
The 25(OH)D3, but Not 1,25(OH)2D3 Levels Are Elevated in IBD Patients Regardless of Vitamin D Supplementation and Do Not Associate with Pain Severity or Frequency

 ,
,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Study Group
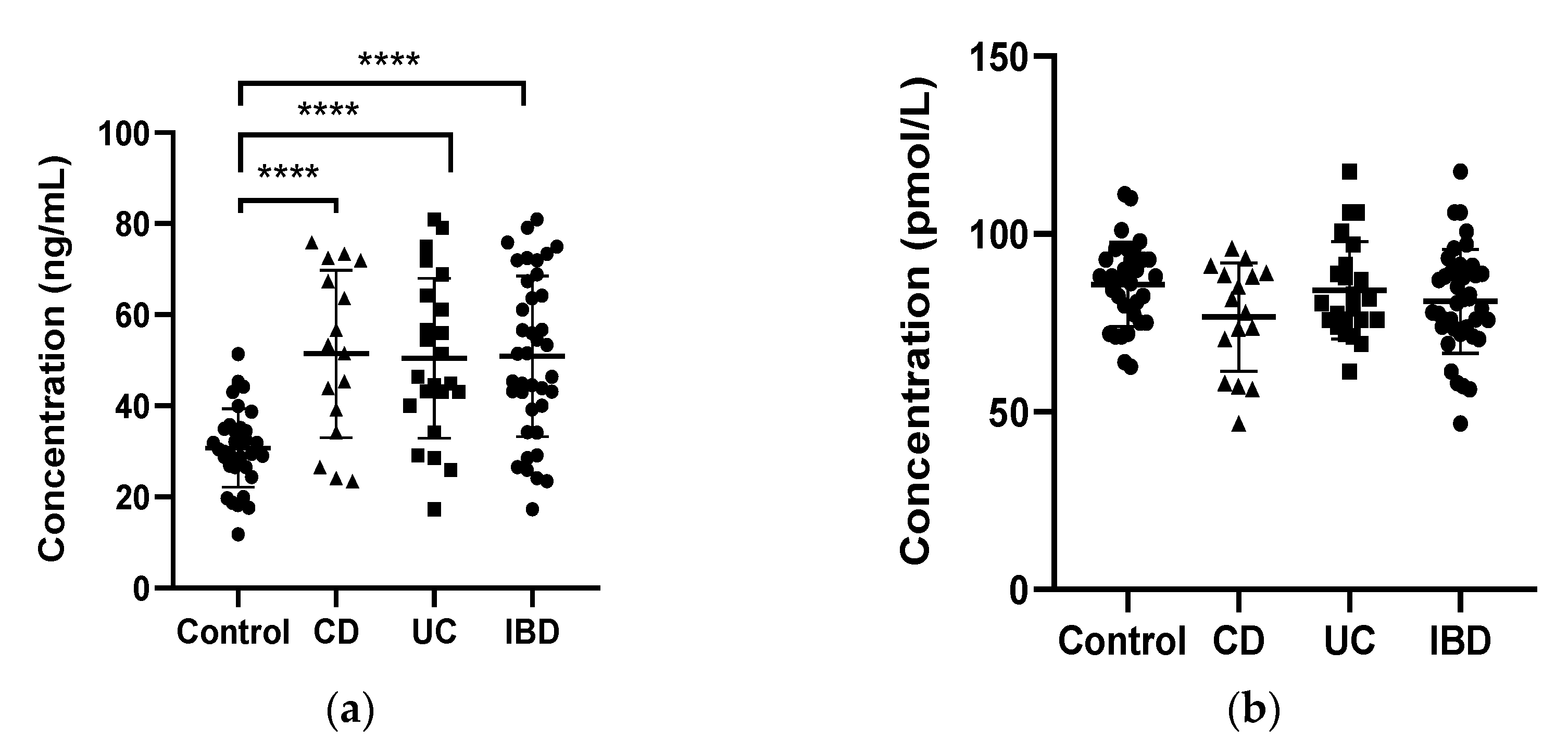
2.2. 25OH D3 and 1,25(OH)2D3 Levels
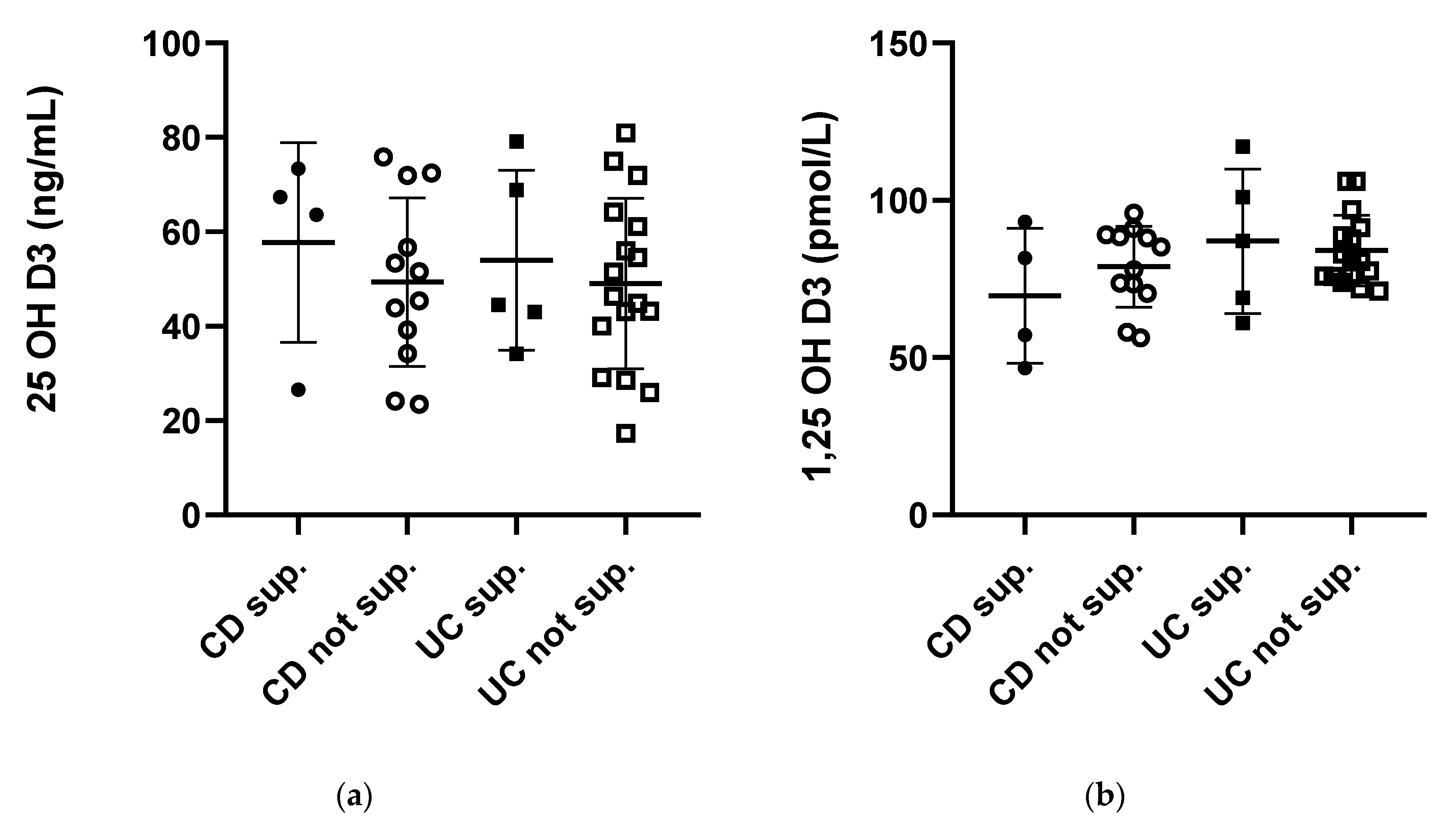
2.3. Vitamin D3 Supplementation
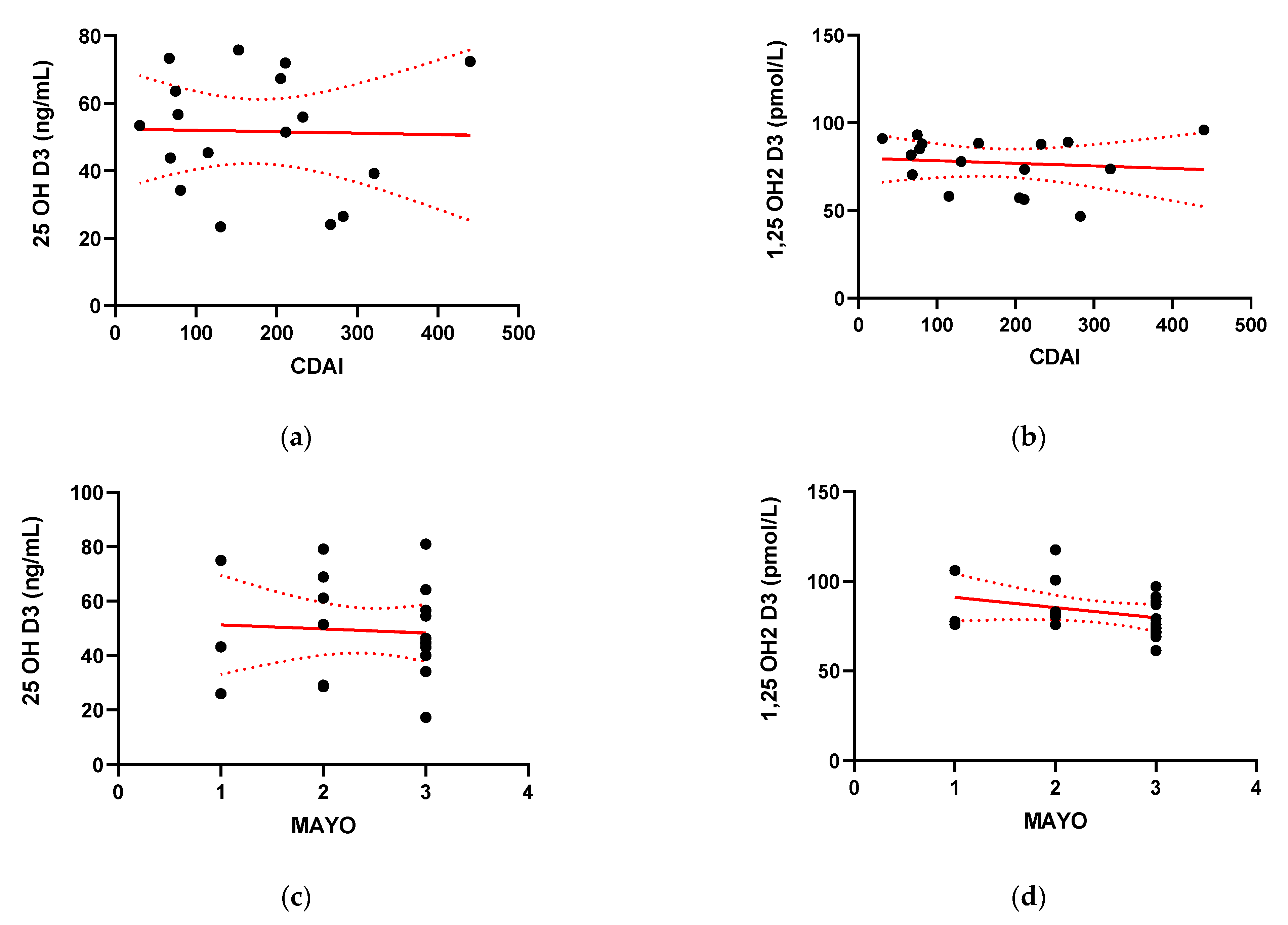
2.4. Disease Activity
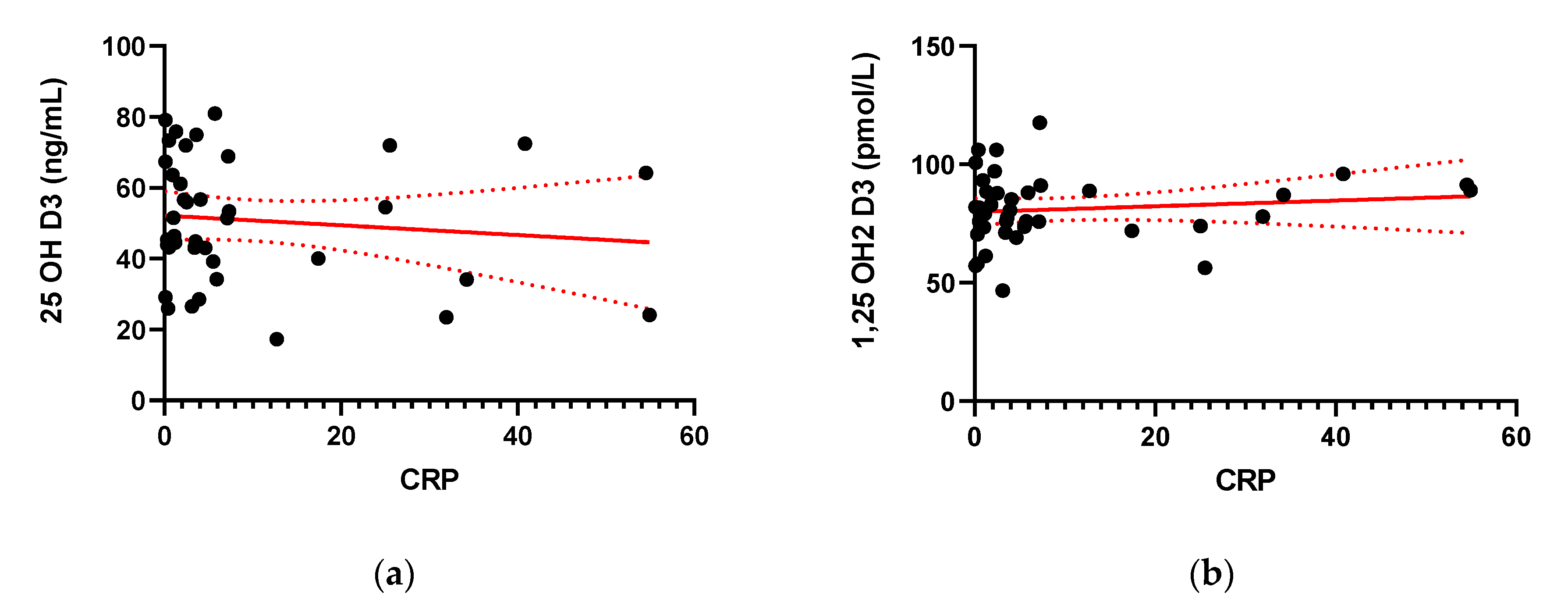
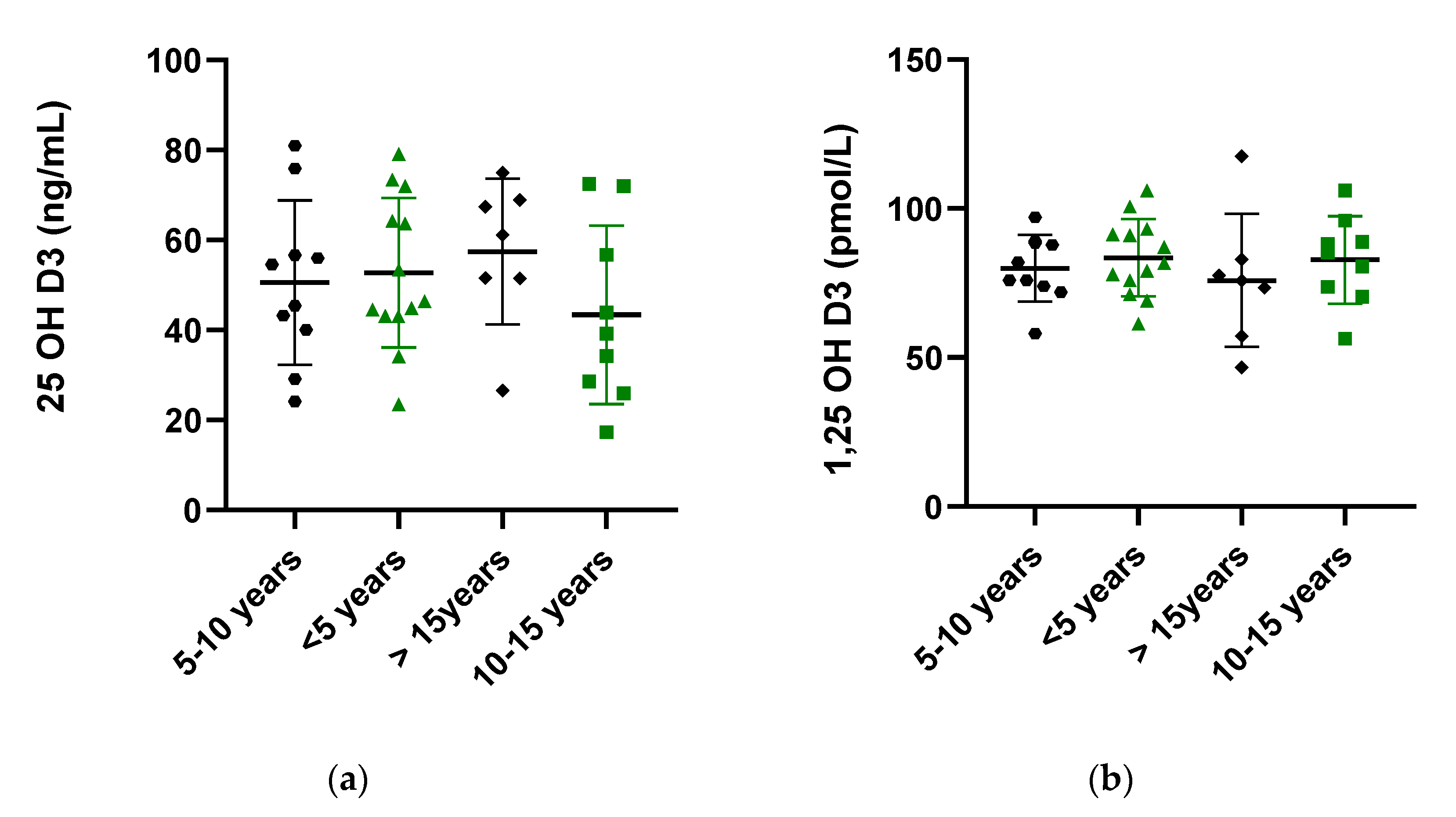
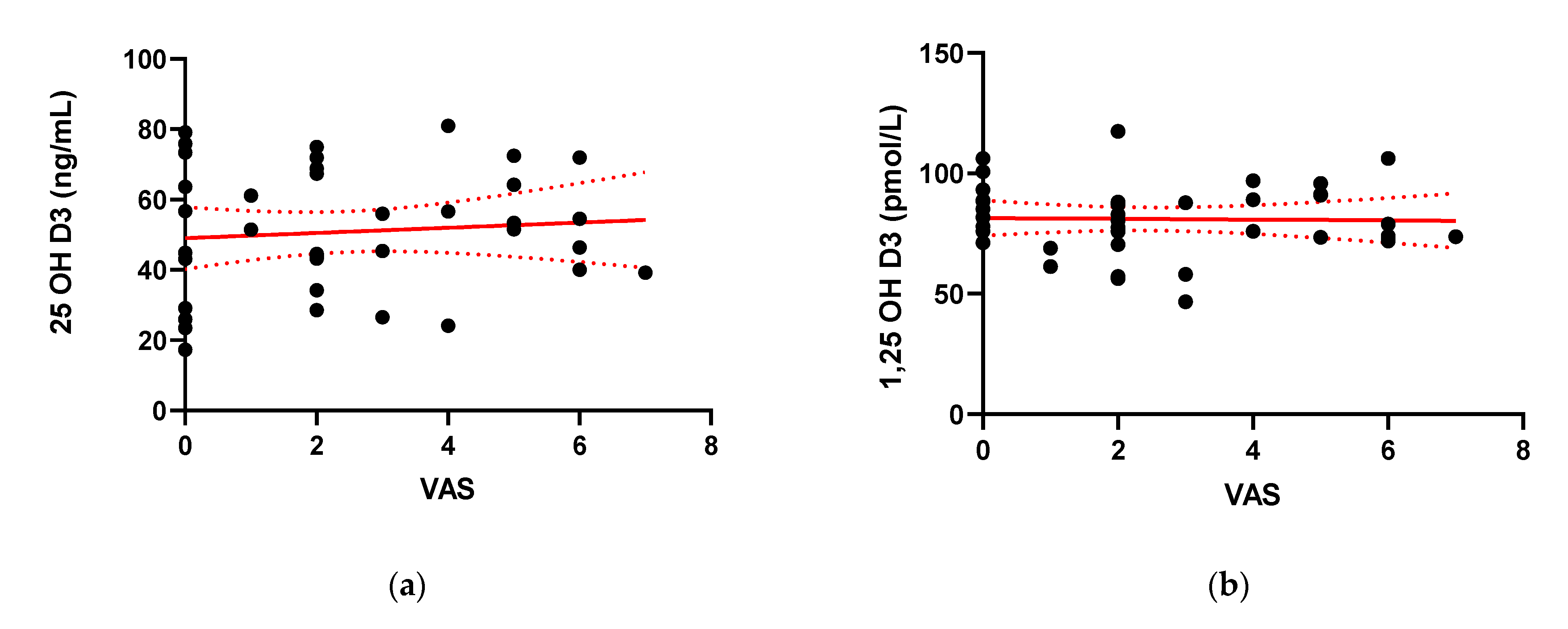
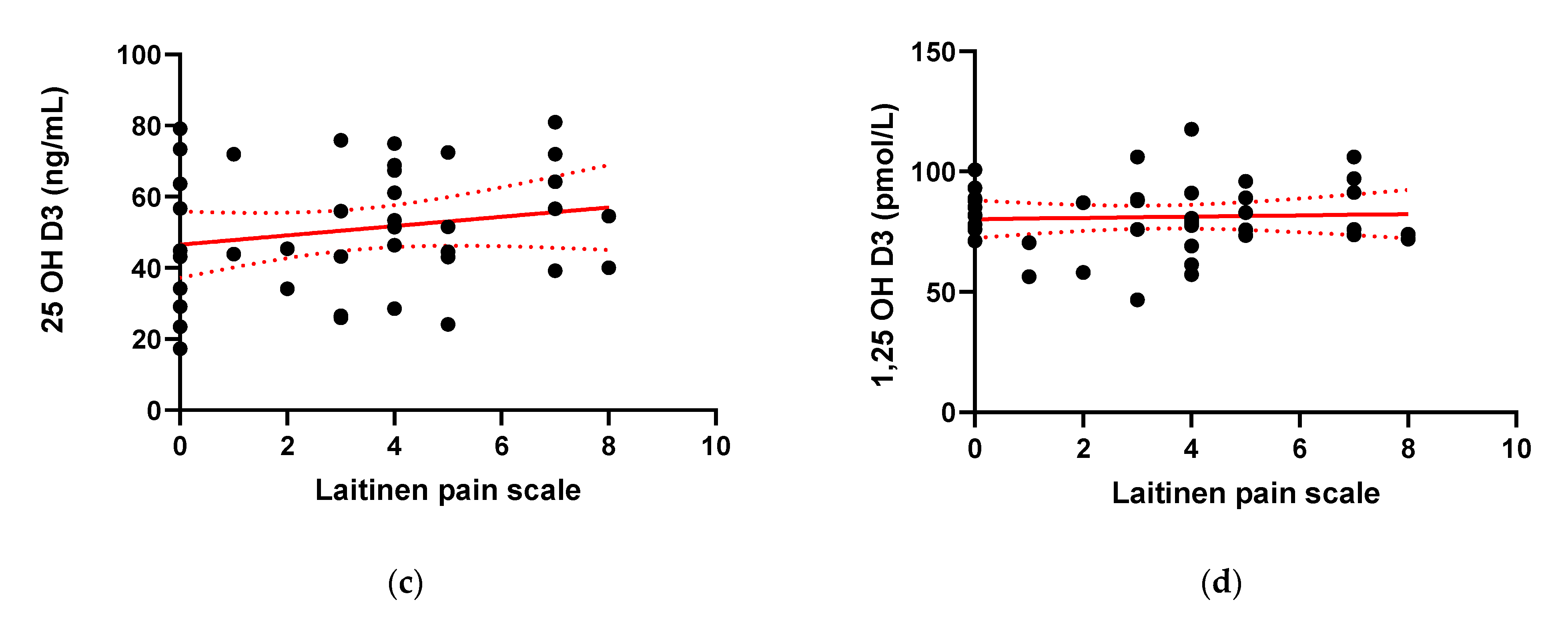
2.5. Inflammatory Status, Duration of the Disease and Pain
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The Role of Vitamin D in Inflammatory Bowel Disease: Mechanism to Management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef] [Green Version]
- Zielińska, A.; Sałaga, M.; Włodarczyk, M.; Fichna, J. Focus on Current and Future Management Possibilities in Inflammatory Bowel Disease-Related Chronic Pain. Int. J. Colorectal Dis. 2019, 34, 217–227. [Google Scholar] [CrossRef] [Green Version]
- Frigstad, S.O.; Høivik, M.L.; Jahnsen, J.; Cvancarova, M.; Grimstad, T.; Berset, I.P.; Huppertz-Hauss, G.; Hovde, Ø.; Bernklev, T.; Moum, B.; et al. Pain Severity and Vitamin D Deficiency in Ibd Patients. Nutrients 2020, 12, 26. [Google Scholar] [CrossRef] [Green Version]
- Ossum, A.M.; Palm, Ø.; Cvancarova, M.; Bernklev, T.; Jahnsen, J.; Moum, B.; Høivik, M.L. The Impact of Spondyloarthritis and Joint Symptoms on Health-Related Quality of Life and Fatigue in IBD Patients. Results from a Popu-lation-Based Inception Cohort (20-Year Follow-up in the Ibsen Study). Inflamm. Bowel Dis. 2020, 26, 114. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology Consensus Guidelines on the Management of Inflammatory Bowel Disease in Adults. Gut 2019, 68, s1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Chen, N.; Wang, D.; Zhang, J.; Gong, X. Efficacy of Vitamin D in Treatment of Inflammatory Bowel Disease: A Meta-Analysis. Medicine 2018, 97, e12662-e. [Google Scholar] [CrossRef] [PubMed]
- Burke, K.E.; Boumitri, C.; Ananthakrishnan, A.N. Modifiable Environmental Factors in Inflammatory Bowel Disease. Curr. Gastroenterol. Rep. 2017, 19, 1. [Google Scholar] [CrossRef] [Green Version]
- Parian, A.; Limketkai, B.N. Dietary Supplement Therapies for Inflammatory Bowel Disease: Crohn’s Disease and Ulcerative Colitis. Curr. Pharm. Des. 2015, 22, 180. [Google Scholar] [CrossRef] [PubMed]
- Bancil, A.; Poullis, A. The Role of Vitamin D in Inflammatory Bowel Disease. Healthcare 2015, 3, 338. [Google Scholar] [CrossRef] [Green Version]
- Mangin, M.; Sinha, R.; Fincher, K. Inflammation and Vitamin D: The Infection Connection. Inflamm. Res. 2014, 63, 803. [Google Scholar] [CrossRef] [Green Version]
- Reich, K.M.; Fedorak, R.N.; Madsen, K.; Kroeker, K.I. Vitamin D Improves Inflammatory Bowel Disease Out-comes: Basic Science and Clinical Review. World J. Gastroenterol. 2014, 20, 4934. [Google Scholar] [CrossRef]
- Abreu, M.T.; Kantorovich, Y.; Vasiliauskas, E.A.; Gruntmanis, U.; Matuk, R.; Daigle, K.; Chen, S.; Zehnder, D.; Lin, Y.C.; Yang, H.; et al. Measurement of Vitamin D Levels in Inflammatory Bowel Disease Patients Reveals a Subset of Crohn’s Disease Patients with Elevated 1,25-Dihydroxyvitamin D and Low Bone Mineral Density. Gut 2004, 53, 1129. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, C.N.; Seeger, L.L.; Anton, P.A.; Artinian, L.; Geffrey, S.; Goodman, W.; Belin, T.R.; Shanahan, F. A Randomized, Placebo-Controlled Trial of Calcium Supplementation for Decreased Bone Density in Corticosteroid-Using Patients with Inflammatory Bowel Disease: A Pilot Study. Aliment. Pharmacol. Ther. 1996, 10, 777. [Google Scholar] [CrossRef]
- Alkhouri, R.H.; Hashmi, H.; Baker, R.D.; Gelfond, D.; Baker, S.S. Vitamin and Mineral Status in Patients with Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 89. [Google Scholar] [CrossRef]
- Lamb, E.J.; Wong, T.; Smith, D.J.; Simpson, D.E.; Coakley, A.J.; Moniz, C.; Muller, A.F. Metabolic Bone Dis-ease Is Present at Diagnosis in Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2002, 16, 1895. [Google Scholar] [CrossRef] [PubMed]
- Nerich, V.; Jantchou, P.; Boutron-Ruault, M.-C.; Monnet, E.; Weill, A.; Vanbockstael, V.; Auleley, G.-R.; Balaire, C.; Dubost, P.; Rican, S.; et al. Low Exposure to Sunlight Is a Risk Factor for Crohn’s Disease. Al-iment. Pharmacol. Ther. 2011, 33, 940. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Cagan, A.; Gainer, V.S.; Cai, T.; Cheng, S.C.; Savova, G.; Chen, P.; Szolovits, P.; Xia, Z.; de Jager, P.L.; et al. Normaliza-tion of Plasma 25-Hydroxy Vitamin D Is Associated with Reduced Risk of Surgery in Crohn’s Disease. Inflamm. Bowel Dis. 2013, 19, 1921. [Google Scholar] [PubMed] [Green Version]
- Ananthakrishnan, A.N.; Khalili, H.; Higuchi, L.M.; Bao, Y.; Korzenik, J.R.; Giovannucci, E.L.; Richter, J.M.; Fuchs, C.S.; Chan, A.T. Higher Predicted Vitamin D Status Is Associated with Reduced Risk of Crohn’s Disease. Gastro-Enterology 2012, 142, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund-Nielsen, J.; Vedel-Krogh, S.; Kobylecki, C.J.; Brynskov, J.; Afzal, S.; Nordestgaard, B.G. Vitamin D and Inflammatory Bowel Disease: Mendelian Randomization Analyses in the Copenhagen Studies and UK Biobank. J. Clin. En-docrinol. Metab. 2018, 103, 3267. [Google Scholar] [CrossRef] [PubMed]
- Augustine, M.V.; Leonard, M.B.; Thayu, M.; Baldassano, R.N.; de Boer, I.H.; Shults, J.; Denson, L.A.; DeBo-er, M.D.; Herskovitz, R.; Denburg, M.R. Changes in Vitamin D-Related Mineral Metabolism after Induction with An-ti-Tumor Necrosis Factor-α Therapy in Crohn’s Disease. J. Clin. Endocrinol. Metab. 2014, 99, E991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.X.; Liu, Y.; Luo, J.; Huang, Z.D.; Zhang, C.; Fu, Y. Vitamin D Deficiency Associated with Crohn’s Disease and Ulcerative Colitis: A Meta-Analysis of 55 Observational Studies. J. Transl. Med. 2019, 17, 1. [Google Scholar] [CrossRef] [Green Version]
- Boden, S.D.; Kaplan, F.S. Calcium Homeostasis. Orthop. Clin. North Am. 1990, 21, 31–42. [Google Scholar] [CrossRef]
- Vanderschueren, D.; Pye, S.R.; O’Neill, T.W.; Lee, D.M.; Jans, I.; Billen, J.; Gielen, E.; Laurent, M.; Claessens, F.; Adams, J.E.; et al. Active Vitamin D (1,25-Dihydroxyvitamin D) and Bone Health in Middle-Aged and Elderly Men: The European Male Aging Study (EMAS). J. Clin. Endocrinol. Metab. 2013, 98, 995. [Google Scholar] [CrossRef] [Green Version]
- Kabbani, T.A.; Koutroubakis, I.E.; Schoen, R.E.; Ramos-Rivers, C.; Shah, N.; Swoger, J.; Regueiro, M.; Barrie, A.; Schwartz, M.; Hashash, J.G.; et al. Association of Vitamin D Level with Clinical Status in Inflammatory Bowel Disease: A 5-Year Longitudinal Study. Am. J. Gastroenterol. 2016, 111, 712. [Google Scholar] [CrossRef] [PubMed]
- Grunbaum, A.; Holcroft, C.; Heilpern, D.; Gladman, S.; Burstein, B.; Menard, M.; Al-Abbad, J.; Cassoff, J.; Mac-namara, E.; Gordon, P.H.; et al. Dynamics of Vitamin D in Patients with Mild or Inactive Inflammatory Bowel Disease and Their Families. Nutr. J. 2013, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suibhne, T.N.; Cox, G.; Healy, M.; O’Morain, C.; O’Sullivan, M. Vitamin D Deficiency in Crohn’s Disease: Prevalence, Risk Factors and Supplement Use in an Outpatient Setting. J. Crohn’s Colitis 2012, 6, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narula, N.; Cooray, M.; Anglin, R.; Muqtadir, Z.; Narula, A.; Marshall, J.K. Impact of High-Dose Vitamin D3 Supplementation in Patients with Crohn’s Disease in Remission: A Pilot Randomized Double-Blind Controlled Study. Dig. Dis. Sci. 2017, 62, 448. [Google Scholar] [CrossRef]
- Palmer, M.T.; Weaver, C.T. Linking Vitamin D Deficiency to Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2013, 19, 2245–2256. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, S.P.; Agnholt, J.; Glerup, H.; Lyhne, S.; Villadsen, G.E.; Hvas, C.L.; Bartels, L.E.; Kelsen, J.; Chris-tensen, L.A.; Dahlerup, J.F. Clinical Trial: Vitamin D3 Treatment in Crohn’s Disease A Randomized Double-Blind Place-bo-Controlled Study. Aliment. Pharmacol. Ther. 2010, 32, 377. [Google Scholar] [CrossRef]
- Yang, L.; Weaver, V.; Smith, J.P.; Bingaman, S.; Hartman, T.J.; Cantorna, M.T. Therapeutic Effect of Vitamin d Supplementation in a Pilot Study of Crohn’s Patients. Clin. Transl. Gastroenterol. 2013, 4, e33. [Google Scholar] [CrossRef]
- Winter, R.W.; Collins, E.; Cao, B.; Carrellas, M.; Crowell, A.M.; Korzenik, J.R. Higher 25-hydroxyvitamin D levels are associated with greater odds of remission with anti-tumour necrosis factor-α medications among patients with inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2017, 45, 653. [Google Scholar]
- Joseph, A.J.; George, B.; Pulimood, A.B.; Seshadri, M.S.; Chacko, A. 25 (OH) Vitamin D Level in Crohn’s Dis-ease: Association with Sun Exposure & Disease Activity. Indian J. Med. Res. 2009, 130, 133. [Google Scholar] [PubMed]
- Blanck, S.; Aberra, F. Vitamin D Deficiency Is Associated with Ulcerative Colitis Disease Activity. Dig. Dis. Sci. 2013, 58, 1698. [Google Scholar] [CrossRef] [PubMed]
- Hassan, V.; Hassan, S.; Seyed-Javad, P.; Ahmad, K.; Asieh, H.; Maryam, S.; Farid, F.; Siavash, A. Association between Serum 25 (OH) Vitamin D Concentrations and Inflammatory Bowel Diseases (IBDS) Activity. Med. J. Malaysia 2013, 68, 34. [Google Scholar]
- Jun, J.C.; Yoon, H.; Choi, Y.J.; Shin, C.M.; Park, Y.S.; Kim, N.; Lee, D.H.; Kim, J.S. The Effect of Vitamin D Ad-ministration on Inflammatory Markers in Patients with Inflammatory Bowel Disease. Intest. Res. 2019, 17, 210. [Google Scholar] [CrossRef] [Green Version]
- Garg, M.; Hendy, P.; Ding, J.N.; Shaw, S.; Hold, G.; Hart, A. The Effect of Vitamin D on Intestinal Inflammation and Faecal Microbiota in Patients with Ulcerative Colitis. J. Crohn’s Colitis 2018, 12, 963. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, A.; Hosseinzadeh-Attar, M.J.; Vahedi, H.; Nedjat, S. A Randomized Controlled Trial on the Effect of Vitamin D3 on Inflammation and Cathelicidin Gene Expression in Ulcerative Colitis Patients. Saudi J. Gastroenterol. 2016, 22, 316. [Google Scholar]
- Tajika, M.; Matsuura, A.; Nakamura, T.; Suzuki, T.; Sawaki, A.; Kato, T.; Hara, K.; Ookubo, K.; Yamo, K.; Kato, M.; et al. Risk Factors for Vitamin D Deficiency in Patients with Crohn’s Disease. J. Gastroenterol. 2004, 39, 527. [Google Scholar] [CrossRef]
- Ulitsky, A.; Ananthakrishnan, A.N.; Naik, A.; Skaros, S.; Zadvornova, Y.; Binion, D.G.; Issa, M. Vitamin D Deficiency in Patients with Inflammatory Bowel Disease: Association with Disease Activity and Quality of Life. J. Parenter. Enter. Nutr. 2011, 35, 308. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Bechtold, M.L.; Nguyen, D.L. Vitamin D and the Pathogenesis of Inflammatory Bowel Dis-ease. Curr. Gastroenterol. Rep. 2016, 18, 1–8. [Google Scholar] [CrossRef]
- Kanof, M.E.; Lake, A.M.; Bayless, T.M. Decreased Height Velocity in Children and Adolescents before the Di-agnosis of Crohn’s Disease. Gastroenterology 1988, 95, 1523. [Google Scholar] [CrossRef]
- Liu, X.; Nelson, A.; Wang, X.; Farid, M.; Gunji, Y.; Ikari, J.; Iwasawa, S.; Basma, H.; Feghali-Bostwick, C.; Rennard, S.I. Vitamin D Modulates Prostaglandin E2 Synthesis and Degradation in Human Lung Fibroblasts. Am. J. Respir. Cell Mol. Biol. 2014, 50, 40. [Google Scholar]
- Von Känel, R.; Müller-Hartmannsgruber, V.; Kokinogenis, G.; Egloff, N. Vitamin D and Central Hypersensi-tivity in Patients with Chronic Pain. Pain Med. 2014, 15, 1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coates, M.D.; Lahoti, M.; Binion, D.G.; Szigethy, E.M.; Regueiro, M.D.; Bielefeldt, K. Abdominal Pain in Ul-cerative Colitis. Inflamm. Bowel Dis. 2013, 19, 2207. [Google Scholar] [CrossRef] [PubMed]
- Test: 1,25-Dihydroxvitamin D (1,25-D) (MPKB). Available online: https://mpkb.org/home/tests/125d (accessed on 13 January 2021).
- Walsh, A.; Palmer, R.; Travis, S. Mucosal Healing as a Target of Therapy for Colonic Inflammatory Bowel Dis-ease and Methods to Score Disease Activity. Gastrointest. Endosc. Clin. North Am. 2014, 24, 367–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vashist, N.M.; Samaan, M.; Mosli, M.H.; Parker, C.E.; Macdonald, J.K.; Nelson, S.A.; Zou, G.Y.; Feagan, B.G.; Khanna, R.; Jairath, V. Endoscopic Scoring Indices for Evaluation of Disease Activity in Ulcerative Colitis. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Goddard, G.; Karibe, H.; McNeill, C. Reproducibility of Visual Analog Scale (VAS) Pain Scores to Mechanical Pressure. Cranio 2004, 22, 250. [Google Scholar] [CrossRef] [PubMed]
- Janusz, K. Kinesiophobia (Fear of Movement) Level Among Patients with Diagnosis of Cervicogenic Headache Poziom Kinezjofobii (Strach Przed Ruchem) u Pacjentów Ze Zdiagnozowanym Szyjnopochodnym Bólem Głowy Janusz Kocjan Medical University of Silesia. School M 2017, 7, 390. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IBD Patients | Control Group | |
|---|---|---|
| Subjects, n (%) | 39 | 33 |
| CD 17 (43.6%) | ||
| UC 22 (56.4%) | ||
| Sex | ||
| Men, n (%) | 22 (56.4%) | 15 (45.5%) |
| Women, n (%) | 17 (43.6%) | 18 (54.5%) |
| Age, year | 35.74 ± 13.61 | 38.73 ± 17.52 |
| BMI, kg/m2 | 32.21 ± 4.88 | 24.45 ± 4.05 |
| Duration of disease, n (%) | ||
| <5 years | 13 (33.3%) | |
| 5–10 years | 10 (25.6%) | |
| 10–15 years | 9 (23.1%) | |
| >15 years | 7 (19%) | |
| Resection, n (%) | 6 (15.4%) | |
| Colostomy, n (%) | 2 (5.1%) | |
| Extraintestinal symptoms, n (%) | 23 (59.1%) | |
| Use of painkillers, n (%) | 13 (33.3%) | 4 (12.1%) |
| NSAIDs | 12 (30.8%) | |
| Opioids-Tramadol | 1 (2.6%) | |
| Biological treatment, n (%) | ||
| IFX | 33 (84.6%) | |
| ADA | 2 (5.1%) | |
| VDZ | 4 (10.3%) | |
| CDAI, points | 180.47 ± 110.32 | |
| MAYO, points | 2.43 ± 0.75 | |
| Vitamin D3 supplementation, n (%) | ||
| None | 30 (76.9%) | 32 (97.0%) |
| 1500 IU | 3 (7.7%) | |
| 2000 IU | 5 (12.8%) | |
| 4000 IU | 1 (2.6%) | 1 (3.0%) |
| Mean 25(OH)D3, ng/mL | 50.85 ± 17.68 | 30.73 ± 8.65 |
| Mean 1,25(OH)2D3, pmol/L | 81.05 ± 14.64 | 85.84 ± 2.10 |
| White blood cell count, ×103/µL | 8.14 ± 4.08 | |
| Red blood cell count, ×106/µL | 4.57 ± 0.54 | |
| Hemoglobin, g/dL | 12.91 ± 3.01 | |
| Hematocrit, % | 39.02 ± 5.31 | |
| Platelet count, ×103/µL | 358.08 ± 154.76 | |
| Mean platelet volume, fL | 9.91 ± 1.01 | |
| CRP, mg/dL | 9.71 ± 14.74 |
| Factor | Subjective Evaluation | Points | n, % |
|---|---|---|---|
| Pain Intensity | Without pain | 0 | 13 (33.3%) |
| Mild | 1 | 18 (46.2%) | |
| Strong | 2 | 8 (20.5%) | |
| Very strong | 3 | 0 | |
| Not sustainable | 4 | 0 | |
| PAIN FREQUENCY | Does not occur | 0 | 12 (30.8%) |
| Periodical | 1 | 18 (46.2%) | |
| Frequent | 2 | 8 (20.5%) | |
| Very frequent | 3 | 0 | |
| Continuous | 4 | 1 (2.6%) | |
| PAINKILLERS’ INTAKE | Without medication | 0 | 13 (33.3%) |
| Periodically | 1 | 24 (61.5%) | |
| Permanently- small doses | 2 | 2 (5.1%) | |
| Permanently- big doses | 3 | 0 | |
| Permanently- very big doses | 4 | 0 | |
| MOTOR ACTIVITY LIMITATION | None | 0 | 18 (46.2%) |
| Partial | 1 | 12 (30.8%) | |
| Demanding partial help/making work difficult | 2 | 8 (20.5%) | |
| Demanding partial help/making work impossible | 3 | 0 | |
| Demanding full help/preventing self sufficiency | 4 | 1 (2.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zielińska, A.; Sobolewska-Włodarczyk, A.; Wiśniewska-Jarosińska, M.; Gąsiorowska, A.; Fichna, J.; Sałaga, M. The 25(OH)D3, but Not 1,25(OH)2D3 Levels Are Elevated in IBD Patients Regardless of Vitamin D Supplementation and Do Not Associate with Pain Severity or Frequency. Pharmaceuticals 2021, 14, 284. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14030284
Zielińska A, Sobolewska-Włodarczyk A, Wiśniewska-Jarosińska M, Gąsiorowska A, Fichna J, Sałaga M. The 25(OH)D3, but Not 1,25(OH)2D3 Levels Are Elevated in IBD Patients Regardless of Vitamin D Supplementation and Do Not Associate with Pain Severity or Frequency. Pharmaceuticals. 2021; 14(3):284. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14030284
Chicago/Turabian StyleZielińska, Anna, Aleksandra Sobolewska-Włodarczyk, Maria Wiśniewska-Jarosińska, Anita Gąsiorowska, Jakub Fichna, and Maciej Sałaga. 2021. "The 25(OH)D3, but Not 1,25(OH)2D3 Levels Are Elevated in IBD Patients Regardless of Vitamin D Supplementation and Do Not Associate with Pain Severity or Frequency" Pharmaceuticals 14, no. 3: 284. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14030284