Seroprevalence of the Strongyloides stercoralis Infection in Humans from Yungas Rainforest and Gran Chaco Region from Argentina and Bolivia

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Populations
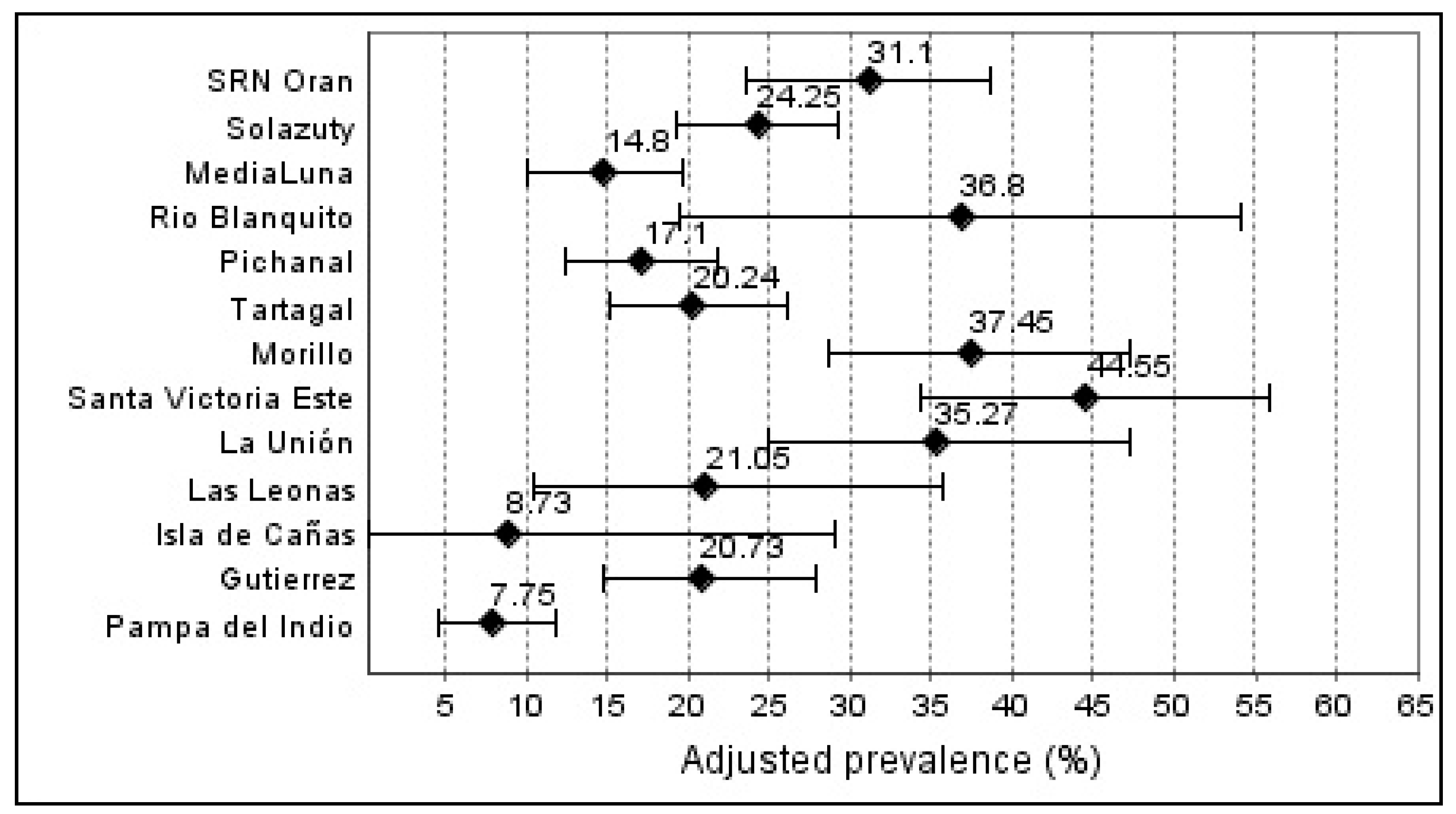
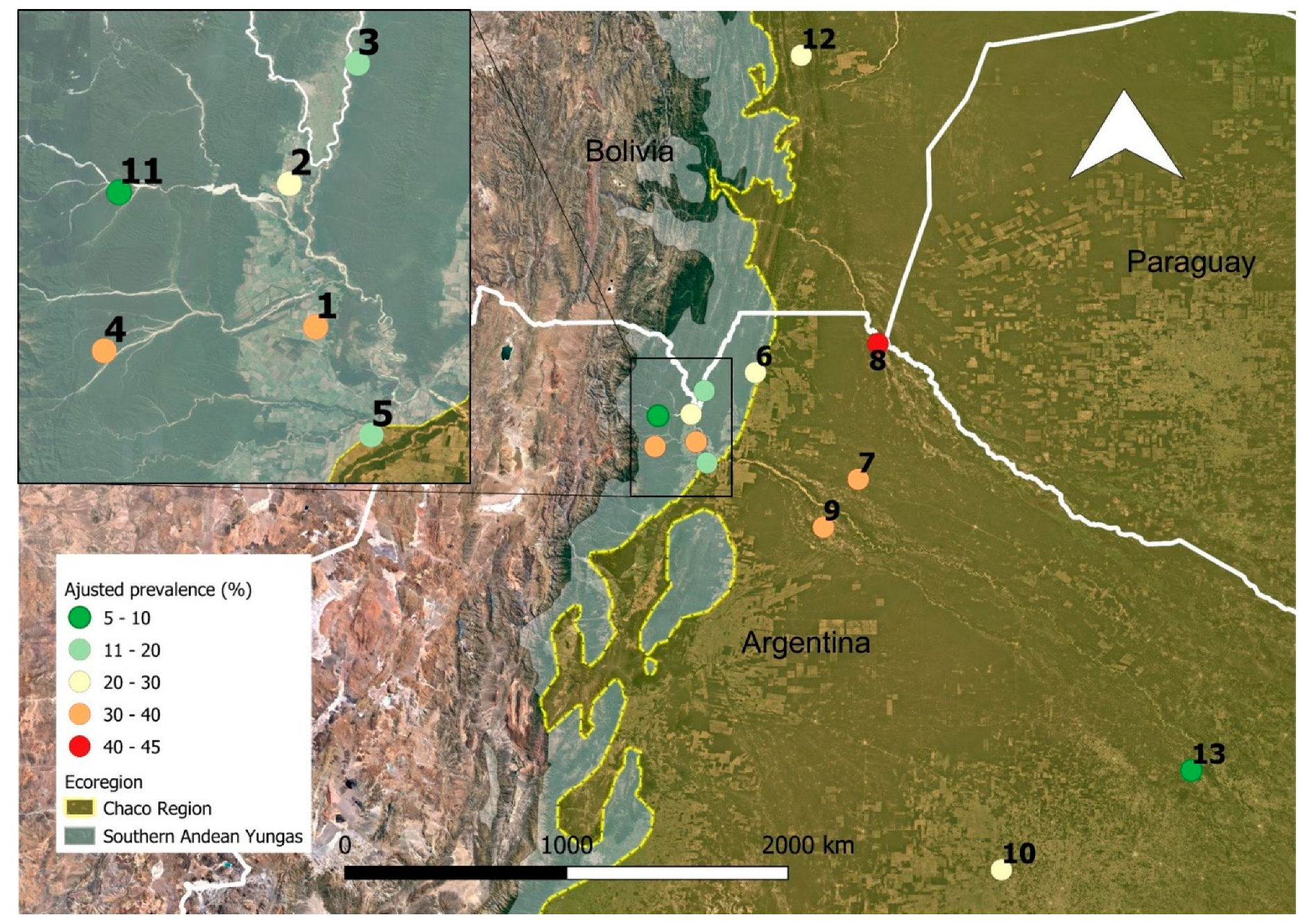
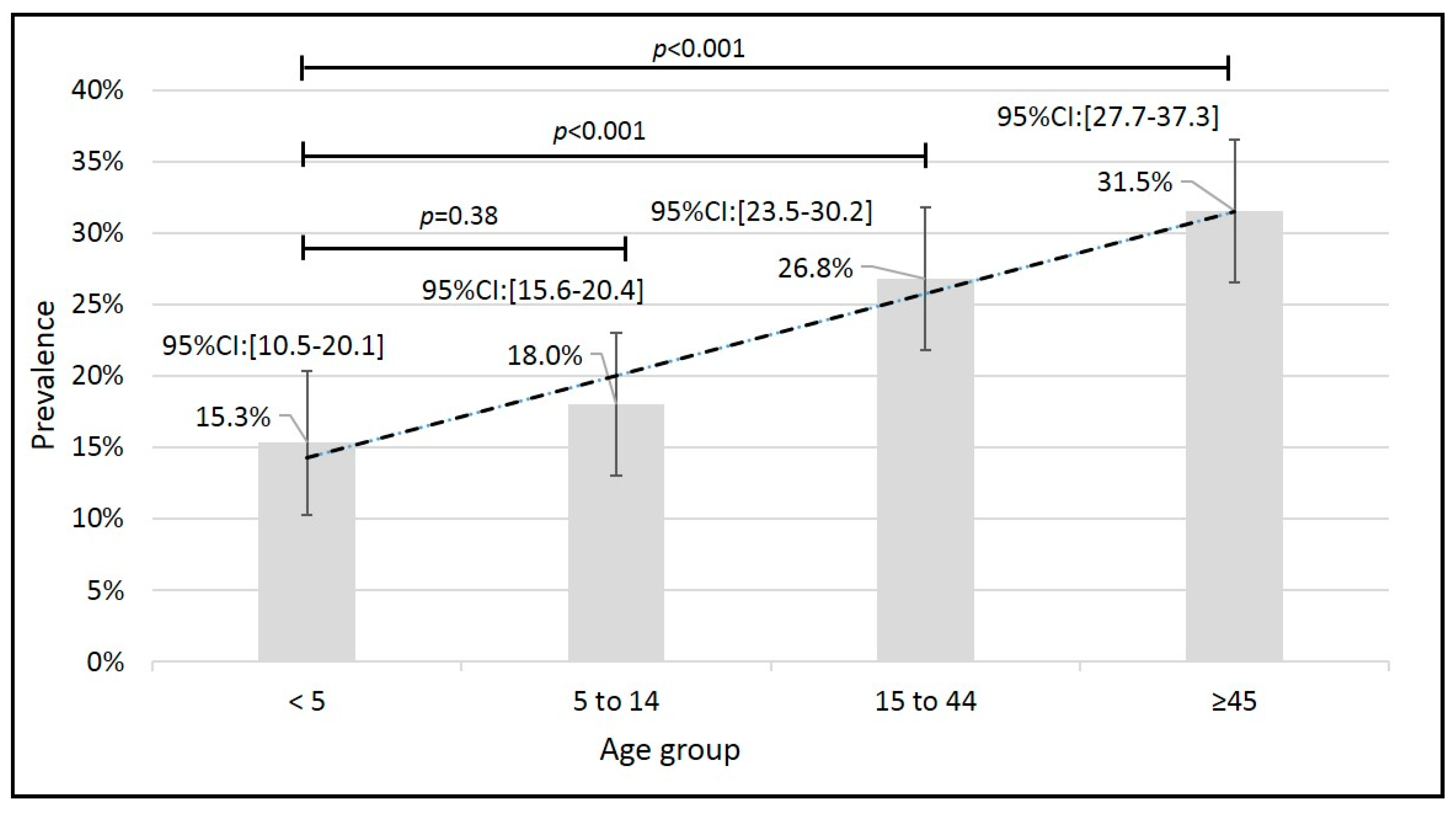
2.2. Seroprevalence Rates
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Serologic Assay
4.3. Statistical Analyses
4.4. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bisoffi, Z.; Buonfrate, D.; Montresor, A.; Requena-Méndez, A.; Muñoz, J.; Krolewiecki, A.J.; Gotuzzo, E.; Mena, M.A.; Chiodini, P.L.; Anselmi, M.; et al. Strongyloides stercoralis: A Plea for Action. PLoS Negl. Trop. Dis. 2013, 7, e2214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krolewiecki, A.; Nutman, T.B. Strongyloidiasis: A Neglected Tropical Disease. Infec. Dis. Clin. North. Am. 2019, 33, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Cimino, R.O.; Krolewiecki, A. The Epidemiology of Human Strongyloidiasis. Curr. Trop. Med. Rep. 2014, 1, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Hotez, P.J. Ten Global “Hotspots” for the Neglected Tropical Diseases. PLoS Negl. Trop. Dis. 2014, 8, e2496. [Google Scholar] [CrossRef] [PubMed]
- Del Fernández, M.; Gaspe, M.S.; Gürtler, R.E. Inequalities in the social determinants of health and Chagas disease transmission risk in indigenous and creole households in the Argentine Chaco. Parasit. vectors 2019, 12, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porcasi, X.; Catalá, S.S.; Hrellac, H.; Scavuzzo, M.C.; Gorla, D.E. Infestation of Rural Houses by Triatoma Infestans (Hemiptera: Reduviidae) in Southern Area of Gran Chaco in Argentina. J. Med. Entomol. 2006, 43, 1060–1067. [Google Scholar] [CrossRef]
- Malizia, L.R.; Pacheco, S.; Blundo, C.M.; Brown, A. Caracterización altitudinal, uso y conservación de las Yungas subtropicales de Argentina. Ecosistemas 2019, 21, 53–73. [Google Scholar]
- Socías, M.E.; Fernández, A.; Gil, J.F.; Krolewiecki, A.J. Geohelmintiasis en la Argentina una revisión sistemática. Medicina (B. Aires) 2014, 74, 29–36. [Google Scholar]
- Buonfrate, D.; Mena, M.A.; Angheben, A.; Requena-Mendez, A.; Munõz, J.; Gobbi, F.; Albonico, M.; Gotuzzo, E.; Bisoffi, Z. Prevalence of strongyloidiasis in Latin America: A systematic review of the literature. Epidemiol. Infec. 2015, 143, 452–460. [Google Scholar] [CrossRef] [Green Version]
- Rivero, M.R.; De Angelo, C.; Nuñez, P.; Salas, M.; Motta, C.E.; Chiaretta, A.; Salomón, O.D.; Liang, S. Environmental and socio-demographic individual, family and neighborhood factors associated with children intestinal parasitoses at Iguazú, in the subtropical northern border of Argentina. PLoS Negl. Trop. Dis. 2017, 11, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Cinquini, M.; Cruciani, M.; Fittipaldo, A.; Giorli, G.; Gobbi, F.; Piubelli, C.; Bisoffi, Z. Accuracy of molecular biology techniques for the diagnosis of Strongyloides stercoralis infection—A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yori, P.P.; Kosek, M.; Gilman, R.H.; Cordova, J.; Bern, C.; Chavez, C.B.; Olortegui, M.P.; Montalvan, C.; Sanchez, G.M.; Worthen, B.; et al. Seroepidemiology of strongyloidiasis in the Peruvian Amazon. Am. J. Trop. Med. Hyg. 2006, 74, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Vargas, P.; Krolewiecki, A.J.; Echazú, A.; Juarez, M.; Cajal, P.; Gil, J.F.; Caro, N.; Nasser, J.; Lammie, P.; Cimino, R.O. Serologic monitoring of public health interventions against Strongyloides stercoralis. Am. J. Trop. Med. Hyg. 2017, 97, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Echazú, A.; Bonanno, D.; Juarez, M.; Cajal, S.P.; Heredia, V.; Caropresi, S.; Cimino, R.O.; Caro, N.; Vargas, P.A.; Paredes, G.; et al. Effect of Poor Access to Water and Sanitation As Risk Factors for Soil-Transmitted Helminth Infection: Selectiveness by the Infective Route. PLoS Negl. Trop. Dis. 2015, 9, e0004111. [Google Scholar] [CrossRef]
- Forrer, A.; Khieu, V.; Vounatsou, P.; Sithithaworn, P.; Ruantip, S.; Huy, R.; Muth, S.; Odermatt, P. Strongyloides stercoralis: Spatial distribution of a highly prevalent and ubiquitous soil-transmitted helminth in Cambodia. PLoS Negl. Trop. Dis. 2019, 13, e0006943. [Google Scholar] [CrossRef] [Green Version]
- Kearns, T.M.; Currie, B.J.; Cheng, A.C.; McCarthy, J.; Carapetis, J.R.; Holt, D.C.; Page, W.; Shield, J.; Gundjirryirr, R.; Mulholland, E.; et al. Strongyloides seroprevalence before and after an ivermectin mass drug administration in a remote Australian Aboriginal community. PLoS Negl. Trop. Dis. 2017, 11, e0005607. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow Up of Strongyloidiasis: A Systematic Review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef]
- Ramanathan, R.; Burbelo, P.D.; Groot, S.; Iadarola, M.J.; Neva, F.A.; Nutman, T.B. A luciferase immunoprecipitation systems assay enhances the sensitivity and specificity of diagnosis of Strongyloides stercoralis infection. J. Infect. Dis. 2008, 198, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Rascoe, L.N.; Price, C.; Shin, S.H.; McAuliffe, I.; Priest, J.W.; Handali, S. Development of Ss-NIE-1 Recombinant Antigen Based Assays for Immunodiagnosis of Strongyloidiasis. PLoS Negl. Trop. Dis. 2015, 9, e0003694. [Google Scholar] [CrossRef] [Green Version]
- Schaffel, R.; Nucci, M.; Carvalho, E.; Braga, M.; Almeida, L.; Portugal, R.; Pulcheri, W. The value of an immunoenzymatic test (enzyme-linked immunosorbent assay) for the diagnosis of strongyloidiasis in patients immunosuppressed by hematologic malignancies. Am. J. Trop. Med. Hyg. 2001, 65, 346–350. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Formenti, F.; Perandin, F.; Bisoffi, Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clin. Microbiol. Infec. 2015, 21, 543–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Doorn, H.R.; Koelewijn, R.; Hofwegen, H.; Gilis, H.; Wetsteyn, J.C.F.M.; Wismans, P.J.; Sarfati, C.; Vervoort, T.; Van Gool, T. Use of enzyme-linked immunosorbent assay and dipstick assay for detection of Strongyloides stercoralis infection in humans. J. Clin. Microbiol. 2007, 45, 438–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krolewiecki, A.J.; Ramanathan, R.; Fink, V.; McAuliffe, I.; Cajal, S.P.; Won, K.; Juarez, M.; Di Paolo, A.; Tapia, L.; Acosta, N.; et al. Improved diagnosis of Strongyloides stercoralis using recombinant antigen-based serologies in a community-wide study in northern Argentina. Clin. Vaccine Immunol. 2010, 17, 1624–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravi, V.; Ramachandran, S.; Thompson, R.W.; Andersen, J.F.; Neva, F. A Characterization of a recombinant immunodiagnostic antigen (NIE) from Strongyloides stercoralis L3-stage larvae. Mol. Biochem. Parasitol. 2002, 125, 73–81. [Google Scholar] [CrossRef]
- Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Degani, M.; Tais, S.; Angheben, A.; Requena-Mendez, A.; et al. Accuracy of Five Serologic Tests for the Follow up of Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2015, 9. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.W.; Klein, D.M.; Dornink, S.M.; Jespersen, D.J.; Kubofcik, J.; Nutman, T.B.; Merrigan, S.D.; Couturier, M.R.; Theel, E.S. Comparison of three immunoassays for detection of antibodies to Strongyloides stercoralis. Clin. Vaccine Immunol. 2014, 21, 732–736. [Google Scholar] [CrossRef] [Green Version]
- Krolewiecki, A.J.; Koukounari, A.; Romano, M.; Caro, N.N.; Scott, A.L.; Fleitas, P.; Cimino, R.; Shiff, C.J. Transrenal DNA-based diagnosis of Strongyloides stercoralis (Grassi, 1879) infection: Bayesian latent class modeling of test accuracy. PLoS Negl. Trop. Dis. 2018, 12, e0006550. [Google Scholar] [CrossRef]
- Hafiznur Yunus, M.; Arifin, N.; Balachandra, D.; Anuar, N.S.; Noordin, R. Lateral Flow Dipstick Test for Serodiagnosis of Strongyloidiasis. Am. J. Trop. Med. Hyg. 2019, 101, 432–435. [Google Scholar] [CrossRef]
- Steinmann, P.; Zhou, X.-N.; Du, Z.-W.; Jiang, J.-Y.; Wang, L.-B.; Wang, X.-Z.; Li, L.-H.; Marti, H.; Utzinger, J. Occurrence of Strongyloides stercoralis in Yunnan Province, China, and Comparison of Diagnostic Methods. PLoS Negl. Trop. Dis. 2007, 1, e75. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Perandin, F.; Formenti, F.; Bisoffi, Z. A retrospective study comparing agar plate culture, indirect immunofluorescence and real-time PCR for the diagnosis of Strongyloides stercoralis infection. Parasitology 2017, 144, 812–816. [Google Scholar] [CrossRef]
- Echazú, A.; Juarez, M.; Vargas, P.A.; Cajal, S.P.; Cimino, R.O.; Heredia, V.; Caropresi, S.; Paredes, G.; Arias, L.M.; Abril, M.; et al. Albendazole and ivermectin for the control of soil-transmitted helminths in an area with high prevalence of Strongyloides stercoralis and hookworm in northwestern Argentina: A community-based pragmatic study. PLoS Negl. Trop. Dis. 2017, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lammie, P.J.; Moss, D.M.; Brook Goodhew, E.; Hamlin, K.; Krolewiecki, A.; West, S.K.; Priest, J.W. Development of a new platform for neglected tropical disease surveillance. Int. J. Parasitol. 2012, 42, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic accuracy of five serologic tests for Strongyloides stercoralis infection. PLoS Negl. Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gétaz, L.; Castro, R.; Zamora, P.; Kramer, M.; Gareca, N.; del Torrico-Espinoza, M.; Macias, J.; Lisarazu-Velásquez, S.; Rodriguez, G.; Valencia-Rivero, C.; et al. Epidemiology of Strongyloides stercoralis infection in Bolivian patients at high risk of complications. PLoS Negl. Trop. Dis. 2019, 13, e0007028. [Google Scholar] [CrossRef]
- Taranto, N.J.; Cajal, S.P.; De Marzi, M.C.; Fernández, M.M.; Frank, F.M.; Brú, A.M.; Minvielle, M.C.; Basualdo, J.A.; Malchiodi, E.L. Clinical status and parasitic infection in a Wichí Aboriginal community in Salta, Argentina. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 554–558. [Google Scholar] [CrossRef]
- Menghi, C.I.; Iuvaro, F.R.; Dellacasa, M.A.; Gatta, C.L. Survey of intestinal parasites among an aboriginal community in Salta. Medicina (B. Aires) 2007, 67, 705–708. [Google Scholar]
- Cancrini, G.; Bartoloni, A.; Paradisi, F.; Nunez, L.E. Parasitological observations on three Bolivian localities including rural communities, cities and institutions. Ann. Trop. Med. Parasit. 1989, 83, 591–594. [Google Scholar] [CrossRef]
- Taranto, N.J.; Bonomi de Filippi, H.; Orione, O. [Prevalence of Strongyloides stercoralis infection in childhood. Orán, Salta, Argentina]. Bol. Chil. Parasitol. 1993, 48, 49–51. [Google Scholar]
- Machicado, J.D.; Marcos, L.A.; Tello, R.; Canales, M.; Terashima, A.; Gotuzzo, E. Diagnosis of soil-transmitted helminthiasis in an Amazonic community of Peru using multiple diagnostic techniques. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 333–339. [Google Scholar] [CrossRef]
- Diep, N.T.N.; Thai, P.Q.; Trang, N.N.M.; Jäger, J.; Fox, A.; Horby, P.; Phuong, H.V.M.; Anh, D.D.; Mai, L.T.Q.; Van Doorn, H.R.; et al. Strongyloides stercoralis seroprevalence in Vietnam. Epidemiol. Infec. 2017, 145, 3214–3218. [Google Scholar] [CrossRef] [Green Version]
- Forrer, A.; Khieu, V.; Schindler, C.; Schär, F.; Marti, H.; Char, M.C.; Muth, S.; Odermatt, P. Ivermectin Treatment and Sanitation Effectively Reduce Strongyloides stercoralis Infection Risk in Rural Communities in Cambodia. PLoS Negl. Trop. Dis. 2016, 10, e0004909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khieu, V.; Schär, F.; Marti, H.; Bless, P.J.; Char, M.C.; Muth, S.; Odermatt, P. Prevalence and risk factors of Strongyloides stercoralis in Takeo Province, Cambodia. Parasit. Vectors 2014, 7, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, A.M.; Clark, E.H.; Galdos-Cardenas, G.; Wiegand, R.E.; Ferrufino, L.; Menacho, S.; Gil, J.; Spicer, J.; Budde, J.; Levy, M.Z.; et al. Epidemiology of and Impact of Insecticide Spraying on Chagas Disease in Communities in the Bolivian Chaco. PLoS Negl. Trop. Dis. 2013, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinicci, M.; Macchioni, F.; Mantella, A.; Gabrielli, S.; Roselli, M.; Rojo Mayaregua, D.; Monasterio Pinckert, J.; Gamboa Barahona, H.; Paredes, G.A.; Halkyer, P.; et al. Seroepidemiological trend of strongyloidiasis in the Bolivian Chaco (1987-2013) in the absence of disease-specific control measures. Trop. Med. Int. Health 2017, 22, 1457–1462. [Google Scholar] [CrossRef] [PubMed]
- Schär, F.; Inpankaew, T.; Traub, R.J.; Khieu, V.; Dalsgaard, A.; Chimnoi, W.; Chamnan, C.; Sok, D.; Marti, H.; Muth, S.; et al. The prevalence and diversity of intestinal parasitic infections in humans and domestic animals in a rural Cambodian village. Parasitol. Int. 2014, 63, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Khieu, V.; Hattendorf, J.; Schär, F.; Marti, H.; Char, M.C.; Muth, S.; Odermatt, P. Strongyloides stercoralis infection and re-infection in a cohort of children in Cambodia. Parasitol. Int. 2014, 63, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Monje-Rumi, M.; Brandán, C.P.; Ragone, P.G.; Tomasini, N.; Lauthier, J.J.; Alberti D’Amato, A.M.; Cimino, R.O.; Orellana, V.; Basombrío, M.A.; Diosque, P. Trypanosoma cruzi diversity in the Gran Chaco: Mixed infections and differential host distribution of TcV and TcVI. Infec. Genet. Evol. 2015, 29, 53–59. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Localities | Department | Province | Country | Altitude (masl) | Region | Community |
|---|---|---|---|---|---|---|
| SRN Orán | Oran (1) | Salta | Argentina | 356m | Yunga | Periurban |
| Pichanal | Chaco | Urban | ||||
| Solazuty | Yunga | Rural | ||||
| Río Blanquito | 773 m | |||||
| Isla de Cañas | Iruya (1) | 610 m | ||||
| Tartagal | General San Martín (1) | 495m | Chaco | Periurban-Rural | ||
| Medialuna | Yunga | Rural | ||||
| La Unión | Rivadavia (1) | 227 m | Chaco | |||
| Coronel Juan Solá (Morillo) | 300 m | Urban-Rural | ||||
| Santa Victoria Este | 262 m | Rural | ||||
| Pampa del Indio | Libertador Gral San Martin | Chaco | 96 m | Chaco | ||
| Las Leonas | 12 de Octubre | 124 m | ||||
| Gutierrez | Cordillera | Santa Cruz | Bolivia | 800 m | Chaco |
| Localities | Samples | Year of Study | Basic Sampling Unit | Population | Unimproved Water Supply | Unimproved Sanitation | Cited in |
|---|---|---|---|---|---|---|---|
| SRN Orán | 142 | 2011 | Household | Community | 0% | 0% | [14] |
| Pichanal | 489 | 2013 | Household | Community | 0% | 0% | [13] |
| Solazuty | 182 | 2010 | Household | Community | 100% | 100% | [14] |
| Río Blanquito | 26 | 2010 | Individuals | Community | 100% | 100% | None |
| Isla de Cañas | 36 | 2011 | Individual | Community | 100% | 100% | None |
| Tartagal | 407 | 2012–2013 | Household | Community | 1% | 82% | [31] |
| Medialuna | 104 | 2016 | Individual | Community | 100% | 100% | [27] |
| La Unión | 128 | 2016 | Individual | Community | 6% | 100% | None |
| Coronel Juan Solá (Morillo) | 189 | 2016 | Individual | Community | 86% | 100% | None |
| Santa Victoria Este | 152 | 2016 | Individual | Community | 100% | 100% | None |
| Pampa del Indio | 585 | 2014 | Individual | Community | 100% | 100% | None |
| Las Leonas | 76 | 2008 | Household | Community | 100% | 100% | [47] |
| Gutierrez | 287 | 2011–2012 | Household | Community | 100% | 100% | [43] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimino, R.O.; Fleitas, P.; Fernández, M.; Echazú, A.; Juarez, M.; Floridia-Yapur, N.; Cajal, P.; Seijo, A.; Abril, M.; Weinberg, D.; et al. Seroprevalence of the Strongyloides stercoralis Infection in Humans from Yungas Rainforest and Gran Chaco Region from Argentina and Bolivia. Pathogens 2020, 9, 394. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9050394
Cimino RO, Fleitas P, Fernández M, Echazú A, Juarez M, Floridia-Yapur N, Cajal P, Seijo A, Abril M, Weinberg D, et al. Seroprevalence of the Strongyloides stercoralis Infection in Humans from Yungas Rainforest and Gran Chaco Region from Argentina and Bolivia. Pathogens. 2020; 9(5):394. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9050394
Chicago/Turabian StyleCimino, Rubén O., Pedro Fleitas, Mariana Fernández, Adriana Echazú, Marisa Juarez, Noelia Floridia-Yapur, Pamela Cajal, Alfredo Seijo, Marcelo Abril, Diego Weinberg, and et al. 2020. "Seroprevalence of the Strongyloides stercoralis Infection in Humans from Yungas Rainforest and Gran Chaco Region from Argentina and Bolivia" Pathogens 9, no. 5: 394. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9050394