
Safe and Effective Treatment of Intracranial Infantile Hemangiomas with Beta-Blockers


Oxford Eye Hospital, Oxford University Hospitals NHS Foundation Trust, Headley Way, Headington, Oxford OX3 9DU, UK
*
Author to whom correspondence should be addressed.
Pediatr. Rep. 2021, 13(3), 347-356; https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13030043
Submission received: 7 March 2021
/
Revised: 7 June 2021
/
Accepted: 29 June 2021
/
Published: 1 July 2021
Abstract
:Infantile hemangiomas are common benign vascular tumors but are rarely found in an intracranial location. Our literature review identified 41 reported cases. There is no general consensus on management of these rare lesions and until recently, treatment was limited to surgery or pharmacological management with steroids or interferon. Although beta-blockers have been widely prescribed in the treatment of cutaneous infantile hemangiomas since 2008, their use in the treatment of intracranial infantile hemangiomas has been minimal. We present a case of infantile hemangioma affecting the right orbit, associated with intracranial extension, causing intermittent right facial nerve palsy. The patient achieved an excellent outcome following combined treatment with oral propranolol and topical timolol maleate 0.5%, with complete regression of the lesion by 4 months. We conclude that beta-blockers are a safe and effective treatment of intracranial infantile hemangiomas and can be employed as first-line management of these lesions.
1. Introduction
Infantile hemangiomas are common benign vascular tumors, occurring at birth or early infancy, with an estimated incidence of 1–5% [1]. Risk factors for development of infantile hemangioma include Caucasian ethnicity, low birth weight, and female sex (female to male ratio of 2.4:1) [2,3]. They can occur in any organ system but have a predilection for the skin and soft tissues of the head and neck. Intracranial infantile hemangiomas, however, are very rare entities.
Although histologically benign, infantile hemangiomas have a capability for rapid growth. They are characterized by a rapid proliferative phase occurring in the first year of life [4,5]. Most hemangioma growth occurs in the first 5 months, at which point 80% of the final size has often been reached, typically reaching maximal size by nine months [4]. This is followed by a gradual involutional phase, whereby 90% of lesions have spontaneously involuted by five years of age [4,5]. Treatment is therefore not required for most lesions. However, rapid intracranial growth may cause severe neurological complications and thus often requires intervention.
This report was reviewed by the Oxford University Hospitals’ ethics team and formal ethical approval was deemed not to be required. We performed a literature review using Pubmed, searching for keywords “intracranial infantile hemangioma/s”, and identified 41 reported cases (Table 1) [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. There was no uniform treatment approach observed. In some cases of small asymptomatic lesions, watchful waiting was indicated. Some patients were treated surgically [9,12,14,17,19,22,24,26,27]. Others received pharmacological therapy with oral prednisolone [7,10,15,23,25], intralesional triamcinolone [15] interferon alpha [7,25], or thalidomide [11]. Efficacy of these treatments was variable, and in some cases significant side effects were encountered. In 2014, the first cases of successful treatment with propranolol were reported [6].
We present a further case of intracranial infantile hemangioma, where an excellent outcome was achieved with combined topical and systemic beta-blocker treatment for 1 year, with no complications observed and no recurrence following cessation of treatment.
2. Case Report
An 8-week-old female infant presented to the Pediatric Ophthalmology clinic with an expanding raised, deep red vascular lesion over the right temporal area which had been present since birth. A few weeks after birth, she developed right proptosis, which continued to progress over the following weeks until review. The proptosis was variable and worse with crying. During this time, her parents also noticed an intermittent right facial nerve palsy with noticeable right facial weakness and an inability to furrow her right brow. She had no past medical history. She was born at 36 + 6 weeks gestation weighing 2.21 kg, following an uncomplicated twin pregnancy.
On examination, there was a large segmental plaque capillary hemangioma overlying her right temporal area, which was easily compressible. The right eye showed marked proptosis with inability to close the eyelids completely (Figure 1). There was a secondary abduction deficit and right hypoglobus. There was no papilledema on fundal examination. Cycloplegic refraction revealed significant astigmatism in the right eye (+6.00/−3.00 × 40 OD, +5.00 DS OS) as a presumed mass effect of the orbital lesion. Urgent same day MRI imaging was arranged which showed an extensive intra- and extraconal lesion within the right orbit (Figure 2). The lesion was located predominantly within the superolateral compartment of the orbit, extending medially and posteriorly to the level of the optic foramen. The T2-weighted sequence showed that the lesion extended intracranially through the superior orbital fissure, with involvement of right Meckel’s cave and the cerebellopontine angle. The lesion was hyperintense on T2 weighting and relatively isointense on T1 weighting (Figure 2). These characteristics were identical to the cutaneous lesion overlying the right frontal bone. Overall, findings were most consistent with a diagnosis of infantile hemangioma. Due to the segmental plaque presentation and intracranial location, the infant was investigated for PHACE syndrome, but no other clinical or radiological features were found.
After consultation with the Neurology and Dermatology teams, she was commenced on combined topical and systemic beta-blocker treatment. Topical timolol maleate 0.5% (3 drops three times daily) painted onto the periocular area was started in view of the risk of amblyopia. Admission was arranged for commencement of oral propranolol 1 mg/kg in two divided doses. ECG was performed and was normal. Monitoring with regular pulse rate and blood pressure was performed at baseline and at 1 h and 2 h after treatment initiation. These parameters remained within normal limits. Propranolol was well tolerated, and the dose was increased to 2 mg/kg in the second week. Hypoglycemia may be the most common serious complication in children treated with propranolol for IH [32]. The patient’s parents were counselled to ensure a minimum of 6 h between doses, to recognise the symptoms of hypoglycemia, hypotension or bradycardia. The parents were also instructed to ensure that the patient was fed regularly and to avoid prolonged fasts. Infants <6 weeks should be fed at least every 4 h, between 6 weeks and 4 months of age should be fed at least every 5 h, and >4 months of age should be fed at least 6 to 8 h. They were also advised to discontinue propranolol and topical timolol during intercurrent illness, especially in the setting of restricted oral intake.
Occlusion therapy to the left eye was commenced to treat early right amblyopia secondary to anisometropia. Lubricants were prescribed to prevent exposure keratopathy.
A review was arranged nine days after commencement of treatment, at which point the proptosis had started to improve. Three weeks later, the proptosis had reduced significantly, with a marked improvement in the position of the globe and the extraocular movements. At four months of follow-up, the proptosis had completely resolved (Figure 3) and the eye movements were now full. The right temporal skin plaque was now flat and pale. Topical timolol was discontinued at this point, as the vision appeared equal with no evidence of amblyopia. MRI head with gadolinium confirmed total resolution of the right proptosis with no evidence of any residual disease within the orbit (Figure 4). There was also total resolution of the intracranial component of the hemangioma. MRI angiogram confirmed normal appearances of the anterior and posterior cerebral circulation, with no evidence suggestive of PHACE syndrome.
Oral propranolol was continued to complete a 12-month course. No recurrence was observed following treatment cessation.
3. Discussion
We identified 41 cases of reported intracranial infantile hemangioma in the literature (Table 1) [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. The majority of patients were female (68%). Mean age at presentation was 3.7 months (range 0–36 months). Most cases tend to occur in association with periorbital hemangiomas, PHACE syndrome, or diffuse neonatal hemangiomatosis. Presenting symptoms were diverse. Over half of patients had no neurological or neuro-ophthalmological signs or symptoms, and their lesions were identified incidentally on imaging of an extracranial lesion. We therefore hypothesize that the true incidence may be underreported. The 20 patients (49%) who did have neurological signs or symptoms had a range of presentations, including seizures, ataxia, central hypotonia, hydrocephalus, enlarged head circumference, and cranial nerve palsy. One patient suffered an arterial ischemic stroke [13]. One infant died following a subarachnoid hemorrhage at the age of 6 weeks [18]
Due to their rarity, there is currently no consensus on the optimal, evidence-based treatment of intracranial infantile hemangiomas. We found that some small asymptomatic lesions were managed with observation alone [13,20,21,23,31], and the hemangiomas spontaneously regressed in some cases [23,31]. Ten patients underwent surgical treatment [9,12,14,17,19,22,24,26,27,30]. In many cases, urgent surgery was necessitated by signs of raised intracranial pressure, or where the preoperative diagnosis was unclear and a more sinister process had been suspected. Surgical resection is associated with a high risk of hemorrhagic complications due to the extensive vascularity of hemangiomas, and alternative treatment options should be considered where possible.
Steroids were the most commonly prescribed pharmacological therapy, with oral prednisolone being the mainstay of treatment [7,10,15,23,25]. Infantile hemangiomas have a variable response to steroid therapy, with one retrospective study reporting regression in one-third, stabilization of growth in another third, and minimal to no response in the final third of lesions located in any organ system [33]. Adverse effects are common, and include irritability, sleep disturbance, adrenal suppression, immunosuppression, hypertension, bone demineralization, and growth retardation [29]. In two cases, intralesional triamcinolone was administered [15], which achieved a reduction in lesion size.
Interferon alpha is an inhibitor of angiogenesis, administered as a daily subcutaneous injection, and has also been used successfully for the treatment of infantile hemangioma [34]. Interferon alpha was used in four patients in our review [7,25], either as primary treatment or following failed corticosteroid therapy. All cases reported a clinical response with reduction in hemangioma size. However, interferon treatment is associated with the risk of significant side effects. Transient neutropenia and liver enzyme abnormalities may develop. Spastic diplegia, irreversible in some cases, has been reported. Consequently, its use is not routinely recommended.
Frei-Jones et al. reported successful treatment of a large unresectable intracranial hemangioma with thalidomide [11]. Treatment did not appear to arrest growth of the lesion initially—despite commencing thalidomide at 35 days of age, its size had increased to 307% of its presenting size at 5 months of age.
In 2008, Léauté-Labrèze et al. described their serendipitous observation that oral propranolol [35], a nonselective blocker of β-adrenergic receptors, was effective and well tolerated in the management of infantile hemangiomas. The mechanism of action likely involves several processes, including vasoconstriction, inhibition of angiogenesis, and stimulation of apoptosis [36,37]. Since then, propranolol has become an increasingly popular treatment for cutaneous infantile hemangiomas, as it is considered to have a better adverse effect profile compared to other systemic therapies. The most commonly reported adverse effects were sleep disturbance and coolness of the distal extremities [38]. Cardiac side effects including bradycardia and hypotension may be encountered; however both are generally asymptomatic and do not require intervention [38]. Less commonly, propranolol can induce hypoglycemia [32]. The risk of this can be minimized by concurrent administration with feedings and withholding doses if oral intake is compromised.
Five cases of intracranial infantile hemangioma successfully treated with oral propranolol have been reported since then. In four cases, there was complete resolution of the intracranial hemangioma [6,8,16], and there was a reduction in lesion size in the final case [28]. No adverse effects were encountered.
We present a rare case of a capillary hemangioma with intracranial and orbital locations, causing a right facial nerve palsy. The patient achieved an excellent outcome following combined treatment with oral propranolol and topical timolol maleate 0.5%, with complete regression of the lesion within 4 months. The patient did not develop any further neurological or neuro-ophthalmic complications, and her amblyopia resolved. Due to their rarity, large scale studies to confirm treatment efficiacy for intracranial infantile hemangiomas are difficult to perform. Our case adds to the small body of evidence that beta blockers are a safe and effective treatment of intracranial infantile hemangiomas and can be employed as first-line management of these lesions.
4. Conclusions
Intracranial infantile hemangiomas are rare entities, with varied reported management strategies. This case and review add to the growing body of evidence that beta-blockers are a safe and effective treatment of intracranial infantile hemangiomas and can be employed as first-line management.
Author Contributions
A.N. conceptualized the case report, performed the literature review, and drafted and revised the manuscript. A.Y.O. performed the literature review and revised the manuscript. G.D.H. conceptualised the case report, acquired relevant clinical data relating to the case, supervised the progress of the paper, and critically reviewed and revised the manuscript for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This work was reviewed by the Joint Research Office study classification group and ethical review was deemed unnecessary.
Informed Consent Statement
Informed consent was obtained from the subject’s parents.
Acknowledgments
We thank Robin Joseph for his contribution towards analysis of the MRI imaging that related to the case.
Conflicts of Interest
The authors report no conflict of interest.
Further Information
The case was presented as a poster at the European Paediatric Ophthalmological Society (EPOS) Annual Meeting 2019, Riga.
References
- Kilcline, C.; Frieden, I.J. Infantile Hemangiomas: How Common Are They? A Systematic Review of the Medical Literature. Pediatr. Dermatol. 2008, 25, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Haggstrom, A.N.; Drolet, B.A.; Baselga, E.; Chamlin, S.L.; Garzon, M.C.; Horii, K.A.; Lucky, A.W.; Mancini, A.J.; Metry, D.W.; Newell, B.; et al. Prospective Study of Infantile Hemangiomas: Demographic, Prenatal, and Perinatal Characteristics. J. Pediatr. 2007, 150, 291–294. [Google Scholar] [CrossRef]
- Drolet, B.A.; Swanson, E.A.; Frieden, I.J. Infantile Hemangiomas: An Emerging Health Issue Linked to an Increased Rate of Low Birth Weight Infants. J. Pediatr. 2008, 153, 712–715.e1. [Google Scholar] [CrossRef] [PubMed]
- Holland, K.E.; Drolet, B.A. Infantile Hemangioma. Pediatr. Clin. N. Am. 2010, 57, 1069–1083. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Haggstrom, A.N.; Drolet, B.A.; Baselga, E.; Chamlin, S.L.; Garzon, M.C.; Horii, K.A.; Lucky, A.W.; Mancini, A.J.; Metry, D.W.; et al. Growth Characteristics of Infantile Hemangiomas: Implications for Management. Pediatrics 2008, 122, 360–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonov, N.K.; Spence-Shishido, A.; Marathe, K.S.; Tlougan, B.; Kazim, M.; Sultan, S.; Hess, C.P.; Morel, K.D.; Frieden, I.J.; Garzon, M.C. Orbital Hemangioma with Intracranial Vascular Anomalies and Hemangiomas: A New Presentation of PHACE Syndrome? Pediatr. Dermatol. 2015, 32, e267–e272. [Google Scholar] [CrossRef]
- Bar-Sever, Z.; Horev, G.; Lubin, E.; Kornreich, L.; Naor, N.; Ziv, N.; Shimoni, A.; Grunebaum, M. A rare coexistence of a multicentric hepatic hemangioendothelioma with a large brain hemangioma in a preterm infant. Pediatr. Radiol. 1994, 24, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, S.; Campos, H.G.D.A.; da Costa, M.D.S. A case of giant fetal intracranial capillary hemangioma cured with propranolol. J. Neurosurg. Pediatr. 2016, 17, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Daenekindt, T.; Weyns, F.; Kho, K.H.; Peuskens, D.; Engelborghs, K.; Wuyts, J. Giant intracranial capillary hemangioma associated with enlarged head circumference in a newborn. J. Neurosurg. Pediatr. 2008, 1, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Ersoy, S.; Mancini, A.J. Hemifacial infantile hemangioma with intracranial extension: A rare entity. Pediatr Dermatol. 2005, 22, 309–313. [Google Scholar] [CrossRef]
- Frei-Jones, M.; McKinstry, R.C.; Perry, A.; Leonard, J.R.; Park, T.S.; Rubin, J.B. Use of thalidomide to diminish growth velocity in a life-threatening congenital intracranial hemangioma. J. Neurosurg. Pediatr. 2008, 2, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haine, E.; Sevely, A.; Boetto, S.; Delisle, M.-B.; Cances, C. Infantile Hemangioma of the Posterior Fossa in a Newborn: Early Management and Long-Term Follow-up. Neuropediatrics 2017, 48, 378–381. [Google Scholar] [CrossRef]
- Heyer, G.L.; Garzon, M.C. An Infant with a Facial Hemangioma and More. Semin. Pediatr. Neurol. 2008, 15, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Jalloh, I.; Dean, A.F.; O’Donovan, D.G.; Cross, J.; Garnett, M.R.; Santarius, T. Giant intracranial hemangioma in a neonate. Acta Neurochir. 2014, 156, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Judd, C.; Chapman, P.; Koch, B.; Shea, C. Intracranial Infantile Hemangiomas Associated With PHACE Syndrome. Am. J. Neuroradiol. 2007, 28, 25–29. [Google Scholar] [PubMed]
- Kang, E.; Friedman, N.; Mamoun, I.; Tamburro, J.; Golden, A. Beta Blockade as Treatment for Intracranial Infantile Hemangioma: Case Report and Literature Review. Pediatr. Neurol. 2016, 59, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Karikari, I.O.; Selznick, L.A.; Cummings, T.J.; George, T.M. Capillary hemangioma of the fourth ventricle in an infant. J. Neurosurgery: Pediatr. 2006, 104, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Le Bihannic, A.; Michot, C.; Heckly, A.; Loget, P.; Beucher, A.; Brassier, G.; Hamlat, A. Capillary haemangioma arising from the anterior choroidal artery. Childs Nerv Syst. 2005, 21, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Philpott, C.; Wray, A.; MacGregor, D.; Coleman, L. Dural Infantile Hemangioma Masquerading as a Skull Vault Lesion. Am. J. Neuroradiol. 2011, 33, E85–E87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poetke, M.; Frommeld, T.; Berlien, H.P. PHACE Syndrome: New Views on Diagnostic Criteria. Eur. J. Pediatr. Surg. 2002, 12, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Poindexter, G.; Metry, D.W.; Barkovich, A.J.; Frieden, I.J. PHACE Syndrome with Intracerebral Hemangiomas, Heterotopia, and Endocrine Dysfunction. Pediatr. Neurol. 2007, 36, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.M.; Shakir, H.J.; McBride, P. Dural-based infantile hemangioma of the posterior fossa: Case report. Surg. Neurol. Int. 2016, 7, 52. [Google Scholar] [CrossRef] [Green Version]
- Tortori-Donati, P.; Fondelli, M.P.; Rossi, A.; Bava, G.L. Intracranial contrast-enhancing masses in infants with capillary haemangioma of the head and neck: Intracranial capillary haemangioma? Neuroradiology 1999, 41, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Uyama, A.; Kawamura, A.; Akiyama, H.; Nakamizo, S.; Yamamoto, K.; Nagashima, T.; Uetani, T.; Takeda, H.; Yoshida, M. A Case of Cerebellar Capillary Hemangioma with Multiple Cysts. Pediatr. Neurosurg. 2008, 44, 344–349. [Google Scholar] [CrossRef]
- Viswanathan, V.; Smith, E.; Mulliken, J.; Fishman, S.; Kozakewich, H.; Burrows, P.; Orbach, D. Infantile Hemangiomas Involving the Neuraxis: Clinical and Imaging Findings. Am. J. Neuroradiol. 2009, 30, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Willing, S.J.; Faye-Petersen, O.; Aronin, P.; Faith, S. Radiologic-pathologic correlation. Capillary hemangioma of the meninges. Am. J. Neuroradiol. 1993, 14, 529–536. [Google Scholar] [PubMed]
- Zheng, S.-P.; Ju, Y.; You, C. Giant intracranial capillary hemangioma in a 3-year-old child: Case report and literature review. Clin. Neurol. Neurosurg. 2012, 114, 1270–1273. [Google Scholar] [CrossRef] [PubMed]
- Benvenisti, H.; Ben-Sira, L.; Constantini, S.; Roth, J. Giant cranial and cerebellar hemangioma treated with propranolol. Child’s Nerv. Syst. 2014, 31, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Dalsin, M.; Silva, R.S.; Chaves, J.P.G.; Oliveira, F.H.; Antunes, Á.C.M.; Vedolin, L.M. Intracranial extra-axial hemangioma in a newborn: A case report and literature review. Surg. Neurol. Int. 2016, 7, 314–316. [Google Scholar] [CrossRef] [Green Version]
- El Rassi, E.; MacArthur, C.J. Propranolol-responsive cranial nerve palsies in a patient with PHACES syndrome. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1778–1781. [Google Scholar] [CrossRef] [PubMed]
- Friedland, R.; Ben Amitai, D.; Zvulunov, A. Screening for Brain Involvement in Infants with Multifocal Cutaneous Infantile Hemangiomas. Dermatology 2017, 233, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Holland, K.E.; Frieden, I.J.; Frommelt, P.C.; Mancini, A.J.; Wyatt, D.; Drolet, B.A. Hypoglycemia in Children Taking Propranolol for the Treatment of Infantile Hemangioma. Arch. Dermatol. 2010, 146, 775–778. [Google Scholar] [CrossRef] [Green Version]
- Enjolras, O.; Riche, M.C.; Merland, J.J.; Escande, J.P. Management of alarming hemangiomas in infancy: A review of 25 cases. Pediatrics 1990, 85, 491–498. [Google Scholar]
- Barrio, V.R.; Drolet, B.A. Treatment of hemangiomas of infancy. Dermatol. Ther. 2005, 18, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Léauté-Labrèze, C.; De La Roque, E.D.; Hubiche, T.; Boralevi, F.; Thambo, J.B.; Taïeb, A. Propranolol for severe hemangiomas of infancy. N. Engl. J. Med. 2008, 358, 2649–2651. [Google Scholar] [CrossRef] [PubMed]
- Painter, S.L.; Hildebrand, G.D. Review of topical beta blockers as treatment for infantile hemangiomas. Surv. Ophthalmol. 2016, 61, 51–58. [Google Scholar] [CrossRef]
- Sipkova, Z.; Xue, K.; Mudhar, H.S.; Wagner, B.; Hildebrand, G.D. Early and Late Histological and Ultrastructural Findings in Resected Infantile Capillary Hemangiomas Following Treatment with Topical Beta-Blocker Timolol Maleate 0.5%. Ocul. Oncol. Pathol. 2017, 4, 100–106. [Google Scholar] [CrossRef]
- Marqueling, A.L.; Oza, V.; Frieden, I.J.; Puttgen, K.B. Propranolol and Infantile Hemangiomas Four Years Later: A Systematic Review. Pediatr. Dermatol. 2013, 30, 182–191. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Infant on presentation. Large segmental plaque capillary hemangioma overlying the right temporal area. Marked proptosis with mild lagophthalmos.
Figure 1.
Infant on presentation. Large segmental plaque capillary hemangioma overlying the right temporal area. Marked proptosis with mild lagophthalmos.

Figure 2.
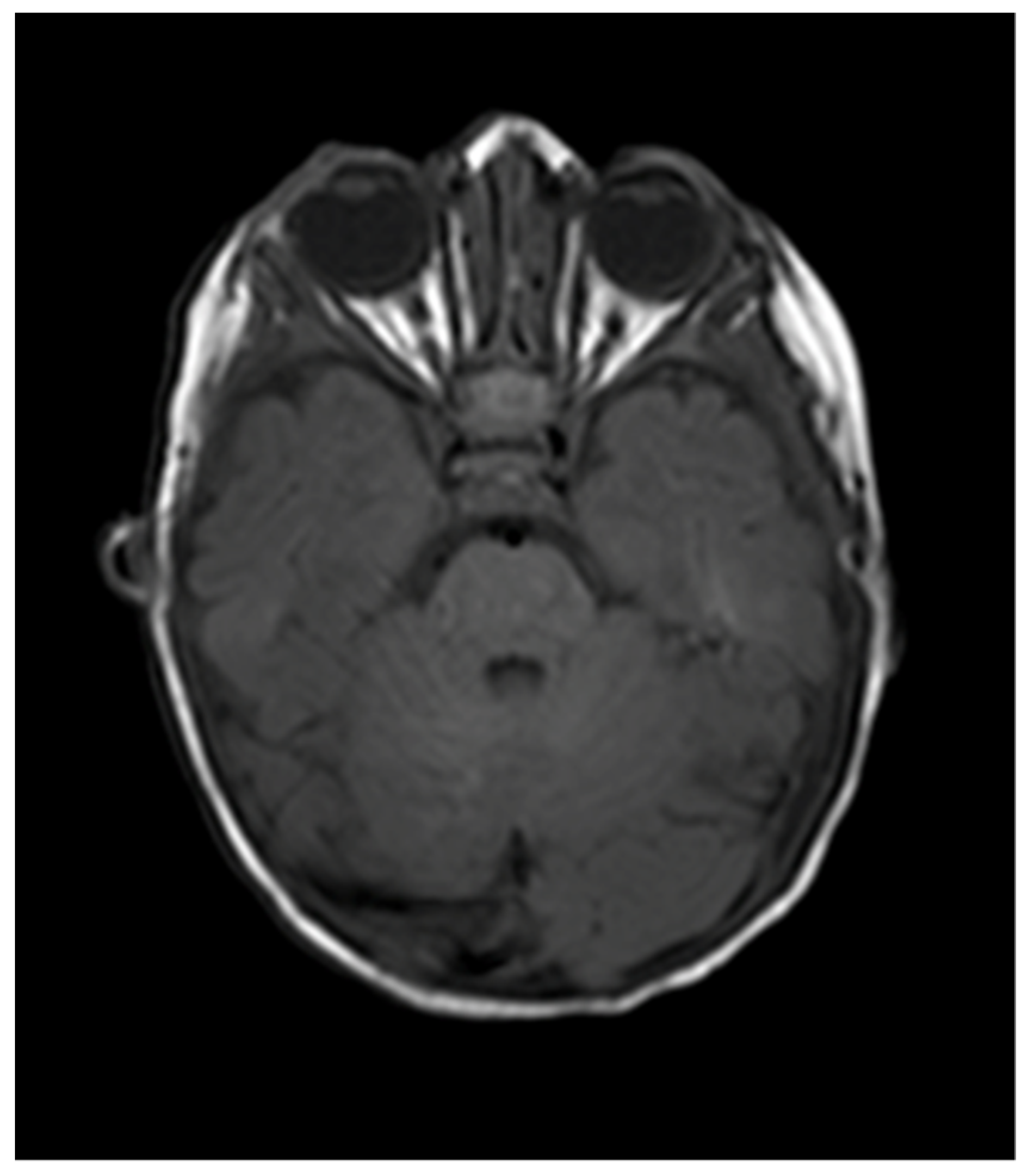
Axial T1 weighted and T2 weighted TSE brain magnetic resonance imaging of patient on presentation. Extensive right orbital lesion with marked proptosis. Extension of the lesion intracranially, with involvement of right Meckel’s cave (pointer) and the cerebellar pontine angle.
Figure 2.
Axial T1 weighted and T2 weighted TSE brain magnetic resonance imaging of patient on presentation. Extensive right orbital lesion with marked proptosis. Extension of the lesion intracranially, with involvement of right Meckel’s cave (pointer) and the cerebellar pontine angle.

Figure 3.
Four months after commencement of treatment. Complete resolution of proptosis. Skin hemangioma flat and pale.
Figure 3.
Four months after commencement of treatment. Complete resolution of proptosis. Skin hemangioma flat and pale.

Figure 4.
MRI 4 months following commencement of treatment with beta blockers. Total resolution of the orbital hemangioma and of the associated intracranial extension.
Figure 4.
MRI 4 months following commencement of treatment with beta blockers. Total resolution of the orbital hemangioma and of the associated intracranial extension.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Cases of intracranial infantile hemangiomas.
| Author, Year | Age at Presentation, Gender | Neurological or Ophthalmic Complaint | Intracranial Location of Hemangioma | Treatment | Outcome |
|---|---|---|---|---|---|
| Willing et al., 1993 | 17 months, male | Focal seizures, mild developmental delay | Right temporal dura | Surgical excision | Resolution |
| Bar-Sever et al., 1994 | 2 weeks, female | Nil | Right middle fossa, extending into the right orbit and suprasellar cistern | Oral prednisolone (for 2 months—no response) Subsequent interferon | Marked reduction with interferon treatment |
| Tortori et al., 1999 | 1 month, female | Nil | Right uncohippocampal | Observation | Resolution |
| 1.5 months, female | Nil | Left CPA, leptomeningeal enhancement at cerebellar surface | Observation | Resolution | |
| 18 months, female | Nil at presentation, developed ataxia | Right CPA, hypothalamus | Systemic steroids, endovascular treatment with contour particles | Unchanged following steroids. Partial resolution following endovascular intervention | |
| 1 month, female | Nil | Left CPA, persistent trigeminal artery | Systemic steroids | Lost to follow-up | |
| Poetke et al., 2002 | 10 weeks, male | Nil | CPA, leptomeningeal enhancement on cerebellar surface | Nil | Unknown |
| Le Bihannic et al., 2005 | 6 weeks, male | Vomiting, disturbance in consciousness, seizures | Anterior choroidal artery, right temporal lobe | Nil | Intracranial haemorrhage, death |
| Ersoy et al., 2005 | 8 months, female | Nil | Lateral medullary cistern, IAC, fourth ventricle | Oral prednisolone | Marked reduction in lesion size |
| Karikari et al., 2006 | 3 months, male | Central hypotonia | Fourth ventricle, left CPA | Surgical resection | Resolution |
| Judd et al., 2007 | 3 weeks, female | Nil | IAC/CPA, | Oral prednisolone | Resolution |
| 3 weeks, female | Right facial paresis | IAC/CPA, fourth ventricle | Oral prednisolone | Resolution | |
| 6 weeks, female | Nil | IAC/CPA | Intralesional triamcinolone | Resolution | |
| 8 weeks, female | Nil | IAC, Meckel’s cave, cavernous sinus | Intralesional triamcinolone | Resolution | |
| Poindexter et al., 2007 | 2.5 months, female | Reduced truncal tone | Left IAC | Observation | Partial involution, developmental delay, diffuse hypotonia |
| Daenekindt et al., 2008 | 7 weeks, male | Enlarged head circumference | Right temporal fossa | Biopsy, Endovascular embolization and surgical resection | Resolution |
| Frei-Jones et al., 2008 | Newborn, female | Left CNVII palsy, left sensorineural hearing loss | Middle cranial fossa, temporal bone, posterior fossa | Biopsy, Thalidomide | Partial Resolution |
| Heyer et al., 2008 | 6 months, female | Nil | Left IAC | Observation | Unchanged |
| Uyama et al., 2008 | 4 months, female | Hydrocephalus | Left cerebellar hemisphere | Neuroendoscopic fenestration of cysts, Surgical resection of lesion | Resolution |
| Viswanathan et al., 2009 | 3 weeks, female | Hydrocephalus | Quad plate cistern, pineal region, left CPA | Corticosteroids | Reduction in lesion size |
| 9 weeks, female | Nil | Left cavernous sinus, Meckel’s cave, IAC | Corticosteroids | Lost to follow-up | |
| 4 months, female | Hydrocephalus | Fourth ventricle, left IAC, CPA | Corticosteroids | Reduction in lesion size | |
| 3 months, female | Left ptosis | Fourth ventricle, left foramen of Luschka, quad plate cistern | Interferon, OK432, subsequent corticosteroids | Reduction in lesion size | |
| 7 weeks, female | Right proptosis | Right temporal fossa, cavernous sinus, Meckel’s cave, sella, quad plate cisterns | Corticosteroids | Reduction in lesion size | |
| 7 weeks, male | Nil | Fourth ventricle, right foramen of Luschka, IAC | Reduction in lesion size | ||
| 3 weeks, male | Nil | Right CPA, foramen of Luschka, fourth ventricle | Corticosteroids, Interferon | Minimal response to corticosteroids, reduction in lesion size with Interferon | |
| Infancy, female | Nil | Peri-mesencephalic cistern, sella, cavernous sinus, left CPA | Interferon | Reduction in lesion size | |
| 3 months, female | Nil at presentation, subsequent stroke and hydrocephalus | Right cavernous sinus, CPA | Corticosteroids | Reduction in lesion size | |
| Philpott et al., 2012 | 12 months, female | Enlarged head circumference | Dura of right parietal lobe | Surgical resection | Resolution |
| Zheng et al., 2012 | 3 years, male | Somnolence, right CNIII palsy | Middle cranial fossa | Surgical resection | Resolution |
| Jalloh et al., 2014 | 2 weeks, Male | Tense anterior fontanelle, enlarging head circumference, seizures | Left middle cranial fossa | Biopsy, Surgical resection | Residual cyst, no recurrence |
| Benvenisti et al., 2014 | 4 weeks, female | Nil | Left posterior fossa | Oral propranolol | Reduction in lesion size, maintained at 12 months |
| Antonov et al., 2015 | 3 months, female | Nil | Middle cranial fossa, right cavernous sinus, prepontine cistern, infratemporal fossa | Oral propranolol | Resolution |
| 3 weeks, female | Nil | Right lateral ventricular trigone | Oral propranolol | Resolution | |
| El Rassi et al., 2015 | 5 weeks, female | Left CN V and VII palsy (PHACE syndrome) | Left CPA, IAC | Oral propranolol | Improvement in facial lesion, status of intracranial hemangioma not described |
| Cavalheiro et al., 2016 | 33 weeks gestation, male | Nil | Posterior fossa | Oral propranolol | Resolution |
| Kang et al., 2016 | 1 month, male | Nil | CPA | Oral propranolol | Resolution |
| Shakir et al., 2016 | 2 weeks, female | Hydrocephalus | Posterior fossa | Surgical resection | Resolution Post operative enlarging head circumference requiring VP shunt |
| Dalsin et al., 2016 | 37 weeks gestation, female | Diagnosed on antenatal ultrasound | Left middle cranial fossa | Surgical resection | Resolution, no neurological deficits |
| Haine et al., 2017 | 3 weeks, male | Symptoms of raised ICP | Posterior fossa | Surgical decompression Oral prednisolone | Resolution on imaging |
| Friedland et al., 2017 | 1 week, male | Nil | Not specified | Observation | Spontaneous resolution |
| Naughton et al., 2020 (this paper) | 6 weeks, female | Right CNVII palsy | Right orbit, right CPA and Meckel’s cave | Oral propranolol and topical timolol maleate 0.5% | Resolution |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Naughton, A.; Ong, A.Y.; Hildebrand, G.D. Safe and Effective Treatment of Intracranial Infantile Hemangiomas with Beta-Blockers. Pediatr. Rep. 2021, 13, 347-356. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13030043
AMA Style
Naughton A, Ong AY, Hildebrand GD. Safe and Effective Treatment of Intracranial Infantile Hemangiomas with Beta-Blockers. Pediatric Reports. 2021; 13(3):347-356. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13030043
Chicago/Turabian StyleNaughton, Aoife, Ariel Yuhan Ong, and Goran Darius Hildebrand. 2021. "Safe and Effective Treatment of Intracranial Infantile Hemangiomas with Beta-Blockers" Pediatric Reports 13, no. 3: 347-356. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13030043