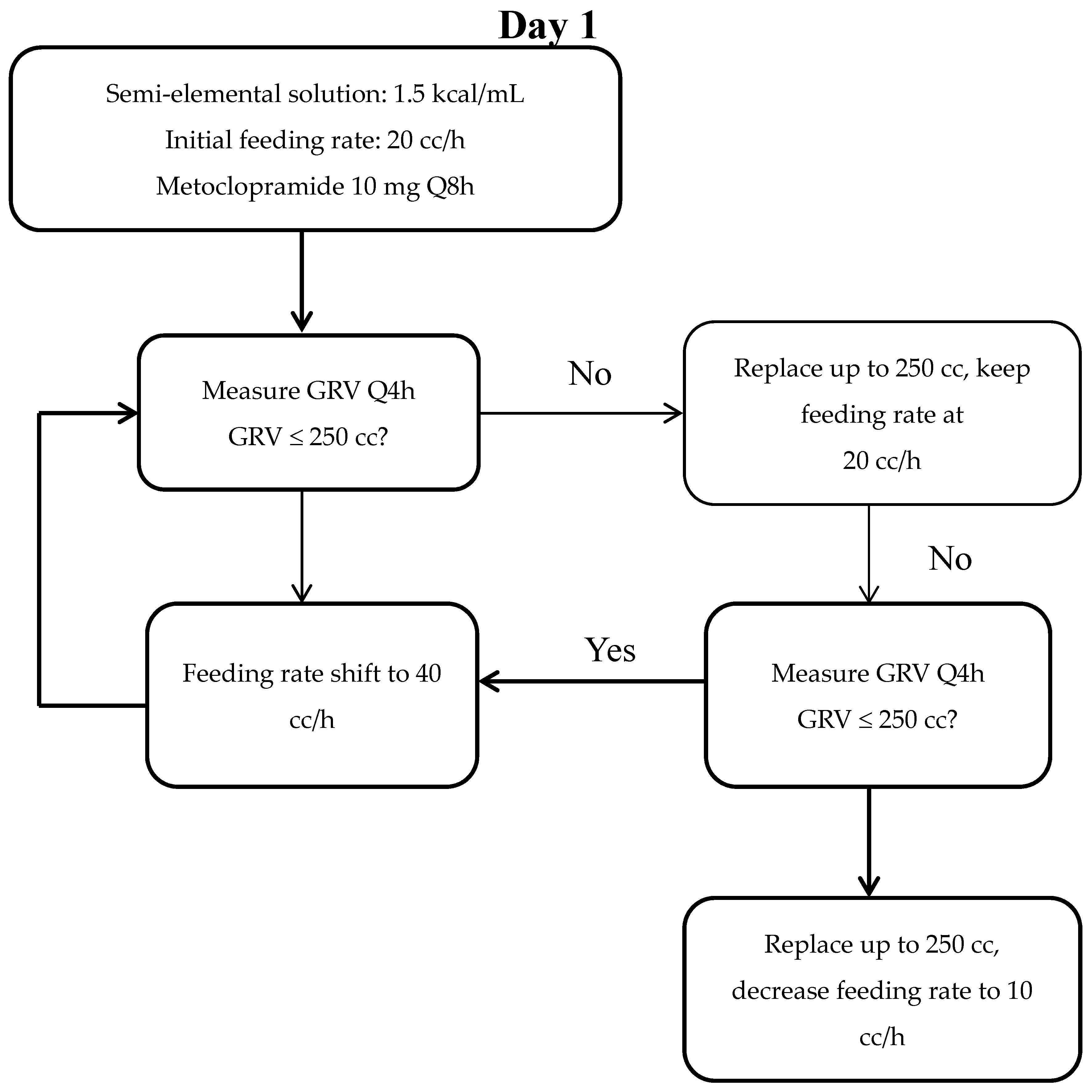
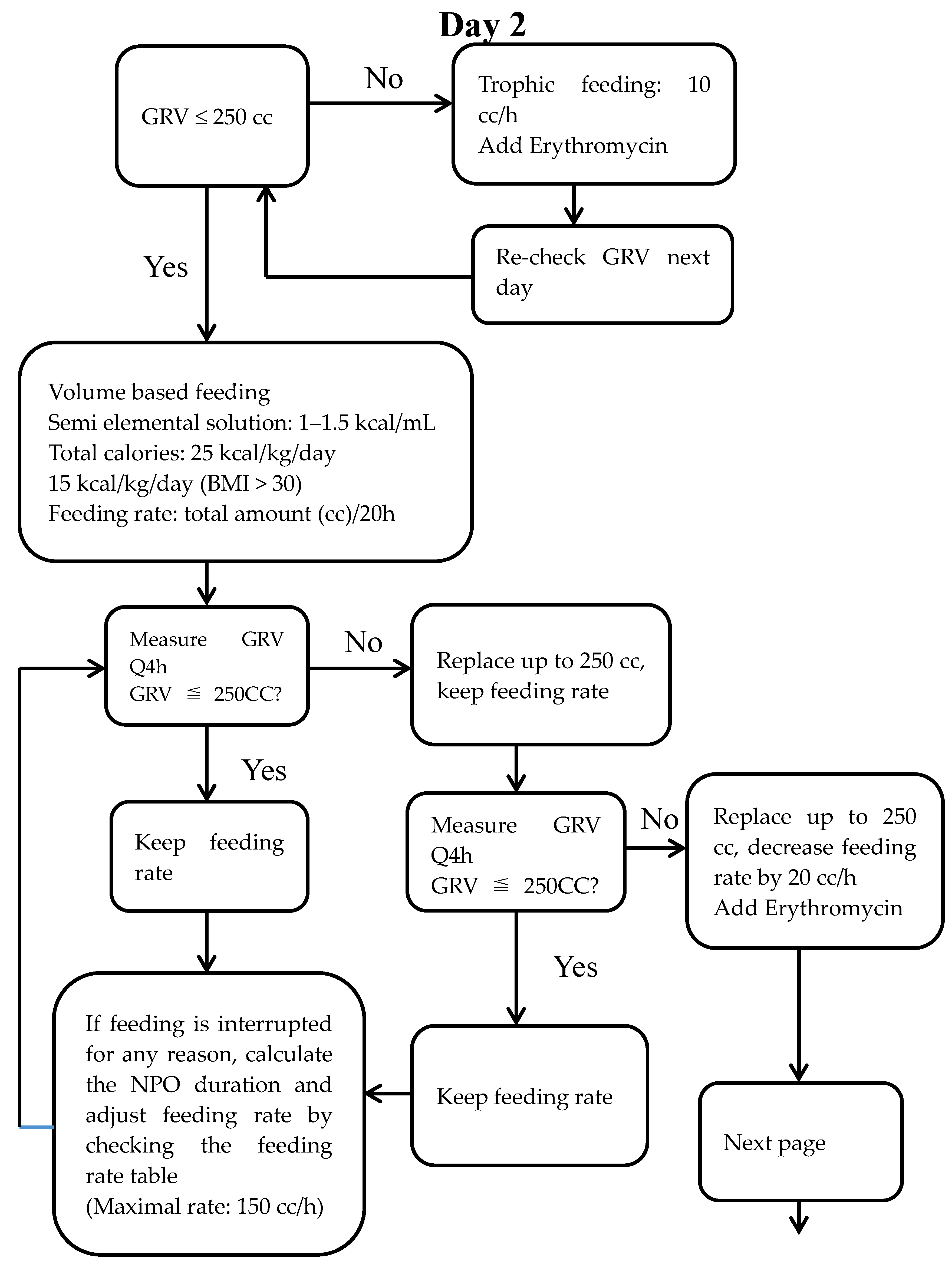
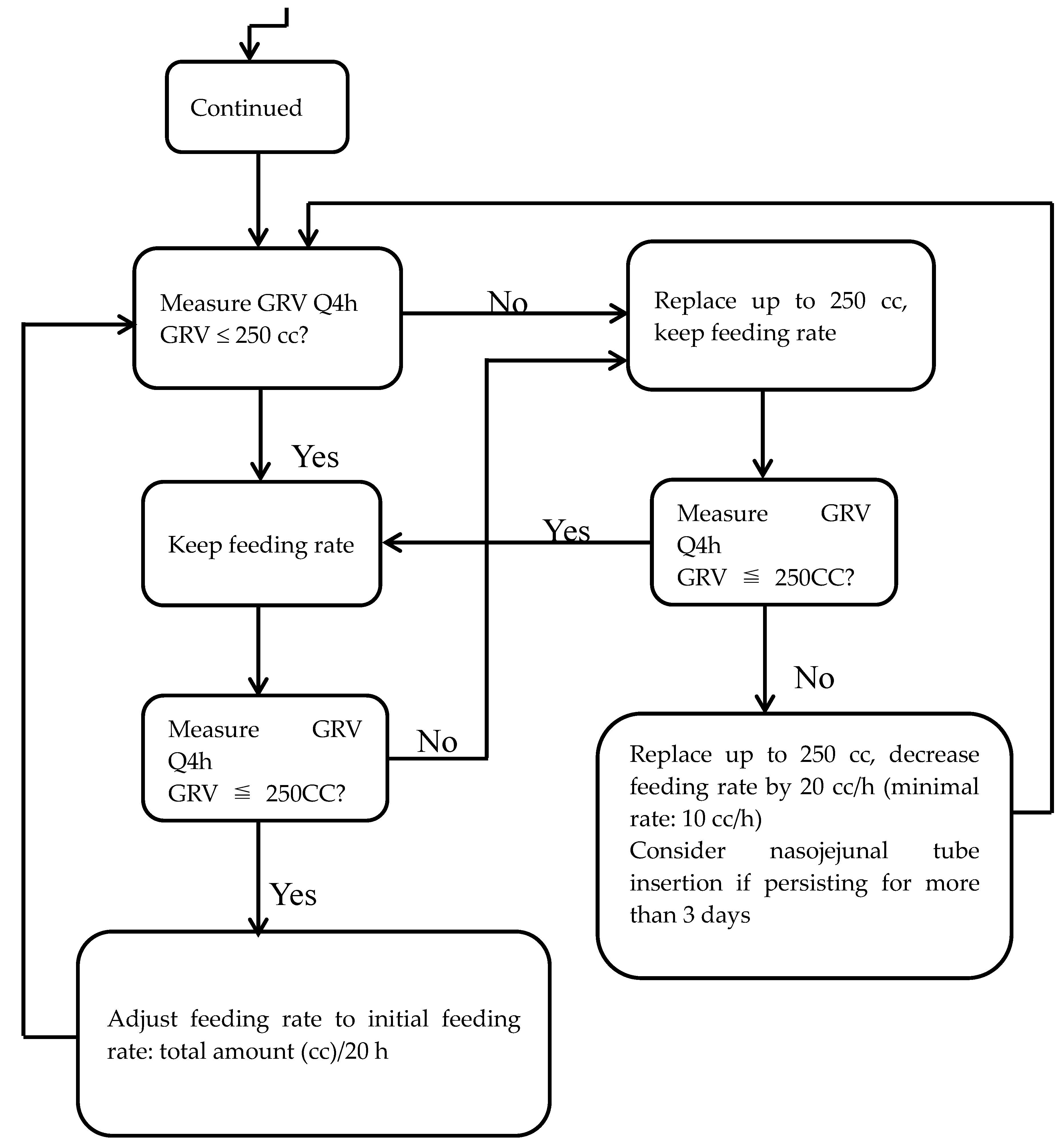
2.2. Feeding Protocol
2.3. Patients
2.4. Data Collection and Energy Intakes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| APACHE II | acute physiology and chronic health evaluation II |
| ASPEN | American Society for Parenteral Enteral Nutrition |
| BMI | body mass index |
| FP | feeding protocol |
| GRVs | gastric residual volumes |
| ICU | intensive care units |
| SCCM | Society of Critical Care Medicine |
| TVGH | Taichung Veterans General Hospital |
References
- Guimaraes, S.M.; Lima, E.Q.; Cipullo, J.P.; Lobo, S.M.; Burdmann, E.A. Low insulin-like growth factor-1 and hypocholesterolemia as mortality predictors in acute kidney injury in the intensive care unit. Crit. Care Med. 2008, 36, 3165–3170. [Google Scholar] [CrossRef] [PubMed]
- Sungurtekin, H.; Sungurtekin, U.; Oner, O.; Okke, D. Nutrition assessment in critically ill patients. Nutr. Clin. Pract. 2008, 23, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Sheean, P.M.; Peterson, S.J.; Chen, Y.; Liu, D.; Lateef, O.; Braunschweig, C.A. Utilizing multiple methods to classify malnutrition among elderly patients admitted to the medical and surgical intensive care units (ICU). Clin. Nutr. 2013, 32, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.C.; Ichai, C.; Orban, J.C.; Groeneveld, A.B. Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Dhaliwal, R.; Cahill, N.; Lemieux, M.; Heyland, D.K. The Canadian critical care nutrition guidelines in 2013: An update on current recommendations and implementation strategies. Nutr. Clin. Pract. 2014, 29, 29–43. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Artinian, V.; Krayem, H.; DiGiovine, B. Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest 2006, 129, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Heighes, P.T.; Simpson, F.; Sweetman, E.A.; Davies, A.R. Early enteral nutrition, provided within 24 h of injury or intensive care unit admission, significantly reduces mortality in critically ill patients: A meta-analysis of randomised controlled trials. Intensive Care Med. 2009, 35, 2018–2027. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Andersen, H.K.; Thomas, S. Early enteral nutrition within 24 h of intestinal surgery versus later commencement of feeding: A systematic review and meta-analysis. J. Gastrointest. Surg. 2009, 13, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Rubinson, L.; Diette, G.B.; Song, X.; Brower, R.G.; Krishnan, J.A. Low caloric intake is associated with nosocomial bloodstream infections in patients in the medical intensive care unit. Crit. Care Med. 2004, 32, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.C.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Petros, S.; Engelmann, L. Enteral nutrition delivery and energy expenditure in medical intensive care patients. Clin. Nutr. 2006, 25, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Faisy, C.; Lerolle, N.; Dachraoui, F.; Savard, J.F.; Abboud, I.; Tadie, J.M.; Fagon, J.Y. Impact of energy deficit calculated by a predictive method on outcome in medical patients requiring prolonged acute mechanical ventilation. Br. J. Nutr. 2009, 101, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Yeh, D.D.; Peev, M.P.; Quraishi, S.A.; Osler, P.; Chang, Y.; Rando, E.G.; Albano, C.; Darak, S.; Velmahos, G.C. Clinical Outcomes of Inadequate Calorie Delivery and Protein Deficit in Surgical Intensive Care Patients. Am. J. Crit. Care 2016, 25, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Alberda, C.; Gramlich, L.; Jones, N.; Jeejeebhoy, K.; Day, A.G.; Dhaliwal, R.; Heyland, D.K. The relationship between nutritional intake and clinical outcomes in critically ill patients: Results of an international multicenter observational study. Intensive Care Med. 2009, 35, 1728–1737. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Cahill, N.; Day, A.G. Optimal amount of calories for critically ill patients: Depends on how you slice the cake! Crit. Care Med. 2011, 39, 2619–2626. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Stephens, K.E.; Day, A.G.; McClave, S.A. The success of enteral nutrition and ICU-acquired infections: A multicenter observational study. Clin. Nutr. 2011, 30, 148–155. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Sexton, L.K.; Spain, D.A.; Adams, J.L.; Owens, N.A.; Sullins, M.B.; Blandford, B.S.; Snider, H.L. Enteral tube feeding in the intensive care unit: Factors impeding adequate delivery. Crit. Care Med. 1999, 27, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Schroter-Noppe, D.; Drover, J.W.; Jain, M.; Keefe, L.; Dhaliwal, R. Nutrition support in the critical care setting: Current practice in Canadian ICUs—Opportunities for improvement? J. Parenter. Enter. Nutr. 2003, 27, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Binnekade, J.M.; Tepaske, R.; Brynzeel, P.; Mathus-Vliegen, E.M.; de Hann, R.J. Daily enteral feeding practice on the ICU: Attainment of goals and interfering factors. Crit. Care Med. 2005, 9, R218–R225. [Google Scholar]
- Heyland, D.K.; Cahill, N.E.; Dhaliwal, R.; Wang, M.; Day, A.G.; Alenzi, A.; Aris, F.; Muscedere, J.; Drover, J.W.; McClave, S.A. Enhanced protein-energy provision via the enteral route in critically ill patients: A single center feasibility trial of the PEP uP protocol. Crit. Care 2010, 14, R78. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Saad, M.A.; Esterle, M.; Anderson, M.; Jotautas, A.E.; Franklin, G.A.; Heyland, D.K.; Hurt, R.T. Volume-Based Feeding in the Critically Ill Patient. J. Parenter. Enter. Nutr. 2015, 39, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Aldawood, A.S.; Haddad, S.H.; et al. Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults. N. Engl. J. Med. 2015, 372, 2398–2408. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; Steingrub, J.; Hite, R.D.; Moss, M.; Morris, A.; Dong, N.; Rock, P. Initial trophic vs full enteral feeding in patients with acute lung injury: The EDEN randomized trial. JAMA 2012, 307, 795–803. [Google Scholar] [PubMed]
- McCowen, K.C.; Friel, C.; Sternberg, J.; Chan, S.; Forse, R.A.; Burke, P.A.; Bistrian, B.R. Hypocaloric total parenteral nutrition: effectiveness in prevention of hyperglycemia and infectious complications—A randomized clinical trial. Crit. Care Med. 2000, 28, 3606–3611. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, C.L.; Barletta, J.F.; Kanji, S.; Tyburski, J.G.; Wilson, R.F.; Janisse, J.J.; Devlin, J.W. Effect of low-calorie parenteral nutrition on the incidence and severity of hyperglycemia in surgical patients: A randomized, controlled trial. Crit. Care Med. 2005, 33, 2507–2512. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Murch, L.; Cahill, N.; McCall, M.; Muscedere, J.; Stelfox, H.T.; Bray, T.; Tanguay, T.; Jiang, X.; Day, A.G. Enhanced protein-energy provision via the enteral route feeding protocol in critically ill patients: Results of a cluster randomized trial. Crit. Care Med. 2013, 41, 2743–2753. [Google Scholar] [CrossRef] [PubMed]
- Barr, J.; Hecht, M.; Flavin, K.E.; Khorana, A.; Gould, M.K. Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest 2004, 125, 1446–1457. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Finfer, S.; Delaney, A.; Davies, A.R.; Mitchell, I.; Dobb, G. Effect of evidence-based feeding guidelines on mortality of critically ill adults. A cluster randomized controlled trial. JAMA 2008, 300, 2731–2741. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.M.; Doig, G.S.; Heyland, D.K.; Morrison, T.; Sibbald, W.J. Multicentre, cluster-randomized clinical trial of algorithms for critical-care enteral and parenteral therapy (ACCEPT). CMAJ 2004, 170, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Weijs, P.J.; Stapel, S.N.; de Groot, S.D.W.; Driessen, R.H.; de Jong, E.; Girbes, A.R.J.; van Schijndel, R.J.M.S.; Beishuizen, A. Optimal protein and energy nutrition decreases mortality in mechanically ventilated, critically ill patients: A prospective observational cohort study. J. Parenter. Enter. Nutr. 2012, 36, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Elke, G.; Wang, M.; Weiler, N.; Day, A.G.; Heyland, D.K. Close to recommended caloric and protein intake by enteral nutrition is associated with better clinical outcome of critically ill septic patients: Secondary analysis of a large international nutrition database. Crit. Care 2014, 18, R29. [Google Scholar] [CrossRef] [PubMed]
- Heidegger, C.P.; Berger, M.M.; Graf, S.; Zingg, W.; Darmon, P.; Costanza, M.C.; Thibault, R.; Pichard, C. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: A randomised controlled clinical trial. Lancet 2013, 381, 385–393. [Google Scholar] [CrossRef]
- Petros, S.; Horbach, M.; Seidel, F.; Weidhase, L. Hypocaloric vs normocaloric nutrition in critically ill patients: A prospective randomized pilot trial. J. Parenter. Enter. Nutr. 2016, 40, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, J.A.; Parce, P.B.; Martinez, A.; Diette, G.B.; Brower, R.G. Caloric intake in medical ICU patients: consistency of care with guidelines and relationship to clinical outcomes. Chest 2003, 124, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Mogan, S.; Hays, M.; Bernard, G.R.; Jensen, G.L.; Wheeler, A.P. A randomized trial of initial trophic versus full-energy enteral nutrition in mechanically ventilated patients with acute respiratory failure. Crit. Care Med. 2011, 39, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Needham, D.M.; Dinglas, V.D.; Bienvenu, O.J.; Colantuoni, E.; Wozniak, A.W.; Rice, T.W.; Hopkins, R.O. One year outcomes in patients with acute lung injury randomised to initial trophic or full enteral feeding: prospective follow-up of EDEN randomised trial. BMJ 2013, 346, f1532. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed]
- Jie, B.; Jiang, Z.M.; Nolan, M.T.; Zhu, S.N.; Yu, K.; Kondrup, J. Impact of preoperative nutritional support on clinical outcome in abdominal surgical patients at nutritional risk. Nutrition 2012, 28, 1022–1027. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 412) | pre-FP Group (n = 214) | FP Group (n = 198) |
|---|---|---|---|
| Age (year) | 69.4 ± 16.0 | 71.3 ± 15.0 | 67.4 ± 16.9 * |
| Gender (women/men) | 169/2473 | 89/125 | 80/118 |
| Weight (kg) | 62.0 ± 14.6 | 61.6 ± 13.3 | 62.5 ± 5.9 |
| Body mass index (kg/m2) | 23.95 ± 5.19 | 23.94 ± 4.77 | 23.97 ± 5.62 |
| Length of ventilatory dependency (day) | 20.9 ± 14.7 | 22.0 ± 16.7 | 19.7 ± 12.0 |
| Length of ICU stay (day) | 13.7 ± 7.3 | 13.2 ± 7.4 | 14.2 ± 7.2 |
| Length of hospital stay (day) | 30.5 ± 18.1 | 30.3 ± 19.3 | 30.6 ± 16.6 |
| APACHE II score | 28.0 ± 5.9 | 27.8 ± 5.5 | 28.2 ± 6.2 |
| Mortality (n, %) | 117, 28.4% | 55, 25.7% | 62, 31.3% |
| Energy Intakes | |||
| Estimated energy requirement (kcal/day) | 1438.2 ± 223.8 | 1419.3 ± 161.1 | 1458.6 ± 275.0 |
| Actual energy intake (kcal/day) | 908.0 ± 333.5 | 811.7 ± 347.4 | 1012.1 ± 283.9 * |
| Achievement rate (%) | 64.3 ± 25.0 | 57.7 ± 25.1 | 70.3 ± 20.6 * |
| Comorbidities (n, %) | |||
| Diabetes mellitus | 159, 38.6% | 81, 37.9% | 78, 39.4% |
| Liver cirrhosis | 37, 9.0% | 27, 12.6% | 10, 5.1% * |
| Uremia | 52, 12.6% | 26, 12.1% | 26, 13.1% |
| Central nervous system disorders | 96, 23.3% | 48, 22.4% | 48, 24.2% |
| Chronic lung diseases | 55, 13.3% | 40, 18.7% | 15, 7.6% * |
| Immunocompromised disorders | 130, 31.6% | 74, 34.6% | 56, 28.3% |
| Variables | Survivor Group (n = 295) | Non-Survivor Group (n = 117) |
|---|---|---|
| Age (year) | 68.7 ± 16.4 | 71.3 ± 15.1 |
| Gender (Female/Male) | 127/168 | 42/75 |
| Weight (kg) | 61.9 ± 14.5 | 62.4 ± 14.8 |
| Body mass index (kg/m2) | 23.90 ± 5.39 | 24.08 ± 4.68 |
| Length of ventilatory dependency (day) | 20.2 ± 14.7 | 22.7 ± 14.5 * |
| Length of ICU stay (day) | 12.9 ± 6.5 | 15.7 ± 8.7 * |
| Length of hospital stay (day) | 31.4 ± 17.7 | 28.1 ± 18.7 * |
| APACHEII | 27.6 ± 5.7 | 28.9 ± 6.2 |
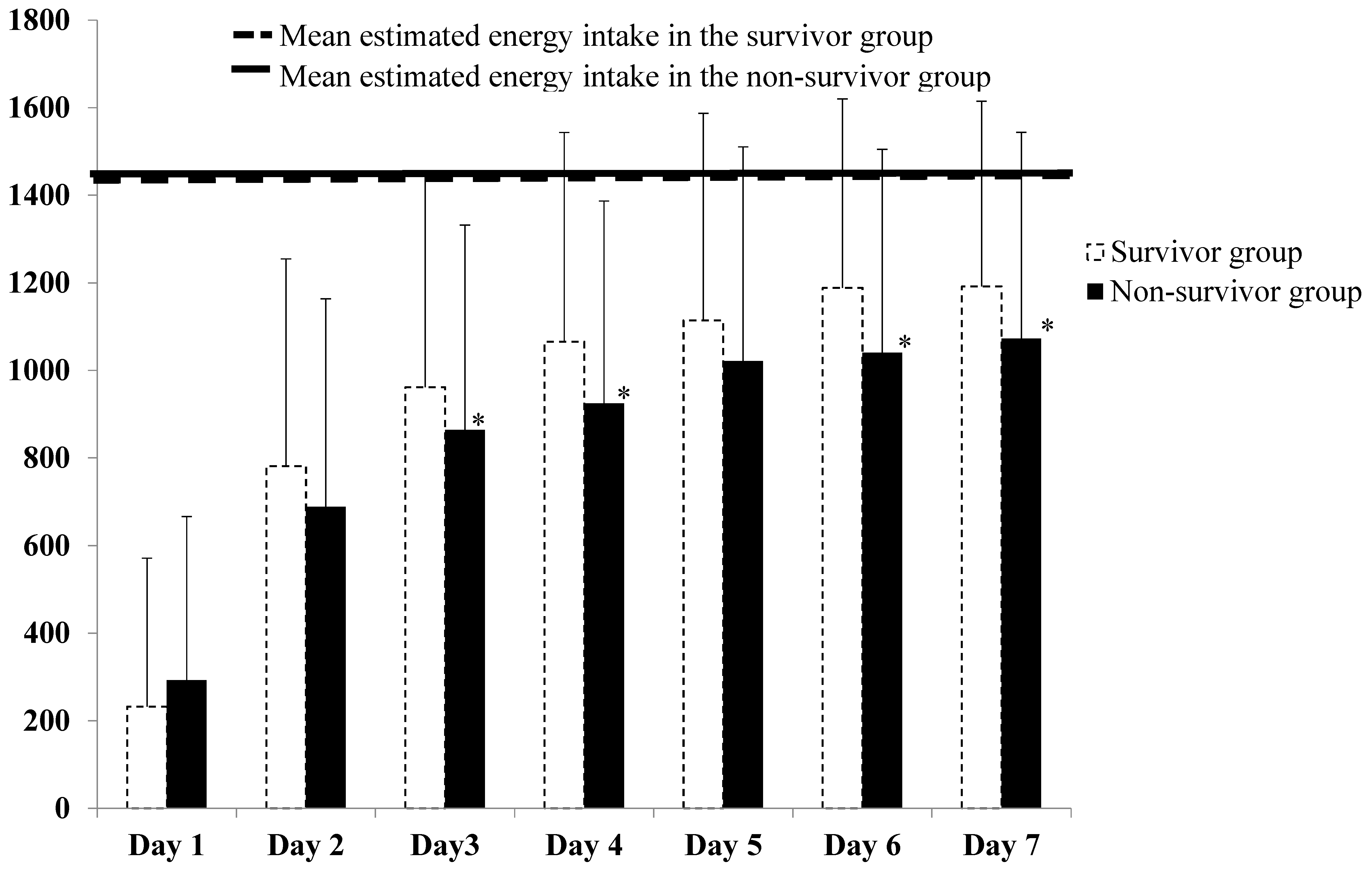
| Energy Intakes Estimated energy intakes (kcal/day) | 1437.5 ± 217.6 | 1439.9 ± 239.6 |
| Actual energy intakes (kcal/day) | 933.7 ± 329.6 | 843.3 ± 335.8 * |
| Achievement rate (%) | 66.1 ± 24.7 | 59.9 ± 25.3 * |
| Comorbidities (n, %) Diabetes mellitus | 117, 39.7% | 42, 35.9% |
| Liver cirrhosis | 19, 6.4% | 18, 15.4% * |
| Uremia | 35, 11.9% | 17, 14.5% |
| CNS disorder | 74, 25.1% | 22, 18.8% |
| Chronic lung disease | 33, 11.2% | 22, 18.8% * |
| Immunocompromised disorders | 81, 27.5% | 49, 41.9% * |
| No Factors Adjusted for | Additional Factors Adjusted for Age, Gender, BMI | Additional Factors Adjusted for Age, Gender, BMI and APACHE II | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Achievement rate (%) | 0.4 | (0.15–0.88) | 0.03 | 0.4 | (0.15–0.89) | 0.03 | 0.4 | (0.15–0.93) | 0.04 |
| Achievement rate (%) | |||||||||
| >65% | 1 | 0.02 | 1 | 0.03 | 1 | 0.04 | |||
| ≤65% | 1.7 | (1.10–2.62) | 1.7 | (1.07–2.58) | 1.6 | (1.01–2.47) | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-Y.; Huang, C.-T.; Chen, C.-H.; Chen, M.-F.; Ching, S.-L.; Huang, Y.-C. Optimal Energy Delivery, Rather than the Implementation of a Feeding Protocol, May Benefit Clinical Outcomes in Critically Ill Patients. Nutrients 2017, 9, 527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9050527
Wang C-Y, Huang C-T, Chen C-H, Chen M-F, Ching S-L, Huang Y-C. Optimal Energy Delivery, Rather than the Implementation of a Feeding Protocol, May Benefit Clinical Outcomes in Critically Ill Patients. Nutrients. 2017; 9(5):527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9050527
Chicago/Turabian StyleWang, Chen-Yu, Chun-Te Huang, Chao-Hsiu Chen, Mei-Fen Chen, Shiu-Lan Ching, and Yi-Chia Huang. 2017. "Optimal Energy Delivery, Rather than the Implementation of a Feeding Protocol, May Benefit Clinical Outcomes in Critically Ill Patients" Nutrients 9, no. 5: 527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9050527