
Evaluation of Critical Quality Attributes of a Pentavalent (A, C, Y, W, X) Meningococcal Conjugate Vaccine for Global Use

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Critical Quality Attributes of Clinical Lots of NmCV-5 and Vaccine Components
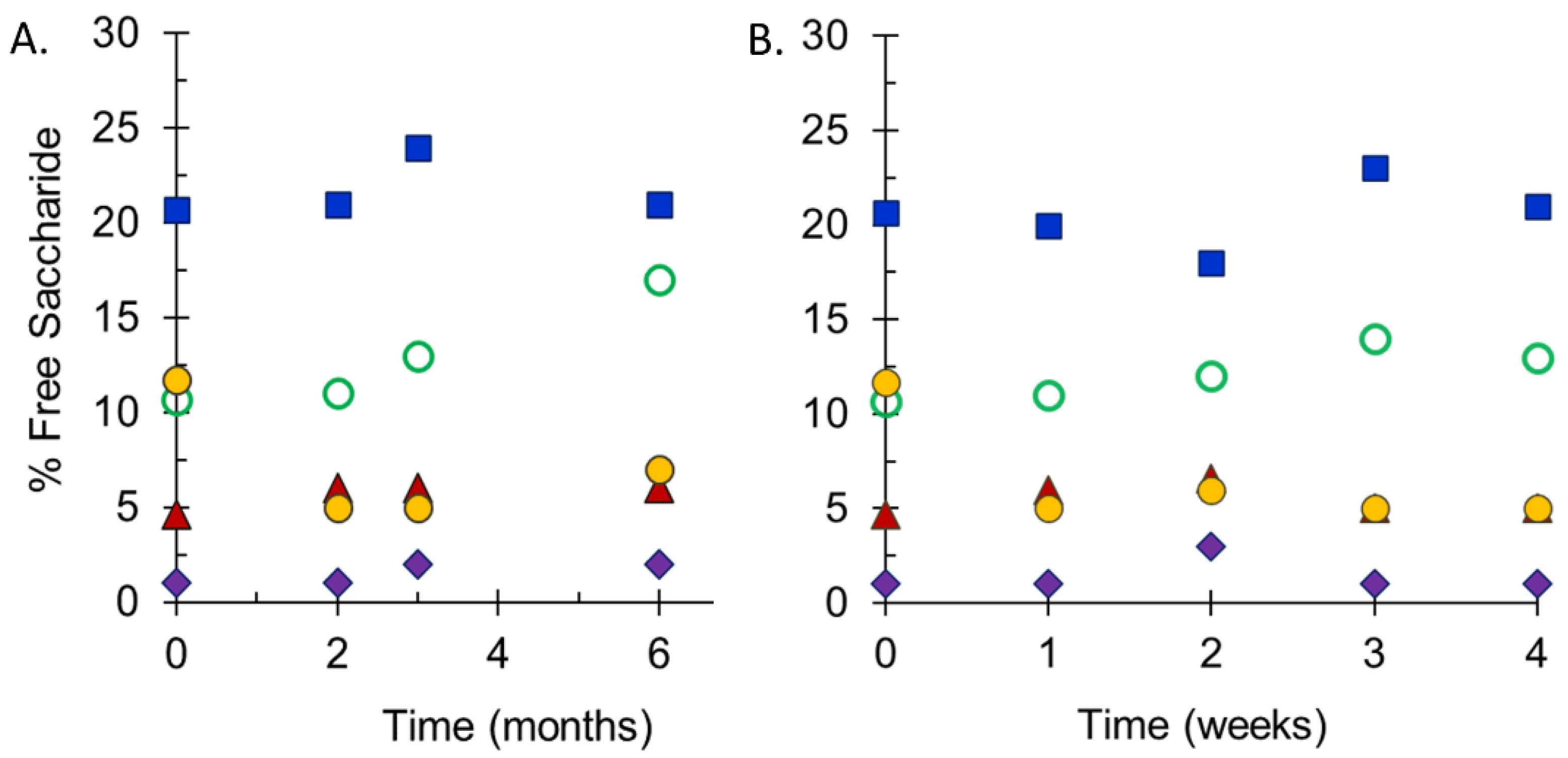
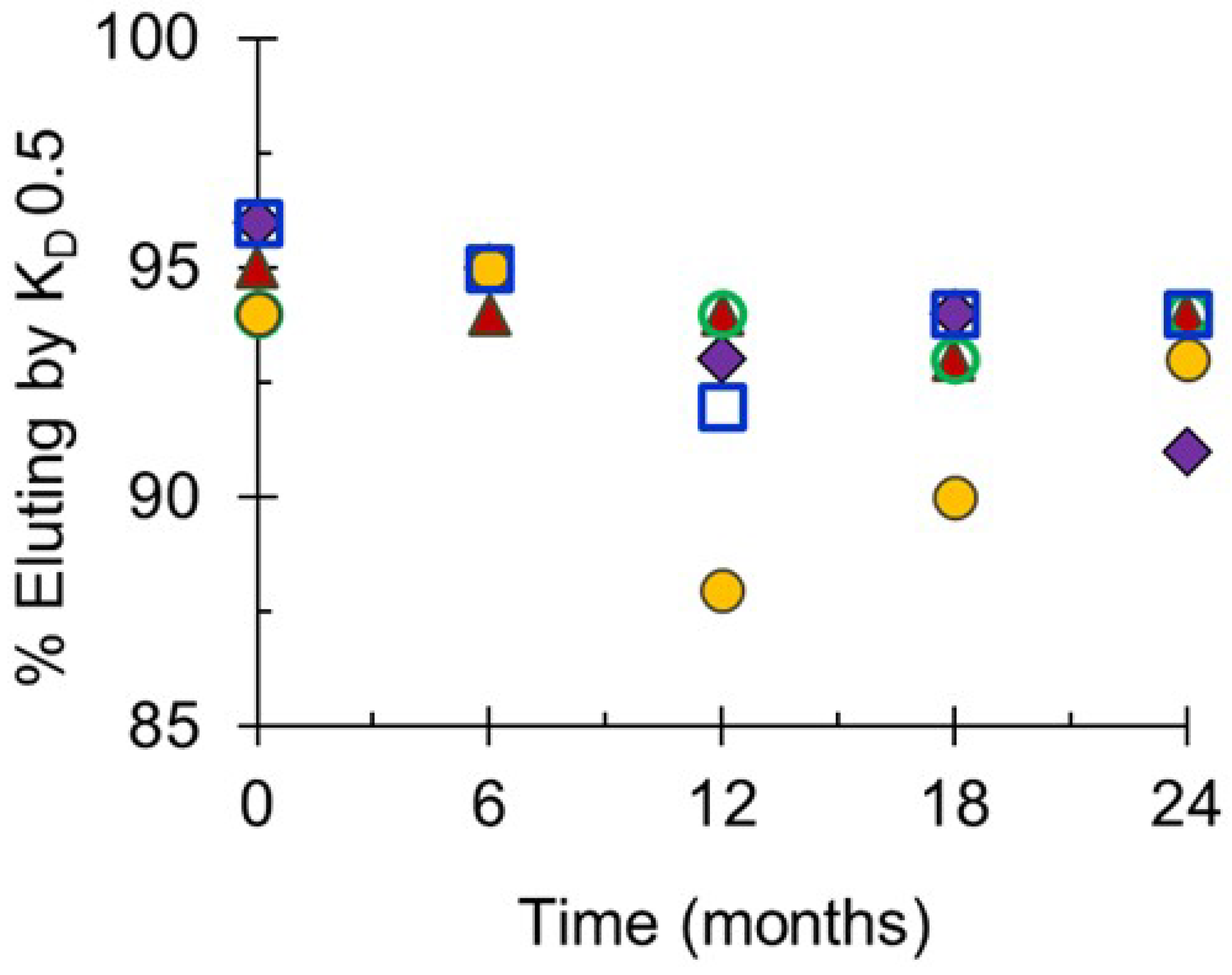
2.2. Stability of Monovalent Drug Substances and NmCV-5 Drug Product
3. Preclinical Immune Responses to NmCV-5
3.1. Serogroup-Specific Polysaccharide Responses in Mice to a Pentavalent R&D Vaccine Formulation
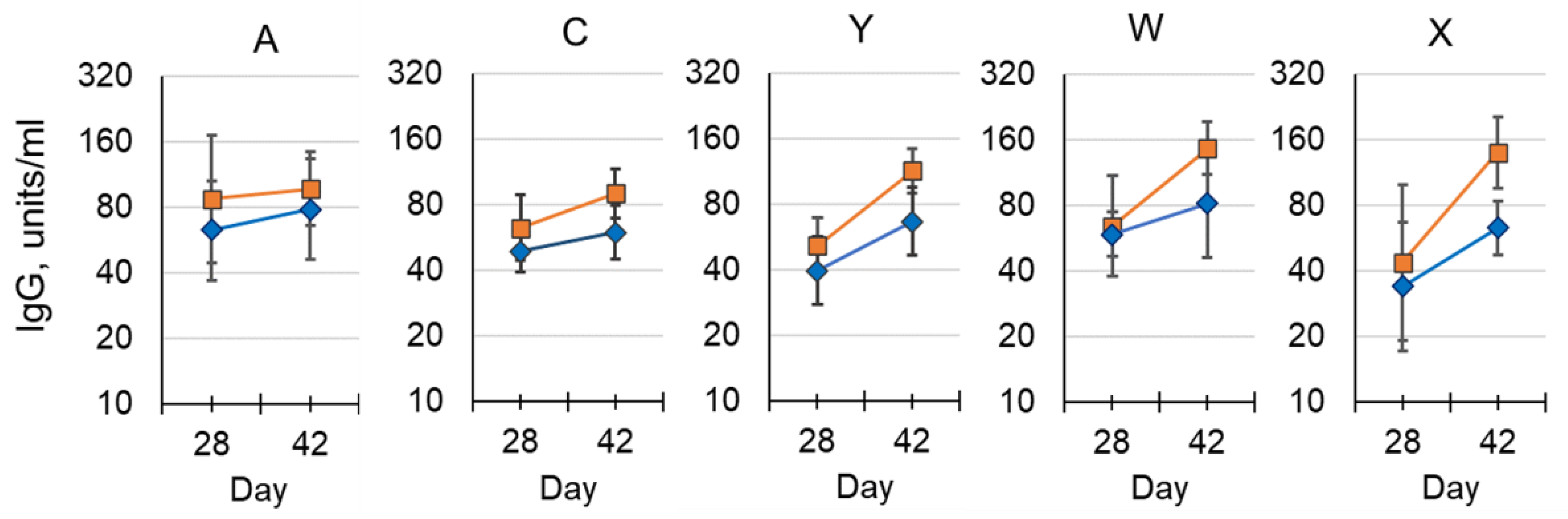
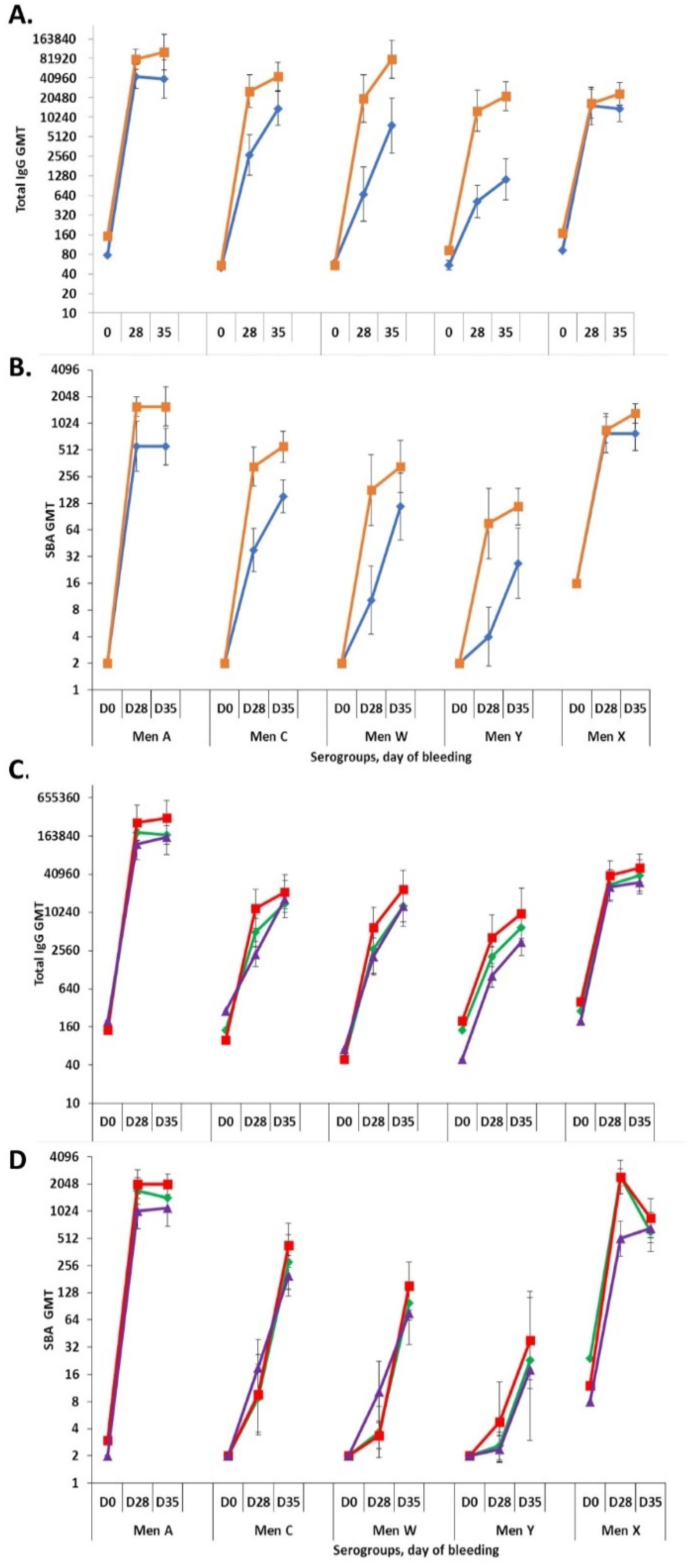
3.2. Serogroup-Specific IgG and Bactericidal Antibody Responses in Rabbits to NmCV-5 Clinical Lots
4. Discussion
5. Materials and Methods
5.1. Materials
5.2. O-acetylation
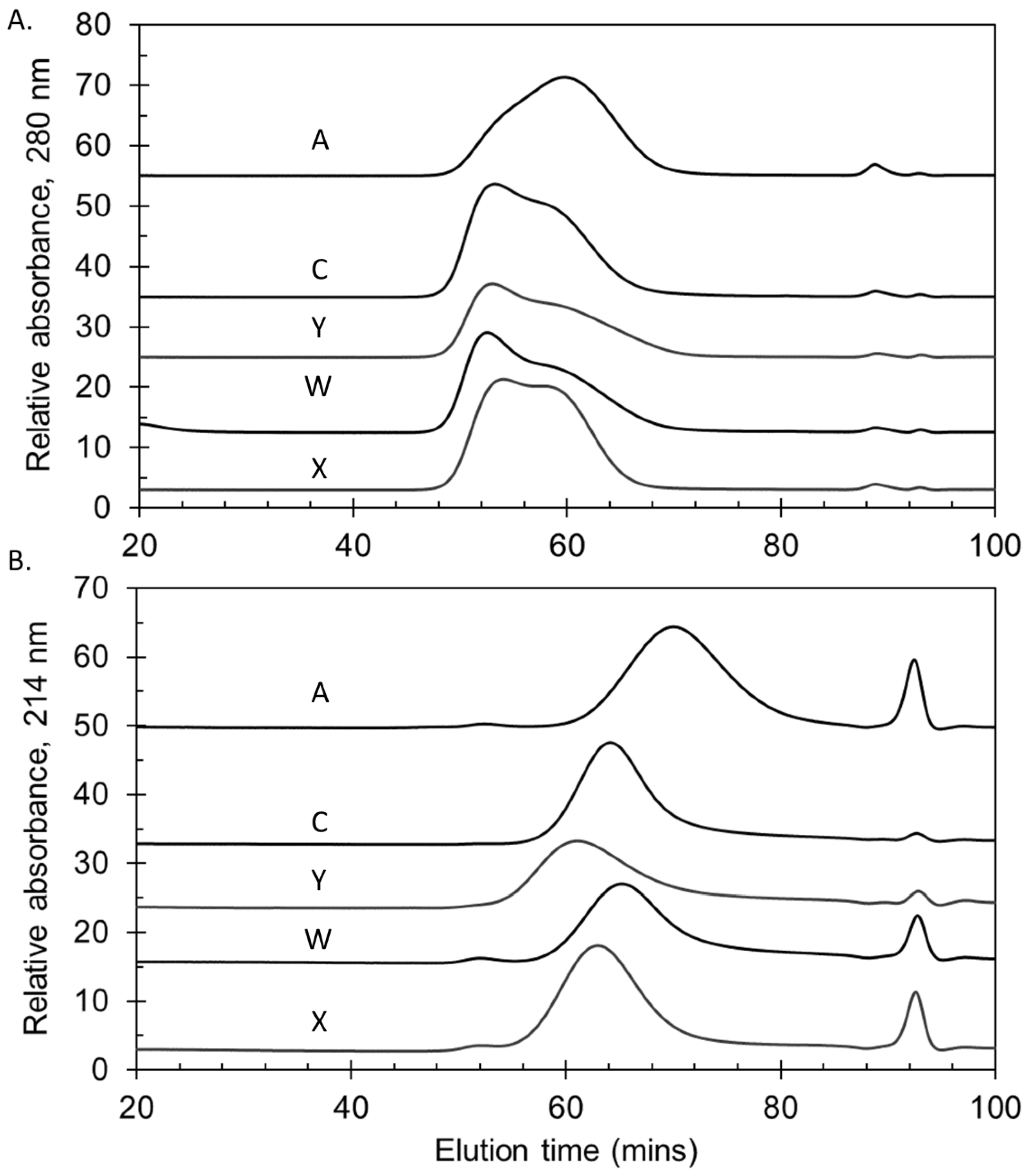
5.3. Molecular Size
5.4. Endotoxin Content
5.5. Protein Content
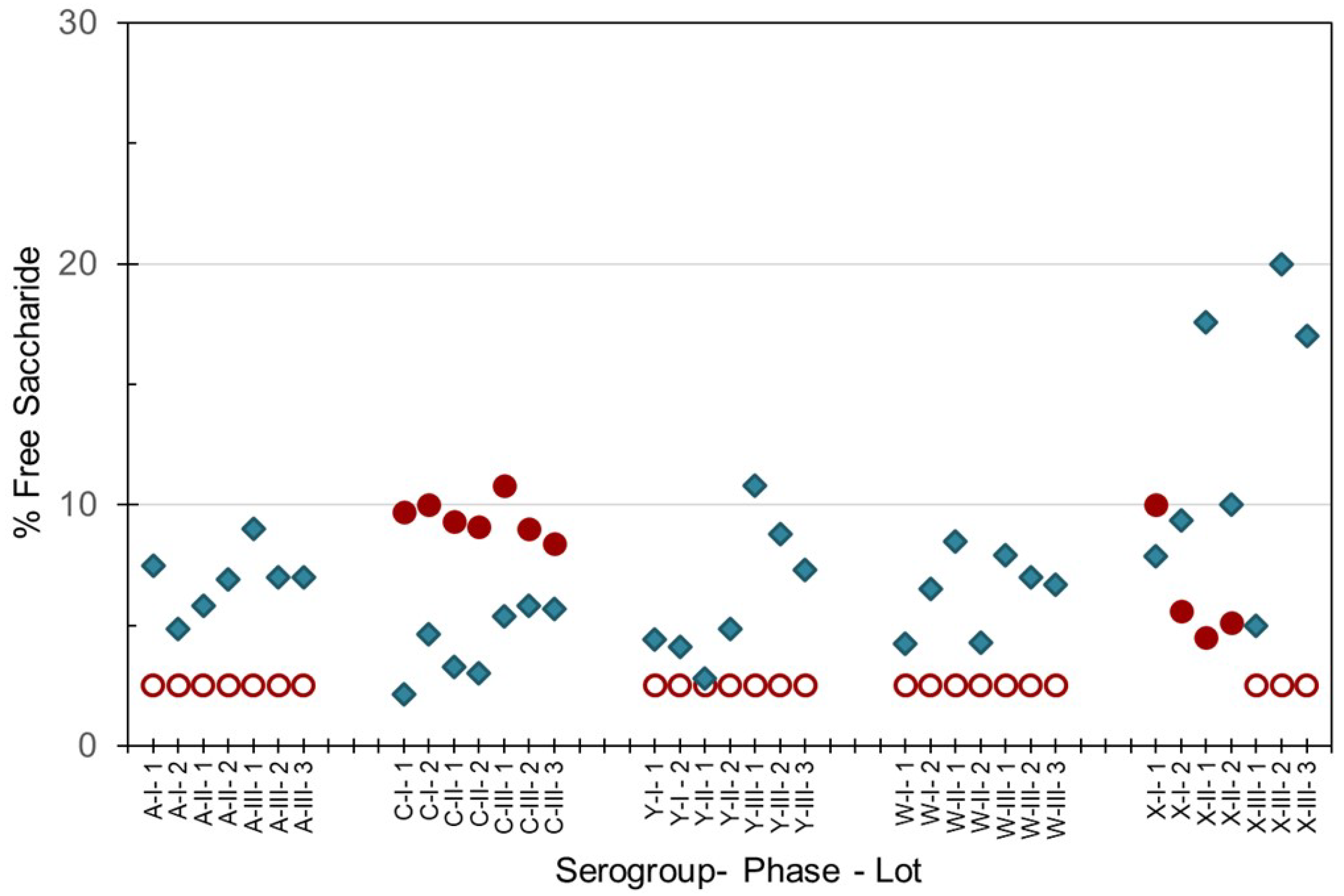
5.6. Free Saccharide
5.7. Adjuvant Adsorption
5.8. Mouse Immunogenicity
5.9. Rabbit Immunogenicity
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Patents
References
- International Coordination Group on Vaccine Provision for Epidemic Meningitis: Report of the Annual Meeting: Geneva, 18 September 2018; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/279828/WHO-WHE-IHM-2019.1-eng.pdf (accessed on 4 March 2021).
- Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019, 18, 459–480. [CrossRef] [Green Version]
- van Kessel, F.; van den Ende, C.; Oordt-Speets, A.M.; Kyaw, M.H. Outbreaks of meningococcal meningitis in non-African countries over the last 50 years: A systematic review. J. Glob. Health 2019, 9, 010411. [Google Scholar] [CrossRef] [PubMed]
- Meningococcal Meningitis; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/en/news-room/fact-sheets/detail/meningococcal-meningitis (accessed on 4 March 2021).
- Alderson, M.R.; Welsch, J.A.; Regan, K.; Newhouse, L.; Bhat, N.; Marfin, A.A. Vaccines to Prevent Meningitis: Historical Perspectives and Future Directions. Microorganisms 2021, 9, 771. [Google Scholar] [CrossRef]
- Immunological Basis for Immunization Series: Module 15: Meningococcal Disease; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/immunization/research/development/Meningococcal_disease_module15.pdf (accessed on 4 March 2021).
- Kulkarni, P.S.; Jadhav, S.S.; LaForce, F.M. Developmental strategy for a new Group A meningococcal conjugate vaccine (MenAfriVac(R)). Hum. Vaccin. Immunother. 2018, 14, 1103–1106. [Google Scholar] [CrossRef] [Green Version]
- Soeters, H.M.; Diallo, A.O.; Bicaba, B.W.; Kadadé, G.; Dembélé, A.Y.; Acyl, M.A.; Nikiema, C.; Sadji, A.Y.; Poy, A.N.; Lingani, C.; et al. Bacterial Meningitis Epidemiology in Five Countries in the Meningitis Belt of Sub-Saharan Africa, 2015–2017. J. Infect Dis. 2019, 220, S165–S174. [Google Scholar] [CrossRef] [PubMed]
- Epidemic meningitis control in countries in the African meningitis belt, 2018. Wkly Epidemiol Rec. 2019, 94, 179–188. Available online: https://apps.who.int/iris/bitstream/handle/10665/311704/WER9414_15.pdf?ua=1 (accessed on 15 May 2021).
- Harrison, L.H.; Trotter, C.L.; Ramsay, M.E. Global epidemiology of meningococcal disease. Vaccine 2009, 27, B51–B63. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, K.; Lingani, C.; Aderinola, O.M.; Goumbi, K.; Bicaba, B.; Edea, Z.A.; Glèlè, C.; Sarkodie, B.; Tamekloe, A.; Ngomba, A.; et al. Meningococcal Meningitis Outbreaks in the African Meningitis Belt After Meningococcal Serogroup A Conjugate Vaccine Introduction, 2011–2017. J. Infect Dis. 2019, 220, S225–S232. [Google Scholar] [CrossRef] [PubMed]
- Sidikou, F.; Zaneidou, M.; Alkassoum, I.; Schwartz, S.; Issaka, B.; Obama, R.; Lingani, C.; Tate, A.; Ake, F.; Sakande, S.; et al. MenAfriNet consortium. Emergence of epidemic Neisseria meningitidis serogroup C in Niger, 2015: An analysis of national surveillance data. Lancet Infect Dis. 2016, 16, 1288–1294. [Google Scholar] [CrossRef] [Green Version]
- No authors listed. Control of epidemic meningitis in countries in the African meningitis belt, 2019. Wkly Epidemiol Rec. 2020, 95, 133–144.
- WHO–Meningococcal vaccines: WHO position paper, November 2011. Wkly Epidemiol Rec. 2011, 47, 521–540. Available online: https://www.who.int/wer/2011/wer8647.pdf?ua=1 (accessed on 15 May 2021).
- WHO-Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control)-List of Prequalified Vaccines-Menactra; World Health Organization: Geneva, Switzerland, 2021; Available online: https://extranet.who.int/pqweb/content/menactra (accessed on 4 March 2021).
- WHO-Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control)-List of Prequalified Vaccines-Menveo; World Health Organization: Geneva, Switzerland, 2021; Available online: https://extranet.who.int/pqweb/content/menveo (accessed on 4 March 2021).
- WHO-Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control)-List of Prequalified Vaccines-Nimenrix; World Health Organization: Geneva, Switzerland, 2021; Available online: https://extranet.who.int/pqweb/content/nimenrix (accessed on 4 March 2021).
- Alderson, M.R.; LaForce, F.M.; Sobanjo-Ter Meulen, A.; Hwang, A.; Preziosi, M.P.; Klugman, K.P. Eliminating Meningococcal Epidemics From the African Meningitis Belt: The Case for Advanced Prevention and Control Using Next-Generation Meningococcal Conjugate Vaccines. J. Infect Dis. 2019, 220, S274–S278. [Google Scholar] [CrossRef] [PubMed]
- Hickey, J.M.; Toprani, V.M.; Kaur, K.; Mishra, R.P.N.; Goel, A.; Oganesyan, N.; Lees, A.; Sitrin, R.; Joshi, S.B.; Volkin, D.B. Analytical Comparability Assessments of 5 Recombinant CRM(197) Proteins From Different Manufacturers and Expression Systems. J. Pharm. Sci. 2018, 107, 1806–1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.H.; Neuzil, K.M.; Boyce, C.R.; Pasetti, M.F.; Reymann, M.K.; Martellet, L.; Hosken, N.; LaForce, F.M.; Dhere, R.M.; Pisal, S.S.; et al. Safety and immunogenicity of a pentavalent meningococcal conjugate vaccine containing serogroups A, C, Y, W, and X in healthy adults: A phase 1, single-centre, double-blind, randomised, controlled study. Lancet Infect Dis. 2018, 18, 1088–1096. [Google Scholar] [CrossRef] [Green Version]
- Chilukuri, S.R.; Reddy, P.; Avalaskar, N.; Mallya, A.; Pisal, S.; Dhere, R.M. Process development and immunogenicity studies on a serogroup ‘X’ Meningococcal polysaccharide conjugate vaccine. Biologicals 2014, 42, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Tapia, M.D.; Sow, S.O.; Naficy, A.; Diallo, F.; Haidara, F.C.; Chaudhari, A.; Martellet, L.; Traore, A.; Townsend-Payne, K.; Borrow, R.; et al. Meningococcal Serogroup ACYWX Conjugate Vaccine in Malian Toddlers. NEJM 2021, 384, 2115–2123. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.G.; Gao, D.; Kim, Y.J.; Harris, R.; Cash, P.W.; Schofield, T.L.; Zhang, R.; Qin, Q. ICH Q5C Stability Testing of Biotechnological/Biological Products. ICH Qual. Guidel. 2017. [CrossRef]
- Requirements for Meningococcal Polysaccharide Vaccine. In Annex 2. WHO Technical Report Series-Number 658; World Health Organization: Geneva, Switzerland, 1980; Available online: https://www.who.int/biologicals/publications/trs/areas/vaccines/meningococcal/WHO_TRS_658_(part2)_MeningA6.pdf (accessed on 4 March 2021).
- Recommendations to Assure the Quality, Safety and Efficacy of Group A Meningococcal Conjugate Vaccines. In Annex 2. WHO Technical Report Series-Number 962; World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/biologicals/vaccines/Annex_2_WHO_TRS_962.pdf (accessed on 4 March 2021).
- Recommendations for the Production and Control of Meningococcal Group C Conjugate Vaccines. In Annex 2. WHO Technical Report Series-Number 924; World Health Organization: Geneva, Switzerland, 2004; Available online: https://www.who.int/biologicals/publications/trs/areas/vaccines/meningococcal/WHO_TRS_924_MeningA2_102-128.pdf (accessed on 4 March 2021).
- Hitri, K.; Kuttel, M.M.; De Benedetto, G.; Lockyer, K.; Gao, F.; Hansal, P.; Rudd, T.R.; Beamish, E.; Rijpkema, S.; Ravenscroft, N.; et al. O-acetylation of typhoid capsular polysaccharide confers polysaccharide rigidity and immunodominance by masking additional epitopes. Vaccine 2019, 37, 3866–3875. [Google Scholar] [CrossRef]
- Bardotti, A.; Averani, G.; Berti, F.; Berti, S.; Carinci, V.; D'Ascenzi, S.; Fabbri, B.; Giannini, S.; Giannozzi, A.; Magagnoli, C.; et al. Physicochemical characterisation of glycoconjugate vaccines for prevention of meningococcal diseases. Vaccine 2008, 26, 2284–2296. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, K.; Gao, F.; Derrick, J.P.; Bolgiano, B. Structural correlates of carrier protein recognition in tetanus toxoid-conjugated bacterial polysaccharide vaccines. Vaccine 2015, 33, 1345–1352. [Google Scholar] [CrossRef]
- Berti, F. Multivalent meningococcal conjugate vaccines: Chemical conjugation strategies used for the preparation of vaccines licensed or in clinical trials. In Carbohydrate-Based Vaccines: From Concept to Clinic; ACS Publications: New York, NY, USA, 2018; pp. 123–137. [Google Scholar]
- Tunheim, G.; Naess, L.M.; Acevedo, R.; Fjeldheim, Å., K.; Bolstad, K.; García, L.; Cardoso, D.; Aase, A.; Zayas, C.; González, H.; et al. Preclinical immunogenicity study of trivalent meningococcal AWX-OMV vaccines for the African meningitis belt. Vaccine 2014, 32, 6631–6638. [Google Scholar] [CrossRef] [PubMed]
- Ravenscroft, N.; Omar, A.; Haralson, S.; Alderson, M.R.; LaForce, F.M.; Gao, F.; Beresford, N.; Moran, E.; Care, R.; Swann, C.; et al. Analytical Methods and Evaluation of a Pentavalent Meningococcal Conjugate Vaccine Candidate [Poster]. In Proceedings of the Meningitis and Septicaemia in Children and Adults, Meningitis Research Foundation, London, UK, 4–5 November 2015. [Google Scholar]
- Ravenscroft, N.; Costantino, P.; Talaga, P.; Rodriguez, R.; Egan, W. Glycoconjugate Vaccines. In Vaccine Analysis: Strategies, Principles, and Control; Nunnally, B.K., Turula, V.E., Sitrin, R.D., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 301–381. [Google Scholar]
- Zipursky, S.; Djingarey, M.H.; Lodjo, J.C.; Olodo, L.; Tiendrebeogo, S.; Ronveaux, O. Benefits of using vaccines out of the cold chain: Delivering meningitis A vaccine in a controlled temperature chain during the mass immunization campaign in Benin. Vaccine 2014, 32, 1431–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Use of MenAfriVac™ (Meningitis A Vaccine) in a Controlled Temperature Chain (CTC) During Campaigns; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/immunization/documents/WHO_IVB_13.04_5_6/en/ (accessed on 4 March 2021).
- Guidelines on the Stability Evaluation of Vaccines for Use Under Extended Controlled Temperature Conditions. In Annex 5. WHO Technical Report Series-Number 999; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/biologicals/areas/vaccines/Annex_5_Guidelines_on_Stability_evaluation_vaccines_ECTC.pdf (accessed on 4 March 2021).
- Barel, L.A.; Mulard, L.A. Classical and novel strategies to develop a Shigella glycoconjugate vaccine: From concept to efficacy in human. Hum. Vaccin Immunother 2019, 15, 1338–1356. [Google Scholar] [CrossRef] [PubMed]
- Defeating Meningitis by 2030 Global Road Map (Version 26 October 2020); World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/m/item/defeating-meningtis-by-2030-global-road-map-(version-20-october-2020) (accessed on 4 March 2021).
- Jones, C.; Lemercinier, X. Use and validation of NMR assays for the identity and O-acetyl content of capsular polysaccharides from Neisseria meningitidis used in vaccine manufacture. J. Pharm. Biomed. Anal. 2002, 30, 1233–1247. [Google Scholar] [CrossRef]
- Gao, F.; Beresford, N.; Lockyer, K.; Burkin, K.; Rigsby, P.; Bolgiano, B. Saccharide dosage content of meningococcal polysaccharide conjugate vaccines determined using WHO International Standards for serogroup A, C, W, Y and X polysaccharides. Biologicals 2021, 70, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.C.; Bliu, A.; Kunkel, J.P. Quantitation of serogroups in multivalent polysaccharide-based meningococcal vaccines: Optimisation of hydrolysis conditions and chromatographic methods. Vaccine 2013, 31, 3702–3711. [Google Scholar] [CrossRef] [PubMed]
- Beresford, N.J.; Martino, A.; Feavers, I.M.; Corbel, M.J.; Bai, X.; Borrow, R.; Bolgiano, B. Quality, immunogenicity and stability of meningococcal serogroup ACWY-CRM(197), DT and TT glycoconjugate vaccines. Vaccine 2017, 35, 3598–3606. [Google Scholar] [CrossRef]
- CombiStats v5; EDQM Council of Europe: Strasbourg, France, 2013; Available online: https://www.edqm.eu/combistats/ (accessed on 4 March 2021).







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolgiano, B.; Moran, E.; Beresford, N.J.; Gao, F.; Care, R.; Desai, T.; Nordgren, I.K.; Rudd, T.R.; Feavers, I.M.; Bore, P.; et al. Evaluation of Critical Quality Attributes of a Pentavalent (A, C, Y, W, X) Meningococcal Conjugate Vaccine for Global Use. Pathogens 2021, 10, 928. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080928
Bolgiano B, Moran E, Beresford NJ, Gao F, Care R, Desai T, Nordgren IK, Rudd TR, Feavers IM, Bore P, et al. Evaluation of Critical Quality Attributes of a Pentavalent (A, C, Y, W, X) Meningococcal Conjugate Vaccine for Global Use. Pathogens. 2021; 10(8):928. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080928
Chicago/Turabian StyleBolgiano, Barbara, Eilís Moran, Nicola J. Beresford, Fang Gao, Rory Care, Trusha Desai, Ida Karin Nordgren, Timothy R. Rudd, Ian M. Feavers, Prashant Bore, and et al. 2021. "Evaluation of Critical Quality Attributes of a Pentavalent (A, C, Y, W, X) Meningococcal Conjugate Vaccine for Global Use" Pathogens 10, no. 8: 928. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10080928