
Comparative In Vitro Evaluation of Commercial Periodontal Gels on Antibacterial, Biocompatibility and Wound Healing Ability

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Periodontal Gels Used in the Study
2.2. Screening of Antimicrobial Activity
2.2.1. Culture and Proliferation Assay of P. gingivalis
2.2.2. Gingipain Activity of P. gingivalis
2.3. Testing of Periodontal Gels on 2D Culture Model with Human Gingival Fibroblasts under Inflammatory Conditions
2.3.1. ihGF Cell Culture
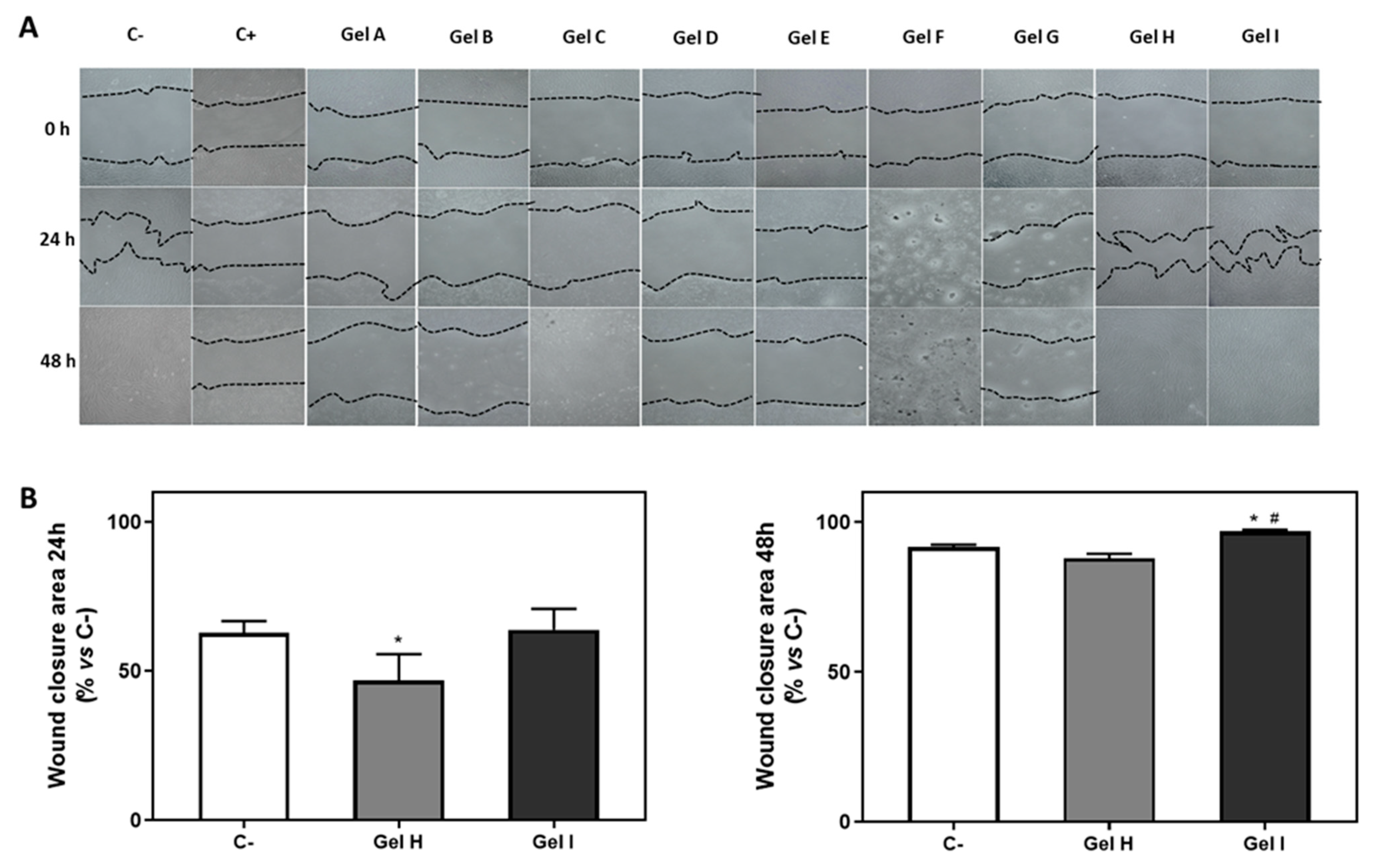
2.3.2. Wound Closure Assay
2.3.3. Cell Cytotoxicity
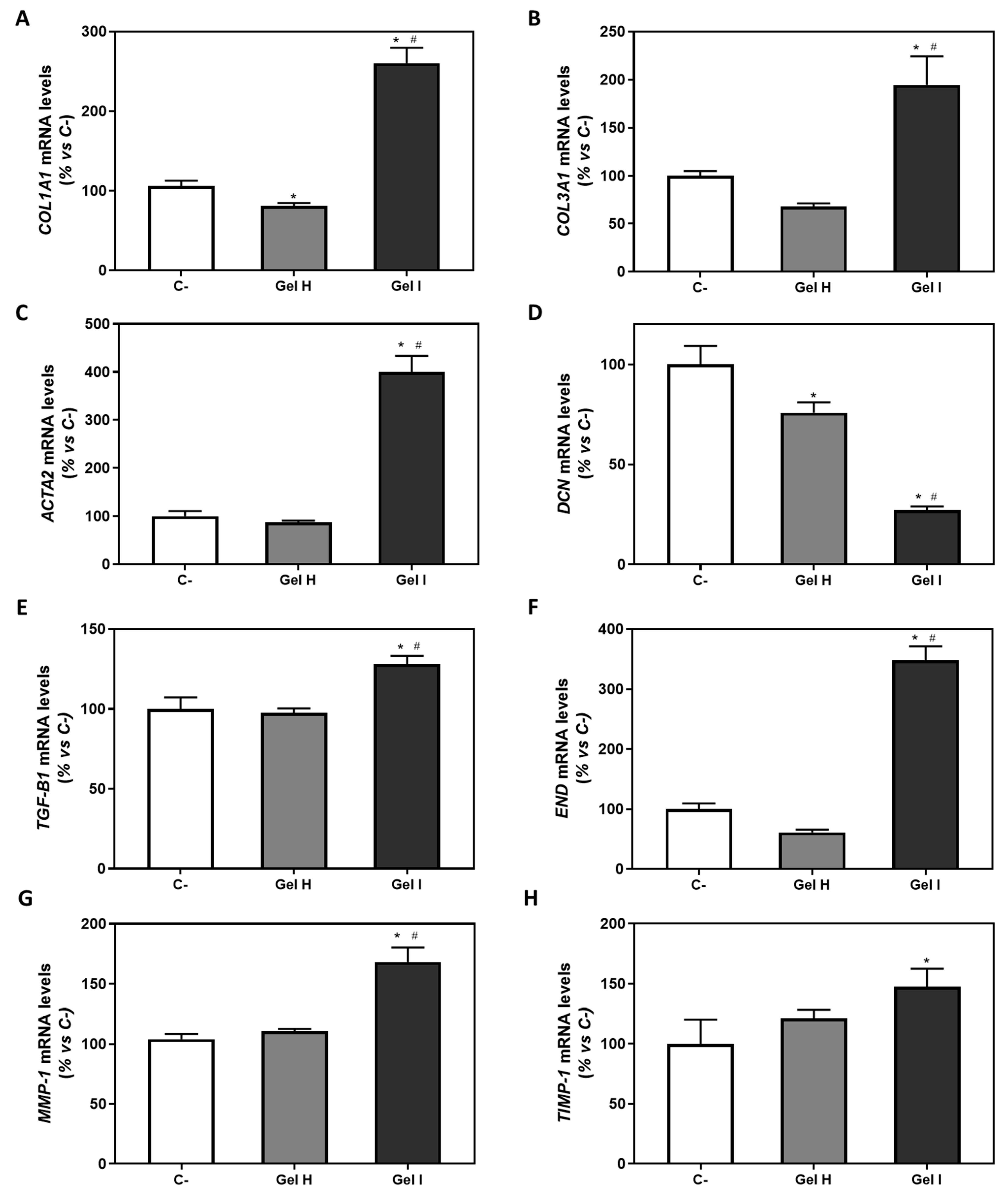
2.3.4. Gene Expression by Real-Time RT-PCR
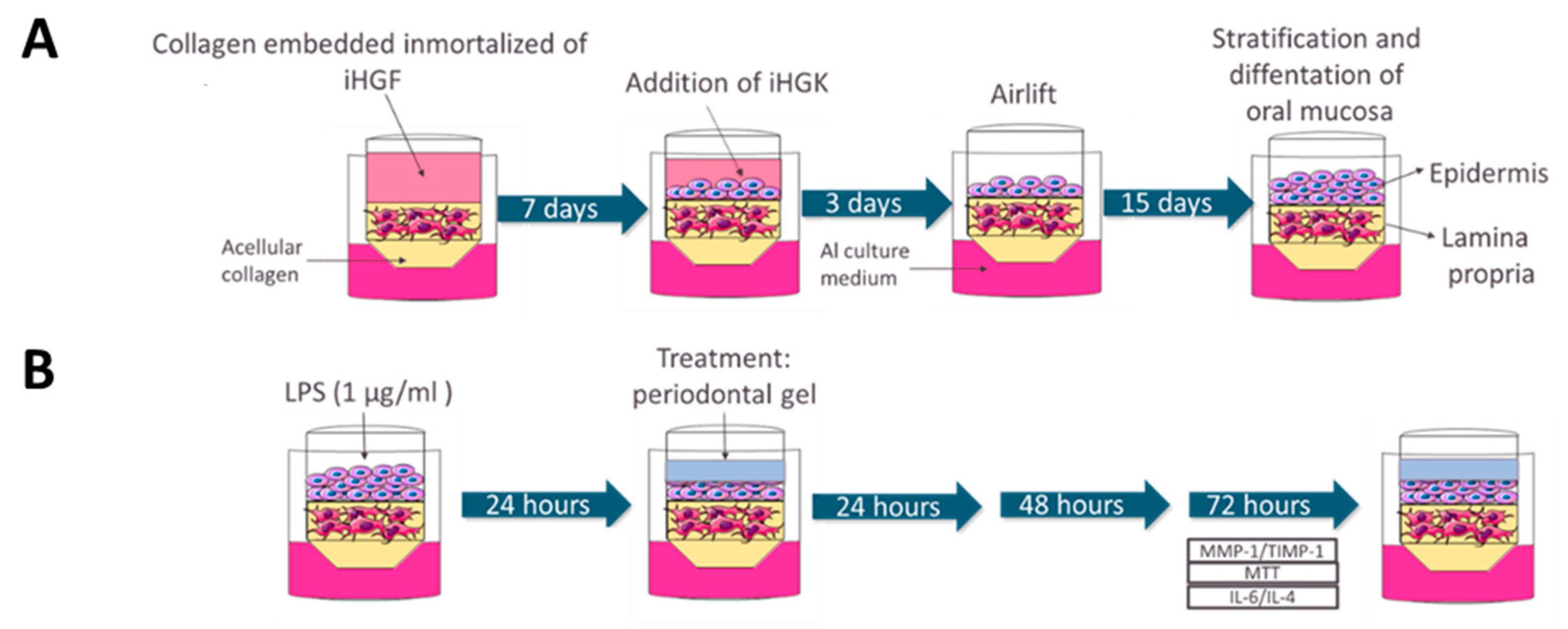
2.4. Testing of Periodontal Gels on 3D Gingival Tissue Equivalents (GTE)
2.4.1. Cell Culture
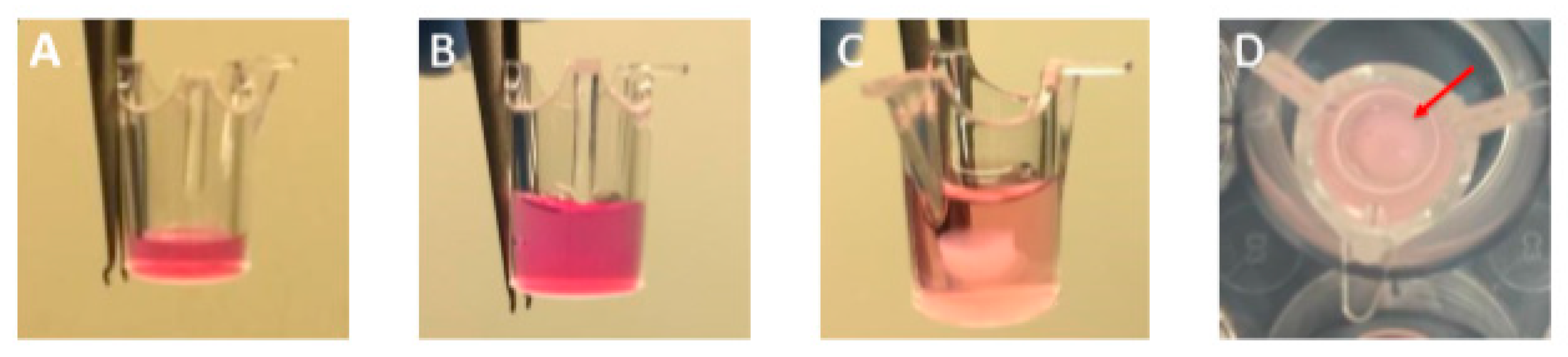
2.4.2. Engineering 3D Gingival Tissue Equivalent (GTE)
2.4.3. 3D Treatment with Periodontal Gels
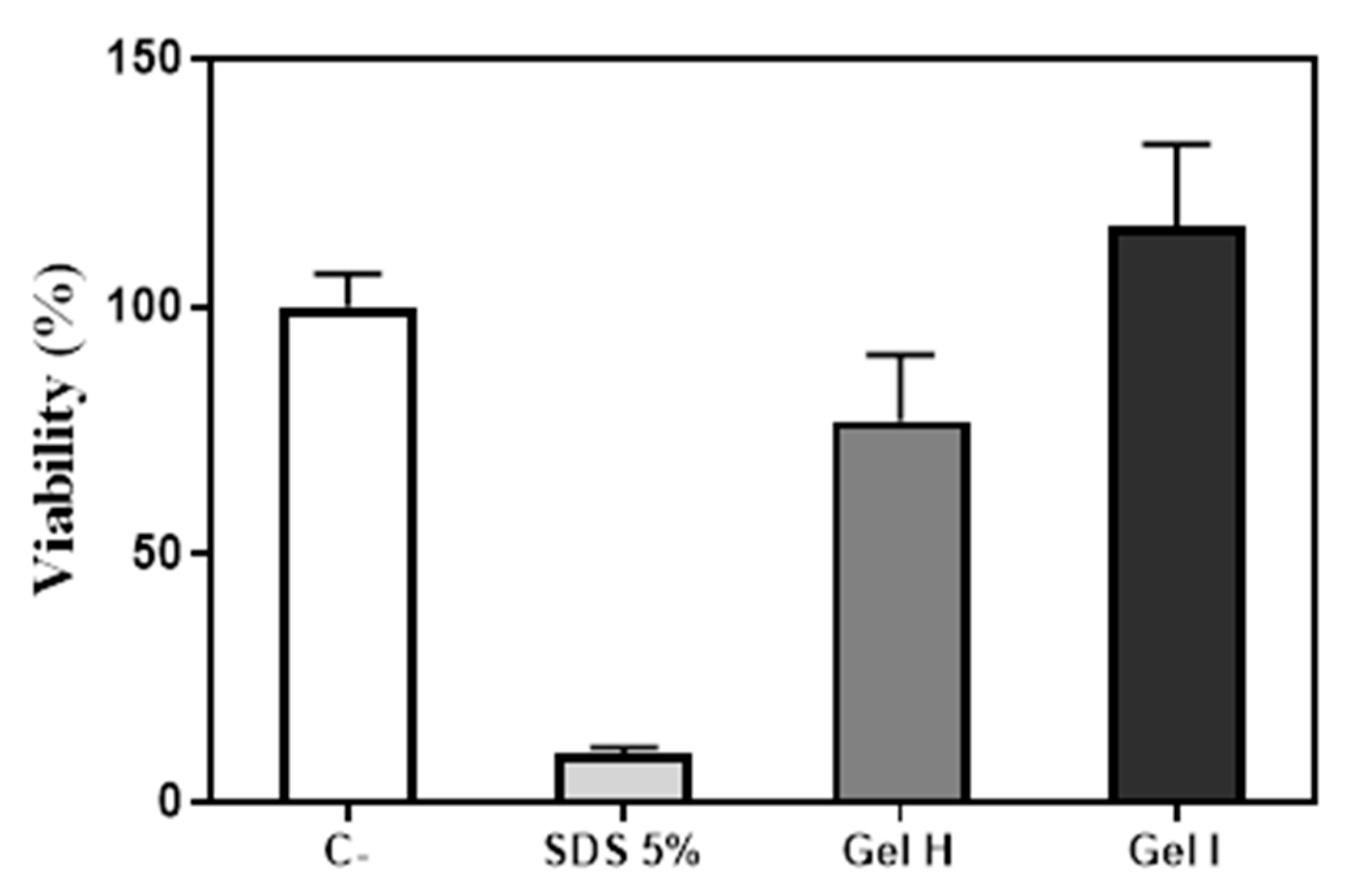
2.4.4. MTT Test
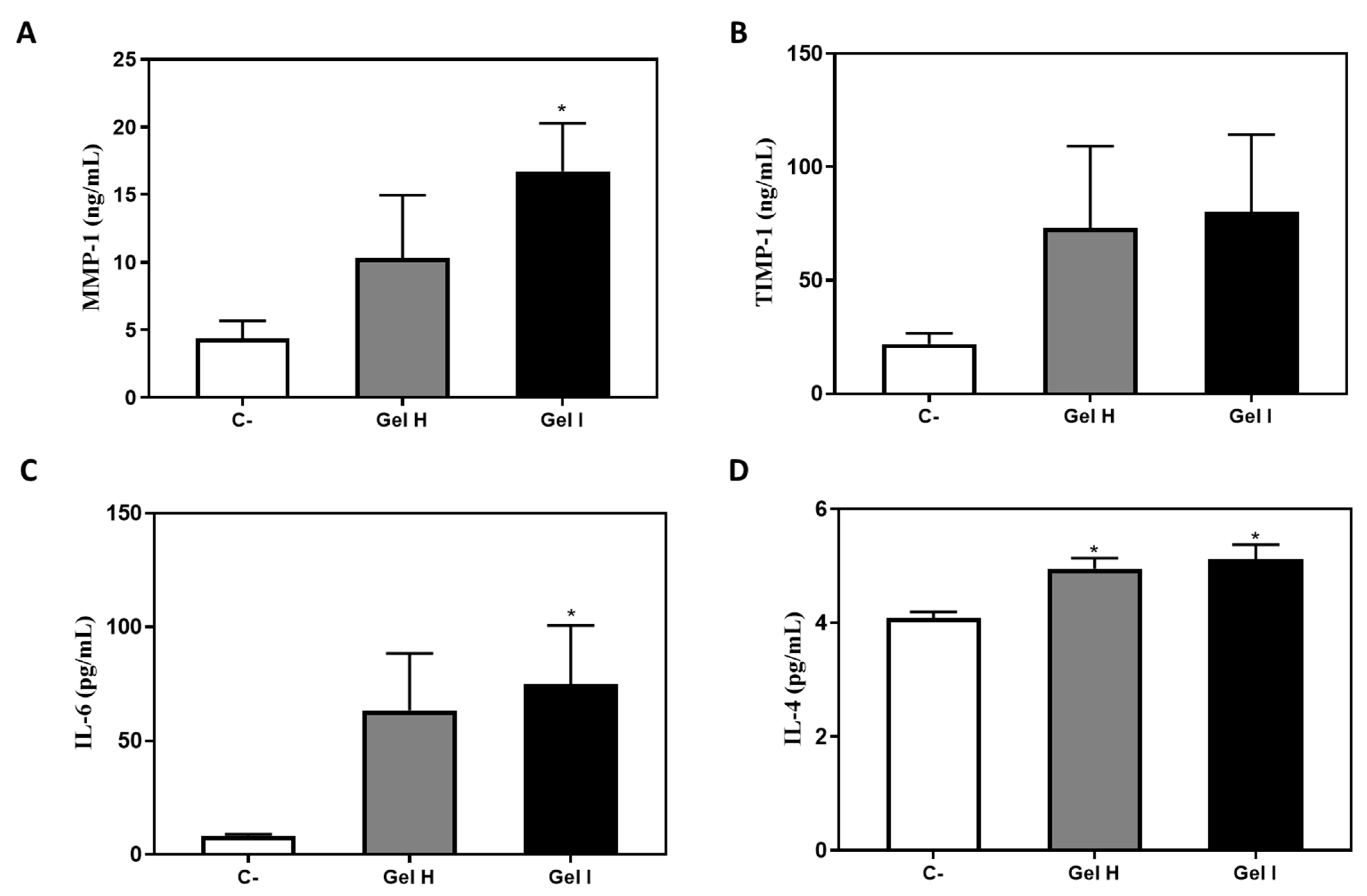
2.4.5. MMP-1 and TIMP-1
2.4.6. Cytokine Levels
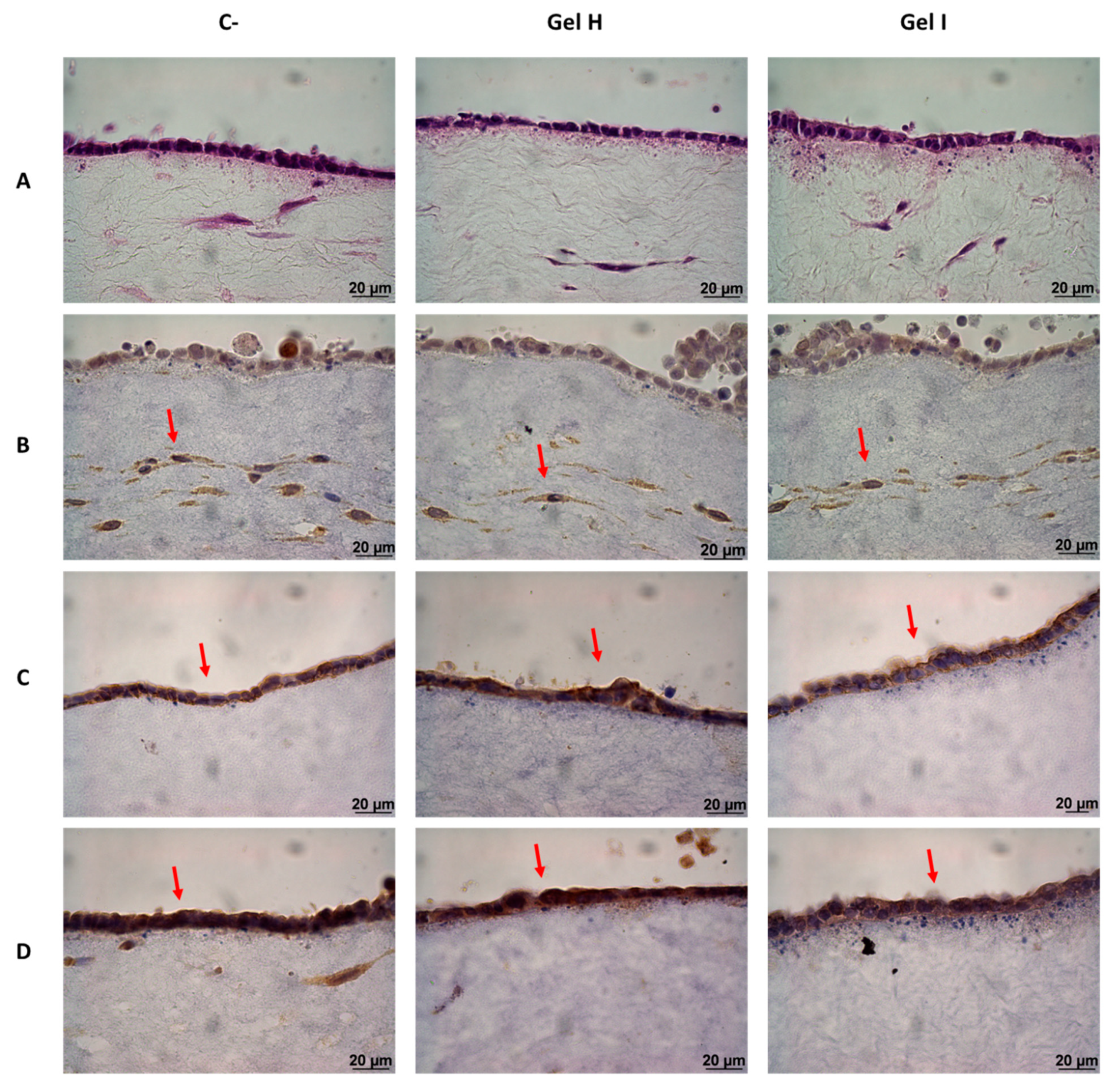
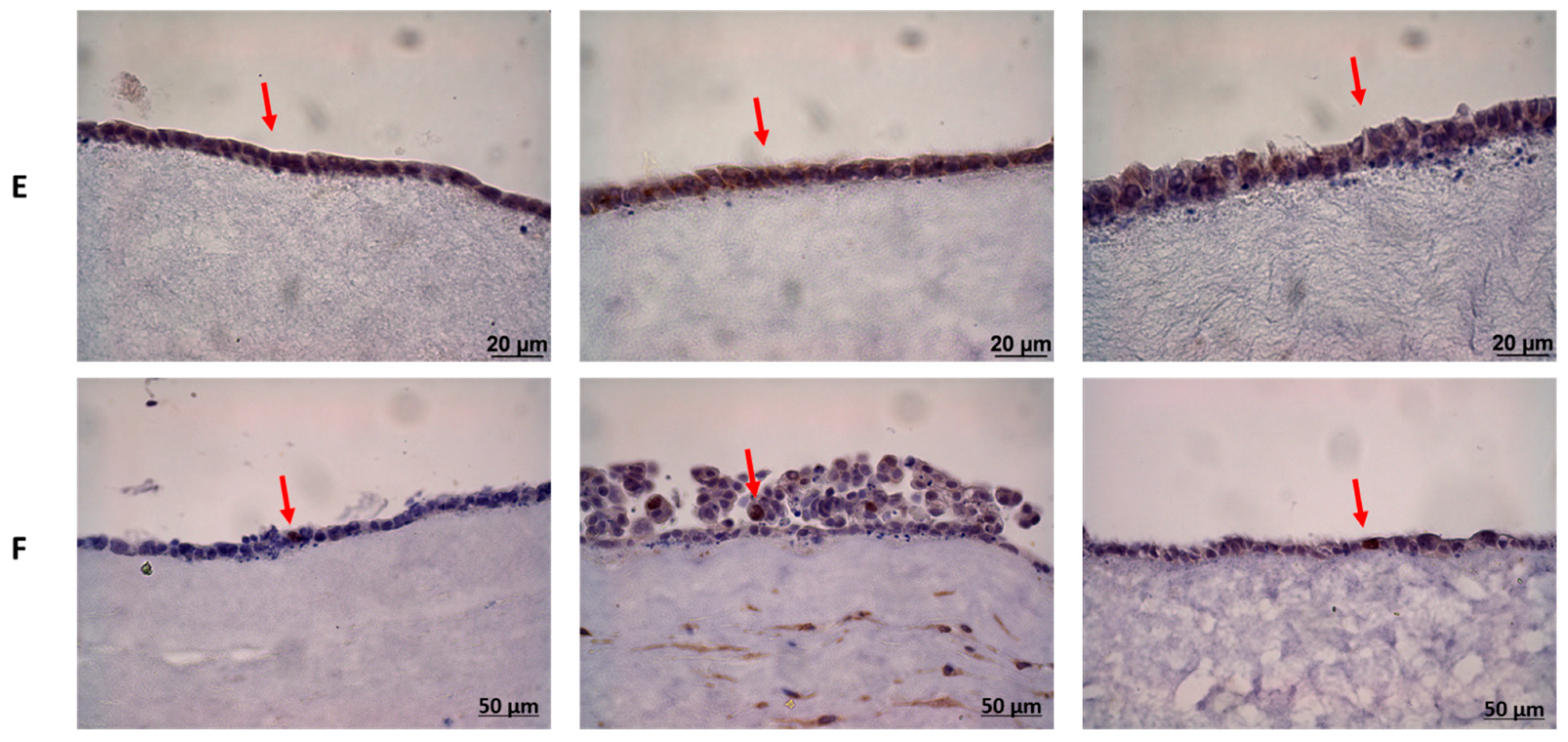
2.4.7. Histology and Inmunohistoquemistry
2.5. Statistical Analysis
3. Results
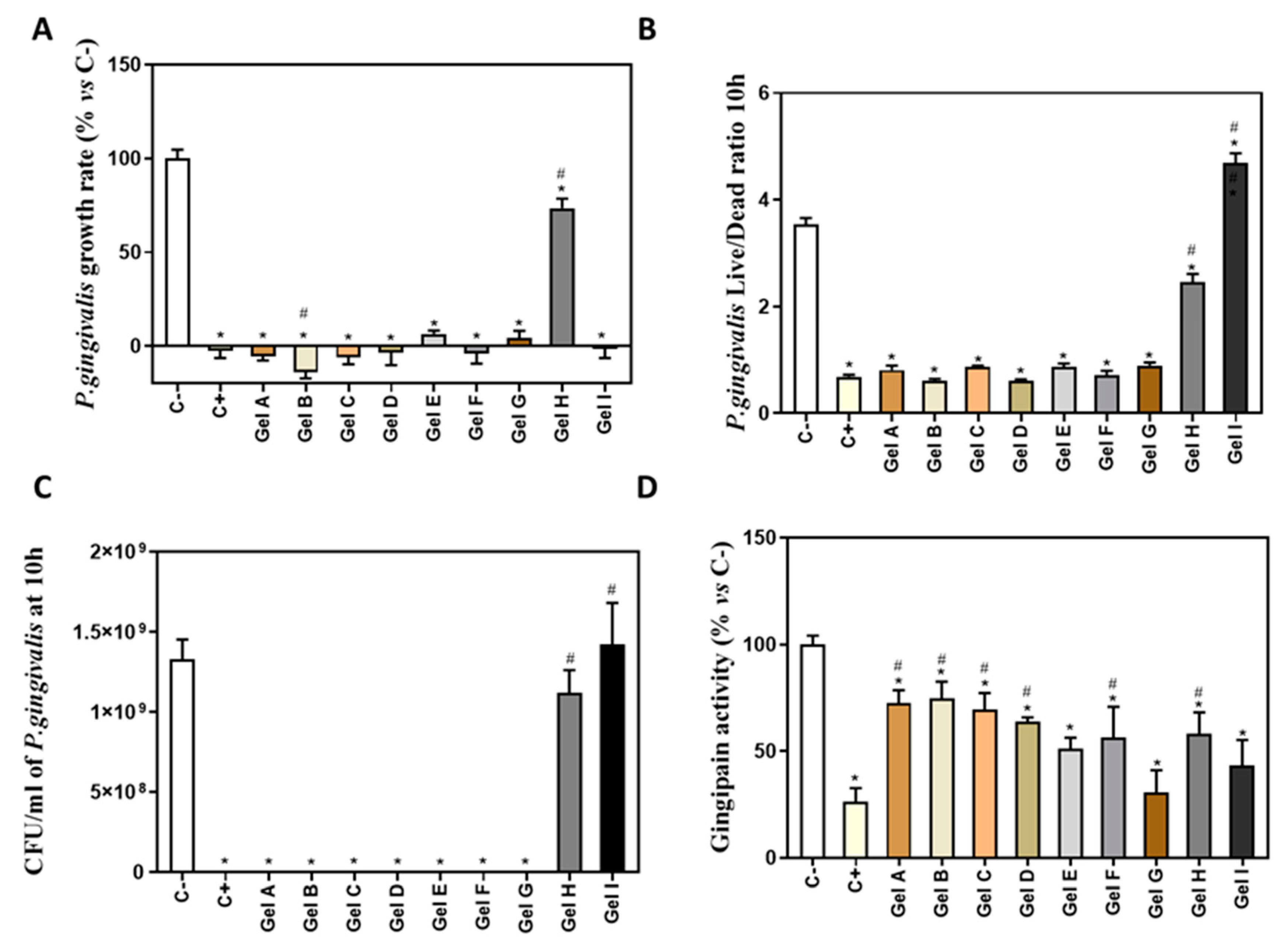
3.1. Results of Antimicrobial Activity of Different Periodontal Gels
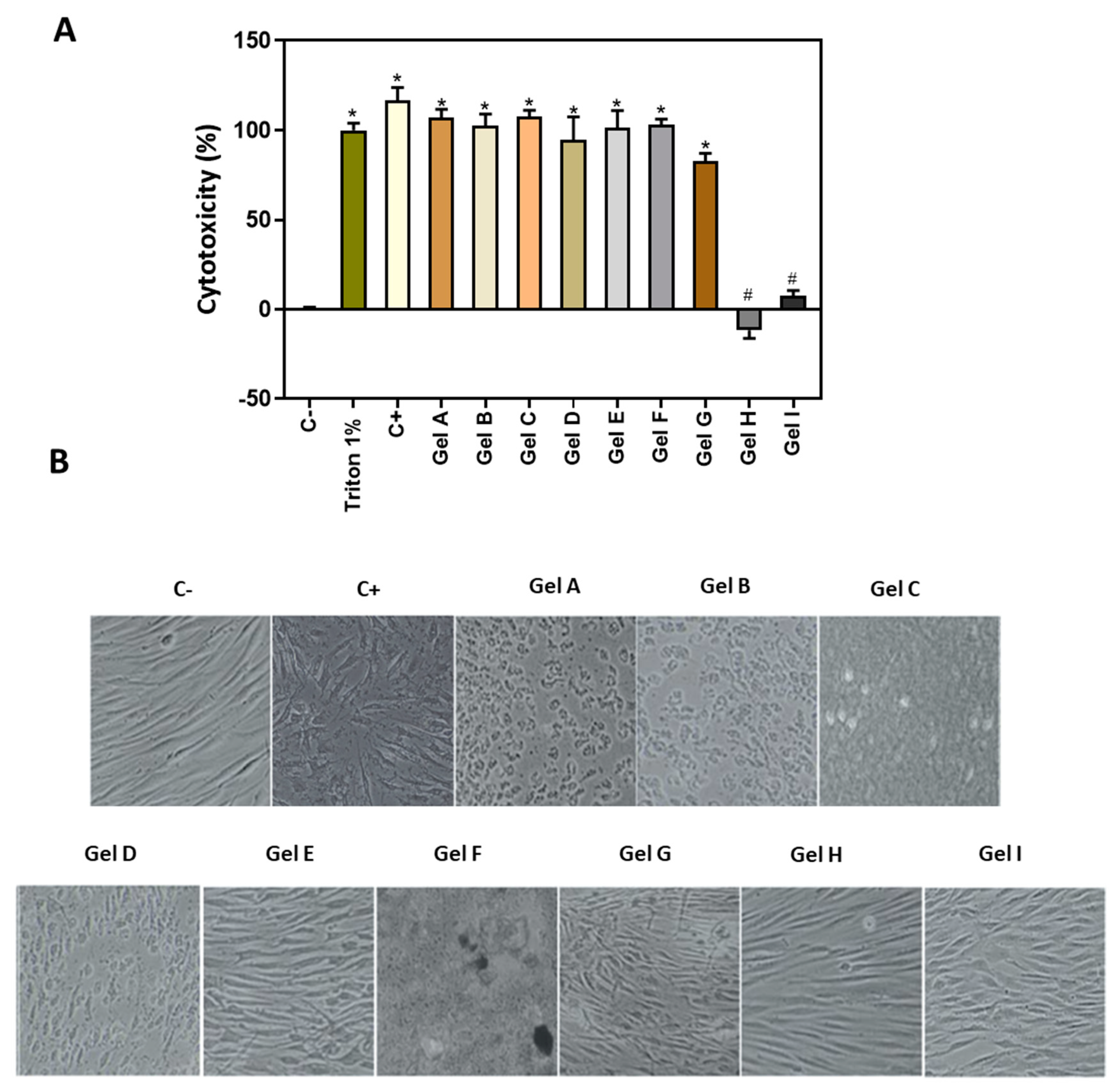
3.2. Effect of Periodontal Gels on 2D Cell Culture
3.3. Results of Periodontal Gels on 3D Cell Culture Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fawzy El-Sayed, K.M.; Dörfer, C.E. Animal Models for Periodontal Tissue Engineering: A Knowledge-Generating Process. Tissue Eng. Part C Methods 2017, 23, 900–925. [Google Scholar] [CrossRef]
- Gómez-Florit, M.; Monjo, M.; Ramis, J.M. Quercitrin for periodontal regeneration: Effects on human gingival fibroblasts and mesenchymal stem cells. Sci. Rep. 2015, 5, 16593. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, A.; Teixeira, C.S. The properties of chlorhexidine and undesired effects of its use in endodontics. Quintessence Int. Berl 2015, 46, 575–582. [Google Scholar]
- Scheibler, E.; Garcia, M.C.R.; Medina da Silva, R.; Figueiredo, M.A.; Salum, F.G.; Cherubini, K. Use of nystatin and chlorhexidine in oral medicine: Properties, indications and pitfalls with focus on geriatric patients. Gerodontology 2017, 34, 291–298. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontology 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Pucher, J.J.; Daniel, C. The Effects of Chlorhexidine Digluconate on Human Fibroblasts In Vitro. J. Periodontol. 1992, 63, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, A.; Kalinowska-Lis, U. 18β-Glycyrrhetinic acid: Its core biological properties and dermatological applications. Int. J. Cosmet. Sci. 2019, 41, 325–331. [Google Scholar]
- Marchese, A.; Barbieri, R.; Coppo, E.; Orhan, I.E.; Daglia, M.; Nabavi, S.F.; Izadi, M.; Abdollahi, M.; Nabavi, S.M.; Ajami, M. Antimicrobial activity of eugenol and essential oils containing eugenol: A mechanistic viewpoint. Crit. Rev. Microbiol. 2017, 43, 668–689. [Google Scholar] [CrossRef]
- Sreenivasan, P.K.; Haraszthy, V.I.; Zambon, J.J. Antimicrobial efficacy of 0.05% cetylpyridinium chloride mouthrinses. Lett. Appl. Microbiol. 2013, 56, 14–20. [Google Scholar] [CrossRef]
- Walter, C.; Jawor, P.; Bernimoulin, J.P.; Hägewald, S. Moderate effect of enamel matrix derivative (Emdogain® Gel) on Porphyromonas gingivalis growth in vitro. Arch. Oral Biol. 2006, 51, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, S.; Ranzato, E. Propolis: A new frontier for wound healing? Burn. Trauma 2015, 3, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozkurt, S.B.; Hakki, S.S.; Hakki, E.E.; Durak, Y.; Kantarci, A. Porphyromonas gingivalis Lipopolysaccharide Induces a Pro-inflammatory Human Gingival Fibroblast Phenotype. Inflammation 2017, 40, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Popova, C.; Dosseva-Panova, V.; Panov, V. Microbiology of periodontal diseases. A review. Biotechnol. Biotechnol. Equip. 2013, 27, 3754–3759. [Google Scholar] [CrossRef]
- Bugueno, I.M.; Batool, F.; Keller, L.; Kuchler-Bopp, S.; Benkirane-Jessel, N.; Huck, O. Porphyromonas gingivalis bypasses epithelial barrier and modulates fibroblastic inflammatory response in an in vitro 3D spheroid model. Sci. Rep. 2018, 8, 14914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.L.; Chang, M.C.; Lin, L.D.; Chan, C.P.; Wang, C.Y.; Lin, P.S.; Jeng, J.H. Stimulation of prostanoids and IL-8 production in human gingival fibroblasts by Porphyromonas gingivalis LPS is associated with MEK/ERK signaling. J. Dent. Sci. 2014, 9, 205. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, S.A.; Madani, S.A.; Abediankenari, S. The review on properties of aloe vera in healing of cutaneous wounds. Biomed. Res. Int. 2015, 2015, 714216. [Google Scholar] [CrossRef] [Green Version]
- Patrulea, V.; Ostafe, V.; Borchard, G.; Jordan, O. Chitosan as a starting material for wound healing applications. Eur. J. Pharm. Biopharm. 2015, 97, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Neuman, M.G.; Nanau, R.M.; Oruña-Sanchez, L.; Coto, G. Hyaluronic acid and wound healing. J. Pharm. Pharm. Sci. 2015, 18, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Jung, E.; Kim, Y.; Park, J.; Park, J.; Hong, S.; Kim, J.; Hyun, C.; Kim, Y.S.; Park, D. Asiaticoside Induces Human Collagen I Synthesis through TGFβ Receptor I Kinase (TβRI Kinase)-Independent Smad Signaling. Planta Med. 2006, 72, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.H.; Foong, W.C.; Cao, T.; Bay, B.H.; Ouyang, H.W.; Yip, G.W. Chondroitin sulfate in palatal wound healing. J. Dent. Res. 2004, 83, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.A.; Coscia, S.A.; Jotwani, R.; Iacono, V.J.; Cutler, C.W. Effects of Enamel Matrix Derivative on Porphyromonas gingivalis. J. Periodontol. 2003, 74, 1191–1195. [Google Scholar] [CrossRef]
- Popovska, M.; Fidovski, J.; Mindova, S.; Dirjanska, K.; Ristoska, S.; Stefanovska, E.; Radojkova-Nikolovska, V.; Mitic, K.; Rusevska, B. The effects of NBF gingival gel application in the treatment of the erosive Lichen planus: Case report. Open Access Maced. J. Med. Sci. 2016, 4, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Florit, M.; Monjo, M.; Ramis, J.M. Identification of Quercitrin as a Potential Therapeutic Agent for Periodontal Applications. J. Periodontol. 2014, 85, 966–974. [Google Scholar] [CrossRef]
- Duval, K.; Grover, H.; Han, L.H.; Mou, Y.; Pegoraro, A.F.; Fredberg, J.; Chen, Z. Modeling physiological events in 2D vs. 3D cell culture. Physiology 2017, 32, 266–277. [Google Scholar] [CrossRef]
- Dongari-Bagtzoglou, A.; Kashleva, H. Development of a highly reproducible three-dimensional organotypic model of the oral mucosa. Nat. Protoc. 2006, 1, 2012–2018. [Google Scholar] [CrossRef] [PubMed]
- Bercy, P.; Lasserre, J. Susceptibility to various oral antiseptics of Porphyromonas gingivalis W83 within a biofilm. Adv. Ther. 2007, 24, 1181–1191. [Google Scholar] [CrossRef]
- Kim, S.R.; Jeon, H.J.; Park, H.J.; Kim, M.K.; Choi, W.S.; Jang, H.O.; Bae, S.K.; Jeong, C.H.; Bae, M.K. Glycyrrhetinic acid inhibits Porphyromonas gingivalis lipopolysaccharide- induced vascular permeability via the suppression of interleukin-8. Inflamm. Res. 2013, 62, 145–154. [Google Scholar] [CrossRef]
- Suwannakul, S.; Chaibenjawong, P. Antibacterial Activities of Glycyrrhiza gabra Linn. (Licorice) Root Extract against Porphyromonas gingivalis rand Its Inhibitory Effects on Cysteine Proteases and Biofilms. J. Dent. Indones. 2017, 24, 85–92. [Google Scholar] [CrossRef]
- Yoo, S.-K.; Kim, K.-Y.; You, Y.-O.; Jang, S.-I.; Kim, K.-J.; Park, J.-K.; Chung, C.-P.; Kurihara, H. Effect of glycyrrhetinic acid on the viability of human gingival fibroblasts. J. Korean Acad. Periodontol. 1998, 28, 453. [Google Scholar] [CrossRef] [Green Version]
- Hou, Q.; Li, M.; Lu, Y.-H.; Liu, D.-H.; Li, C.-C. Burn wound healing properties of asiaticoside and madecassoside. Exp. Ther. Med. 2016, 12, 1269–1274. [Google Scholar] [CrossRef] [Green Version]
- Babykutty, S.; Padikkala, J.; Sathiadevan, P.P.; Vijayakurup, V.; Abdul Azis, T.K.; Srinivas, P.; Gopala, S. Apoptosis induction of Centella asiatica on human breast cancer cells. Afr. J. Tradit. Complement. Altern. Med. 2009, 6, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Tyszka-Czochara, M.; Paśko, P.; Reczyński, W.; Szlósarczyk, M.; Bystrowska, B.; Opoka, W. Zinc and propolis reduces cytotoxicity and proliferation in skin fibroblast cell culture: Total polyphenol content and antioxidant capacity of propolis. Biol. Trace Elem. Res. 2014, 160, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimasu, Y.; Ikeda, T.; Sakai, N.; Yagi, A.; Hirayama, S.; Morinaga, Y.; Furukawa, S.; Nakao, R. Rapid Bactericidal Action of Propolis against Porphyromonas gingivalis. J. Dent. Res. 2018, 97, 928–936. [Google Scholar] [CrossRef]
- Nagata, H.; Inagaki, Y.; Yamamoto, Y.; Maeda, K.; Kataoka, K.; Osawa, K.; Shizukuishi, S. Inhibitory effects of macrocarpals on the biological activity of Porphyromonas gingivalis and other periodontopathic bacteria. Oral Microbiol. Immunol. 2006, 21, 159–163. [Google Scholar] [CrossRef]
- Kim, J.E.; Shklar, G. The effect of vitamin E on the healing of gingival wounds in rats. J. Periodontol. 1983, 54, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Teng, F.; He, T.; Huang, S.; Bo, C.P.; Li, Z.; Chang, J.L.; Liu, J.Q.; Charbonneau, D.; Xu, J.; Li, R.; et al. Cetylpyridinium Chloride Mouth Rinses Alleviate Experimental Gingivitis by Inhibiting Dental Plaque Maturation. Int. J. Oral Sci. 2016, 8, 182–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feres, M.; Figueiredo, L.C.; Faveri, M.; Stewart, B.; De Vizio, W. The effectiveness of a preprocedural mouthrinse containing cetylpyridiniuir chloride in reducing bacteria in the dental office. J. Am. Dent. Assoc. 2010, 141, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Fromm-Dornieden, C.; Rembe, J.-D.; Schäfer, N.; Böhm, J.; Stuermer, E.K. Cetylpyridinium chloride and miramistin as antiseptic substances in chronic wound management-prospects and limitations. J. Med. Microbiol. 2015, 64, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Prashar, A.; Locke, I.C.; Evans, C.S. Cytotoxicity of clove (Syzygium aromaticum) oil and its major components to human skin cells. Cell Prolif. 2006, 39, 241–248. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Zhu, X.; Cao, P.; Wei, S.; Lu, Y. Antibacterial and antibiofilm activities of eugenol from essential oil of Syzygium aromaticum (L.) Merr. & L. M. Perry (Clove) leaf against periodontal pathogen Porphyromonas gingivalis. Microb. Pathog. 2017, 113, 396–402. [Google Scholar]
- Wyganowska-Swiatkowska, M.; Urbaniak, P.; Lipinski, D.; Szalata, M.; Kotwicka, M. Human gingival fibroblast response to enamel matrix derivative, porcine recombinant 21.3-kDa amelogenin and 5.3-kDa tyrosine-rich amelogenin peptide. Hum. Cell 2017, 30, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gestrelius, S.; Andersson, C.; Johansson, A.C.; Persson, E.; Brodin, A.; Rydhag, L.; Hammarström, L. Formulation of enamel matrix derivative for surface coating. Kinetics and cell colonization. J. Clin. Periodontol. 1997, 24, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Olitzky, I. Antimicrobial properties of a propylene glycol based topical therapeutic agent. J. Pharm. Sci. 1965, 54, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Spahr, A.; Lyngstadaas, S.P.; Boeckh, C.; Andersson, C.; Podbielski, A.; Haller, B. Effect of the enamel matrix derivative Emdogain on the growth of periodontal pathogens in vitro. J. Clin. Periodontol. 2002, 29, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Bartold, P.M.; Narayanan, A.S. Molecular and cell biology of healthy and diseased periodontal tissues. Periodontology 2000 2006, 40, 29–49. [Google Scholar] [CrossRef]
- Satish, L.; Kathju, S. Cellular and Molecular Characteristics of Scarless versus Fibrotic Wound Healing. Dermatol. Res. Pract. 2010, 2010, 790234. [Google Scholar] [CrossRef] [Green Version]
- Häkkinen, L.; Strassburger, S.; Kähäri, V.M.; Scott, P.G.; Eichstetter, I.; Lozzo, R.V.; Larjava, H. A role for decorin in the structural organization of periodontal ligament. Lab. Investig. 2000, 80, 1869–1880. [Google Scholar] [CrossRef] [Green Version]
- Ivanovski, S.; Haase, H.R.; Bartold, P.M. Isolation and characterization of fibroblasts derived from regenerating human periodontal defects. Arch. Oral Biol. 2001, 46, 679–688. [Google Scholar] [CrossRef]
- Birkedal-Hansen, H. Role of matrix metalloproteinases in human periodontal diseases. J. Periodontol. 1993, 64, 474–484. [Google Scholar]
- Sakagami, G.; Sato, E.; Sugita, Y.; Kosaka, T.; Kubo, K.; Maeda, H.; Kameyama, Y. Effects of nifedipine and interleukin-1alpha on the expression of collagen, matrix metalloproteinase-1, and tissue inhibitor of metalloproteinase-1 in human gingival fibroblasts. J. Periodontal Res. 2006, 41, 266–272. [Google Scholar] [CrossRef]
- Pandya, M.; Diekwisch, T.G.H. Enamel biomimetics-fiction or future of dentistry. Int. J. Oral Sci. 2019, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Hinz, B.; Phan, S.H.; Thannickal, V.J.; Galli, A.; Bochaton-Piallat, M.-L.; Gabbiani, G. The myofibroblast: One function, multiple origins. Am. J. Pathol. 2007, 170, 1807–1816. [Google Scholar] [CrossRef]
- Goda, S.; Inoue, H.; Kaneshita, Y.; Nagano, Y.; Ikeo, T.; Ikeo, Y.T.; Iida, J.; Domae, N. Emdogain stimulates matrix degradation by osteoblasts. J. Dent. Res. 2008, 87, 782–787. [Google Scholar] [CrossRef]
- Lyngstadaas, S.P.; Lundberg, E.; Ekdahl, H.; Andersson, C.; Gestrelius, S. Autocrine growth factors in human periodontal ligament cells cultured on enamel matrix derivative. J. Clin. Periodontol. 2001, 28, 181–188. [Google Scholar] [CrossRef]
- Jiang, J.; Fouad, A.F.; Safavi, K.E.; Spångberg, L.S.W.; Zhu, Q. Effects of enamel matrix derivative on gene expression of primary osteoblasts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Villa, O.; Brookes, S.J.; Thiede, B.; Heijl, L.; Lyngstadaas, S.P.; Reseland, J.E. Subfractions of enamel matrix derivative differentially influence cytokine secretion from human oral fibroblasts. J. Tissue Eng. 2015, 6, 2041731415575857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reijnders, C.M.A.; van Lier, A.; Roffel, S.; Kramer, D.; Scheper, R.J.; Gibbs, S. Development of a Full-Thickness Human Skin Equivalent In Vitro Model Derived from TERT-Immortalized Keratinocytes and Fibroblasts. Tissue Eng. Part A 2015, 21, 2448–2459. [Google Scholar] [CrossRef] [Green Version]
- Watt, F.M. Involucrin and other markers of keratinocyte terminal differentiation. J. Investig. Dermatol. 1983, 81, 100s–103s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gröger, S.; Michel, J.; Meyle, J. Establishment and characterization of immortalized human gingival keratinocyte cell lines. J. Periodontal Res. 2008, 43, 604–614. [Google Scholar] [CrossRef]
- Mujyambere, B.; Jayaraj, R.; Suja, S. Cytokeratin 19 (CK19) as a marker for Epithelial Differentiation and Malignant Transformation: Its Clinical relevance in Diagnosis, Prognosis and Treatment response monitoring. IRE J. 2018, 2, 51–61. [Google Scholar]
- Moll, R.; Franke, W.W.; Schiller, D.L.; Geiger, B.; Krepler, R. The catalog of human cytokeratins: Patterns of expression in normal epithelia, tumors and cultured cells. Cell 1982, 31, 11–24. [Google Scholar] [CrossRef]
- Scholzen, T.; Gerdes, J. The Ki-67 protein: From the known and the unknown. J. Cell. Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nomenclature | Gel | Manufacturer | Antibacterial Factor | Regenerative Factor |
|---|---|---|---|---|
| Gel A | Bexident post Gel | ISDIN, Barcelona, Spain | CHX 0.2% | Chitosan 0.5% |
| Gel B | Perio-Aid Gel Bioadhesive | Dentaid SL, Barcelona, Spain | CHX 0.2% | Hyaluronic acid 0.2% |
| Gel C | Lacer Mucorepair Gel | Lacer SA, Barcelona, Spain | Enoxolone 0.2% | Hyaluronic acid 0.2%, asiaticoside 0.3% |
| Gel D | Clorhexidina Lacer Gel Bioadhesive | Lacer SA, Barcelona, Spain | CHX 0.2% | - |
| Gel E | Oralsan Gel Gengivale | IDS Spa, Savona, Italy | CHX 0.5% | Aloe vera |
| Gel F | Oralsan NBF Gel Gengivale | IDS Spa, Savona, Italy | Propolis extract, Plant extracts | Propolis extract, Vitamin C and E, Plant extracts |
| Gel G | Klirich Pro | Itena Clinical, Villepinte, France | CPC 1–2.5%, Eugenol 0–1%, Plant extracts | Hyaluronic acid, Plant extracts |
| Gel H | Syntoss Biogel | DSI dental solution Israel Ltd., Ashdod, Israel | CHX 0.025% | Chondroitin Sulfate |
| Gel I | Emdogain (EMD) | Straumann, Basel, Switzerland | PGA | Amelogenin 30 mg/mL |
| Related Function | Gene | Primer Sequence (5′-3′) | Product Size (bp) | GenBank ID |
|---|---|---|---|---|
| ECM component | Collagen I α1 (COL1A1) | S: CCTGACGCACGGCCAAGAGG A: GGCAGGGCTCGGGTTTCCAC | 122 | NM_000088.3 |
| Collagen III α1 (COL3A1) | S: GGCTACTGGGCCTGGTGGT A: CCACGTTCACCAGGGGCACC | 190 | NM_000090.3 | |
| Decorin (DCN) | S: ATCTCAGCTTTGAGGGCTCC A: GCCTCTCTGTTGAAACGGTC | 146 | NM_001920.3 | |
| ECM turnover | Matrix metalloproteinase-1 (MMP-1) | S: TGTCAGGGGAGATCATCGGGAC A: TGGCCGAGTTATGAGCTGCA | 177 | NM_002421.3 |
| Tissue inhibitor of metalloproteinase-1 (TIMP-1) | S: TTCCGACCTCGTCATCAGGG A: TAGACGAACCGGATGTCAGC | 144 | NM_003254.2 | |
| Wound Healing/Fibrogenic | α-Smooth muscle actin 2 (ACTA2) | S: TAAGACGGGAATCCTGTGAAGC A: TGTCCCATTCCCACCATCAC | 184 | NM_001141945.1 |
| Transforming growth factor-β1 (TGF-β1) | S: TGTCACCGGAGTTGTGCGGC A: GGCCGGTAGTGAACCCGTTG | 131 | NM_000660.4 | |
| Endothelin-1 (END) | S: ACGGCGGGGAGAAACCCACT A: ACGGAACAACGTGCTCGGGA | 147 | NM_001955.4 | |
| Reference gene | Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) | S: TGC ACC ACC AAC TGC TTA GC A: AAG GGA CTT CCT GTA ACA A | 87 | NM_002046.3 |
| Beta-Actin (ACTBL2) | S: CTG GAA CGG TGA AGG TGA CA A: AAG GGA CTT CCT GTA ACA A | 140 | NM_001101.3 | |
| 18S ribosomal RNA (18S rRNA) | S: GTAACCCGTTGAACCCCATT A: CCATCCAATCGGTAGTAGCG | 151 | NR_146156.1 |
| Antibody | Dilution | Clone | Isotype | Manufacturer |
|---|---|---|---|---|
| Keratin 17 | 1:50 | E-4 | IgG1 | Santa Cruz Biotechnology, Inc., Santa Cruz, CA |
| Keratin 19 | 1:50 | A-3 | IgG1 | Santa Cruz Biotechnology |
| Involucrin | 1:20 | SY5 | IgG1 | Santa Cruz Biotechnology |
| Vimentin | 1:1000 | E-5 | IgG1 | Santa Cruz Biotechnology |
| KI-67 | 1:100 | MM1 | IgG1 | Novocastra, Newcastle, UK |
| Nomenclature | Gel | Antimicrobial Activity | Cytotoxicity | Wound Closure (2D Model) | ||
|---|---|---|---|---|---|---|
| Inhibition of Bacterial Growth | Gingipain Activity | LDH (2D Model) | MTT (3D Model) | |||
| Gel A | Bexident post Gel | +++ | + | +++ | ND | − |
| Gel B | Perio-Aid Gel Bioadhesive | +++ | + | +++ | ND | − |
| Gel C | Lacer Mucorepair Gel | +++ | + | +++ | ND | − |
| Gel D | Clorhexidina Lacer Gel Bioadhesive | +++ | + | +++ | ND | − |
| Gel E | Oralsan Gel Gengivale | +++ | ++ | +++ | ND | − |
| Gel F | Oralsan NBF Gel Gengivale | +++ | + | +++ | ND | − |
| Gel G | Klirich Pro | +++ | ++ | +++ | ND | − |
| Gel H | Syntoss Biogel | − | + | − | − | − |
| Gel I | Emdogain (EMD) | − | ++ | − | − | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munar-Bestard, M.; Llopis-Grimalt, M.A.; Ramis, J.M.; Monjo, M. Comparative In Vitro Evaluation of Commercial Periodontal Gels on Antibacterial, Biocompatibility and Wound Healing Ability. Pharmaceutics 2021, 13, 1502. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13091502
Munar-Bestard M, Llopis-Grimalt MA, Ramis JM, Monjo M. Comparative In Vitro Evaluation of Commercial Periodontal Gels on Antibacterial, Biocompatibility and Wound Healing Ability. Pharmaceutics. 2021; 13(9):1502. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13091502
Chicago/Turabian StyleMunar-Bestard, Marta, Maria Antonia Llopis-Grimalt, Joana Maria Ramis, and Marta Monjo. 2021. "Comparative In Vitro Evaluation of Commercial Periodontal Gels on Antibacterial, Biocompatibility and Wound Healing Ability" Pharmaceutics 13, no. 9: 1502. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13091502