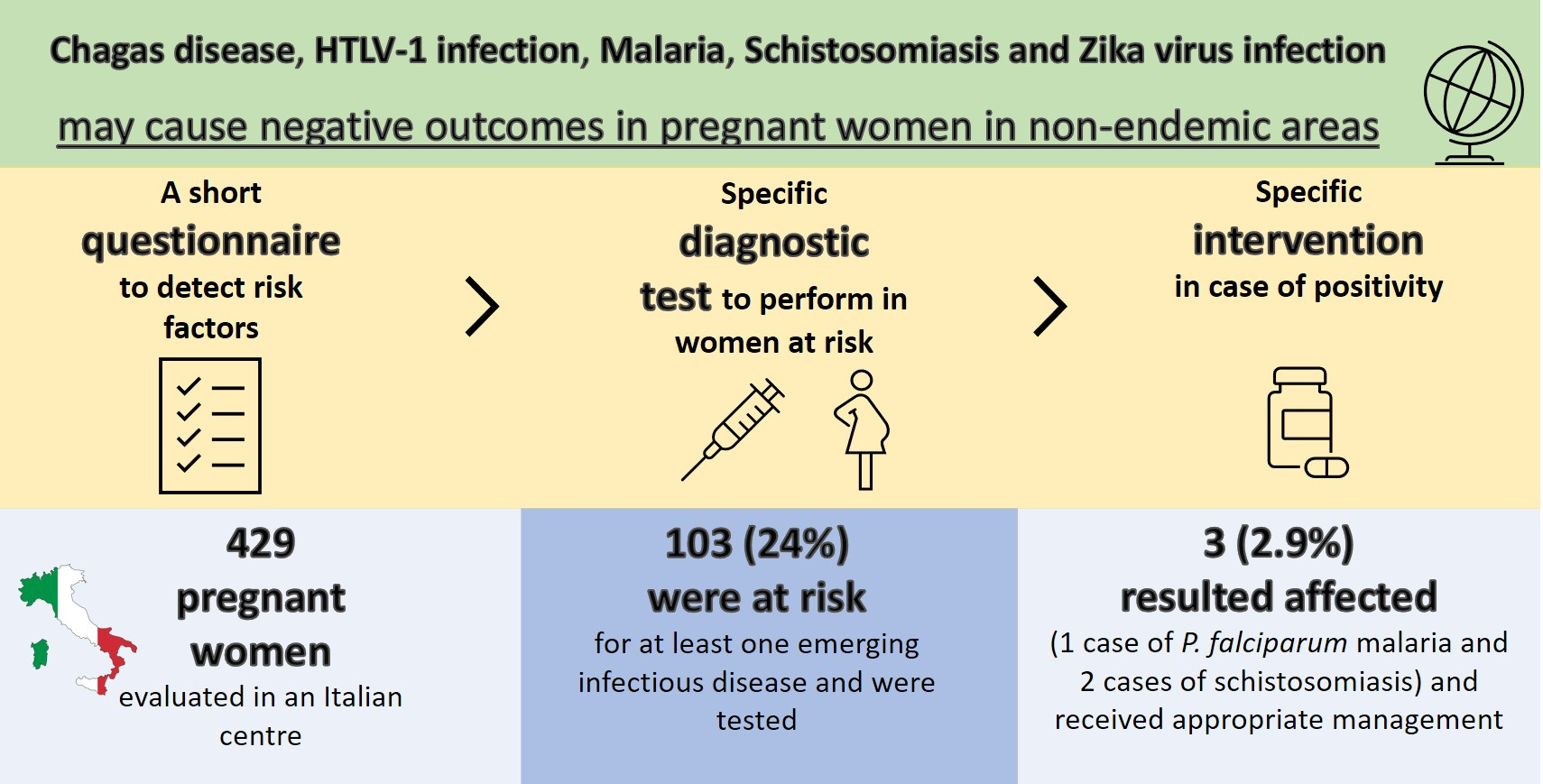
Emerging Infectious Diseases in Pregnant Women in a Non-Endemic Area: Almost One Out of Four Is at Risk

 , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bern, C. Chagas’ Disease. N. Engl. J. Med. 2015, 373, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Carlier, Y.; Altcheh, J.; Angheben, A.; Freilij, H.; Luquetti, A.O.; Schijman, A.G.; Segovia, M.; Wagner, N.; Vinas, P.A. Congenital Chagas disease: Updated recommendations for prevention, diagnosis, treatment, and follow-up of newborns and siblings, girls, women of childbearing age, and pregnant women. PLoS Negl. Trop. Dis. 2019, 13, e0007694. [Google Scholar] [CrossRef] [PubMed]
- Gallo, R.C.; Willems, L.; Hasegawa, H. Screening transplant donors for HTLV-1 and -2. Blood 2016, 128, 3029–3031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, I.; Clarke, S.E.; Gosling, R.; Hamainza, B.; Killeen, G.; Magill, A.; O’Meara, W.; Price, R.N.; Riley, E.M. “Asymptomat-ic” Malaria: A Chronic and Debilitating Infection That Should Be Treated. PLoS Med. 2016, 13, e1001942. [Google Scholar] [CrossRef] [PubMed]
- Salas-Coronas, J.; Vázquez-Villegas, J.; Lozano-Serrano, A.B.; Soriano-Pérez, M.J.; Cabeza-Barrera, I.; Cabezas-Fernández, M.T.; Villarejo-Ordóñez, A.; Sánchez-Sánchez, J.C.; Vivas-Pérez, J.I.A.; Blanc, S.V.; et al. Severe complications of imported schistosomiasis, Spain: A retrospective observational study. Travel Med. Infect. Dis. 2020, 35, 101508. [Google Scholar] [CrossRef]
- De Carvalho, N.S.; De Carvalho, B.F.; Dóris, B.; Biscaia, E.S.; Fugaça, C.A.; Noronha, L. Zika virus and pregnancy: An overview. Am. J. Reprod. Immunol. 2017, 77, e12616. [Google Scholar] [CrossRef] [Green Version]
- Requena-Mendez, A.; Albajar-Viñas, P.; Angheben, A.; Chiodini, P.; Gascón, J.; Muñoz, J.; Chagas Disease COHEMI Working Group. Health Policies to Control Chagas Disease Transmission in European Countries. PLoS Negl. Trop. Dis. 2014, 8, e3245. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Parasites—American Trypanosomiasis (also Known as Chagas Disease) Congenital Chagas Disease. Available online: https://www.cdc.gov/parasites/chagas/health_professionals/congenital_chagas.html (accessed on 8 January 2021).
- Minakami, H.; Maeda, T.; Fujii, T.; Hamada, H.; Iitsuka, Y.; Itakura, A.; Itoh, H.; Iwashita, M.; Kanagawa, T.; Kanai, M.; et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J. Obstet. Gynaecol. Res. 2014, 40, 1469–1499. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA. 2018. Available online: https://www.ecdc.europa.eu/sites/portal/files/documents/Public%20health%20guidance%20on%20screening%20and%20vaccination%20of%20migrants%20in%20the%20EU%20EEA.pdf (accessed on 8 January 2021).
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; Macdonald, N.E.; et al. Evidence-based clinical guidelines for immigrants and refugees. Can. Med. Assoc. J. 2010, 183, E824–E925. [Google Scholar] [CrossRef] [Green Version]
- Stauffer, W.M.; Cetron, M.S.; Newman, R.D.; Hamel, M.J.; Slutsker, L.; Weinberg, M.; Causer, L.M. Pre-departure and Post-arrival Management of P. falciparum Malaria in Refugees Relocating from Sub-Saharan Africa to the United States. Am. J. Trop. Med. Hyg. 2008, 79, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Oduyebo, T.; Polen, K.D.; Walke, H.T.; Reagan-Steiner, S.; Lathrop, E.; Rabe, I.B.; Kuhnert-Tallman, W.L.; Martin, S.W.; Walker, A.T.; Gregory, C.J.; et al. Update: Interim Guidance for Health Care Providers Caring for Pregnant Women with Possible Zika Virus Exposure—United States (Including U.S. Territories), July 2017. Morb. Mortal. Wkly. Rep. 2017, 66, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. 2020–2025 Italian National Arboviroses Prevention and Surveillance Plan. Available online: http://www.statoregioni.it/media/2371/p-1-csr-rep-n-1-15gen2020.pdf (accessed on 8 January 2021).
- World Health Organization. Integrating Neglected Tropical Diseases into Global Health and Development: Fourth WHO Report on Neglected Tropical Diseases; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Martelli, G.; Di Girolamo, C.; Zammarchi, L.; Angheben, A.; Morandi, M.; Tais, S.; Degani, M.; El Hamad, I.; Caligaris, S.; Ciannameo, A.; et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: A cross-sectional study. Clin. Microbiol. Infect. 2017, 23, 335.e1–335.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zammarchi, L.; Vellere, I.; Stella, L.; Bartalesi, F.; Strohmeyer, M.; Bartoloni, A. Spectrum and burden of neglected tropical diseases observed in an infectious and tropical diseases unit in Florence, Italy (2000–2015). Intern. Emerg. Med. 2017, 12, 467–477. [Google Scholar] [CrossRef] [PubMed]
- United Nations World Migration Report. 2020. Available online: https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed on 8 January 2021).
- Schmunis, G.A. Epidemiology of Chagas disease in non endemic countries: The role of international migration. Mem. Inst. Oswaldo Cruz 2007, 102, 75–86. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Natalità e Fecondità Della Popolazione Residente. 2018. Available online: https://www.istat.it/it/files/2019/11/Report_natalit%C3%A0_anno2018_def.pdf (accessed on 8 January 2021).
- Colombo, V.; Giacomelli, A.; Casazza, G.; Galimberti, L.; Bonazzetti, C.; Sabaini, F.; Ridolfo, A.L.; Antinori, S. Trypanosoma cruzi infection in Latin American pregnant women living outside endemic countries and frequency of congenital transmission: A systematic review and meta-analysis. J. Travel Med. 2020. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Geographical Distribution of Areas with a High Prevalence of HTLV-1 Infection; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2015; Available online: www.ecdc.europa.eu (accessed on 8 January 2021).
- Eusebio-Ponce, E.; Anguita, E.; Paulino-Ramirez, R.; Candel, F.J. HTLV-1 infection: An emerging risk. Pathogenesis, epi-demiology, diagnosis and associated diseases. Rev. Esp. Quimioter. 2019, 32, 485–496. [Google Scholar]
- World Health Organisation (WHO). World Malaria Report 2019; World Health Organisation (WHO): Geneva, Switzerland, 2019. [Google Scholar]
- Moya-Alvarez, V.; Abellana, R.; Cot, M. Pregnancy-associated malaria and malaria in infants: An old problem with present consequences. Malar. J. 2014, 13, 271. [Google Scholar] [CrossRef]
- Fried, M.; Duffy, P.E. Malaria during Pregnancy. Cold Spring Harb. Perspect. Med. 2017, 7, a025551. [Google Scholar] [CrossRef]
- Friedman, J.F.; Mital, P.; Kanzaria, H.K.; Olds, G.R.; Kurtis, J.D. Schistosomiasis and pregnancy. Trends Parasitol. 2007, 23, 159–164. [Google Scholar] [CrossRef]
- Sistema Nazionale per le Linee Guida. I Controlli Alla Frontiera/La Frontiera dei Controlli. Controlli Sanitari all’Arrivo e Percorsi di Tutela per i Migranti Ospiti nei Centri di Accoglienza. Linee Guida Salute Migranti. Available online: https://www.saluteinternazionale.info/2018/06/i-controlli-alla-frontiera-la-frontiera-dei-controlli/ (accessed on 8 January 2021).
- Chaves, N.J.; Paxton, G.; Biggs, B.A.; Thambiran, A.; Smith, M.; Williams, J.; Gardiner, J.; Davis, J.S.; on Behalf of the Australasian Society for Infectious Diseases and Refugee Health Network of Australia Guidelines Writing Group. Recommendations for Comprehensive Post-Arrival Health Assessment for People from Refugee-Like Backgrounds. 2016. Available online: https://www.asid.net.au/documents/item/1225 (accessed on 8 January 2021).
- Brasil, P.; Vasconcelos, Z.; Kerin, T.; Gabaglia, C.R.; Ribeiro, I.P.; Bonaldo, M.C.; Damasceno, L.; Pone, M.V.D.S.; Pone, S.M.; Zin, A.; et al. Zika virus vertical transmission in children with confirmed antenatal exposure. Nat. Commun. 2020, 11, 3510. [Google Scholar] [CrossRef]
- Ospina, M.L.; Tong, V.T.; Gonzalez, M.; Valencia, D.; Mercado, M.; Gilboa, S.M.; Rodriguez, A.J.; Tinker, S.C.; Rico, A.; Winfield, C.M.; et al. Zika Virus Disease and Pregnancy Outcomes in Colombia. N. Engl. J. Med. 2020, 383, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Shapiro-Mendoza, C.K.; Rice, M.E.; Galang, R.R.; Fulton, A.C.; Vanmaldeghem, K.; Prado, M.V.; Ellis, E.; Anesi, M.S.; Simeone, R.M.; Petersen, E.E.; et al. Pregnancy Outcomes After Maternal Zika Virus Infection During Pregnancy—U.S. Territories, January 1, 2016–April 25, 2017. Morb. Mortal. Wkly. Rep. 2017, 66, 615–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Programma Regionale per la Prevenzione e il Controllo Della Malattia di Chagas Congenita: Indicazioni per l’Assistenza in Gravidanza. 2012. Available online: https://www.regione.toscana.it/documents/10180/13329059/Allegato+parere+n.+46-2015+Prev+e+conrollo+malattia+di+Chagas.pdf/6e153700-0d7b-4d70-b098-faba975c6de8?version=1.0 (accessed on 8 January 2021).
- Investing to Overcome the Global Impact of Neglected Tropical Diseases: Third WHO Report on Neglected Tropical Diseases 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/152781/9789241564861_eng.pdf?sequence=1 (accessed on 8 January 2021).
- Centre for Disease Control and Prevention. Zika Travel Information. Available online: https://wwwnc.cdc.gov/travel/page/zika-travel-information (accessed on 8 January 2021).
- Asundi, A.; Beliavsky, A.; Liu, X.J.; Akaberi, A.; Schwarzer, G.; Bisoffi, Z.; Requena-Méndez, A.; Shrier, I.; Greenaway, C. Prevalence of strongyloidiasis and schistosomiasis among migrants: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e236–e248. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.F.; Olveda, R.M.; Mirochnick, M.H.; Bustinduy, A.L.; Elliott, A.M. Praziquantel for the treatment of schistosomiasis during human pregnancy. Bull. World Health Organ. 2017, 96, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Monge-Maillo, B.; Lopez-Velez, R. Is screening for malaria necessary among asymptomatic refugees and immigrants coming from endemic countries? Expert Rev. Anti-Infect. Ther. 2011, 9, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Pousibet-Puerto, J.; Cabezas-Fernández, M.T.; Lozano-Serrano, A.B.; Vázquez-Villegas, J.; Soriano-Pérez, M.J.; Cabeza-Barrera, I.; Cuenca-Gómez, J.A.; Salas-Coronas, J. Submicroscopic Malaria in Migrants from Sub-Saharan Africa, Spain. Emerg. Infect. Dis. 2019, 25, 349–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takem, E.N.; D’Alessandro, U. Malaria in Pregnancy. Mediterr. J. Hematol. Infect. Dis. 2013, 5, e2013010. [Google Scholar] [CrossRef]
- Krajden, S.; Panisko, D.; Tobe, B.; Yang, J.; Keystone, J. Prolonged infection with Plasmodium falciparum in a semiimmune patient. Trans. R. Soc. Trop. Med. Hyg. 1991, 85, 731–732. [Google Scholar] [CrossRef]
- Ashley, E.A.; White, N.J. The duration of Plasmodium falciparum infections. Malar. J. 2014, 13, 500. [Google Scholar] [CrossRef] [Green Version]
- Zammarchi, L.; Angheben, A.; Galli, L.; Dani, C.; Di Tommaso, M.; Petraglia, F.; Aliani, F.B.; Trotta, M.; Spinicci, M.; Viñas, P.A.; et al. Ongoing mother-to-child transmission of Chagas disease in Italy: 2014–18 estimates. J. Travel Med. 2020. [Google Scholar] [CrossRef]
- Taylor, G.P.; Bodéus, M.; Courtois, F.; Pauli, G.; Del Mistro, A.; Machuca, A.; Padua, E.; Andersson, S.; Goubau, P.; Chieco-Bianchi, L.; et al. The Seroepidemiology of Human T-Lymphotropic Viruses. J. Acquir. Immune Defic. Syndr. 2005, 38, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Reagan-Steiner, S.; Goodenough, D.; Russell, K.; Tanner, M.; Lewis, L.; Petersen, E.E.; Powers, A.M.; Kniss, K.; Meaney-Delman, D.; et al. Patterns in Zika Virus Testing and Infection, by Report of Symptoms and Pregnancy Status—United States, January 3–March 5, 2016. Morb. Mortal. Wkly. Rep. 2016, 65, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Mendez, A.; Bussion, S.; Aldasoro, E.; Jackson, Y.; Angheben, A.; Moore, D.; Pinazo, M.-J.; Gascón, J.; Muñoz, J.; Sicuri, E. Cost-effectiveness of Chagas disease screening in Latin American migrants at primary health-care centres in Europe: A Markov model analysis. Lancet Glob. Health 2017, 5, e439–e447. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Emerging Infectious Diseases | Main Epidemiological Features | Rate of Mother to Child Transmission | Main Clinical Consequences on Maternal and Neonatal Health | Recommended Management in Pregnant Women and Their Newborns |
|---|---|---|---|---|
| Chagas disease | Endemic in continental Latin America. | ≈4% in non-endemic setting [21]. | Chagasic cardiopathy and intestinal megasyndromes in ≈30% of infected subjects. | Serological screening in pregnant women at risk. Testing and follow-up of their children. Antiparasitic treatment of the infected children within 1 year of life. Antiparasitic treatment of infected women by the end of breastfeeding [2]. |
| Human T-lymphotropic virus 1 infection | Higher prevalence in several sub-Saharan African and Latin American countries, Japan, Iran, Romania [22]. | 15–20% (mainly through breastfeeding) [9]. | Adult T-cell leukemia/lymphoma or HTLV-1-associated myelopathy/tropical spastic paraparesis in <10% of infected subjects [23]. | Serological screening in pregnant women at risk. Short term breast feeding or breastfeeding avoidance in HTLV-1 infected women [9]. |
| Malaria | Endemic in several tropical and sub-tropical countries. 90% of cases occur in Africa [24]. | Congenital malaria occurs in <1–6% of cases [25]. | Increased incidence of maternal anemia, LBW, IUGR, stillbirth, miscarriage, congenital malaria [26]. | Testing with polymerase chain reaction for malaria all pregnant refugees originating from sub-Saharan Africa not receiving pre-departure therapy [12]. Treatment of affected women. |
| Schistosomiasis | Endemic in several tropical and sub-tropical countries. 85% of cases occur in Africa. | Congenital transmission is only anecdotally reported. | Increased incidence, of maternal anemia, LBW and prematurity [27]. | Serological screening of migrants from endemic countries and antiparasitic treatment of those seropositive [10,28,29]. |
| Zika virus infection | Causes outbreak in several tropical and subtropical countries. | Up to 65% [30]. | Reported risk of CZS (characterized by microcephaly and other clinical features) is highly variable (from 1 to 8%) in neonates from pregnant women with confirmed infection [31,32] | Testing of all symptomatic and asymptomatic pregnant women returning from an at risk area or sexually exposed to a partner recently returned from an at risk area [14]. |
| Disease | Diagnostic Test Performed in Pregnant Women at Risk | Management of Pregnant Woman in Case of Positive Results | Suggested Management of the Newborn in Case of Positive Results |
|---|---|---|---|
| Chagas disease | Chemiluminescent Microparticle Immunoassay (CMIA), Architect Chagas®, Abbott Laboratories, Wiesbaden, Germany. | Confirmation with a second different serological test. Clinical and instrumental evaluation (electrocardiogram and echocardiogram) of the women to assess presence of cardiac or gastrointestinal involvement. Treatment with benznidazole or nifurtimox of the women after breastfeeding. | Clinical and laboratory evaluation at birth. Referral to a pediatric infectious diseases centre for clinical and laboratory follow-up. |
| Human T-lymphotropic virus 1 infection | CMIA, Architect rHTLV-I/II, Abbott Laboratories, Wiesbaden, Germany. | Confirmation with Western Blot (WB) and proviral load determination.Infected women should avoid breastfeeding, preferring formula milk feeding, frozen-thawed breast milk or short-term breastfeeding (≤3 months). | Referral to a pediatric infectious diseases centre for clinical and laboratory follow-up. |
| Malaria | Loop mediated isothermal amplification (LAMP), Alethia™ Malaria, Launch Diagnostics, Longfield, United Kingdom. | Microscopy is necessary for confirmation and definition of parasitemia; PCR real time for the determination of the species.Infected women will receive antimalarial treatment according to severity, Plasmodium species and gestational age. | Clinical and laboratory evaluation at birth and follow-up. |
| Schistosomiasis | Western blot (WB), LD-BIO Diagnostics, Lyon, France. | Parasitological exams of urine (three samples) and stools (three samples) and determination of CCA (circulating cathodic antigen) are needed to confirm active parasitosis.Treatment with praziquantel can be programmed during the second/third trimester of pregnancy or after childbirth. | Clinical evaluation and follow-up. |
| Zika virus infection | Serological test (ELISA ZIKV IgG-IgM, Euroimmun AG, Luebeck, Germany) and a molecular test for virus identification in serum and urine (Zika Virus Real Time RT-PCR Kit, Liferiver/Shanghai ZJ Biotech Co. China). | Serial fetal ultrasounds; Possibility of amniocentesis; possibility of VTP according to current legislation. | Clinical and laboratory evaluation at birth. Referral to a pediatric infectious diseases centre for clinical and laboratory follow-up. |
| Type of Potential Risk Factor | Frequency of Potential Risk Factor |
|---|---|
| Being foreign-born | 145/429 (34%) |
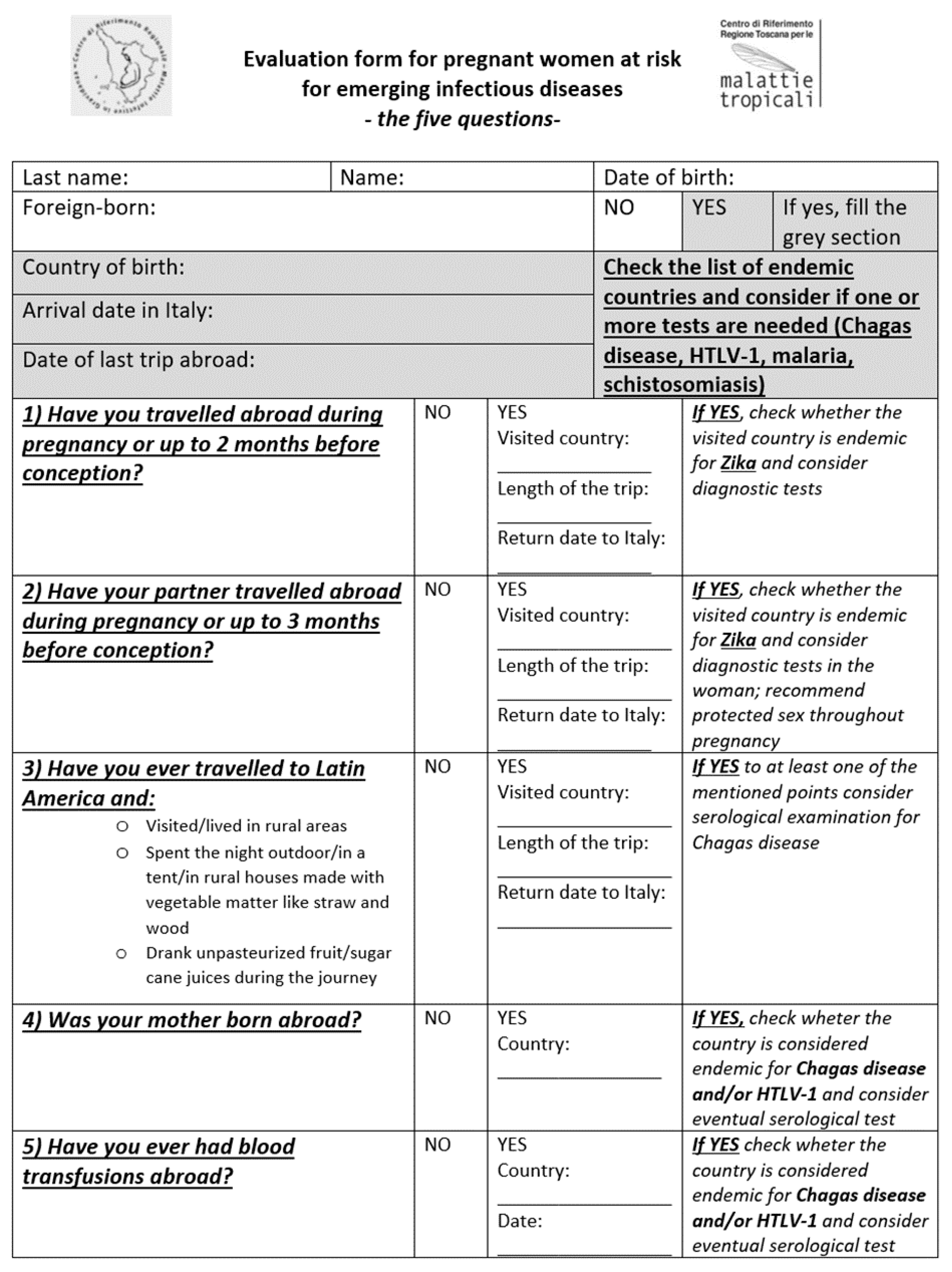
| Having travelled abroad during pregnancy or up to 2 months before conception | 27/429 (6%) |
| Having a partner who has travelled abroad during pregnancy or up to 3 months before conception | 23/429 (5%) |
| Having ever travelled to Latin America and having had high risk behavior (see Figure 1) | 19/429 (4%) |
| Having a foreign-born mother | 148/429 (34%) * |
| Having ever received blood transfusions abroad | 0/429 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modi, G.; Borchi, B.; Giaché, S.; Campolmi, I.; Trotta, M.; Di Tommaso, M.; Strambi, N.; Bartoloni, A.; Zammarchi, L. Emerging Infectious Diseases in Pregnant Women in a Non-Endemic Area: Almost One Out of Four Is at Risk. Pathogens 2021, 10, 56. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10010056
Modi G, Borchi B, Giaché S, Campolmi I, Trotta M, Di Tommaso M, Strambi N, Bartoloni A, Zammarchi L. Emerging Infectious Diseases in Pregnant Women in a Non-Endemic Area: Almost One Out of Four Is at Risk. Pathogens. 2021; 10(1):56. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10010056
Chicago/Turabian StyleModi, Giulia, Beatrice Borchi, Susanna Giaché, Irene Campolmi, Michele Trotta, Mariarosaria Di Tommaso, Noemi Strambi, Alessandro Bartoloni, and Lorenzo Zammarchi. 2021. "Emerging Infectious Diseases in Pregnant Women in a Non-Endemic Area: Almost One Out of Four Is at Risk" Pathogens 10, no. 1: 56. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10010056