Calcium and Vitamin D Supplementation for Prevention of Preeclampsia: A Systematic Review and Network Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Interventions
2.4. Outcomes of Interest
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Statistical Analysis
2.7.1. Direct Meta-Analysis
2.7.2. Network Meta-Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Risk of Bias Assessment
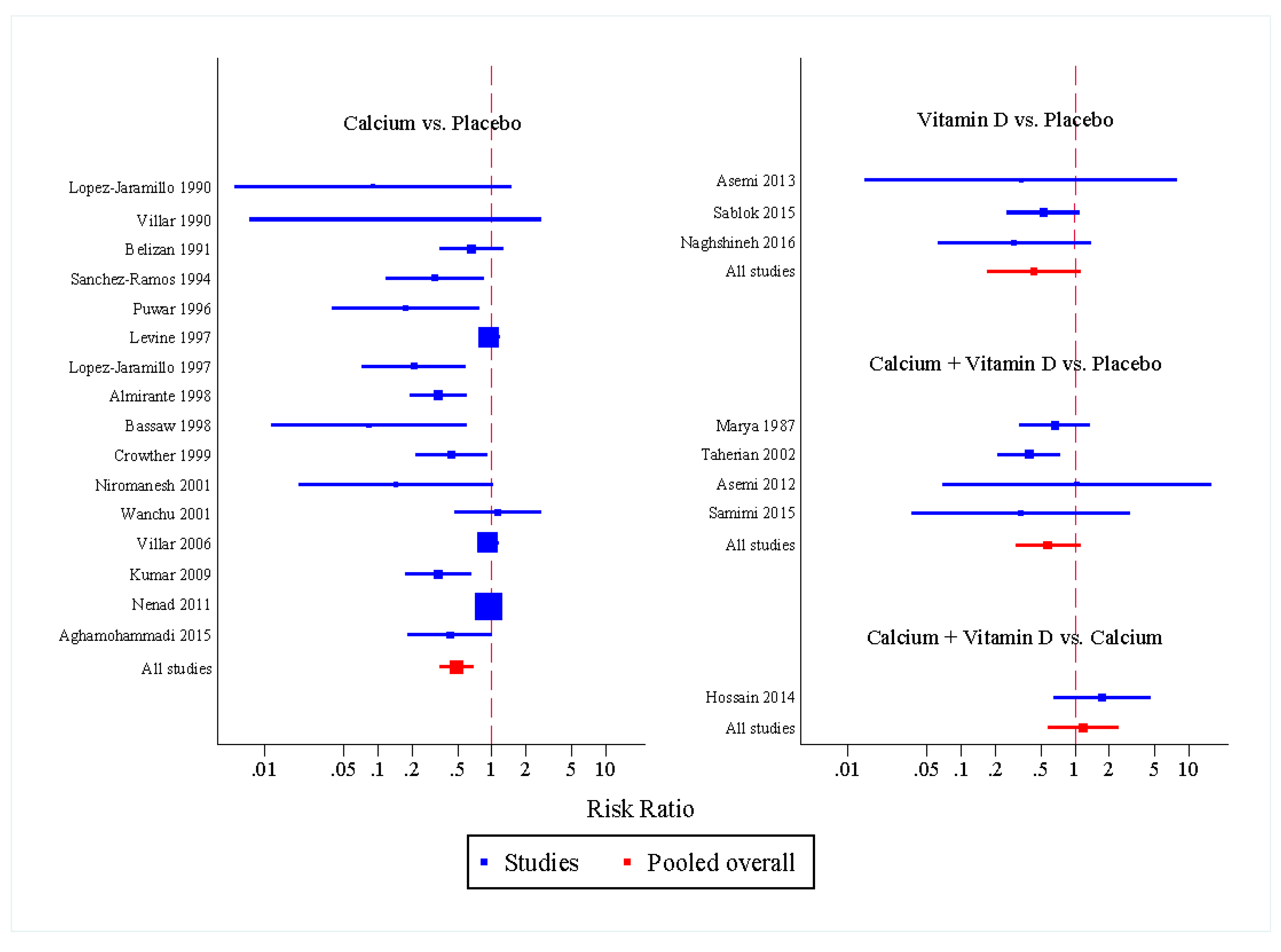
3.3. Direct Meta-Analysis
3.3.1. Preeclampsia
3.3.2. GH/PIH
3.4. Network Meta-Analysis
4. Discussion
4.1. Strengths and Limitations
4.2. Summary of Evidence
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. Search Terms and Search Strategy
Appendix A.1. PubMed Database
Appendix A.2. Scopus Database

{kind=link}
{kind=link}
| Domain | Terms | |
|---|---|---|
| 1 | Pregnancy | “pregnancy”[Mesh] ◈ |
| 2 | “pregnant women” | |
| 3 | 1 OR 2 | |
| 4 | Calcium supplementation | calcium supplement* |
| 5 | “calcium carbonate” | |
| 6 | “calcium gluconate” | |
| 7 | “calcium acetate” | |
| 8 | “calcium citrate” | |
| 9 | “calcium lactate” | |
| 10 | 4 OR 5 OR 6 OR 7 OR 8 OR 9 | |
| 11 | Vitamin D supplementation | “vit* D supplement*” |
| 12 | “cholecalciferol” | |
| 13 | “ergocalciferol” | |
| 14 | 11 OR 12 OR 13 | |
| 15 | Calcium or Vitamin D | 10 OR 14 |
| 16 | Preeclampsia | “pre-eclampsia”[Mesh] ◈ |
| 17 | “eclampsia”[Mesh] ◈ | |
| 18 | “preeclampsia” | |
| 19 | “gestational hypertension” | |
| 20 | “gestational hypertensive disorder” | |
| 21 | “hypertensive disorder during pregnancy” | |
| 22 | “pregnancy induced hypertension” | |
| 23 | PIH | |
| 24 | “pre-eclamptic toxaemia” | |
| 25 | 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 | |
| 26 | 3 AND 15 AND 25 | |
| 27 | systematic[sb] AND 26 ◈ |
Appendix B
Appendix B.1. Data Extraction Form
| Study ID | ……………………………………………………………………… | ||
|---|---|---|---|
| Reviewer | ……………………………………………………………………… | ||
| Date of review | (DD/MM/YYYY) ………………………………….……………… | ||
| Study title | ……………………………………………………………………… | ||
| First Authors | ……………………………………………………………………… | ||
| Journal | ……………………………………………… | Year | ………… |
| Setting | ☐ 1. Hospital Based | ☐ 2. Community Based |
|---|---|---|
| Country of study | ………………………………………………………………… | |
| Study Design | ☐ 1. Randomized Controlled Trial | ☐ 2. Quasi-Experimental Design |
|---|---|---|
| Period of the study | ……………………………………………… months | |
| Pregnant Women | ☐ 1. Low Risk Women ☐ 2. High Risk Women |
|---|
| Calcium Supplementation | |||
| ☐ 1. Yes ☐ 2. No | |||
| Form | ☐ 1. Calcium carbonate ☐ 2. Calcium gluconate ☐ 3. Calcium acetate ☐ 4. Calcium citrate ☐ 5. Calcium lactate ☐ 6. Not specified ☐ 7. Other …………………………… | ||
| Dosage | …………………… g | Duration | ………… weeks |
| Timing | ☐ 1. Single Dose ☐ 2. Daily ☐ 3. Weekly ☐ 4. Monthly ☐ 5. Other ……………….. | ||
| Started at | ☐ 1. First Trimester (0 to 13 Weeks) ☐ 2. Second Trimester (14 to 26 Weeks) ☐ 3. Third Trimester (27 to 40 Weeks) ☐ 4. No mention | ||
| Co-Supplement | ☐ 1. Yes, specify…………………… ☐ 2. No | ||
| Vitamin D Supplementation | |||
| ☐ 1. Yes ☐ 2. No | |||
| Form | ☐ 1. Ergocalciferol ☐ 2 .Cholecalciferol ☐ 3. Not specified ☐ 4. Other …………………………… | ||
| Dosage | …………………… IU | Duration | ………… weeks |
| Timing | ☐ 1. Single Dose ☐ 2. Daily ☐ 3. Weekly ☐ 4. Monthly ☐ 5. Other ……………….. | ||
| Started at | ☐ 1. First Trimester (0 to 13 Weeks) ☐ 2. Second Trimester (14 to 26 Weeks) ☐ 3. Third Trimester (27 to 40 Weeks) ☐ 4. No mention | ||
| Co-Supplement | ☐ 1. Yes, specify…………………… ☐ 2. No | ||
| Calcium plus Vitamin D Supplementation | |||
| ☐ 1. Yes ☐ 2. No | |||
| Calcium Form | ☐ 1. Calcium carbonate ☐ 2. Calcium gluconate ☐ 3. Calcium acetate ☐ 4. Calcium citrate ☐ 5. Calcium lactate ☐ 6. Not specified ☐ 7. Other …………………………… | ||
| Dosage | …………………… g | Duration | ………… weeks |
| Timing | ☐ 1. Single Dose ☐ 2. Daily ☐ 3. Weekly ☐ 4. Monthly ☐ 5. Other ……………….. | ||
| Vit D Form | ☐ 1. Ergocalciferol ☐ 2 .Cholecalciferol ☐ 3. Not specified ☐ 4. Other …………………………… | ||
| Dosage | …………………… IU | Duration | ………… weeks |
| Timing | ☐ 1. Single Dose ☐ 2. Daily ☐ 3. Weekly ☐ 4. Monthly ☐ 5. Other ……………….. | ||
| Started at | ☐ 1. First Trimester (0 to 13 Weeks) ☐ 2. Second Trimester (14 to 26 Weeks) ☐ 3. Third Trimester (27 to 40 Weeks) ☐ 4. No mention | ||
| Co-Supplement | ☐ 1. Yes, specify…………………… ☐ 2. No | ||
| Characteristics | Intervention n = | Control n = | Total n = |
|---|---|---|---|
| Mean Age (year) | |||
| Mean Gestation age at enrolment (week) (mean, SD) | |||
| SBP (mean, SD) | |||
| DBP (mean, SD) | |||
| Abnormal Proteinuria (%) | |||
| BMI (mean, SD) | |||
| Primigravida (%) | |||
| Nulliparous (%) | |||
| Gestational Diabetes Mellitus (%) | |||
| Smoking (%) | |||
| Mean total weight gain (mean, SD) | |||
| % Withdraw (lost FU) | |||
| Mean gestational age at delivery (mean, SD) | |||
| Mean baseline calcium level (mean, SD) | |||
| Mean baseline vitamin D level (mean, SD) |
| Preeclampsia | ☐ 1. Yes ☐ 2. No | |
| ☐ Preeclampsia | ☐ SBP ≥ 140 mmHg, DBP ≥ 90 mmHg and Proteinuria >2+ | |
| ☐ Severe preeclampsia | ☐ SBP ≥ 160 mmHg, DBP ≥ 1100 mmHg and Proteinuria >2+ | |
| ☐ Early onset preeclampsia | ☐ preeclampsia occur <34 weeks’ gestation | |
| ☐ Late onset preeclampsia | ☐ preeclampsia occur ≥34 weeks’ gestation | |
| Eclampsia | ☐ 1. Yes ☐ 2. No | |
| GH or PIH | ☐ 1. Yes ☐ 2. No SBP ≥ 140 mmHg or DBP ≥ 90 mmHg | |
Appendix B.2. Intervention and Outcomes
| Treatment | Preeclampsia | |||
|---|---|---|---|---|
| Yes | No | RR/OR | 95% CI | |
| Calcium | ||||
| Vitamin D | ||||
| Calcium + Vit D | ||||
| Placebo | ||||
| Treatment | Eclampsia | |||
|---|---|---|---|---|
| Yes | No | RR/OR | 95% CI | |
| Calcium | ||||
| Vitamin D | ||||
| Calcium + Vit D | ||||
| Placebo | ||||
| Treatment | GH/PIH | |||
|---|---|---|---|---|
| Yes | No | RR/OR | 95% CI | |
| Calcium | ||||
| Vitamin D | ||||
| Calcium + Vit D | ||||
| Placebo | ||||
Appendix C. Cochrane “Risk of Bias” Assessment
| Low (2) | High (1) | Unclear (0) | Comment | |
|---|---|---|---|---|
| Adequate sequence generation | ☐ | ☐ | ☐ | |
| Allocation concealment | ☐ | ☐ | ☐ | |
| Blinding of participants and personnel | ☐ | ☐ | ☐ | |
| Blinding of outcome assessment | ☐ | ☐ | ☐ | |
| Incomplete outcome data addressed | ☐ | ☐ | ☐ | |
| Selective outcome reporting | ☐ | ☐ | ☐ | |
| Other sources of bias | ☐ | ☐ | ☐ |
Criteria for Judging Risk of Bias in the “Risk of Bias Assessment” Tool
| Selection Bias (Biased Allocation to Interventions) Due to Inadequate Generation of a Randomized Sequence | |
|---|---|
| Criteria for judgment of “Low risk” of bias | Randomization was performed using any of following methods: Using a random number table; Simple or block or stratified randomization by using a computer random number generator with or without detailed description of generation process; Tossing Coin; Shuffling cards or envelopes; Throwing dice; Drawing of lots; |
| Criteria for judgment of “High risk” of bias | Systematic, non-random sequence generation was performed using any of the follow methods: Odd or even sequence generated by birth date; Sequence generated by some rule based on date (or day) of admission; Sequence generated by some rule based on hospital or clinic record number. Categorized with non-random approach using any of the following methods: by judgement of the clinician; by preference of the participant; based on the results of a laboratory test or a series of tests; by availability of the intervention. |
| Criteria for judgment of “Unclear risk” of bias | Insufficient information about the sequence generation process to permit judgement of ‘Low risk’ or ‘High risk’. |
| Selection Bias (Biased Allocation to Interventions) Due to Inadequate Concealment of Allocations Prior to Assignment | |
|---|---|
| Criteria for judgment of “Low risk” of bias | If any of following was applied or mentioned Central allocation (including telephone, web-based and pharmacy-controlled randomization); Sequentially numbered drug containers of identical appearance; Sequentially numbered, opaque, sealed envelopes. |
| Criteria for judgment of “High risk” of bias | Authors used any of following Using an open random allocation schedule (e.g., a list of random numbers); Assignment envelopes were used without appropriate safeguards (e.g., if envelopes were unsealed or non-opaque or not sequentially numbered); Alternation or rotation; Date of birth; Case record number; Any other explicitly unconcealed procedure. |
| Criteria for judgment of “Unclear risk” of bias | Insufficient information to permit judgement of ‘Low risk’ or ‘High risk’. This is usually the case if the method of concealment is not described or not described in sufficient detail to allow a definite judgement–for example if the use of assignment envelopes is described, but it remains unclear whether envelopes were sequentially numbered, opaque and sealed |
| Performance Bias Due to Knowledge of the Allocated Interventions by Participants and Personnel during the Study | |
|---|---|
| Criteria for judgment of “Low risk” of bias | Any one of the following: Blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken; Incomplete blinding, such as blinding had to be uncovered because of characteristic side effect of intervention, but the outcome is not likely to be influenced by lack of blinding; No blinding, but the outcome is not likely to be influenced by lack of blinding. |
| Criteria for judgment of “High risk” of bias | Any one of the following: Single blinding of key study participants and personnel attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding; No blinding or incomplete blinding, and the outcome is likely to be influenced by lack of blinding. |
| Criteria for judgment of “Unclear risk” of bias | Any one of the following: Insufficient information to permit judgment of ‘Low risk’ or ‘High risk’; The study did not address this outcome. |
| Detection Bias Due to Knowledge of the Allocated Interventions by Outcome Assessors | |
|---|---|
| Criteria for judgment of “Low risk” of bias | Any one of the following: Blinding of outcome assessment ensured, and unlikely that the blinding could have been broken; No blinding of outcome assessment, but the outcome measurement is not likely to be influenced by lack of blinding. |
| Criteria for judgment of “High risk” of bias | Any one of the following: Blinding of outcome assessment, but likely that the blinding could have been broken and the outcome measurement is likely to be influenced by lack of blinding; No blinding of outcome assessment, and the outcome measurement is likely to be influenced by lack of blinding. |
| Criteria for judgment of “Unclear risk” of bias | Any one of the following: Insufficient information to permit judgment of ‘Low risk’ or ‘High risk’; The study did not address this outcome. |
| Attrition Bias Due to Amount, Nature or Handling of Incomplete Outcome Data | |
|---|---|
| Criteria for judgment of “Low risk” of bias | Any one of the following: No missing outcome data; By checking the similarity between the remaining patients and loss to follow up patients, the reasons for missing outcome data unlikely to be related to preeclampsia such as migrating to another area; Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate; For continuous outcome data, plausible effect size (difference in means or standardized difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size; Missing data have been imputed using appropriate methods. |
| Criteria for judgment of “High risk” of bias | Any one of the following: By checking the similarity between the remaining patients and loss to follow up patients, the reasons for missing outcome data likely to be related to preeclampsia such as diabetes mellitus, smoking status, BMI, with either imbalance in numbers or reasons for missing data across intervention groups; For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk is enough to induce clinically relevant bias in intervention effect estimate; For continuous outcome data, plausible effect size (difference in means or standardized difference in means), among missing outcomes enough to induce clinically relevant bias in observed effect size; ‘As-treated’ analysis done with substantial departure of the intervention received from that assigned at randomization; Potentially inappropriate application of simple imputation. |
| Criteria for judgment of “Unclear risk” of bias | Any one of the following: Insufficient reporting of attrition/exclusions to permit judgement of ‘Low risk’ or ‘High risk’ (e.g., number randomized not stated, no reasons for missing data provided); The study did not address this outcome. |
| Reporting Bias Due to Selective Outcome Reporting | |
|---|---|
| Criteria for judgment of “Low risk” of bias | Any of the following: The study protocol is available and all of the study‘s pre-specified outcomes (preeclampsia, maternal and fetal outcomes) which are of interest in the review have been reported in the pre-specified way; The study protocol is not available, but it is clear that the published reports include all expected outcomes, including those that were pre-specified. |
| Criteria for judgment of “High risk” of bias | Any one of the following: Not all of the study’s pre-specified primary outcomes (preeclampsia) have been reported; One or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g., early onset preeclampsia, late onset preeclampsia) that were not pre-specified; One or more reported primary outcomes were not pre-specified One or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta-analysis; The study report fails to include results for a key outcome that would be expected to have been reported for such a study. |
| Criteria for judgment of “Unclear risk” of bias | Insufficient information to permit judgement of ‘Low risk’ or ‘High risk’. It is likely that the majority of studies will fall into this category. |
| Bias Due to Problems Not Covered Elsewhere in the Table | |
|---|---|
| Criteria for judgment of “Low risk” of bias | The study appears to be free of other sources of bias like baseline imbalance of important factors like obesity, or smoking by checking characteristics of participants between groups |
| Criteria for judgment of “High risk” of bias | There is at least one important risk of bias. For example, the study: Had a potential source of bias related to the specific study design used (e.g., problem in randomization, protocol violation, in cluster-randomized trials, there is loss of clusters (or) in cross-over trials, there is carry-over effect); or Had been claimed to have been fraudulent; or Had some other problem. |
| Criteria for judgment of “Unclear risk” of bias | There may be a risk of bias, but there is either: Insufficient information to assess whether an important risk of bias exists; or Insufficient rationale or evidence that an identified problem will introduce bias. |
References
- Tranquilli, A.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.; Steyn, W.; Zeeman, G.; Brown, M. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the isshp. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2014, 4, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Abalos, E.; Cuesta, C.; Grosso, A.L.; Chou, D.; Say, L. Global and regional estimates of preeclampsia and eclampsia: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ananth, C.V.; Keyes, K.M.; Wapner, R.J. Pre-eclampsia rates in the United States, 1980–2010: Age-period-cohort analysis. BMJ 2013, 347, f6564. [Google Scholar] [CrossRef] [PubMed]
- Osungbade, K.O.; Ige, O.K. Public health perspectives of preeclampsia in developing countries: Implication for health system strengthening. J. Pregnancy 2011, 2011, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Abalos, E.; Cuesta, C.; Carroli, G.; Qureshi, Z.; Widmer, M.; Vogel, J.P.; Souza, J.P.; WHO Multicountry Survey on Maternal and Newborn Health Research Network. Pre-eclampsia, eclampsia and adverse maternal and perinatal outcomes: A secondary analysis of the world health organization multicountry survey on maternal and newborn health. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Berzan, E.; Doyle, R.; Brown, C.M. Treatment of preeclampsia: Current approach and future perspectives. Curr. Hypertens. Rep. 2014, 16, 473. [Google Scholar] [CrossRef] [PubMed]
- MacKay, A.P.; Berg, C.J.; Atrash, H.K. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet. Gynecol. 2001, 97, 533–538. [Google Scholar] [PubMed]
- Cunningham, F.G.; Roberts, J.M.; Taylor, R.N. The clinical spectrum of preeclampsia. In Chesley’s Hypertensive Disorders in Pregnancy, 4th ed.; Taylor, R.N., Roberts, J.M., Cunningham, F.G., Lindheimer, M.D., Eds.; Elsevier Science: Amsterdam, The Netherlands, 2014; pp. 25–36. [Google Scholar]
- Belizán, J.M.; Villar, J.; Repke, J. The relationship between calcium intake and pregnancy-induced hypertension: Up-to-date evidence. Am. J. Obstet. Gynecol. 1988, 158, 898–902. [Google Scholar] [CrossRef]
- Villar, J.; Belizan, J.M.; Fischer, P.J. Epidemiologic observations on the relationship between calcium intake and eclampsia. Int. J. Gynaecol. Obstet. 1983, 21, 271–278. [Google Scholar] [CrossRef]
- Villar, J.; Repke, J.; Belizan, J.M.; Pareja, G. Calcium supplementation reduces blood pressure during pregnancy: Results of a randomized controlled clinical trial. Obstet. Gynecol. 1987, 70, 317–322. [Google Scholar] [PubMed]
- Hofmeyr, G.J.; Atallah, A.N.; Duley, L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2006, CD001059. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Duley, L.; Atallah, A. Dietary calcium supplementation for prevention of pre-eclampsia and related problems: A systematic review and commentary. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2010, CD001059. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Torloni, M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2014, 6, CD001059. [Google Scholar]
- World Health Organization. Guideline: Calcium Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Pérez-López, F.R. Vitamin D: The secosteroid hormone and human reproduction. Gynecol. Endocrinol. 2007, 23, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Pena-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016, CD008873. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin d level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.C.; Holroyd, C.; Ntani, G.; Javaid, K.; Cooper, P.; Moon, R.; Cole, Z.; Tinati, T.; Godfrey, K.; Dennison, E. Vitamin d supplementation in pregnancy: A systematic review. Health Technol. Assess. (Winch. Engl.) 2014, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P. The prisma extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health (UK). Hypertension in Pregnancy: The Management of Hypertensive Disorders during Pregnancy. (Nice Clinical Guidelines, No. 107); RCOG Press: London, UK, 2010. [Google Scholar]
- Higgins, J.P.T.; Douglas, G.A. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, 5th ed.; Higgins, J.P.T., Green, S., Eds.; Wiley: Chisester, UK, 2011. [Google Scholar]
- White, I.R. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar]
- Chaimani, A.; Salanti, G. Using network meta-analysis to evaluate the existence of small-study effects in a network of interventions. Res. Synth. Methods 2012, 3, 161–176. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Aghamohammadi, A.; Zafari, M. Calcium supplementation in pregnancy and prevention of hypertensive disorders in elderly women. Sci. Asia 2015, 41, 259–262. [Google Scholar] [CrossRef]
- Almirante, C. Calcium supplementation during pregnancy in the prevention of eph gestosis. Prenat. Neonatal Med. 1998, 3, 1–24. [Google Scholar]
- Bassaw, S.R.A.; Roopnarinesingh, H.; Homer, B. Prevention of hypertensive disorders of pregnancy. J. Obstet. Gynaecol. 1998, 18, 123–126. [Google Scholar] [PubMed]
- Belizan, J.M.; Villar, J.; Gonzalez, L.; Campodonico, L.; Bergel, E. Calcium supplementation to prevent hypertensive disorders of pregnancy. N. Engl. J. Med. 1991, 325, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Crowther, C.A.; Hiller, J.E.; Pridmore, B.; Bryce, R.; Duggan, P.; Hague, W.M.; Robinson, J.S. Calcium supplementation in nulliparous women for the prevention of pregnancy-induced hypertension, preeclampsia and preterm birth: An australian randomized trial. Fracog and the act study group. Aust. N. Z. J. Obstet. Gynaecol. 1999, 39, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Devi, S.G.; Batra, S.; Singh, C.; Shukla, D.K. Calcium supplementation for the prevention of pre-eclampsia. Int. J. Gynaecol. Obstet. 2009, 104, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.J.; Hauth, J.C.; Curet, L.B.; Sibai, B.M.; Catalano, P.M.; Morris, C.D.; DerSimonian, R.; Esterlitz, J.R.; Raymond, E.G.; Bild, D.E.; et al. Trial of calcium to prevent preeclampsia. N. Engl. J. Med. 1997, 337, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo, P.; Delgado, F.; Jacome, P.; Teran, E.; Ruano, C.; Rivera, J. Calcium supplementation and the risk of preeclampsia in ecuadorian pregnant teenagers. Obstet. Gynecol. 1997, 90, 162–167. [Google Scholar] [CrossRef]
- Lopez-Jaramillo, P.; Narvaez, M.; Weigel, R.M.; Yepez, R. Calcium supplementation reduces the risk of pregnancy-induced hypertension in an andes population. Br. J. Obstet. Gynaecol. 1989, 96, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo, P.; Narvaez, M.; Felix, C.; Lopez, A. Dietary calcium supplementation and prevention of pregnancy hypertension. Lancet 1990, 335, 293. [Google Scholar] [CrossRef]
- Nenad, S.; Olivera, K.V.; Goran, R.; Ljiljana, S. P32. Did calcium management prevent preeclampsia? Pregnancy Hypertens. 2011, 1, 287. [Google Scholar] [CrossRef] [PubMed]
- Niromanesh, S.; Laghaii, S.; Mosavi-Jarrahi, A. Supplementary calcium in prevention of pre-eclampsia. Int. J. Gynaecol. Obstet. 2001, 74, 17–21. [Google Scholar] [CrossRef]
- Purwar, M.; Kulkarni, H.; Motghare, V.; Dhole, S. Calcium supplementation and prevention of pregnancy induced hypertension. J. Obstet. Gynaecol. Res. 1996, 22, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.S.; Fung, H.Y.; Hung, C.Y. Calcium and low-dose aspirin prophylaxis in women at high risk of pregnancy-induced hypertension. Hypertens. Pregnancy 1999, 18, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Ramos, L.; Briones, D.K.; Kaunitz, A.M.; Delvalle, G.O.; Gaudier, F.L.; Walker, C.D. Prevention of pregnancy-induced hypertension by calcium supplementation in angiotensin ii-sensitive patients. Obstet. Gynecol. 1994, 84, 349–353. [Google Scholar] [PubMed]
- Villar, J.; Abdel-Aleem, H.; Merialdi, M.; Mathai, M.; Ali, M.M.; Zavaleta, N.; Purwar, M.; Hofmeyr, J.; Nguyen, T.N.; Campodonico, L.; et al. World health organization randomized trial of calcium supplementation among low calcium intake pregnant women. Am. J. Obstet. Gynecol. 2006, 194, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Repke, J.T. Calcium supplementation during pregnancy may reduce preterm delivery in high-risk populations. Am. J. Obstet. Gynecol. 1990, 163, 1124–1131. [Google Scholar] [CrossRef]
- Wanchu, M.; Malhotra, S.; Khullar, M. Calcium supplementation in pre-eclampsia. J. Assoc. Phys. India 2001, 49, 795–798. [Google Scholar]
- Asemi, Z.; Hashemi, T.; Karamali, M.; Samimi, M.; Esmaillzadeh, A. Effects of vitamin d supplementation on glucose metabolism, lipid concentrations, inflammation, and oxidative stress in gestational diabetes: A double-blind randomized controlled clinical trial. Am. J. Clin. Nutr. 2013, 98, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Naghshineh, E.; Sheikhaliyan, S. Effect of vitamin d supplementation in the reduce risk of preeclampsia in nulliparous women. Adv. Biomed. Res. 2016, 5, 7. [Google Scholar] [PubMed]
- Sablok, A.; Batra, A.; Thariani, K.; Batra, A.; Bharti, R.; Aggarwal, A.R.; Kabi, B.; Chellani, H. Supplementation of vitamin d in pregnancy and its correlation with feto-maternal outcome. Clin. Endocrinol. 2015, 83, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Tabassi, Z.; Heidarzadeh, Z.; Khorammian, H.; Sabihi, S.-S.; Samimi, M. Effect of calcium-vitamin D supplementation on metabolic profiles in pregnant women at risk for pre-eclampsia: A randomized placebo-controlled trial. Pak. J. Biol. Sci. 2012, 15, 316–324. [Google Scholar] [PubMed]
- Marya, R.K.; Rathee, S.; Manrow, M. Effect of calcium and vitamin D supplementation on toxaemia of pregnancy. Gynecol. Obstet. Investig. 1987, 24, 38–42. [Google Scholar] [CrossRef]
- Samimi, M.; Kashi, M.; Foroozanfard, F.; Karamali, M.; Bahmani, F.; Asemi, Z.; Hamidian, Y.; Talari, H.; Esmaillzadeh, A. The effects of vitamin D plus calcium supplementation on metabolic profiles, biomarkers of inflammation, oxidative stress and pregnancy outcomes in pregnant women at risk for pre-eclampsia. J. Hum. Nutr. Diet. 2015, 29, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Taherian, A.A.; Taherian, A.; Shirvani, A. Prevention of preeclampsia with low-dose aspirin or calcium supplementation. Arch. Iran. Med. 2002, 5, 151–156. [Google Scholar]
- Hossain, N.; Kanani, F.H.; Ramzan, S.; Kausar, R.; Ayaz, S.; Khanani, R.; Pal, L. Obstetric and neonatal outcomes of maternal vitamin d supplementation: Results of an open-label, randomized controlled trial of antenatal vitamin d supplementation in pakistani women. J. Clin. Endocrinol. Metab. 2014, 99, 2448–2455. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Tang, I.C.; Henry, A.; Welsh, A. Limited evidence for calcium supplementation in preeclampsia prevention: A meta-analysis and systematic review. Hypertens. Pregnancy 2015, 34, 181–203. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Bhutta, Z.A. Effects of calcium supplementation during pregnancy on maternal, fetal and birth outcomes. Paediatr. Perinat. Epidemiol. 2012, 26, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.; Karumanchi, S.A.; Lafayette, R. Pathophysiology of the clinical manifestations of preeclampsia. Clin. J. Am. Soc. Nephrol. 2007, 2, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Jim, B.; Karumanchi, S.A. Preeclampsia: Pathogenesis, Prevention, and Long-Term Complications. Semin. Nephrol. 2017, 37, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M.; Hubel, C.A. The two stage model of preeclampsia: Variations on the theme. Placenta 2009, 30, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Repke, J.; Belizan, J. Relationship of blood pressure, calcium intake, and parathyroid hormone. Am. J. Clin. Nutr. 1989, 49, 183–184. [Google Scholar] [PubMed]
- Cardus, A.; Parisi, E.; Gallego, C.; Aldea, M.; Fernandez, E.; Valdivielso, J. 1,25-dihydroxyvitamin D3 stimulates vascular smooth muscle cell proliferation through a vegf-mediated pathway. Kidney Int. 2006, 69, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Evans, K.N.; Bulmer, J.N.; Kilby, M.D.; Hewison, M. Vitamin D and placental-decidual function. J. Soc. Gynecol. Investig. 2004, 11, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Hollis, B.W.; Kotsa, K.; Fakhoury, H.; Karras, S.N. Vitamin D administration during pregnancy as prevention for pregnancy, neonatal and postnatal complications. Rev. Endocr. Metab. Disord. 2017, 18, 307–322. [Google Scholar] [CrossRef] [PubMed]


| Author (Year) | Country | Outcome | Study Period (Months) | Type of Pregnancy | n Control | n Intervention | Supplement Started GA (Weeks) | Mean Age (Years) | Mean GA at Enrolment (Weeks) | Mean GA at Delivery (Weeks) | SBP (mmHg) | DBP (mmHg) | BMI (kg/m2) | Weight Gain (g/Week) | Nulliparity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Calcium vs. Placebo | |||||||||||||||
| Aghamohammadi (2015) [28] | Iran | PE | - | High Risk Women | 40 | 40 | <20 weeks | 37.15 | - | - | - | - | 26.8 | - | - |
| Almirante (1998) [29] | Philippines | PE | - | High Risk Women | 210 | 212 | <20 weeks | - | 18.00 | - | - | - | - | - | 100.00 |
| Bassaw (1998) [30] | Bangladesh | Both | 36 | Low Risk Women | 250 | 81 | <20 weeks | 27 | - | 38.6 | - | - | - | - | - |
| Belizan (1991) [31] | Argentina | Both | 33 | High Risk Women | 588 | 579 | ≥20 weeks | 23.70 | 20.80 | - | 103.95 | 66.45 | - | - | 100.00 |
| Crowther (1999) [32] | Australian | Both | 53 | Low Risk Women | 229 | 227 | ≥20 weeks | 24.70 | 18.37 | - | 115.80 | 68.20 | 26.60 | - | 100.00 |
| Kumar (2009) [33] | New Delhi | PE | 36 | Low Risk Women | 251 | 273 | <20 weeks | 21.85 | 17.83 | 38.44 | 113.19 | 74.00 | 23.35 | - | - |
| Levine (1997) [34] | US | Both | 36 | Low Risk Women | 2294 | 2295 | <20 weeks | 21.00 | 17.15 | 38.90 | 106.50 | 59.70 | - | - | 100.00 |
| Lopez-Jaramillo (1997) [35] | Ecuador | PE | 56 | High Risk Women | 135 | 125 | ≥20 weeks | 15.99 | 20.00 | 39.13 | - | - | - | 414.19 | 100.00 |
| Lopez-Jaramillo (1990) [37] | Ecuador | Both | 30 | Low Risk Women | 34 | 22 | ≥20 weeks | 19.4 | - | - | - | - | - | - | 100.00 |
| Lopez-Jaramillo (1989) [36] | Ecuador | GH/PIH | 30 | Low Risk Women | 43 | 49 | ≥20 weeks | 18.47 | 23.00 | - | - | - | - | 430.80 | 100.00 |
| Nenad (2011) [38] | Serbia | Both | - | Low Risk Women | 4588 | 4590 | <20 weeks | - | 18.50 | - | - | - | - | - | 100.00 |
| Niromanesh (2001) [39] | Iran | Both | - | High Risk Women | 15 | 15 | ≥20 weeks | 23.15 | 29.70 | 38.60 | - | - | - | - | - |
| Puwar (1996) [40] | India | Both | 15 | Low Risk Women | 93 | 97 | ≥20 weeks | 21.93 | 18.07 | 37.50 | 103.02 | 63.32 | - | - | 100.00 |
| Rogers (1999) [41] | Hong Kong | GH/PIH | 30 | High Risk Women | 75 | 144 | ≥20 weeks | 27.31 | 21.67 | 38.9 | - | - | - | - | 100.00 |
| Sanchez-Ramos (1994) [42] | Florida | Both | 55 | High Risk Women | 34 | 29 | ≥20 weeks | 18.38 | 24.44 | - | 113.50 | 64.01 | - | - | 100.00 |
| Villar (1987) [11] | Baltimore, Argentina | GH/PIH | 36 | Low Risk Women | 27 | 25 | ≥20 weeks | 21.10 | - | - | - | - | - | 388.2 | 100.00 |
| Villar (1990) [44] | Baltimore | Both | 36 | High Risk Women | 88 | 90 | ≥20 weeks | 16.25 | 23.55 | 38.55 | 102.75 | 61.10 | - | - | 85.26 |
| Villar (2006) [43] | Argentina, Egypt, India, Peru, South Africa, Vietnam | Both | 21 | Low Risk Women | 4161 | 4151 | <20 weeks | 22.65 | 15.10 | - | 105.05 | 60.80 | 21.90 | - | 100.00 |
| Wanchu (2001) [45] | India | PE | - | High Risk Women | 50 | 50 | ≥20 weeks | - | 14.2 | - | 111.57 | 72.45 | - | - | 100.00 |
| Vitamin D vs. Placebo | |||||||||||||||
| Asemi (2013) [46] | Iran | PE | 4 | High Risk Women | 27 | 27 | ≥20 weeks | 17.44 | 26 | - | - | - | 30.8 | - | - |
| Naghshineh (2016) [47] | Iran | PE | 5 | High Risk Women | 70 | 68 | <20 weeks | 25 | - | 37.4 | - | - | - | - | 100.00 |
| Sablok (2015) [48] | India | PE | 36 | High Risk Women | 57 | 108 | <20 weeks | - | - | - | - | - | - | - | 100.00 |
| Calcium plus Vitamin D vs. Placebo | |||||||||||||||
| Asemi (2012) [49] | Pakistan | PE | 11 | High Risk Women | 25 | 24 | ≥20 weeks | 24.9 | - | - | - | - | 27.58 | - | 100.00 |
| Marya (1987) [50] | India | PE | - | Low Risk Women | 200 | 200 | ≥20 weeks | - | 22.00 | - | - | - | - | - | - |
| Taherian (2002) [52] | Iran | PE | 36 | Low Risk Women | 330 | 330 | ≥20 weeks | 21.55 | 20.00 | 38.80 | 97.25 | 57.88 | 22.55 | 10.25 * | - |
| Samimi (2015) [51] | Iran | PE | 6 | High Risk Women | 30 | 30 | ≥20 weeks | 27.2 | - | - | 111.7 | 72.4 | 26.5 | - | - |
| Calcium plus Vitamin D vs. Calcium | |||||||||||||||
| Hossain (2014) [53] | Pakistan | Both | 21 | Low Risk Women | 89 | 86 | ≥20 weeks | 25.57 | 20.00 | 37.61 | - | - | 23.64 | - | - |
| Intervention | Calcium | Vitamin D | Calcium + Vitamin D |
|---|---|---|---|
| Calcium | 0.49 (0.35 0.69) * {66.1, 31.6} | 0.89 (0.33, 2.41) *† | 1.18 (0.58, 2.37) *‡ |
| Vitamin D | 0.43 (0.17, 1.11) † {70.7, 47.4} | 1.33 (0.42, 4.18) †‡ | |
| Calcium + Vitamin D | 0.57 (0.30, 1.10) ‡ {52.2, 19.6} |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaing, W.; Vallibhakara, S.A.-O.; Tantrakul, V.; Vallibhakara, O.; Rattanasiri, S.; McEvoy, M.; Attia, J.; Thakkinstian, A. Calcium and Vitamin D Supplementation for Prevention of Preeclampsia: A Systematic Review and Network Meta-Analysis. Nutrients 2017, 9, 1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9101141
Khaing W, Vallibhakara SA-O, Tantrakul V, Vallibhakara O, Rattanasiri S, McEvoy M, Attia J, Thakkinstian A. Calcium and Vitamin D Supplementation for Prevention of Preeclampsia: A Systematic Review and Network Meta-Analysis. Nutrients. 2017; 9(10):1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9101141
Chicago/Turabian StyleKhaing, Win, Sakda Arj-Ong Vallibhakara, Visasiri Tantrakul, Orawin Vallibhakara, Sasivimol Rattanasiri, Mark McEvoy, John Attia, and Ammarin Thakkinstian. 2017. "Calcium and Vitamin D Supplementation for Prevention of Preeclampsia: A Systematic Review and Network Meta-Analysis" Nutrients 9, no. 10: 1141. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9101141