Micronutrient Deficiencies among Breastfeeding Infants in Tanzania

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Blood Sampling
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wang, H.; Bhutta, Z.A.; Coates, M.M.; Coggeshall, M.; Dandona, L.; Diallo, K.; Franca, E.B.; Fraser, M.F.; Nancy, G.; Peter, W.; et al. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1725–1774. [Google Scholar] [CrossRef]
- UNDP. Sustainable Development Goals: Goal 3: Good Health and Well Being: Goal 3 Targets. Available online: http://www.undp.org/content/undp/en/home/sustainable-development-goals/goal-3-good-health-and-well-being/targets/ (accessed on 30 April 2017).
- UN Inter-Agency Group for Child Mortality Estimation. Levels and Trends in Child Mortality; Report; UNICEF: New York, NY, USA, 2015; Available online: https://www.unicef.org/publications/files/Child_Mortality_Report_2015_Web_9_Sept_15.pdf (accessed on 30 April 2017).
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Black, R.E.; Morris, S.S.; Bryce, J. Where and why are 10 million children dying every year? Lancet 2003, 361, 2226–2234. [Google Scholar] [CrossRef]
- Bailey, R.L.; West, K.P.; Black, R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015, 66 (Suppl. S2), 22–33. [Google Scholar] [CrossRef] [PubMed]
- Muthayya, S.; Rah, J.H.; Sugimoto, J.D.; Roos, F.F.; Kraemer, K.; Black, R.E. The Global Hidden Hunger Indices and Maps: An Advocacy Tool for Action. PLoS ONE 2013, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ruel-Bergeron, J.C.; Stevens, G.A.; Sugimoto, J.D.; Roos, F.F.; Ezzati, M.; Black, R.E.; Kraemer, K. Global update and trends of hidden hunger, 1995–2011: The hidden hunger Index. PLoS ONE 2015, 10, e0143497. [Google Scholar] [CrossRef] [PubMed]
- Hettiarachchi, M.; Liyanage, C. Coexisting micronutrient deficiencies among Sri Lankan pre-school children: A community-based study. Matern. Child Nutr. 2012, 8, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Khan, M.R.; Banu, C.P.; Qazi, M.R.; Akhtaruzzaman, M. The coexistence of other micronutrient deficiencies in anaemic adolescent schoolgirls in rural Bangladesh. Eur. J. Clin. Nutr. 2008, 62, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Ulak, M.; Chandyo, R.K.; Thorne-Lyman, A.L.; Henjum, S.; Ueland, P.M.; Midttun, Ø.; Shrestha, P.; Fawzi, W.; Graybill, L.; Strand, T.A. Vitamin Status among Breastfed Infants in Bhaktapur, Nepal. Nutrients 2016, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Pinzone, M.R.; Di Rosa, I.; Malaguarnera, M.; Madeddu, G. Vitamin D deficiency in HIV infection: An underestimated and undertreated epidemic. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1218–1232. [Google Scholar] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide health problem. Am. J. Clin. Nutr. 2008, 87, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and Immune Function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K. Vitamin D status during pregnancy. Curr. Opin. Obstet. Gynecol. 2011, 23, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Greer, F.R. 25-Hydroxyvitamin D: Functional outcomes in infants and young children. Am. J. Clin. Nutr. 2008, 88, 529S–533S. [Google Scholar] [PubMed]
- De Benoist, B. Conclusions of a WHO Technical Consultation on Folate and Vitamin B12 Deficiencies. Food Nutr. Bull. 2008, 29, S238–S244. [Google Scholar] [CrossRef] [PubMed]
- Akcaboy, M.; Malbora, B.; Zorlu, P.; Altınel, E.; Oguz, M.M.; Senel, S. Vitamin B12 Deficiency in Infants. Indian J. Pediatr. 2015, 82, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Vitamin B12 metabolism and status during pregnancy, lactation and infancy. Adv. Exp. Med. Biol. 1994, 352, 173–186. [Google Scholar] [PubMed]
- Allen, L.H. Causes of vitamin B12 and folate deficiency. Food Nutr. Bull. 2008, 29, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Casterline, J.E.; Allen, L.H.; Ruel, M.T. Vitamin B-12 deficiency is very prevalent in lactating Guatemalan women and their infants at three months postpartum. J. Nutr. 1997, 127, 1966–1972. [Google Scholar] [PubMed]
- Cobayashi, F.; Tomita, L.Y.; Augusto, R.A.; D’Almeida, V.; Cardoso, M.A. Genetic and environmental factors associated with vitamin B12 status in Amazonian children. Public Health Nutr. 2015, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bjørke-Monsen, A.L.; Ueland, M. Cobalamin status in children. J. Inherit. Metab. Dis. 2011, 34, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Lamers, Y. Folate recommendations for pregnancy, lactation, and infancy. Ann. Nutr. Metab. 2011, 59, 32–37. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.L.; Green, T.; Picciano, M.F. Maternal folate status and lactation. J. Mammary Gland Biol. Neoplasia 1997, 2, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Balarajan, Y.; Ramakrishnan, U.; Özaltin, E.; Shankar, A.H.; Subramanian, S.V. Anaemia in low-income and middle-income countries. Lancet 2011, 378, 2123–2135. [Google Scholar] [CrossRef]
- Lozoff, B.; Beard, J.; Connor, J.; Felt, B.; Georgieff, M.; Schallert, T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006, 64, S34–S43. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Lou, J.; Rao, R.; Georgieff, M.K.; Kaciroti, N.; Felt, B.T.; Zhao, Z.; Lozoff, B. Maternal serum ferritin concentration is positively associated with newborn iron stores in women with low ferritin status in late pregnancy. J. Nutr. 2012, 142, 2004–2009. [Google Scholar] [CrossRef] [PubMed]
- Siddappa, A.M.; Rao, R.; Long, J.D.; Widness, J.A.; Georgieff, M.K. The Assessment of Newborn Iron Stores at Birth: A review of the Literature and Standards for Ferritin Concentrations. Neonatology 2007, 92, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Bahl, R.; Bhandari, N.; Dube, B.; Edmond, K.; Fawzi, W.; Fontaine, O.; Kaur, J.; Kirkwood, B.; Martines, J.; Masanja, H.; et al. Efficacy of early neonatal vitamin A supplementation in reducing mortality during infancy in Ghana, India and Tanzania: Study protocol for a randomized controlled trial. Trials 2012, 13, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masanja, H.; Smith, E.R.; Muhihi, A.; Briegleb, C.; Mshamu, S.; Ruben, J.; Noor, R.A.; Yoshida, P.; Martines, J.; Bahl, R.; et al. Effect of neonatal vitamin A supplementation on mortality in infants in Tanzania (Neovita): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 385, 1324–1332. [Google Scholar] [CrossRef]
- Bio-Rad. Bio-Rad Quantaphase B-12/Folate Radioassay Instruction Manual. Indianapolis (IN); Roche Diagnostics: Basel, Switzerland, 1995. [Google Scholar]
- Institute of Medicine (IOM). Dietary Reference Intakes for Calcium and Vitamin D; The National Academy Press: Washington, DC, USA, 2011. [Google Scholar]
- World Health Organization (WHO). Serum ferritin concentrations for the assessment of iron status and iron deficiency in populations. In Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Rao, R.; Georgieff, M.K. Iron in fetal and neonatal nutrition. Semin. Fetal Neonatal Med. 2007, 12, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Spiegelman, D.; Hertzmark, E. Easy SAS Calculations for Risk or Prevalence Ratios and Differences. Am. J. Epidemiol. 2005, 162, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Toko, E.N.; Sumba, O.P.; Daud, I.I.; Ogolla, S.; Majiwa, M.; Krisher, J.T.; Mehta, S. Maternal Vitamin D Status and Adverse Birth Outcomes in Children from Rural Western Kenya. Nutrients 2016, 8, 794. [Google Scholar] [CrossRef] [PubMed]
- Cusick, S.E.; Opoka, R.O.; Lund, T.C.; John, C.C.; Polgreen, L.E. Vitamin D insufficiency is common in Ugandan children and is associated with severe malaria. PLoS ONE 2014, 9, e113185. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.C.; Stewart, A.W.; Scragg, R.; Milne, T.; Rowden, J.; Ekeroma, A.; Wall, C.; Mitchell, E.A.; Crengle, S.; Trencholme, A.; et al. Vitamin D during Pregnancy and Infancy and Infant Serum 25-Hydroxyvitamin D Concentration. Pediatrics 2014, 133, e143–e153. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.E.; Nelson, S.E.; Jeter, J.M. Iron Stores of Breastfed Infants during the First Year of Life. Nutrients 2014, 6, 2023–2034. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A. Vitamin D and the breastfed infant. J. Obstet. Gynecol. Neonatal Nurs. 2005, 34, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Duggan, C.; Srinivasan, K.; Thomas, T.; Samuel, T.; Rajendran, R.; Muthayya, S.; Kurpad, A.V. Vitamin B-12 supplementation during pregnancy and early lactation increases maternal, breast milk, and infant measures of vitamin B-12 status. J. Nutr. 2014, 144, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Kearns, A.; Hurst, T.; Caglia, J.; Langer, A. Focused Antenatal Care in Tanzania. Country Level Programs. 2014. Available online: http://www.mhtf.org/wp-content/uploads/sites/32/2014/09/HSPH-Tanzania5.pdf (accessed on 30 April 2017).
- WHO. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. 2016. Available online: http://apps.who.int/iris/bitstream/10665/250796/1/9789241549912-eng.pdf?ua=1 (accessed on 30 April 2017).



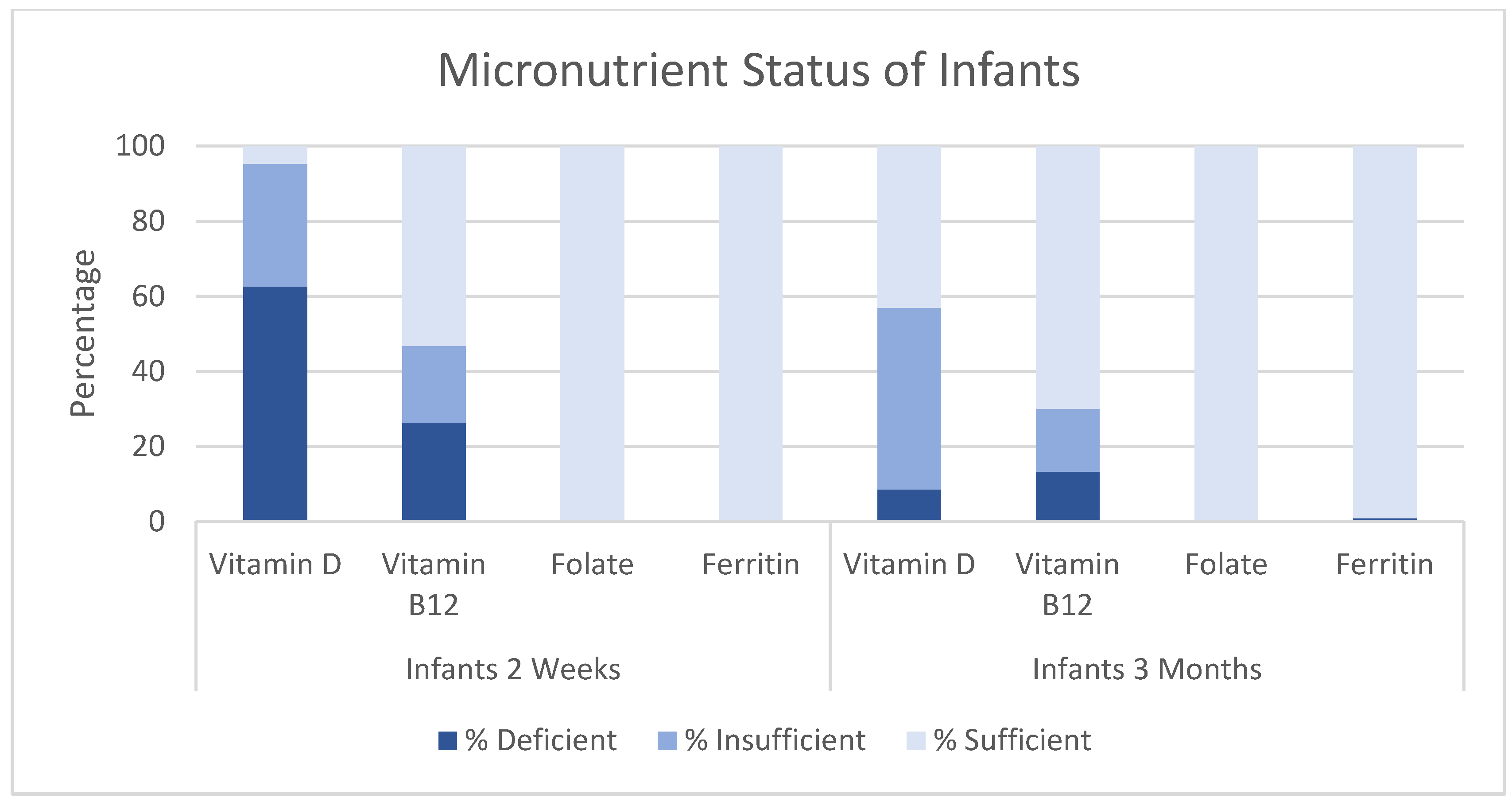{kind=link}
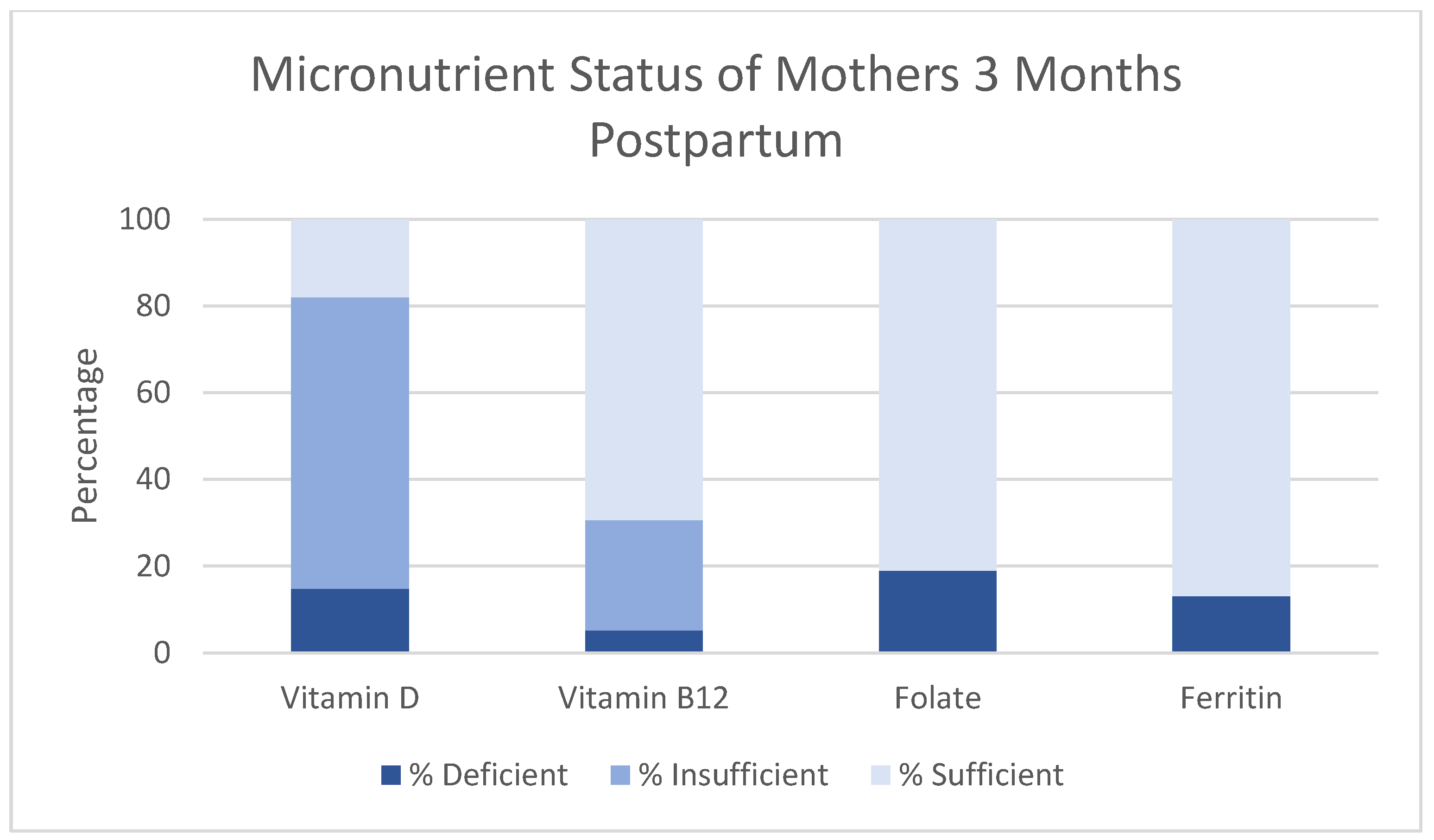{kind=link}
| Indicator | Definition | Population | Cutoff |
|---|---|---|---|
| Serum 25(OH)D | Vitamin D Deficiency [34] | All Ages | <50 nmol/L |
| Insufficient Vitamin D [34] | All Ages | 50–75 nmol/L | |
| Serum Vitamin B12 | Vitamin B12 Deficiency [18] | All Ages | <203 pg/mL |
| Insufficient Vitamin B12 [18] | All Ages | 203–271 pg/mL | |
| Serum Folate | Folate Deficiency [18] | All Ages | <4 ng/ml |
| Serum Ferritin | Iron Deficiency | Adults [35] | <15 ng/mL |
| Infants 3 months [35] | <12 ng/mL | ||
| Infants 2 weeks [36] | <30 ng/mL |
| Infants 2 Weeks (n = 446) | Infants 3 Months (n = 408) | |
|---|---|---|
| Infant Characteristics | ||
| Age (weeks) (mean (SD)) | 2.4 (0.3) | 13.2 (0.5) |
| Male (n (%)) | 231 (51.8) | 214 (52.5) |
| Preterm (<37 weeks) (n (%)) | 51 (13.1) | 50 (16.9) |
| Birthweight (g) (mean (SD)) | 3084.3 (449.5) | 3063.3 (475.6) |
| Small for gestational age (n (%)) | 68 (17.4) | 56 (19.0) |
| Twin or triplet (n (%)) | 8 (1.8) | 13 (3.2) |
| Cesarean section (n (%)) | 26 (5.8) | 18 (4.4) |
| Breastfed within 1 h of birth (n (%)) | 395 (88.6) | 374 (91.7) |
| Fed Colostrum (n (%)) | 435 (97.5) | 401 (98.3) |
| Breastfeeding status at 3 months (n (%)) | ||
| Exclusive | 1 | 175 (42.9) |
| Predominant/Partial | 1 | 189 (46.3) |
| None | 1 | 8 (2.0) |
| Unknown/missing | 1 | 36 (8.8) |
| Randomized to Vitamin A group (n (%)) | 215 (48.2) | 214 (52.4) |
| Residency 2 | ||
| Urban (n (%)) | 66 (14.8) | 141 (34.6) |
| Rural (n (%)) | 380 (85.2) | 267 (65.4) |
| Maternal Characteristics | ||
| Maternal Age (mean (SD)) | 25.0 (5.8) | 26.4 (6.3) |
| First Pregnancy (n (%)) | 98 (22.0) | 84 (20.6) |
| Maternal Education (n (%)) | ||
| None | 35 (7.9) | 34 (8.3) |
| Primary | 359 (80.5) | 314 (77.0) |
| Secondary+ | 39 (8.7) | 46 (11.2) |
| Missing | 13 (2.9) | 14 (3.43) |
| Provided Maternal Vitamin A Supplement (n (%)) | 142 (31.9) | 111 (27.2) |
| Antenatal Care Visits ≥ 4 (n (%)) 3 | 103 (23.1) | 103 (25.3) |
| Infants Two Weeks | Infants Three Months | Mothers Three Months Postpartum | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | Median (Q1, Q3) * | n | Mean (SD) | Median (Q1, Q3) * | n | Mean (SD) | Median (Q1, Q3) * | |
| Vitamin D (nmol/L) | 428 | 47.6 (14.8) | 45.5 (37.1–55.6) | 405 | 75.0 (21.5) | 72.7 (60.6–86.0) | 427 | 63.7 (14.8) | 61.8 (53.3–71.6) |
| Vitamin B12 (pg/mL) | 254 | 310.3 (154.0) | 279.6 (197.3–378.9) | 324 | 370.7 (190.8) | 332.1 (248.3–434.8) | 427 | 434.6 (202.3) | 395.4 (286.8–523.5) |
| Folate (ng/mL) | 253 | 15.5 (5.8) | 14.3 (11.2–18.3) | 324 | 20.9 (8.1) | 19.4 (15.2–27.8) | 427 | 7.3 (4.4) | 6.1 (4.4–8.8) |
| Ferritin (ng/mL) | 250 | 318.9 (192.9) | 274.2 (192.2–393.8) | 324 | 142.1 (165.2) | 102.8 (59.9–170.2) | 427 | 39.4 (44.2) | 25.9 (14.6–47.7) |
| Infants Two Weeks | Infants Three Months | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate 5 | |||||||
| n (%) | RR (95% CI) | p Value | RR (95% CI) | p Value | n (%) | RR (95% CI) | p Value | RR (95% CI) | p Value | |
| Low Birthweight 1 | 28 (6.5) | 1.03 (0.77, 1.37) | 0.85 | 0.99 (0.75, 1.33) | 1.00 | 31 (7.7) | 3.02 (1.43, 6.34) | 0.004 | 4.37 (1.95, 9.77) | 0.0003 |
| Preterm 2 | 50 (13.4) | 0.95 (0.74, 1.21) | 0.66 | 0.93 (0.73, 1.18) | 0.57 | 50 (17.1) | 1.48 (0.67, 3.26) | 0.33 | 1.57 (0.72, 3.45) | 0.26 |
| Male | 225 (52.6) | 0.96 (0.83, 1.11) | 0.56 | 0.97 (0.84, 1.11) | 0.63 | 212 (52.4) | 0.96 (0.51, 1.82) | 0.91 | 0.97 (0.53, 1.77) | 0.92 |
| Urban Residence 3 | 66 (15.4) | 1.05 (0.86, 1.27) | 0.63 | 1.10 (0.90, 1.34) | 0.37 | 141 (34.8) | 1.98 (1.06, 3.72) | 0.03 | 2.95 (1.46, 5.97) | 0.003 |
| ANC < 4 4 | 232 (69.9) | 1.00 (0.83, 1.2) | 0.99 | 1.03 (0.85, 1.23) | 0.79 | 218 (67.9) | 1.08 (0.46, 2.54) | 0.86 | 1.21 (0.52, 2.81) | 0.65 |
| Maternal Education | ||||||||||
| None | 34 (8.2) | Ref (1.00) | Ref (1.00) | 34 (8.7) | Ref (1.00) | Ref (1.00) | ||||
| Primary (1–7) | 342 (82.4) | 1.57 (1.10, 2.24) | <0.0001 * | 1.58 (1.10, 2.26) | <0.0001 * | 312 (79.8) | 4.46 (0.62, 32.00) | 0.17 * | 5.15 (1.04, 25.53) | 0.03 * |
| Secondary+ (>7) | 39 (9.4) | 2.03 (1.39, 2.96) | 2.05 (1.40, 3.00) | 45 (11.5) | 5.33 (0.65, 43.91) | 8.45 (1.45, 49.18) | ||||
| Maternal Age (years) | ||||||||||
| <20 | 78 (18.2) | Ref (1.00) | Ref (1.00) | 65 (16.1) | Ref (1.00) | Ref (1.00) | ||||
| 20–25 | 171 (40.0) | 0.86 (0.72, 1.04) | 0.52 | 0.84 (0.70, 1.01) | 0.70 | 129 (31.9) | 0.71 (0.23, 2.14) | 0.37 * | 0.55 (0.16, 1.85) | 0.16 * |
| 26–29 | 81 (18.9) | 0.79 (0.62, 1.00) | 0.80 (0.63, 1.02) | 83 (20.5) | 1.88 (0.70, 5.07) | 1.95 (0.72, 5.32) | ||||
| 30+ | 98 (22.9) | 0.93 (0.76, 1.14) | 0.94 (0.77, 1.14) | 128 (31.6) | 1.12 (0.41, 3.08) | 1.21 (0.45, 3.26) | ||||
| Maternal Vitamin D Status | ||||||||||
| Maternal Vitamin D >50nmol/L | n/a | n/a | n/a | 307 (75.8) | Ref (1.00) | Ref (1.00) | ||||
| Maternal Vitamin D <50nmol/L | n/a | n/a | n/a | 54 (15.0) | 3.29 (1.66,6.52) | 0.0006 | 2.83 (1.45, 5.52) | 0.002 | ||
| Infants Two Weeks | Infants Three Months | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate 6 | Univariate | Multivariate 6 | |||||||
| n (%) | RR (95% CI) | p Value | RR (95% CI) | p Value | n (%) | RR (95% CI) | p Value | RR (95% CI) | p Value | |
| Low Birthweight 1 | 18 (7.1) | 0.83 (0.34, 2.03) | 0.69 | 0.93 (0.42, 2.07) | 0.86 | 26 (8.0) | 1.51 (0.65, 3.50) | 0.34 | 1.06 (0.43, 2.56) | 0.89 |
| Preterm 2 | 30 (14.3) | 0.75 (0.35, 1.59) | 0.45 | 0.85 (0.39, 1.83) | 0.67 | 31 (13.6) | 0.71 (0.23, 2.19) | 0.55 | 0.65 (0.24, 1.79) | 0.41 |
| Male | 140 (55.1) | 0.89 (0.59, 1.34) | 0.58 | 0.87 (0.58, 1.30) | 0.49 | 176 (54.3) | 1.29 (0.73, 2.28) | 0.39 | 1.11 (0.65, 1.91) | 0.70 |
| Urban Residence 3 | 62 (24.4) | 0.68 (0.39, 1.18) | 0.17 | 0.64 (0.36, 1.14) | 0.13 | 140 (43.2) | 0.63 (0.35, 1.15) | 0.14 | 1.01 (0.57, 1.80) | 0.98 |
| ANC < 4 4 | 142 (69.6) | 1.04 (0.63, 1.71) | 0.89 | 0.99 (0.60, 1.63) | 0.97 | 171 (64.5) | 1.47 (0.71, 3.02) | 0.30 | 1.68 (0.84, 3.37) | 0.14 |
| Maternal Education | ||||||||||
| None | 20 (8.2) | Ref (1.00) | Ref (1.00) | 27 (8.6) | Ref (1.00) | Ref (1.00) | ||||
| Primary (1–7) | 197 (80.4) | 1.25 (0.59, 2.65) | 0.20 * | 1.32 (0.64, 2.73) | 0.12 * | 248 (79.0) | 0.82 (0.37, 1.82) | 0.55 * | 0.76 (0.39, 1.49) | 0.86 * |
| Secondary + (>7) | 28 (11.4) | 1.73 (0.72, 4.12) | 1.84 (0.79, 4.25) | 39 (12.4) | 0.63 (0.19, 2.06) | 0.94 (0.30, 2.88) | ||||
| Maternal Age (years) | ||||||||||
| <20 | 38 (15.0) | Ref (1.00) | Ref (1.00) | 53 (16.4) | Ref (1.00) | Ref (1.00) | ||||
| 20–25 | 112 (44.1) | 2.21 (0.82, 5.91) | 0.001 * | 2.29 (0.84, 6.22) | 0.0006 | 104 (32.1) | 0.31 (0.14, 0.71) | 0.23 * | 0.45 (0.20, 1.02) | 0.18 * |
| 26–29 | 47 (18.5) | 3.23 (1.18, 8.87) | 3.44 (1.22, 9.71) | 67 (20.7) | 0.67 (0.33, 1.37) | 1.01 (0.51, 2.00) | ||||
| 30+ | 57 (22.4) | 3.50 (1.30, 9.39) | 3.66 (1.35, 9.92) | 100 (30.9) | 0.45 (0.22, 0.93) | 0.49 (0.24, 1.01) | ||||
| Maternal Vitamin B12 Status 5 | ||||||||||
| Maternal Vitamin B12 Sufficiency | n/a | n/a | n/a | 227 (70.1) | Ref (1.00) | Ref (1.00) | ||||
| Maternal Vitamin B12 Insufficiency | n/a | n/a | n/a | 48 (16.6) | 3.72 (1.80, 7.68) | 0.0004 | 4.06 (1.88, 8.70) | 0.0003 | ||
| Maternal Vitamin B12 Deficiency | n/a | n/a | n/a | 14 (4.8) | 9.27 (4.69, 18.30) | <0.0001 | 9.63 (4.83, 19.17) | <0.0001 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellows, A.L.; Smith, E.R.; Muhihi, A.; Briegleb, C.; Noor, R.A.; Mshamu, S.; Sudfeld, C.; Masanja, H.; Fawzi, W.W. Micronutrient Deficiencies among Breastfeeding Infants in Tanzania. Nutrients 2017, 9, 1258. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9111258
Bellows AL, Smith ER, Muhihi A, Briegleb C, Noor RA, Mshamu S, Sudfeld C, Masanja H, Fawzi WW. Micronutrient Deficiencies among Breastfeeding Infants in Tanzania. Nutrients. 2017; 9(11):1258. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9111258
Chicago/Turabian StyleBellows, Alexandra L., Emily R. Smith, Alfa Muhihi, Christina Briegleb, Ramadhani A. Noor, Salum Mshamu, Christopher Sudfeld, Honorati Masanja, and Wafaie W. Fawzi. 2017. "Micronutrient Deficiencies among Breastfeeding Infants in Tanzania" Nutrients 9, no. 11: 1258. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9111258