
Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses


1
Department of Nursing and Physiotherapy, University of the Balearic Islands, 07122 Palma, Spain
2
Department of Nursing, University of Valencia, 46010 Valencia, Spain
3
Department of Methodology for the Behavioral Sciences, University of Valencia, 46010 Valencia, Spain
*
Author to whom correspondence should be addressed.
Nurs. Rep. 2021, 11(2), 311-319; https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020030
Submission received: 29 March 2021
/
Revised: 24 April 2021
/
Accepted: 26 April 2021
/
Published: 30 April 2021
Abstract
:Nursing has been identified as a very stressful profession. Specifically in end-of-life care, nurses frequently experience stressful situations related to death and dying. This study aims to develop and validate a short scale of stress in nurses, the Brief Nursing Stress Scale. A cross-sectional survey of Spanish end-of-life care professionals was conducted; 129 nurses participated. Analyses included a confirmatory factor analysis of the Brief Nursing Stress Scale, estimation of reliability, relation with sex, age and working place, and the estimation of a structural equation model in which BNSS predicted burnout and work satisfaction The confirmatory factor analysis showed an adequate fit: χ2(9) = 20.241 (p = 0.017); CFI = 0.924; SRMR = 0.062; RMSEA = 0.098 [0.040,0.156]. Reliability was 0.712. Women and men showed no differences in stress. Younger nurses and those working in hospital compared to homecare showed higher levels of stress. A structural equation model showed nursing stress positively predicted burnout, which in turn negatively predicted work satisfaction. Nursing stress also had an indirect, negative effect on work satisfaction. The Brief Nursing Stress Scale showed adequate estimates of validity, reliability, and predictive power in a sample of end-of-life care nurses. This is a short, easy-to-use measure that could be employed in major batteries assessing quality of healthcare institutions.
1. Introduction
Nursing has been generally identified as a very stressful profession, ‘by its very nature’ [1], and prevalence of occupational stress and burnout has been repeatedly stated [2,3]. In Spain, studies have pointed high levels of emotional exhaustion in nurses, and moderate levels of depersonalization [4,5].
Stress is an important cause of job dissatisfaction in nursing [6] and can cause job leaves [7]. It is worth highlighting that occupational stress among nurses usually decreases their efficiency of job performance, with a consequently negative effect on the quality of patient care and patient satisfaction [8,9]. Occupational stress has been related to staff conflicts, absenteeism, decreased productivity, lowered morale, and burnout, among others [10]. The immediate responses of the human body to occupational stress and burnout can be physiological, psychological, and behavioral. Stressful situations also have devastating consequences at the psychosomatic level, such as headaches, fatigue, nausea, skin rash, and weight fluctuations [11]; and several psychological symptoms have also been related to stress situations, including anxiety, nervousness, tension, depression, and irritation [12].
Research on nursing stress has pointed out several risk factors defining such stress, including working conditions like low job control and high job demands, being moved among different patient care units within the organization, being short of essential resources, and having low supportive work relationships with co-workers, supervisors, and/or physicians [13,14,15,16,17,18], together with personal variables, such as neuroticism and emotional coping [5]. These causes of stress are common to the nursing work environment and have been found in all specialties [15].
Specifically, in the palliative care context, nurses frequently experience stressful situations related to death and dying. Nursing providing end-of-life care face additional stressful and demanding situations, such as caring with scientific technical knowledge, decision-making related to ethical issues, and constant contact with suffering, end of life, and death of people for whom they care [19,20]. These challenges usually cause physical, psychological, and emotional distress as well as work-related stress, which can lead to the development of burnout [21,22].
Thus, some sources of stress identified as key in the nursing literature, both at a general level and in end-of-life care, include [23]: (1) stressful situations derived from the process of dying or death; (2) stressful situations derived from conflicts with physicians; (3) stressful situations derived from lack of support; (4) stressful situations derived from conflict between nurses; (5) stressful situations derived from workload; and (6) stressful situations derived from uncertainty of the treatment.
Due to its importance for the development of burnout and the well-being of nurses, but also due to the consequences on patients’ health and the quality of care, the measurement of stress in nursing is key for health institutions. As pointed, stress can cause job dissatisfaction [6], job leaves [7], and even the consumption of addictive substances [24]. However, the stressful conditions to be measured in the healthcare context are enormous, and having to answer infinite questionnaires makes the workload of the nurses even greater, limiting their valuable time. For these reasons, it is very important to have brief measures in place to screen and detect potential sources of stress. And then, only then, apply longer batteries, which allow us to deepen our understanding of these conditions and try to solve them.
To respond to these circumstances, the present study aims to develop and validate a short scale of stress in nurses, the Brief Nursing Stress Scale (BNSS). For this purpose, we will present the scale, study its internal structure, gather reliability evidence, and quantify its predictive power over burnout and work satisfaction.
2. Materials and Methods
2.1. Development of the Brief Nursing Stress Scale
The Brief Nursing Stress Scale (BNSS) is based the dimensions of stress pointed in the Nursing Stress Scale (NSS) [25], which included: (1) stressful situations derived from the process of dying or death; (2) stressful situations derived from conflicts with doctors; (3) stressful situations derived from lack of support; (4) stressful situations derived from conflict between nurses; (5) stressful situations derived from workload; and (6) stressful situations derived from uncertainty of the treatment. This scale is one of the most popular and widely used instrument to assess stressors in nursing [23] and was originally developed based on the psychological model of stress described by Lazarus [26] and Appley and Trumbull [27].
Taking into account the six stressors already pointed, two experts in nursing and methodology turned the dimensions into the six final items that composed the instrument. For example, if the dimension was “stressful situations derived from the process of dying or death”, the item corresponding to the dimension specifically asked for “how frequently you suffer stressful situations derived from the process of dying or death”. This procedure was used for the six dimensions. The sentences were rated according to agreement, using a Likert-type, 4-point scale, from 1 (never) to 4 (almost always); therefore, using the original scale of the Spanish version of the Nursing Stress Scale [28]. Total score was calculated with the mean of the scores in the six items, and ranged from 1 to 4. Item content can be consulted in Table 1.
2.2. Design, Setting, and Participants
A cross-sectional survey of Spanish end-of-life care professionals was conducted to assess variables influencing professionals’ compassionate care. This cross-sectional study has been reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement [29].
The survey was conducted during January–February 2020. Professionals were encouraged to participate through the Spanish Society for Palliative Care (SECPAL). Participants were sampled from their lists of members, who were asked to complete an online survey using SurveyMonkey, a secure and anonymous online platform that also restricted multiple survey responses. Participation was voluntary and required respondents’ informed consent.
For inclusion, the participants had to be a healthcare professional (physician, nurse, psychologist, nursing assistant, social worker, or others), who currently cared for patients at the end of their lives, but not necessarily in palliative care settings.
The sample consisted of 296 end-of-life care professionals who answered the survey, including nurses, physicians, psychologists, social workers, etc. Specifically for this study, the subsample of 129 nurses was selected. Following Wolf, Harrington, Clark and Miller’s [30] work, one-factor, six-indicator model with loadings of 0.50, 0.65, and 0.80 required sample sizes of 90, 60, and 40, respectively [30]. According to this work, sample size was sufficient to detect medium factor loadings.
2.3. Variables
Sociodemographic variables included age, sex, and place of work. Other variables measured were:
- Workload, measured with the item “I have too much workload”, ranging from 0 (never) to 3 (almost always).
- Work control, measured with the item “I have control over my workload”, ranging from 0 (never) to 3 (almost always).
- Burnout, measured with the Maslach Burnout Inventory—Human Services Survey (MBI) [31]. This is a 22-item questionnaire that relates to three constructs of burnout: emotional exhaustion (9 items), depersonalization (5 items), and personal accomplishment (8 items). Each item rated on a seven-point Likert-type scale for how frequently they experience the feeling, from 0 (never) to 6 (every day).
- Work satisfaction, measured with the General Work Satisfaction Scale from the Michigan Organizational Assessment Scale [32]. The scale is composed by three items. Each item rated on a five-point Likert-type scale, from 1 (completely disagree) to 5 (completely agree).
2.4. Analyses
First of all, descriptive statistics were calculated for the items of the scale, including means and standard deviations. Additionally, means and standard deviations of the total score in the Brief Nursing Stress Scale, burnout dimensions, and work satisfaction were also calculated.
Second, and in order to study the factorial structure of the BNSS, a one-factor confirmatory factor analysis (CFA) model was hypothesized, estimated, and tested. Model fit was assessed using the following statistic and fit indexes: the chi-square, the Comparative Fit Index (CFI), the Root Mean Squared Error of Approximation (RMSEA) and the Standardized Root Mean Squared Residuals (SRMR) index. Adequate fit is generally assumed with CFI > 0.90 together with a RMSEA/SRMR < 0.08, while values of CFI/TLI > 0.95 and RMSEA/SRMR < 0.05 indicate excellent fit [33]. The method of estimation for the CFA was Weighted Least Squares Mean and Variance corrected (WLSMV), given the ordinal nature of the data [34].
Reliability was estimated using the Composite Reliability Index.
t tests for independent samples were used to study differences between women and men, and between home and hospital workers. Nursing stress relation with age, workload, and work control was studied using Pearson correlations.
Finally, the predictive power of nursing stress, as measured with the BNSS, over burnout and work satisfaction was assessed using a full structural equation model. Specifically, nursing stress was hypothesized to predict burnout, which in turn predicted work satisfaction. The three constructs, nursing stress, burnout, and work satisfaction, were modeled as latent factors, and consequently, free of error of measurement. In order to assess model fit, the fit criteria mentioned above were used.
2.5. Ethical Considerations
The study was approved by the Ethics Research Committee at the University of the Balearic Islands (82CER18). Given the characteristics of the study, the people who decided to participate voluntarily were told the reason and purpose for carrying out the work. This entire study complied with the ethical principles for research in health sciences established at the national and international levels in the Declaration of Helsinki [37]. Special attention was paid to confidentiality and protection of privacy, guaranteeing the anonymity of the information provided, which was used exclusively for this work and was held in the custody of the research team. In addition, our research team is committed to strictly complying with the Organic Spanish Law on Personal Data Protection, which guarantees that the participants in this study can exercise their rights of access, rectification, cancellation, and opposition to the collected data.
3. Results
3.1. Participants Description
Mean age was 43.5 years old (SD = 10.63); 84.5% (n = 109) were women. 44.2% (n = 57) were hospital workers, 39.5% were home care workers, and 16.3% (n = 21) worked in other facilities, such as elderly institutions or hospices.
3.2. Descriptive Statistics
BNSS items showed medium levels in the six domains of nursing stress, with means ranging from 1.96 (item 3, stressful situations derived from lack of support) to 2.74 (item 5, stressful situations derived from workload) (see Table 2). The total score of the scale was 2.36.
Regarding the rest of the variables, levels of workload were high, work control was medium, emotional exhaustion was moderate, depersonalization was low, and personal acceptance and work satisfaction were high.
3.3. Internal Structre and Reliability
The CFA showed an adequate fit, except for the RMSEA: χ2(9) = 20.241 (p = 0.017); CFI = 0.924; SRMR = 0.062; RMSEA = 0.098 [0.040,0.156]. Based on Kenny et al.’s results [38], the overall fit was considered good. Factor loadings were adequate, ranging from 0.338 (item 2) to 0.710 (item 4). Details can be consulted in Table 2.
Reliability of the BNSS was adequate, with CRI = 0.712.
3.4. Relations between Nursing Stress, Sex, Age, Working Place, Workload, and Work Control
The t test for independence samples showed no statistically significant differences in nursing stress between women and men: t(127) = 1.027; p = 0.307. The correlation between nursing stress and age showed a negative, statistically significant relation (r = −0.181; p = 0.044), although of small value. Regarding the study of the relationship between nursing stress and working place, the t test was statistically significant: t(106) = −2.683; p = 0.008. Hospital nurses showed higher levels of stress (M = 2.47; SD = 0.44) compared to homecare nurses (M = 2.26; SD = 0.35).
3.5. Prediction of Burnout and Work Satisfaction
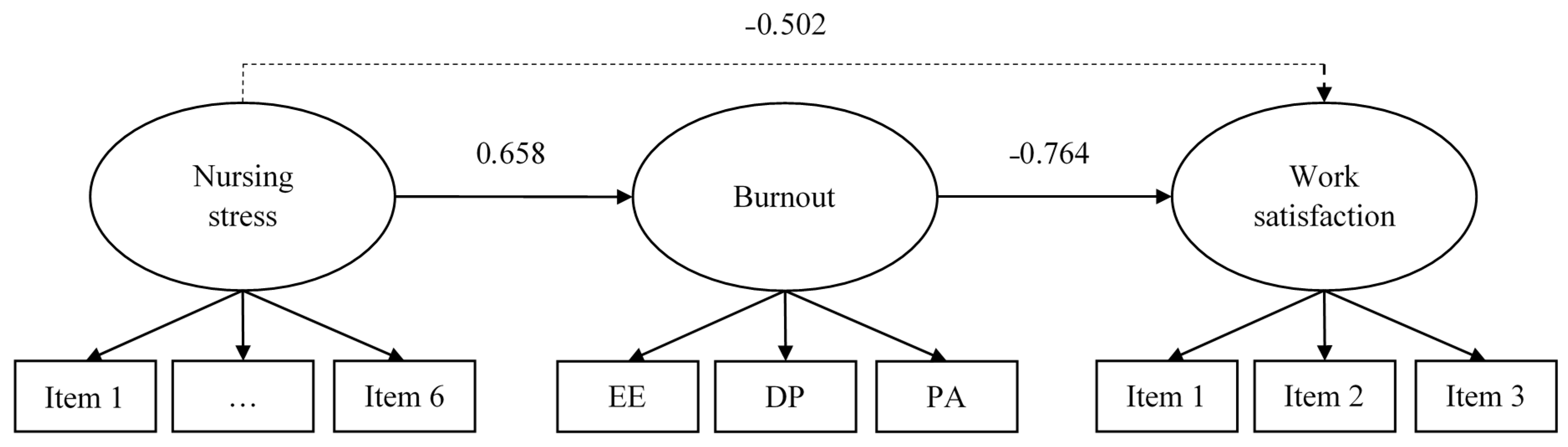
Nursing stress was related to burnout and work satisfaction. Specifically, we hypothesized, estimated, and tested a structural equation model, in which nursing stress directly predicted burnout and indirectly predicted work satisfaction, an effect mediated by burnout.
The model showed an adequate fit: χ2(52) = 93.854 (p < 0.001); CFI = 0.925; SRMR = 0.084; RMSEA = 0.079 [0.053,0.104]. As regards the analytical fit, and as can be seen in Figure 1, nursing stress positively predicted burnout, which in turn negatively predicted work satisfaction. Nursing stress also had an indirect, negative effect on work satisfaction. Overall, more than 40% of burnout variance was explained (R2 = 0.432; p < 0.001), and almost 60% of work satisfaction (R2 = 0.584; p < 0.001).
4. Discussion
The aim of the study was to develop and test the psychometric properties of the Brief Nursing Stress Scale, a short measure of nursing stress, in a sample of end-of-life care nurses. The scale, composed by six items that represented the six original dimensions of the Nursing Stress Scale [25], presented adequate evidence of reliability and validity.
The results of this study are similar with a previous study that showed a high level of occupational stress among cancer care nurses [39]. Although Kim & Kim [39] used a different scale to measure stress, they found that the dimension related to excessive workload was the most affected, as was in the present study. To be aware of such stress levels is of great importance due to the well-known association of stress with reduced work performance, higher job turnover, decreased job satisfaction, loss of productivity, high rates of absenteeism, and reduced quality of nursing care for patients [40,41,42,43].
In addition, our results pointed estimates of adequate internal validity, supporting the appropriateness of the one-factor structure of the BNSS scale. Its six items were loaded into a single dimension of nursing stress. Reliability was also adequate.
Regarding age, the results of this study sample show a negative statistically significant relation between nursing stress and age, confirming previous studies [44]. Nevertheless, the results obtained in the current study do not fully coincide with previous research, where the greatest stress was found among those aged 40 or over, followed by those in the age group of 25 to 39 years and under 25 years [39]. Additionally, no gender differences were found. In the literature, results on the relation between age and gender are not clear. Whereas there are some studies which found a positive association between female gender and stress [45,46,47,48], some others found that male nurses are at greater risk [49,50]. Talking about the association of stress with the working place, the great stress found among hospital nurses over homecare nurses is not coincident with previous research, such as Martens, where no differences were found among different work places [51].
Finally, we tested a structural equation model in which nursing stress explained both burnout syndrome and job satisfaction. Nursing stress, as measured with the BNSS, showed evidence of test-criterion validity, being a strong, direct predictor of burnout syndrome, and indirectly related to job satisfaction. This is in line with previous research, which had already pointed how nursing stress can produce high levels of burnout [18,52,53,54], and low levels of job satisfaction [54,55].
Limitations of the study are mainly referred to the sample size. Furthermore, some shortcomings include the lack of test-retest reliability, due to the study cross-sectional nature. Other limitation is the absence of information regarding the public or private ownership of the centers, or the cities in which professionals worked. These limitations could be addressed in future works in which the BNSS could be used in bigger samples, longitudinal studies, or other cultural contexts. Among its strengths is its briefness. This scale could be used as a quick, screening tool to detect stressful situations in the working environment.
5. Conclusions
All in all, evidence gathered in this study has shown adequate estimates of validity, reliability, and predictive power of the Brief Nursing Stress Scale in a sample of end-of-life care nurses. Based on the well-known and widely recognized model of Nursing Stress Scale, the BNSS is a short, easy-to-use measure that could be employed in major batteries assessing quality of healthcare institutions, with adequate prediction capacity of problems of burnout and job satisfaction.
Author Contributions
Conceptualization, N.S. and L.G.; methodology, L.G.; software, L.G.; validation, N.S., G.V.-B., and L.G.; formal analysis, L.G.; investigation, N.S.; resources, N.S. and L.G.; data curation, L.G.; writing—original draft preparation, N.S., G.V.-B., and L.G.; writing—review and editing N.S., G.V.-B., and L.G.; supervision, N.S. and L.G.; project administration, N.S. and L.G.; funding acquisition, N.S. and L.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by FEDER/Ministerio de Ciencia e Innovación—Agencia Estatal de Investigación, Spain/Project Longitudinal study of compassion and other professional quality of life determinants: A national level research on palliative care professionals (CompPal) [Estudio longitudinal de la compasión y otros determinantes de la calidad de vida profesional: Una investigación en profesionales de cuidados paliativos a nivel nacional (CompPal)] (RTI2018-094089-I00).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Research Committee at the University of the Balearic Islands (protocol code 82CER18 approved on 9 October 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank all of the participants and palliative care professional associations’ representatives in Spain for their valuable support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hingley, P. The Humane Face of Nursing. Nurs. Mirror 1984, 159, 19–22. [Google Scholar] [PubMed]
- Cañadas-De la Fuente, G.A.; Vargas, C.; San Luis, C.; García, I.; Cañadas, G.R.; De la Fuente, E.I. Risk factors and prevalence of burnout syndrome in the nursing profession. Int. J. Nurs. Stud. 2015, 52, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress. Anxiety 2009, 26, 1118–1126. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, M.E.; de Bengoa Vallejo, R.B.; Fuentes, P.S. The relationship between experiential avoidance and burnout syndrome in critical care nurses: A cross-sectional questionnaire survey. Int. J. Nurs. Stud. 2010, 47, 30–37. [Google Scholar] [CrossRef]
- Fornés-Vives, J.; García-Banda, G.; Frias-Navarro, D.; Pascual-Soler, M. Longitudinal study predicting burnout in Spanish nurses: The role of neuroticism and emotional coping. Pers. Individ. Differ. 2019, 138, 286–291. [Google Scholar] [CrossRef]
- Keidel, G.C. Burnout and compassion fatigue among hospice caregivers. Am. J. Hosp. Palliat. Care 2002, 19, 200–205. [Google Scholar] [CrossRef]
- Flanagan, N.A.; Flanagan, T.J. An analysis of the relationship between job satisfaction and job stress in correctional nurses. Res. Nurs. Health 2002, 25, 282–294. [Google Scholar] [CrossRef]
- Sarafis, P.; Rousaki, E.; Tsounis, A.; Malliarou, M.; Lahana, L.; Bamidis, P.; Niakas, D.; Papastavrou, E. The impact of occupational stress on nurses’ caring behaviors and their health related quality of life. BMC Nurs. 2016, 15, 56. [Google Scholar] [CrossRef] [Green Version]
- Teng, C.-I.; Hsiao, F.-J.; Chou, T.-A. Nurse-perceived time pressure and patient-perceived care quality. J. Nurs. Manag. 2010, 18, 275–284. [Google Scholar] [CrossRef]
- Iglesias, M.E.L.; de Bengoa Vallejo, R.B. Prevalence and relationship between burnout, job satisfaction, stress, and clinical manifestations in Spanish critical care nurses. Dimens. Crit. Care Nurs. 2013, 32, 130–137. [Google Scholar] [CrossRef]
- Levi, L. Occupational stress: Spice of life or kiss of death? Am. Psychol. 1990, 45, 1142–1145. [Google Scholar] [CrossRef]
- Olkinuora, M.A.; Lrappänen, R.A. Psychological stress experienced by health care personnel. Scand. J. Work Environ. Health 1987, 13, 1–8. [Google Scholar]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A. Occupational stress in nursing: A review of the literature. J. Nurs. Manag. 2001, 9, 101–106. [Google Scholar] [CrossRef] [PubMed]
- McGrath, A.; Reid, N.; Boore, J. Occupational stress in nursing. Int. J. Nurs. Stud. 2003, 40, 555–565. [Google Scholar] [CrossRef]
- McHugh, M.D.; Kutney-Lee, A.; Cimiotti, J.P.; Sloane, D.M.; Aiken, L.H. Nurses’ Widespread Job Dissatisfaction, Burnout, And Frustration With Health Benefits Signal Problems For Patient Care. Health Aff. 2011, 30, 202–210. [Google Scholar] [CrossRef]
- Van Bogaert, P.; Clarke, S.; Willems, R.; Mondelaers, M. Nurse practice environment, workload, burnout, job outcomes, and quality of care in psychiatric hospitals: A structural equation model approach. J. Adv. Nurs. 2013, 69, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Van Bogaert, P.; Meulemans, H.; Clarke, S.; Vermeyen, K.; Van De Heyning, P. Hospital nurse practice environment, burnout, job outcomes and quality of care: Test of a structural equation model. J. Adv. Nurs. 2009, 65, 2175–2185. [Google Scholar] [CrossRef] [PubMed]
- Benbunan-Bentata, B.; Cruz-Quintana, F.; Roa-Venegas, J.M.; Villaverde-Gutiérrez, C.; Benbunan-Bentata, B.R. Nursing Students’ Coping with Pain and Death: A Proposal for Ameliorative Action. Int. J. Clin. Health Psychol. 2007, 7, 197–205. [Google Scholar]
- Stone, P.; Thorns, A. Ethics and Palliative Care: A Case-Based Manual; Radcliffe Publishing: Oxford, UK, 2005. [Google Scholar]
- Maslach, C. Burnout: The Cost of Caring; Malor Books: Cambridge, MA, USA, 2003. [Google Scholar]
- Pavelková, H.; Bužgová, R. Burnout among healthcare workers in hospice care. Central Eur. J. Nurs. Midwifery 2015, 6, 218–223. [Google Scholar] [CrossRef] [Green Version]
- French, S.E.; Lenton, R.; Walters, V.; Eyles, J. An Empirical Evaluation of an Expanded Nursing Stress Scale. J. Nurs. Meas. 2000, 8, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.H.; Badiani, A.; Miczek, K.A.; Müller, C.P. Non-pharmacological factors that determine drug use and addiction. Neurosci. Biobehav. Rev. 2020, 110, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Gray-Toft, P.; Anderson, J.G. The Nursing Stress Scale: Development of an instrument. J. Behav. Assess. 1981, 3, 11–23. [Google Scholar] [CrossRef]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1966. [Google Scholar]
- Appley, M.H.; Trumbull, R. Psychological Stress, Issues in Research; Appleton-Century-Crofts: New York, NY, USA, 1967. [Google Scholar]
- Escribà, V.; Más, R.; Cárdenas, M.; Pérez, S. Validación de la escala de estresores laborales en personal de enfermería: «The Nursing Stress Scale». Gac. Sanit. 1999, 13, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Wolf, E.J.; Harrington, K.M.; Clark, S.L.; Miller, M.W. Sample Size Requirements for Structural Equation Models: An Evaluation of Power, Bias, and Solution Propriety. Educ. Psychol. Meas. 2013, 73, 913–934. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M.P.; Schaufeli, W.B.; Schwab, R.L. Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Seashore, S.E.; Lawler, E.E., III; Mirvis, P.H.; Cammann, C. (Eds.) Assessing Organizational Change. A Guide to Methods, Measures, and Practices; Wiley: New York, NY, USA, 1983. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2015; ISBN 978-1-60623-876-9. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0.; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Muthén, L.K.; Muthén, B. (Eds.) Mplus. The Comprehensive Modelling Program for Applied Researchers: User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The Performance of RMSEA in Models with Small Degrees of Freedom. Sociol. Methods Res. 2014, 44, 486–507. [Google Scholar] [CrossRef]
- Kim, H.; Kim, K. Palliative Cancer Care Stress and Coping Among Clinical Nurses Who Experience End-of-Life Care. J. Hosp. Palliat. Nurs. 2020, 22, 115–122. [Google Scholar] [CrossRef] [PubMed]
- McKinney, B.K. Withstanding the Pressure of the Profession. J. Nurses Staff Dev. 2011, 27, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Mojoyinola, J. Effects of Job Stress on Health, Personal and Work Behaviour of Nurses in Public Hospitals in Ibadan Metropolis, Nigeria. Stud. Ethno-Med. 2008, 2, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Nabirye, R.C.; Brown, K.C.; Pryor, E.R.; Maples, E.H. Occupational stress, job satisfaction and job performance among hospital nurses in Kampala, Uganda. J. Nurs. Manag. 2011, 19, 760–768. [Google Scholar] [CrossRef]
- Wazqar, D.Y.; Kerr, M.; Regan, S.; Orchard, C. Overview of Cancer Care and Oncology Nursing in the Kingdom of Saudi Arabia. Am. J. Nurs. Sci. 2017, 6, 324. [Google Scholar] [CrossRef]
- Xie, Z.; Wang, A.; Chen, B. Nurse burnout and its association with occupational stress in a cross-sectional study in Shanghai. J. Adv. Nurs. 2011, 67, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Raeissi, P.; Raoofi, S.; Soltani, A.; Sokhanvar, M.; Visentin, D.; Cleary, M. Occupational stress and associated risk factors among nurses: A cross-sectional study. Contemp. Nurse 2019, 55, 237–249. [Google Scholar] [CrossRef]
- Kwiatosz-Muc, M.; Fijałkowska-Nestorowicz, A.; Fijałkowska, M.; Aftyka, A.; Kowalczyk, M. Stress prevalence and stressors among anaesthesiology and intensive care unit workers: A multicentre survey study. Aust. Crit. Care 2018, 31, 391–395. [Google Scholar] [CrossRef]
- Jaracz, M.; Rosiak, I.; Bertrand-Bucińska, A.; Jaskulski, M.; Nieżurawska, J.; Borkowska, A. Affective temperament, job stress and professional burnout in nurses and civil servants. PLoS ONE 2017, 12, e0176698. [Google Scholar] [CrossRef] [Green Version]
- Stecker, M.; Stecker, M.M. Disruptive Staff Interactions: A Serious Source of Inter-Provider Conflict and Stress in Health Care Settings. Issues Ment. Health Nurs. 2014, 35, 533–541. [Google Scholar] [CrossRef]
- Al-Kandari, F.; Thomas, D. Adverse nurse outcomes: Correlation to nurses’ workload, staffing, and shift rotation in Kuwaiti hospitals. Appl. Nurs. Res. 2008, 21, 139–146. [Google Scholar] [CrossRef]
- Tankha, G. A Comparative Study of Role Stress in Government and Private Hospital Nurses. J. Health Manag. 2006, 8, 11–22. [Google Scholar] [CrossRef]
- Martens, M.L. A Comparison of Stress Factors in Home and Inpatient Hospice Nurses. J. Hosp. Palliat. Nurs. 2009, 11, 144–153. [Google Scholar] [CrossRef]
- Kogoj, T.K.; Cebašek-Travnik, Z.; Zaletel-Kragelj, L. Role of Stress in Burnout among Students of Medicine and Dentistry--a Study in Ljubljana, Slovenia, Faculty of Medicine. Coll. Antropol. 2014, 38, 879–887. [Google Scholar] [PubMed]
- Munnangi, S.; Dupiton, L.; Boutin, A.; Angus, L.D.G. Burnout, Perceived Stress, and Job Satisfaction among Trauma Nurses at a Level I Safety-Net Trauma Center. J. Trauma Nurs. 2018, 25, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work Related Stress, Burnout, Job Satisfaction and General Health of Nurses. Int. J. Environ. Res. Public Health 2015, 12, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhao, Y.; While, A. Job satisfaction among hospital nurses: A literature review. Int. J. Nurs. Stud. 2019, 94, 21–31. [Google Scholar] [CrossRef]
Figure 1.
Structural equation modeling predicting burnout and work satisfaction. Notes: EE = Emotional exhaustion; DP = Depersonalization; PA = Personal acceptance. All the factor loadings, direct effects and the indirect effect were statistically significant (p < 0.001). Script line represents the indirect effect.
Figure 1.
Structural equation modeling predicting burnout and work satisfaction. Notes: EE = Emotional exhaustion; DP = Depersonalization; PA = Personal acceptance. All the factor loadings, direct effects and the indirect effect were statistically significant (p < 0.001). Script line represents the indirect effect.


{kind=link}
Table 1.
The Brief Nursing Stress Scale (BNSS).
| Item Number | Item Content Please Indicate How Frequently You Suffer… |
|---|---|
| 1 | stressful situations derived from the process of dying or death |
| 2 | stressful situations derived from conflicts with doctors |
| 3 | stressful situations derived from lack of support |
| 4 | stressful situations derived from conflict between nurses |
| 5 | stressful situations derived from workload |
| 6 | stressful situations derived from the uncertainty of the treatment |
Table 2.
Descriptive statistics for the Brief Nursing Stress Scale (BNSS) items, total score, indicators of workload and work control, dimensions of burnout, and work satisfaction.
Table 2.
Descriptive statistics for the Brief Nursing Stress Scale (BNSS) items, total score, indicators of workload and work control, dimensions of burnout, and work satisfaction.
| Variable | Mean | SD 1 | Minimum | Maximum | λ |
|---|---|---|---|---|---|
| Item 1 | 2.60 | 0.65 | 1.00 | 4.00 | 0.347 |
| Item 2 | 2.35 | 0.67 | 1.00 | 4.00 | 0.338 |
| Item 3 | 1.96 | 0.61 | 1.00 | 4.00 | 0.664 |
| Item 4 | 2.35 | 0.67 | 1.00 | 4.00 | 0.710 |
| Item 5 | 2.74 | 0.75 | 1.00 | 4.00 | 0.478 |
| Item 6 | 2.16 | 0.67 | 1.00 | 4.00 | 0.666 |
| Nursing stress | 2.36 | 0.40 | 1.33 | 3.67 | --- |
| Workload | 2.91 | 0.78 | 1.00 | 4.00 | --- |
| Work control | 2.44 | 1.03 | 1.00 | 4.00 | --- |
| Emotional exhaustion | 17.53 | 8.68 | 2.00 | 45.00 | --- |
| Depersonalization | 4.55 | 3.67 | 0.00 | 19.00 | --- |
| Personal acceptance | 33.30 | 6.22 | 14.00 | 48.00 | --- |
| Work satisfaction | 4.36 | 0.75 | 1.67 | 5.00 | --- |
1 Standard deviation.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sansó, N.; Vidal-Blanco, G.; Galiana, L. Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses. Nurs. Rep. 2021, 11, 311-319. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020030
AMA Style
Sansó N, Vidal-Blanco G, Galiana L. Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses. Nursing Reports. 2021; 11(2):311-319. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020030
Chicago/Turabian StyleSansó, Noemí, Gabriel Vidal-Blanco, and Laura Galiana. 2021. "Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses" Nursing Reports 11, no. 2: 311-319. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020030