
The Effects of the Civility, Respect, and Engagement in the Workplace (CREW) Program on Social Climate and Work Engagement in a Psychiatric Ward in Japan: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
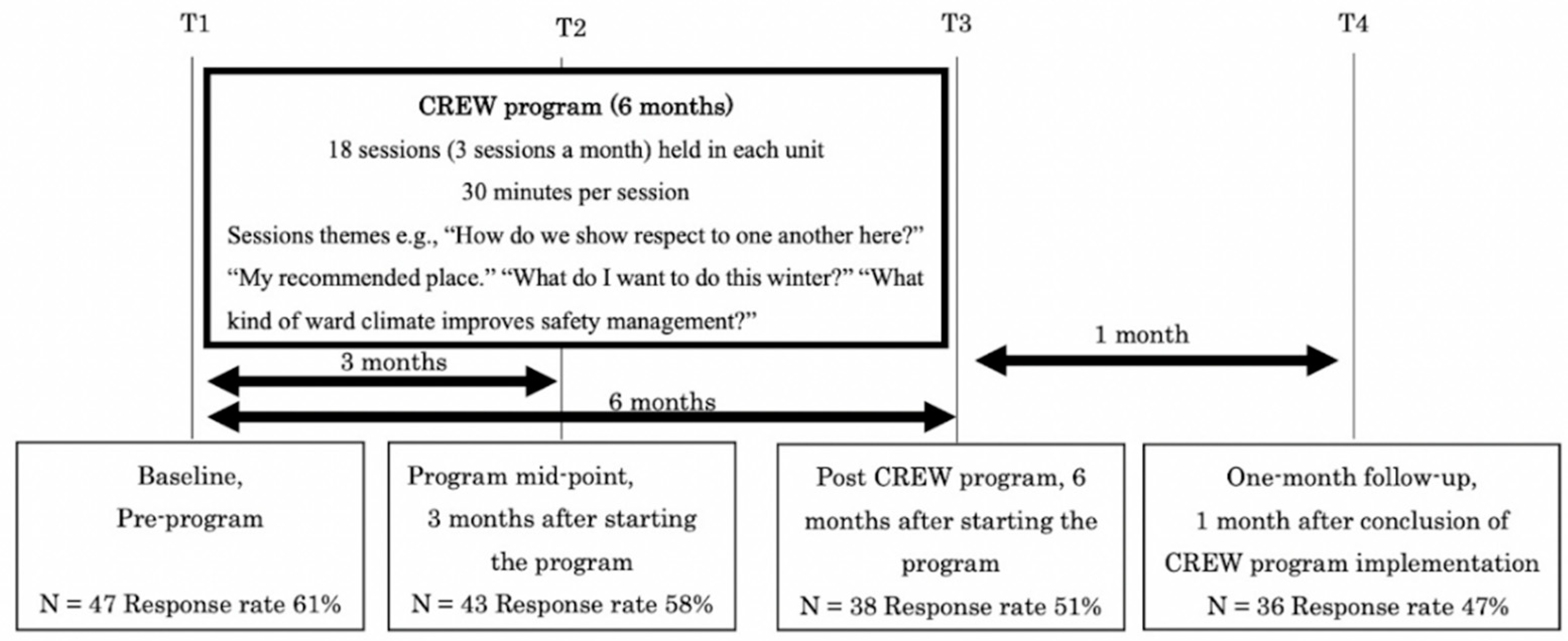
2.1. The CREW Program Process
2.2. Survey Procedure
2.3. Outcome Measurement and Assessment
2.3.1. Social Climate
EssenCES
CREW Civility Scale (Civility)
2.3.2. Work Engagement
Utrecht Work Engagement Scale (UWES)
2.3.3. Demographic Characteristics and Freeform Comments
2.4. Statistical Analysis
2.5. Ethics
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nieuwenhuijsen, K.; Bruinvels, D.; Frings-Dresen, M. Psychosocial work environment and stress-related disorders, a systematic review. Occup. Med. 2010, 60, 277–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef]
- Fløvik, L.; Knardahl, S.; Christensen, J.O. The Effect of Organizational Changes on the Psychosocial Work Environment: Changes in Psychological and Social Working Conditions Following Organizational Changes. Front. Psychol. 2019, 10, 2845. [Google Scholar] [CrossRef]
- Way, M.; MacNeil, M. Organizational characteristics and their effect on health. Nurs. Econ. 2006, 24, 67–76. [Google Scholar]
- Jansson von Vultée, P.; Axelsson, R.; Arnetz, B. The impact of organisational settings on physician wellbeing. Int. J. Health Care Qual. Assur. 2007, 20, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Iwu, C.G.; Allen-lle, C.; Ukpere, W.I. A model of employee satisfaction amongst health-related professionals in South Africa: The case of Western Cape Province. Afr. J. Bus. Manag. 2012, 6, 9658–9670. [Google Scholar]
- Ancarani, A.; Mauro, C.D.; Giammanco, M.D. Linking organizational climate to work engagement: A study in the healthcare sector. Int. J. Public Adm. 2019, 42, 547–557. [Google Scholar] [CrossRef]
- Laschinger, H.K.S.; Leiter, M.P. The impact of nursing work environments on patient safety outcomes: The mediating role of burnout engagement. JONA J. Nurs. Adm. 2006, 36, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Lautizi, M.; Laschinger, H.K.; Ravazzolo, S. Workplace empowerment, job satisfaction and job stress among Italian mental health nurses: An exploratory study. J. Nurs. Manag. 2009, 17, 446–452. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Salanova, M.; González-Romá, V.; Bakker, A.B. The measurement of burnout and engagement: A confirmative analytic approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire: A cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Schaufeli, W.B. Do burnout and work engagement predict depressive symptoms and life satisfaction? A three-wave seven-year prospective study. J. Affect. Disord. 2012, 141, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, L.; Grawitch, M.J.; Munz, D.C. Are better sleepers more engaged workers? A self-regulatory approach to sleep hygiene and work engagement. Stress Health 2013, 29, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, H.; Shimazu, A.; Kawakami, N.; Inoue, A.; Nakata, A.; Tsutsumi, A. Work engagement and high-sensitivity C-reactive protein levels among Japanese workers: A 1-year prospective cohort study. Int. Arch. Occup. Environ. Health 2015, 88, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Middelboe, T.; Schjødt, T.; Byrsting, K.; Gjerris, A. Ward atmosphere in acute psychiatric in-patient care: Patients’ perceptions, ideals and satisfaction. Acta Psychiatr. Scand. 2001, 103, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, B.A.; Gill, K.J.; Fitzgerald, E.; Sclafani, M.; Grandison, P. The association of ward atmosphere with burnout and attitudes of treatment team members in a state psychiatric hospital. Am. J. Psychiatr. Rehabil. 2006, 9, 111–129. [Google Scholar] [CrossRef]
- Røssberg, J.I.; Friis, S. A suggested revision of the Ward Atmosphere Scale. Acta Psychiatr. Scand. 2003, 108, 374–380. [Google Scholar] [CrossRef]
- Moos, R.; Shelton, R.; Petty, C. Perceived ward climate and treatment outcome. J. Abnorm. Psychol. 1973, 82, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Jörgensen, K.N.; Römma, V.; Rundmo, T. Associations between ward atmosphere, patient satisfaction and outcome. J. Psychiatr. Mental Health Nurs. 2009, 16, 113–120. [Google Scholar] [CrossRef]
- Tuvesson, H.; Wann-Hansson, C.; Eklund, M. The ward atmosphere important for the psychosocial work environment of nursing staff in psychiatric in-patient care. BMC Nurs. 2011, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Magnavita, N. Violence prevention in a small-scale psychiatric unit: Program planning and evaluation. Int. J. Occup. Environ. Health 2011, 17, 336–344. [Google Scholar] [CrossRef]
- Osatuke, K.; Moore, S.C.; Ward, C.; Dyrenforth, S.R.; Belton, L. Civility, respect, engagement in the workforce (CREW) nationwide organization development intervention at Veterans Health Administration. J. Appl. Behav. Sci. 2009, 45, 384–410. [Google Scholar] [CrossRef]
- Leiter, M.P.; Laschinger HK, S.; Day, A.; Oore, D.G. The impact of civility interventions on employee social behavior, distress, and attitudes. J. Appl. Psychol. 2011, 96, 1258–1274. [Google Scholar] [CrossRef]
- Osatuke, K.; Leiter, M.; Belton, L.; Dyrenforth, S.; Ramsel, D. Civility, Respect and Engagement at the Workplace (CREW): A national organization development program at the Department of Veterans Affairs. J. Manag. Policies Pract. 2013, 1, 25–34. [Google Scholar]
- Leiter, M.P.; Day, A.; Oore, D.G.; Spence Laschinger, H.K. Getting better and staying better: Assessing civility, incivility, distress, and job attitudes one year after a civility intervention. J. Occup. Health Psychol. 2012, 17, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Gilin Oore, D.E.B.R.A.; Leblanc, D.; Day, A.; Leiter, M.P.; Spence Laschinger, H.K.; Price, S.L.; Latimer, M. When respect dete-riorates: Incivility as a moderator of the stressor–strain relationship among hospital workers. J. Nurs. Manag. 2010, 18, 878–888. [Google Scholar] [CrossRef]
- Rabøl, L.I.; McPhail, M.A.; Østergaard, D.; Andersen, H.B.; Mogensen, T. Promoters and barriers in hospital team communication. A focus group study. J. Commun. Healthc. 2012, 5, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Fewster-Thuente, L.; Velsor-Friedrich, B. Interdisciplinary collaboration for healthcare professionals. Nurs. Adm. Q. 2008, 32, 40–48. [Google Scholar] [CrossRef]
- Tschannen, D.; Schoville, R.; Schmidt, P.; Buehler, K.; Borst, S.; Flaherty-Robb, M. Communication practices among nurses in the acute care setting. J. Commun. Healthc. 2013, 6, 171–179. [Google Scholar] [CrossRef]
- Hossny, E.K.; Sabra, H.E. Effect of nurses’ perception to workplace civility climate on nurse–physician collaboration. Nurs. Open 2021, 8, 620–627. [Google Scholar] [CrossRef]
- Pearson, C.M.; Andersson, L.M.; Porath, C.L. Assessing and attacking workplace incivility. Organ. Dyn. 2000, 29, 123–137. [Google Scholar] [CrossRef]
- Clark, C.M. Pursuing a culture of civility: An intervention study in one program of nursing. Nurse Educ. 2011, 36, 98–102. [Google Scholar] [CrossRef]
- Clark, C.M.; Kenaley, B.L.D. Faculty empowerment of students to foster civility in nursing education: A merging of two conceptual models. Nurs. Outlook 2011, 59, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L.M.; Pearson, C.M. Tit for tat? The spiraling effect of incivility in the workplace. Acad. Manag. Rev. 1999, 24, 452–471. [Google Scholar] [CrossRef] [Green Version]
- King, E.B.; Dawson, J.F.; West, M.A.; Gilrane, V.L.; Peddie, C.I.; Bastin, L. Why organizational and community diversity matter: Representativeness and the emergence of incivility and organizational performance. Acad. Manag. J. 2011, 54, 1103–1118. [Google Scholar] [CrossRef] [Green Version]
- Oppel, E.M.; Mohr, D.C.; Benzer, J.K. Let’s be civil: Elaborating the link between civility climate and hospital performance. Health Care Manag. Rev. 2019, 44, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.M.; Kenski, D. Promoting civility in the OR: An ethical imperative. Aorn J. 2017, 105, 60–66. [Google Scholar] [CrossRef]
- Merkel, R.; Olsen, J.; Pehler, S.R.; Sperstad, R.; Sisto, H.; Brunsell, K.; Mades, H. An Innovative Civility Intervention Created by a Faculty and Student Action Research Team. J. Nurs. Educ. 2020, 59, 214–217. [Google Scholar] [CrossRef]
- McAdams-Jones, D. Using cognitive rehearsal to build a culture of civility. J. Contin. Educ. Nurs. 2020, 51, 253–255. [Google Scholar] [CrossRef]
- Noda, T.; Sato, M.; Sugiyama, N.; Yoshihama, F.; Ito, H. Kanja oyobi kangoshi ga hyoukasuru seishinkabyoutou no fuudo: Essen seishinka byoutou fuudo hyouka schema nihongoban wo mochiita kentou (Assessment of Ward Climate by Patients and Nurses in Psychiatric Hospital using the Essen Climate Evaluation schema). Seishin Igaku 2014, 56, 715–722. [Google Scholar]
- Schalast, N.; Redies, M.; Collins, M.; Stacey, J.; Howells, K. EssenCES, a short questionnaire for assessing the social climate of forensic psychiatric wards. Crim. Behav. Mental Health 2008, 18, 49–58. [Google Scholar] [CrossRef]
- Noda, T.; Sugiyama, N.; Matsumoto, K. Psychometric Properties of the Japanese Version of the Essen Climate Evaluation Schema (Essen CES). Seishin Igaku 2012, 54, 211–217. [Google Scholar]
- Tsuno, K.; Kawakami, N.; Shimazu, A.; Shimada, K.; Inoue, A.; Leiter, M.P. Workplace incivility in Japan: Reliability and validity of the Japanese version of the modified Work Incivility Scale. J. Occup. Health 2017, 59, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Shimazu, A.; Schaufeli, W.B.; Kosugi, S.; Suzuki, A.; Nashiwa, H.; Kato, A.; Sakamoto, M.; Irimajiri, H.; Amano, S.; Hirohata, K.; et al. Work engagement in Japan: Validation of the Japanese version of the Utrecht Work Engagement Scale. Appl. Psychol. 2008, 57, 510–523. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Donders, A.R.T.; Van Der Heijden, G.J.; Stijnen, T.; Moons, K.G. A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef]
- Kagata, S.; Inoue, A.; Kubota, K.; Shimazu, A. Association of Emotional Labor with Work Engagement and Stress Responses among Hospital Ward Nurses. Jpn. J. Behav. Med. 2015, 21, 83–90. [Google Scholar]


{kind=link}
| Baseline (T1) | Midpoint (T2) | Post (T3) | One-Month Post (T4) | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| n = 47 | n = 43 | n = 38 | n = 36 | ||||||
| n (%) | Mean (SD) | n (%) | Mean (SD) | n (%) | Mean (SD) | n (%) | Mean (SD) | ||
| Gender | 0.549 | ||||||||
| Male | 11 (23.4) | 6 (14.0) | 10 (26.3) | 7 (19.4) | |||||
| Female | 35 (74.5) | 37 (86.0) | 28 (73.7) | 26 (72.2) | |||||
| Not provided | 1 (2.1) | - | - | 3 (8.3) | |||||
| Age | 0.901 | ||||||||
| 20–29 | 19 (40.4) | 18 (41.9) | 17 (44.7) | 15 (41.7) | |||||
| 30–39 | 14 (29.8) | 10 (23.3) | 10 (26.3) | 9 (25) | |||||
| 40–49 | 8 (17.0) | 7 (16.3) | 4 (10.5) | 7 (19.4) | |||||
| 50–59 | 3 (6.4) | 4 (9.3) | 4 (10.5) | 3 (8.3) | |||||
| Over 60 | 3 (6.4) | 3 (7.0) | 2 (5.3) | - | |||||
| Not provided | - | 1 (2.0) | 1 (2.6) | 2 (5.6) | |||||
| Job | 0.837 | ||||||||
| Nurse | 22 (46.8) | 25 (58.1) | 17 (44.7) | 19 (52.8) | |||||
| Medical doctor | 13 (27.7) | 9 (20.9) | 11 (28.9) | 9 (25.0) | |||||
| Others | 10 (21.3) | 9 (20.9) | 8 (21.1) | 6 (16.7) | |||||
| Not provided | 2 (4.3) | - | 2 (5.3) | 2 (5.6) | |||||
| Employment status | 0.446 | ||||||||
| Full-time | 38 (80.9) | 34 (79.1) | 25 (65.8) | 26 (72.2) | |||||
| Part-time | 9 (19.1) | 8 (18.6) | 12 (31.6) | 7 (19.4) | |||||
| Not provided | - | 1 (2.3) | 1 (2.6) | 3 (8.3) | |||||
| Years of experience in job | 0.796 | ||||||||
| All | 4.2 (5.1) | 8 (7.3) | 7.1 (6.5) | 7.9 (6.5) | |||||
| Nurse | 7.9 (8.1) | 8.1 (7.7) | 8.6 (8.5) | 8.2 (6.7) | |||||
| Medical doctor | 8.8 (7.5) | 7.1 (8.3) | 4.9 (5.4) | 7.9 (8.1) | |||||
| Others | 9.7 (9.0) | 8.5 (5.6) | 7.1 (2.5) | 7 (2.7) | |||||
| Baseline (T1) | Mid-Survey (T2) | Post-Survey (T3) | 1-Month Follow-Up Survey (T4) | Cohen’s d (95% CI; LL–UL) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables (Range Potential) | n | Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | F | p | T2-T1 | T3-T1 | T4-T1 | |
| EssenCES | All * | 46 | 14.0 | 2.6 | 41 | 14.3 | 2.1 | 37 | 14.9 | 2.5 | 36 | 13.8 | 2.4 | 1.65 | 0.17 | 0.13 (−0.30–0.55) | 0.35 (−0.09–0.79) | −0.08 (−0.52–0.36) |
| (0–20) | Nurse | 22 | 13.5 | 3.0 | 25 | 14.2 | 2.1 | 17 | 15.1 | 2.5 | 19 | 14.3 | 2.0 | 1.32 | 0.28 | 0.27 (−0.32–0.86) | 0.57 (−0.10–1.24) | 0.31 (−0.33–0.95) |
| Medical doctors | 13 | 13.8 | 2.2 | 9 | 13.8 | 2.6 | 11 | 15.5 | 2.3 | 9 | 13.1 | 3.4 | 1.54 | 0.22 | 0.0 (−0.90–0.90) | 0.76 (−0.12–1.64) | −0.18 (−1.09–0.72) | |
| Others | 9 | 15.1 | 1.9 | 7 | 15.1 | 1.3 | 7 | 14.7 | 2.5 | 6 | 13.7 | 2.0 | 0.80 | 0.51 | 0.0 (−1.08–1.08) | −0.18 (−1.27–0.90) | −0.73 (−1.90–0.45) | |
| Civility | All * | 46 | 3.9 | 0.5 | 39 | 3.9 | 0.4 | 36 | 3.9 | 0.5 | 34 | 3.8 | 0.4 | 0.40 | 0.76 | 0.0 (−0.43–0.43) | 0.0 (−0.44–0.44) | −0.01 (−0.46–0.44) |
| (0–5) | Nurse | 22 | 3.9 | 0.6 | 25 | 3.9 | 0.4 | 17 | 3.9 | 0.4 | 19 | 3.9 | 0.4 | 0.01 | 0.99 | 0.0 (−0.59–0.59) | 0.0 (−0.65–0.65) | −0.06 (−0.69–0.58) |
| Medical doctors | 13 | 3.8 | 0.5 | 9 | 4.1 | 0.4 | 11 | 4.2 | 0.5 | 8 | 3.7 | 0.3 | 2.35 | 0.09 | 0.63 (−0.30–1.55) | 0.79 (−0.09–1.67) | −0.18 (−1.12–0.76) | |
| Others | 9 | 4.0 | 0.5 | 5 | 3.8 | 0.5 | 6 | 3.6 | 0.4 | 5 | 3.8 | 0.5 | 0.66 | 0.59 | −0.41 (−1.63–0.82) | −0.84 (−2.03–0.34) | −0.39 (−1.61–0.84) | |
| UWES | All * | 47 | 2.9 | 1.1 | 42 | 2.8 | 0.9 | 38 | 3.0 | 1.0 | 35 | 2.6 | 1.2 | 1.11 | 0.44 | −0.10 (−0.52–0.32) | 0.09 (−0.34–0.53) | −0.25 (−0.69–0.2) |
| (0–5) | Nurse | 22 | 2.4 | 0.8 | 25 | 2.7 | 0.9 | 17 | 2.9 | 1.0 | 19 | 2.6 | 1.1 | 0.87 | 0.46 | 0.35 (−0.24–0.94) | 0.56 (−0.11–1.23) | 0.24 (−0.4–0.88) |
| Medical doctors | 13 | 3.1 | 1.0 | 9 | 3.3 | 0.9 | 11 | 3.3 | 1.3 | 9 | 2.7 | 1.4 | 0.68 | 0.57 | 0.21 (−0.70–1.12) | 0.17 (−0.68–1.03) | −0.37 (−1.28–0.54) | |
| Others | 10 | 3.5 | 1.4 | 8 | 2.8 | 1.0 | 8 | 3.2 | 0.7 | 6 | 3.1 | 0.6 | 0.60 | 0.62 | −0.71 (−1.75–0.32) | −0.34 (−1.35–0.60) | −0.48 (−1.6–0.64) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawada, U.; Shimazu, A.; Kawakami, N.; Miyamoto, Y.; Speigel, L.; Leiter, M.P. The Effects of the Civility, Respect, and Engagement in the Workplace (CREW) Program on Social Climate and Work Engagement in a Psychiatric Ward in Japan: A Pilot Study. Nurs. Rep. 2021, 11, 320-330. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020031
Sawada U, Shimazu A, Kawakami N, Miyamoto Y, Speigel L, Leiter MP. The Effects of the Civility, Respect, and Engagement in the Workplace (CREW) Program on Social Climate and Work Engagement in a Psychiatric Ward in Japan: A Pilot Study. Nursing Reports. 2021; 11(2):320-330. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020031
Chicago/Turabian StyleSawada, Utako, Akihito Shimazu, Norito Kawakami, Yuki Miyamoto, Lisa Speigel, and Michael P. Leiter. 2021. "The Effects of the Civility, Respect, and Engagement in the Workplace (CREW) Program on Social Climate and Work Engagement in a Psychiatric Ward in Japan: A Pilot Study" Nursing Reports 11, no. 2: 320-330. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020031